GOOD PRACTICES SRH APPROACHES FOR YOUTHS - ESA INITIATIVE GERAÇÃOBIZ - CORESULT
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Republic of Mozambique
ESA Initiative
GeraçãoBIZ
Good Practices
SRH approaches for youths
Intro
Young women defend
their dreams.
The busy generation takes over
M arisa wants to become a teacher. Joana wants to Marisa, Joana, Ábida and Xiluva are doing things diffe-
rently. These four young women, like many others, are ta-
study in South Africa, Capetown would be her preferred
city, Ábida would like to work in a bank, and Xiluva wants king control of their lives. They volunteer in youth groups
to run a volunteer organisation.* These young women are comprising young women and men. These groups aim to
between 16 and 18 years old and live in Mocuba, a small spread the word on adolescent’s sexual self-determina-
town 150 kilometres north of Zambezia’s capital Queli- tion – and they are the target group of adolescent and
mane in central Mozambique. They are four of Mozam- youth friendly health services and comprehensive sexual
bique’s 2.9 million young women aged 14 to 24. and reproductive education.
Statistically, at least one of them has already experienced
gender-based violence, and two of them could already be
mother of one or two children. To realise their dreams
would be much more difficult then.
But the barriers already start before pregnancy: Most
young women have no experienced older friend with
whom they can talk about sexuality and reproductive
health. In many (rural) communities, aunts or mothers will
most likely tell them to have babies early. Boys’ views are
shaped by their fathers and uncles. It can be difficult to
find information, with health facilities usually being the only
source. But many young people won’t visit a health facility
to seek information: They are afraid that family members
or neighbours might see them and ask: What’s wrong with
you, are you ill? Therefore, many adolescents become
young adults believing that having lots of children as early
as possible is important for social standing and women's
identity. For many adolescent girls, early pregnancy leads
to school drop-out. Even those wanting to return to school
after having given birth often face obstacles.
* Not real name; persons shown in the picture do not correspond
to the people referred to in the text due to privacy reasons.
Index
About ESA, the mission, and this brochure 4
︎
▶︎ Access to reproductive health
and what it means to Mozambican youth 4
▼ Mozambique 7
▼ GeraçãoBIZ 8
PGB: About the Programme GeraçãoBIZ 8
▼ Good Practice 10
PGB Monitoring 10
From paper to digital — the challenge 10
The true reports come by WhatsApp Testimony: Clotilde 11
School Approach 12
►“Cantinho”: the little health corner 12
►For healthier youth: cooperation of schools,
Testimony: Carlos
nurses and community 13
►Cantinhos’ empty fridges 14
►“Most of the visitors are boys” Testimony: Marie Rosa 15
& Olinda
►Girls for Girls 16
►Leading the girl volunteers Testimony: Lídia 17
►Young mothers back at school 18
►Favours for good marks Testimony: Josina 19
Clinical Approach 20
►SAAJ — the safe health alternative 20
►SAAJ in action Testimony: Digna 21
►Schools revitalise Youth Health Facilities Testimony: Feliciana 22
►Community outreach: “First, we talk
Testimony: Digna
to the people” 23
About ESA, the mission, and this brochure
Access to reproductive health
and what it means to Mozambican youth
T his brochure aims to present a picture of the
current situation regarding the sexual and reproductive
health (SRH) of youth in Mozambique, using the example
of Zambezia Province. It describes approaches to providing
better access to preventive health care and other services
for youth in the school environment and in communities.
These include measures rolled-out regionally, as well as lo-
cally-developed solutions that are considered good prac- vinces to strengthen the linkages between the provision of
tices in addressing challenges on the ground. It also sexuality education and youth-friendly health services, the
examines gender equality issues, which are important for national level has only little information about these. It is
understanding and responding to the needs of youth. against this background that the PGB stakeholders at na-
tional level have requested the GIZ ESA Regional Pro-
gramme to support the assessment of approaches on linking
The brochure is one of the products of a consultancy and CSE and Youth-Friendly Health Services (YFHS) in Zambe-
field mission in the Mozambican province Zambezia during zia Province.
the first half of 2018. The consultancy was undertaken in the
context of the German Development Cooperation’s (GIZ)
ESA Regional Programme to support the implementation of
the Eastern and Southern African (ESA) Commitment.
The Programa GeraçãoBIZ is Mozambique’s large um-
brella programme, led by the Government, under which About the Eastern and Southern Africa (ESA)
most of the youth-health related activities are implemented. Initiative
Both ESA and PGB objectives aim to strengthen youths’ ac-
cess to health information and services. Through this, they The Eastern and Southern Africa Commitment Process
has its origins in late 2013. It is a self-commitment of
contribute to reducing the number of early pregnancies and
20 governments in Eastern and Southern Africa to
early marriages, as well as the incidence of HIV and gen- scale-up initiatives on sexual and reproductive health,
der-based violence. Whereas the PGB focuses particularly education and services for youth. The process was ini-
on peer-to-peer approaches, the ESA Commitment also tiated by UNAIDS, and is supported by UNESCO,
considers the scaling-up of comprehensive sexuality edu- UNFPA, Germany’s Ministry for Economic Cooperation
and Development (BMZ) as well as other development
cation (CSE) in schools, including the integration of CSE into
partners. Twenty Ministers of Health and Education
the curricula and teacher training. have committed to achieving set targets by 2020. Im-
plementation is tracked through a regional accountabi-
lity framework. Since April 2015, BMZ has
The GIZ ESA Regional Programme has supported Mo- commissioned GIZ with the ESA Regional Programme
zambique’s Ministry of Education in the roll-out of CSE to support the implementation of the ESA commitment
teacher training in both Nampula and Zambezia provinces in four cluster countries - Mozambique, Zambia, Nami-
in close cooperation with UNESCO and UNFPA. Although bia and South Africa.
quite a number of activities are happening in these pro-
4
The objective of this consultancy mission was hence to
Mozambique
support Mozambique’s ESA commitment and the PGB im-
plementation process by mapping projects and approaches
regarding youth’s access to sexual and reproductive health
knowledge and services. The outputs are reports explaining
the mission’s detailed findings; the reporting mechanism of
the state driven youth initiative Programa GeraçãoBIZ
(PGB), and the involved public services and departments of
health, education and youth; as well as identified good prac-
tices.
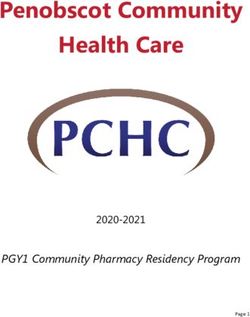
This consultancy was implemented by Health Focus, com-
missioned by the GIZ ESA Regional Programme. The mis-
Zambezia
sion’s consultants were accompanied by a representative of
Quelimane
MISAU and of MINEDH. They cooperated closely with the
provincial and district administration in Zambezia’s capital
Quelimane, as well as surrounding districts. Some of the
local officials also accompanied the field visits. Interviews
were held with staff of health centres, schools and local
community-based organisations (CBO); with community
members as well as with youth volunteer groups. The first
step involved mapping projects and their targets using a
web-based survey tool. From this overview, some projects
were identified as potentially good practices, which were
then more closely documented. An important challenge of
Credit: wikiMedia
this mission was that comprehensive quantitative data and
result based outcomes were rarely available. Maputo
MINEDH:Ministério da Educação e Desenvolvi
mento Humano / Ministry of Education Zambezia is a province in Mozambique’s central region
and Human Development with over five million inhabitants in an area of the size of
MISAU: Ministério da Saúde / Ministry of Health Iceland; its capital is Quelimane. In 1999 it was the first
province, along with Maputo City, where PGB was im-
MJD: Ministério da Juventude e Desporto / plemented. The national partners decided that the field
Ministry of Youth and Sports mission should be conducted in Zambezia Province,
MGCAS: Ministério do Género, Criança, e Acção since many activities are currently implemented in that
Social / Ministry of Gender, Children and province. The fact that PGB started in 1999 in Zambezia
Social Affairs and Maputo City may have also influenced the decision.
5
The products of the field mission – the reports, this bro- that the examples selected were indeed good practices, and
chure, and documentation of selected good practices – were discussed how these could be improved upon and/or repli-
developed with significant input from key stakeholders, na- cated in other areas. In June, PGB committee members at
mely representatives from the Ministry of Youth and Sport national level participated in a workshop, where the draft
(MJD), Ministry of Education and Human Development (MI- brochure and good practices documentation were presented
NEDH), and Ministry of Health (MISAU); PGB’s new part- and discussed. Participants provided concrete suggestions
ners, Ministry of Gender, Children and Social Action for improving the documents, with a particular focus on ma-
(MGCAS) and Ministry of Justice; as well as important in- king them useful and appropriate for national stakeholders.
ternational and national partners such as UNFPA, Currently, the PGB stakeholders plan to develop a new stra-
UNESCO, UNAIDS and the youth network Coalizão. The tegy for their coordination of youth (including health-related)
findings of, and key recommendations emerging from the objectives. The outcomes of this mission deliver important
field mission, were first presented at a workshop for key sta- inputs to this process. This presents a great opportunity to
keholders at the provincial level, as well as PGB committee align the PGB priorities to the targets of the ESA commit-
members, in Beira in May 2018. Stakeholders confirmed ment.
Map of countries included in the ESA Commitment
Process
All interviewees consented to the publication of their
pictures and statements. However, in order to protect
the privacy, names of youths have been changed and
photographs are not of the youths mentioned in the ar-
Credit: youngpeopletoday.net
ticle on the same page.
This brochure could only be developed due to the
openness and professionalism of all involved stakehol-
ders. Therefore, the consultants want to express their
gratitude to these partners.
Note: Map is indicative and does not reflect official boundaries
6
Mozambique
M ozambique is one of the poorest countries of the world with an extremely young population (ave-
rage age: 17.2 years). Almost half of the population is under 15 years old. This equates to about 13 million
people, many of whom will become adolescents in the near future. A fifth of the population are already ado-
lescents (in Mozambique up to 24 years old). Half of the adolescent girls have their first child before the
Credit: GDJ — Pixabay
age of 18, more than 20 per cent before 16. Access to education and to health services has improved si-
gnificantly in the past years. Nevertheless, knowledge regarding sexual and reproductive health is limited
among large parts of the population. The initiative Programa GeraçãoBIZ is the most important access
point to youth – and in some cases indirectly to their parents – to facilitate behaviour change that enables
adolescents to lead healthy and autonomous lives.
Mozambique Demographic Baseline Data
Profile 2018 Prevalence in per cent
65+ - 3%
Target
Woman married
ESA
48%
5
55-64 - 3% before the age of 18 ***
Target
Prevalence of
ESA
37%
4
genderbased violence *
age 25-54
27% Pregnancies
56%
among 18 year olds *
Pregnancies
39%
among 17 year olds *
Target
ESA
3
Pregnancies
22%
age 15-24 among 16 year olds *
22%
Pregnancies
10.5%
among 15 year olds *
HIV prevalence
2.8%
among young men
HIV prevalence
4.6%
among young women
age 0-14 HIV prevalence rate
Target
45% among men aged 10.2%
ESA
1
15 to 49
HIV prevalence rate
among women aged 14.2%
15 to 49
HIV prevalence rate
among adult aged 12.3%
15 to 49 **
Age
* INE 2013; data 2011 (Instituto Nacional de Estatistica, MZ)
** HIV prevalences: UNAIDS 2016
Source: IndexMundi.com *** UNICEF 2015
7
GeraçãoBIZ
PGB: About the Programme GeraçãoBIZ
M ozambique's youth are socio-cultural, physical/sports and economic activities as a
always busy, or ‘bizy’ as many young mechanism to improve … life quality and well-being”. Some
people like to write. That’s why it is the of PGB’s objectives are also related to the National HIV
BIZgeneration – GeraçãoBIZ: Always Council’s strategic objectives for 2015 to 2019 (PEN IV).
seeking challenges and trying to do
things differently. This at least was the
assumption when the initiative Pro- After some years of limited activity, PGB has been under-
grama GeraçãoBIZ (PGB) was laun- going a process of revival since 2016. Zambezia is again
ched in 1999, first in Mozambique’s central province one of the priority provinces. The largest current PGB initia-
Zambezia, and the nation’s capital Maputo, then all over the tives are financed and implemented by UNICEF, UNFPA and
country. PEPFAR. It is steered by a committee comprising the Minis-
try for Youth and Sports (MJD), the Ministry of Education
(MINEDH), and the Ministry of Health (MISAU) with the par-
PGB is Mozambique’s most important initiative that targets ticipation of the ministries of gender and of justice, and im-
youth. It covers social and educational activities. The main plemented by local and international organisations,
objective is based on the 2nd priority of Mozambique’s Five- predominantly through large networks of youth volunteers.
Year-Plan, namely: to “promote the participation of youth in
Coherence between GeraçãoBIZ and the ESA Initiative
ESA
ESAtargets
targets PGB targets
TARGET 1: Consolidate recent and hard-won gains Main Objective: Improve adolescent sexual and re-
in the reduction of HIV prevalence, and push towards productive health (ASRH) and reduce the incidence
eliminating all new HIV infections among adolescents of HIV and AIDS… and STIs.
and young people aged 10-24. PEN IV: Reduce … HIV infection by 30% until 2019.
Reduce the vulnerability of adolescents and youth by
promotion of access to information about SRH, STI,
TARGET 2: Increase to 95% the number of adoles- HIV/AIDS.
cents and young people aged 10-24 who demonstrate PEN IV: Increase the comprehensive knowledge of
comprehensive HIV prevention knowledge levels. youth 15 to 24 years old in regard to HIV by 60% until
2019.
TARGET 3: Reduce early and unintended pregnan- Specific Obj.: Reduce the incidence of early pre-
cies among young people by 75%. gnancy; Reduce the incidence of unsafe abortions.
TARGET 4: Eliminate gender-based violence. Foster life skills and the promotion of quality clinical
(medical) services, in regard to human rights and gen-
der (equality).
TARGET 5: Eliminate child-marriage.
8
ESA and PGB objectives
aim to strengthen youths’
access to SRH information.
Mozambique’s Ministry of Health (MISAU)
has inaugurated youth-oriented spaces in a
large number of health centres (Serviço de
Amigos dos Adolescentes e Jovens, SAAJ).
Other donor funded initiatives include an
anonymous SMS counselling service, which
aims to provide education on reproductive
health and to sensitise youth on HIV preven-
tion. It also promotes the use of family plan-
ning services and motivates its users to seek
health advice at a SAAJ. The cascading
mentoring system among girls and young
women, used by the projects “DREAMS”
and “raparigaBIZ” has similar objectives:
specially trained nurses counsel the pupils
on SRH and refer them to newly (re-)establi-
shed youth friendly health services (SAAJ).
Mentors – youth volunteers – pro-actively hold presentations
about SRH topics for school students and community youth
and, where required, refer them to the school nurses or
SAAJ. The mentors also link communities and schools, for
example when they help young mothers to return to school
after having dropped out during pregnancy. The innovation
in this approach is that this represents a shift from PGB’s
traditional peer-to-peer approach to a mentor-based ap-
proach. Many more activities are implemented by local and
national NGOs, such as AMODEFA, which is the only civil
society organisation providing youth counselling and a youth
health facility, thereby supporting the public service with the
provision of better access to SRH services.
● A “SAAJ” is an area of a health facility especially
for youth to facilitate their access to SRH services.
.
● A “Cantinho” is a dedicated space in schools,
where a nurse provides counselling in SRH, and
ensures the linkage to the nearest SAAJ.
The ESA Commitment targets complement the
PGB’s targets. The main focus of PGB measures are ● “DREAMS” and “raparigaBIZ” are two of the lar-
on peer-to-peer approaches for in and out-of-school gest current programs targeting youth health.
youth. The institutionalisation of CSE in schools is DREAMS targets youth irrespective of gender,
not addressed by the PGB. The ESA Commitment while RaparigaBIZ focusses on girls and young
targets consider both the development of a CSE cur- women. Both contribute significantly to lower rates
riculum framework as well as capacity building of of early pregnancy, marriage, and school drop out
teachers in CSE. of young mothers.
9
Good Practice
PGB Monitoring
From paper to digital — the challenge
M onitoring is complex. The simplest tasks are level, with representatives of the three main stakeholder mi-
those most prone to error: volunteers fill out short forms sta- nistries of health, education and youth, accompanied by the
ting whom they visit when and why. Their supervisor reviews ministries of justice and gender. There are also similar mul-
and aggregates the information. Everything is written by tisectoral committees at province level. Their members’
hand. That is the case with most of the volunteer programs, tasks are to coordinate implementing organisations; to liaise
including “raparigaBIZ”, which provides young female men- with NGOs and other sectors; and understand the needs
tors for adolescent girls. “Since I started coordinating the ra- and demands on the ground. Therefore, theoretically, data
parigaBIZ mentors, I never had a reporting form,” says a from the health, education and youth ministries feeds into
youth volunteer coordinator. She developed one herself, and the PGB reports. But at the community level, reporting from
now aggregates the information on her computer and sectors is combined. Data on numbers of youth trained at
passes this on to her organisation’s supervisor. So far, she an individual school in health, may therefore be fed into to
never received any feedback on the data. “I have no idea all three sectors at the provincial and national level, and, as
what they do with it,” she says. a result, be over-reported in national reports.
Nurses in youth health centres also fill in forms that are Furthermore, PGB at national level collects youth-relevant
crammed with columns. They record patients, number of data from several ministries, but may also receive data from
youth counselled, as well as results of health tests. Some- the PGB province committee, as well as from implementa-
times they get confused and fill the monthly totals in each tion partners. Their data may or may not have already been
of the four week-columns, quadrupling the number of pa- integrated at province level. As a result, it is difficult to inter-
tients. Simple offices, overflowing folders and shelves, and pret aggregated data.
humid air pose difficulties for storing
these paper-based forms. District health
officers are meant to collect the forms. The revitalisation of PGB led to an effort
That’s why for many administration per- to strengthen data collection and mana-
sonnel, monitoring is considered equal gement, especially in Zambezia. The
to field visits. Sometimes, nobody PGB provincial coordinators were ex-
comes to collect the forms. In other pected to implement a mapping process
cases, the forms are only collected by by June 2017. However, only eight of
the international organisation who finan- Mozambique’s eleven provinces contri-
ced the equipment. buted data; Zambezia had not finalised
its mapping by May 2018. In addition,
many of the coordination meetings at
The forms that reach the district or pro- provincial and district level were not
vince office have to be digitised into held in 2017.
Excel sheets. Thousands of handwritten
numbers combined with time pressure
can lead to simple errors, for example
mixing-up the use of decimal and thou-
sands separators.
PGB follows a multisectoral approach: it At ground level, monitoring is
is steered by a committee at national paper based.
10Clotilde receives reports
via WhatsApp.
Testimony
Clotilde
The true reports
come by WhatsApp
Clotilde plays with her mo-
The group exists since March 2016; planning. Sexually transmitted di-
currently there are 19 district coordi- seases will be another important
bile phone. In front of her, on her nators, 12 nurses and five province topic during discussions and
desk, are a laptop and an old compu- staff in the group. Three district coor- speeches.
ter. Mostly she uses the laptop, but dinators are not in the group because
some data are still stored on the old they do not have mobile phones that Four participants will be awarded a
computer. Eleven other desks with support WhatsApp. prize for asking questions. Who asks
computers, and another with a ty- the most, or most pertinent, ques-
pewriter, stand in the large room on Some group members send pictures tions will receive a t-shirt for example.
the third floor of a Portuguese colo- from health days in remote commu- The aim is to motivate youth to speak
nial building. The room’s floor looks nities or schools. Others use the out, to ask questions, and to share
like a spider web made of power group to prepare a health market with knowledge. Where youth are reluc-
cords. Four colleagues sit in the different prevention activities, pre- tant to ask when something is not un-
room, their backs to the big windows. sentations and testing opportunities. derstood, such approach is of high
The provincial health administration “The true reports are here”, she value.
has its offices in this building. says. Clear messages, short sen-
tences, facts, pictures and observa- Clotilde has been working for one
Clotilde checks her WhatsApp mes- tions. Formal reports need much year at the provincial health adminis-
sages: “Here I get the news from more time. tration coordinating PGB activities.
my colleagues in the schools and She is directly subordinate to the di-
health centre,” she says. As the per- “Right now, we are preparing a rector to strengthen health at
son responsible for school health, school show”, says Clotilde. “The schools. Before that, she worked as
she is part of a WhatsApp group health director had the idea last a nurse and studied psychology, and
comprising officers and focal points year. Two months later, the first was a youth health counsellor. So-
from education, youth and sports, school show was held. That was metimes she misses working directly
and health in the various administra- not planned nor budgeted. Even with youth and patients.
tions. One member asks for some so, we managed to get the money Again she checks her messages: a
statistical data. Clotilde answers that together from our budget, and by nurse from a youth health centre 150
the district officer for youth and edu- involving some NGOs.” Four more kilometres away just sent a photo-
cation has this. The inquirer now school shows are planned for 2018 in graph of the weekly monitoring
knows to whom to write the letter re- and around Quelimane, Zambezia’s sheet, packed with columns showing
questing information. “This is much provincial capital. They anticipate numbers of youth advised, tested,
faster, than the usual way: asking about 200 participants for each and adhering to treatment plans. Clo-
here and there, writing letters to event, mostly school students. Volun- tilde will have to transfer the numbers
several institutions one after ano- teers will be there to provide counsel- to the Excel sheet on one of her com-
ther”, Clotilde states. ling to participants regarding family puters.
11Good Practice
School Approach
Volunteer mentors pro-actively talk
to school students and motivate
them to seek advice in the
school’s health corner.
“Cantinho”: the little health corner
177 is the number of cantinhos in Mozambique.
Many secondary schools have a “little corner”, where school
students can receive counselling, family planning advice,
and condoms. Here they can talk about gender roles as well
as sexual harassment or early pregnancies. In Zambezia
province, nurses specifically trained to counsel youth work
here every day.
All the rooms look very much the same, usually equipped cess to the students than the nurse. They make contact with
with a small black sofa, a few white metal chairs, and an the students during the school assembly before the school
empty refrigerator. The equipment is donor financed, the shift starts or during school breaks. The pupils share their
nurses’ salaries too.* The schools provide a room and personal cases with the mentors, who try to convince them
contribute with electricity supply. As yet no concept has to seek counselling at the cantinho. Some students may
been developed to facilitate the integration of nurses into also be advised to visit the psychologist, who attends about
the public health sector to ensure sustainability. once a week.
A similar approach was previously implemented until The use of volunteer-“mentoras” to refer students to the can-
2011/2012: Students ran small school clubs, where other tinho’s nurse is a good practice, as it helps overcome the
students could seek advice regarding sexual and reproduc- reluctance of many adolescents to ask the nurse for advice
tive health. Nowadays, cooperation exists between the can- because of their respect for her. This is despite the fact that
tinhos and the nearest health facility or youth friendly health many of the nurses are only five to ten years older than the
service (SAAJ). If a school’s nurse thinks that a student students.
should do a health test, she advises them accordingly. It
may take one meeting or several, until a student is ready to
take a HIV test. Then she refers the student to the health
facility. A voucher system is used for monitoring: the health
facility staff signs one copy for return to the school nurse
and keeps another. This enables the nurse to count and fol-
low-up how many referred students really went to the health
facility.
The school nurse cooperates with volunteer mentors, the * The installation of “cantinhos” with nurses in schools and mento-
ras, is part of PEPFAR’s regional project “DREAMS”; in Mozam-
school director, and a psychologist. Volunteers are about bique with 13 local partners at least until 2019
the age of the elder students and therefore have easier ac- (www.pepfar.gov/documents/organization/249176.pdf).
12Carlos from the education district administration
visits a school’s health corner, which is managed
by the health administration.
Testimony
Carlos
For healthier youth:
cooperation of schools,
nurses and community
“C antinhos are a big phies of women who fight against neficiaries receive a backpack, pens,
challenge”, says Helder. “There is gender inequality and violence. The and notebooks. This is supposed to
simply not enough space”. The nurses could also support the motivate the parents to send their
personnel of the provincial education schools’ focal points and social assis- children back to school.
administration are responsible for tants, who are there to support the
health at schools, including HIV pre- teachers in terms of HIV prevention The distribution of the school mate-
vention (Saúde Escolar), as well as and mitigation. Healthier teachers – rials, as well as coordination tasks
for the coordination with the district that would probably also reduce the with local organisations and cantin-
administration and the provincial number and length of absences. hos, is recorded in reports compiled
PGB committee. “Without the sup- by Helder and Carlos. The report
port of individual organisations, The idea to integrate HIV or health contains everything that has to do
we would hardly be able to imple- subjects in the school curricula has with youth or education, and is inten-
ment the Program GeraçãoBIZ,” been discussed for a number of ded to be transferred to the provincial
adds Carlos, responsible at district years already. However, a final deci- administration. Additionally, Helder
level for education, youth and sports. sion has yet to be reached. There is meets with his counterparts in the pu-
There are volunteers to coordinate, a Pacote Básico, the basic package: blic health sector – sometimes infor-
decisions to make regarding the lo- a book, some brochures, and maybe mally, sometimes in official meetings.
cation of new cantinhos, and schools some flyers informing about HIV pre- Topics are the management of the
to advise on how to cooperate with vention and mitigation. Most schools volunteers, who may be exempt from
the cantinhos’ nurses. are said to have received the basic school or university fees, or enjoy
package, some of them may use the priority in selection processes for pu-
But the administration staff are al- material. This year, Carlos had just blic service vacancies.
ready thinking ahead. Wouldn’t it be 23 sets to distribute for one hundred
great, if the nurses in the schools schools that requested one. “We report what we consider rele-
also provided advice to the teachers? vant to the Program GeraçãoBIZ
The aim would be for teachers to feel Carlos also participates in the distri- committee,” confirm Carlos and Hel-
more confident to integrate health is- bution of school material to poor pu- der. The activities are discussed du-
sues into the lessons: multiplying pils. Most of them already dropped ring trimestral meetings of the
condoms in math; discussing the be- out of school in order to help at provincial GeraçãoBIZ committee
ginning of HIV in history lessons. In home. The beneficiaries are chosen and may find their way to the national
language lessons there may be by local community leaders. During level via reporting of the ministries’,
space for stories about famous peo- the half-day event, which includes GeraçãoBIZ, and the partner organi-
ple living with HIV, and for the biogra- speeches and TV interviews, the be- sations.
13Good Practice
School Approach
Nurses are specially trained
to counsel youth.
Cantinhos’ empty fridges
M ost cantinhos are equipped with a refrigerator. The little
cube with a glass door usually stands on one of the metal
chairs in the room where nurses provide advice to students
on sexual and reproductive health. The refrigerator is always
empty.
It was intended to be filled with several health and HIV tests. leader, would be the ideal institution to convince the parents
However, schools are prohibited from providing HIV tests. of the importance of this measure, once the health ministry
The public administration is concerned about the reaction approves health tests being conducted in schools.
from parents. Would they protest? Would they tell their chil-
dren not to go to school anymore? Therefore, the schools’
nurses refer students to health facilities if they believe a The discussion regarding the availability of HIV testing in
health test is appropriate. After leaving the cantinho, some schools, performed by the specifically trained nurses, be-
of the students may choose not to came more important again during the
take the test. They may have deve- field mission for the ESA initiative in
loped confidence and trust in the Mozambique. Some individuals in the
school nurse, but she would not be education and health ministries are in
there when they receive their result favour of allowing HIV testing in
in a health centre or SAAJ. schools. However, official approval is
still needed from the ministries.
In the first quarter of 2018, the pu-
blic discussion was relaunched:
some administrators in the educa-
tion ministry are now in favour of
permitting HIV testing in schools.
This will likely require a consulta-
tion process with parents to obtain
their consent. Probably the school
councils, composed of teachers Youth health facilities are equipped
and parents and sometimes a local with new furniture.
14When boys ask for condoms, the
cantinho nurse starts talking to
Testimony them about family planning and
Maria Rosa Olinda responsibility.
“Most of the visitors
are boys”
M aria Rosa’s work day
starts about seven o’clock in the mor-
ning. At this time, the young nurse the uterus, or that the
opens the door to her cantinho. Only free public condoms
a few months ago, this small room are of bad quality.
was a storage room. Now, a plaque The topics are similar with female pu- to zero”, says the female director of
outside the room states “Cantinho” – pils. the school. In 2016, before there was
the school’s health corner. “Some- a cantinho, more than twenty young
times more than hundred students “It is harder to make girls visit the women aged between 14 and 18 had
come through each day”, she says. cantinho”, observed Olinda. They left school before their final exam.
“It wouldn’t be so many, if there are afraid of being laughed at by their Most of them have since returned
weren’t the mentoras”, Maria Rosa classmates, “and they are asha- after being visited by a mentora.
adds. 3,552 students are registered med to talk to a respected person,
at this school in the suburbs of Zam- such as a nurse.” This is despite the If Maria Rosa considers it necessary,
bezia’s capital Quelimane. “Mento- fact that Maria Rosa is only a few she refers students to the nearest
ras” are female youths who actively years older than the senior students. SAAJ, or arranges a meeting with the
seek contact with the students, to psychologist. “It would be impor-
motivate them to visit the cantinhos. Four mentoras volunteer at this tant for us to be able to do HIV
Olinda is one of them: “Just a few school. They are trained peer-educa- tests at the school”, she says, and
years ago, I was also a student tors. During the morning gathering, or the school director agrees. She also
here.” when teachers are absent or late, would like to cooperate more with the
they explain different aspects of school’s HIV Focal Person to find a
“Most of our visitors are boys”, sexual and reproductive health, gen- way to integrate health and HIV
observed Maria Rosa, they ask for der-based violence, or family plan- knowledge in school lessons. But her
condoms. In March 2018 alone she ning to the classes. “There is time is limited. Since the volunteers
distributed 4,000 male and 50 female always someone approaching us motivate the students to use the can-
condoms. But before she gives them after the presentation”, says tinho, there are only very few mo-
some, she starts a discussion. She Olinda. That’s how they can initiate ments when the cantiho is empty.
tries to get them talking about sexua- regular contact with the students.
lity, family planning, STIs, HIV and They can follow up their concerns Maria Rosa is employed by an inter-
other related topics. She asks them and refer them to the cantinho. Ge- national organisation. Her contract is
to show, using a wooden penis neral issues are also discussed with limited to approximately two years.
model, that they know how to use a the school directorate. “Since ha- Her training and the training of the
condom correctly. Lots of myths also ving a cantinho, the number of volunteers is implemented by an or-
have to be debunked, such as the school drop-outs due to unwanted ganisation from the USA.
beliefs that contraception will burn pregnancy has decreased almost
15Good Practice
School Approach
Program raparigaBIZ:
girls learn and discuss
about family planning
and their rights in safe
spaces.
Girls for Girls
T he raparigaBIZ approach seeks to create safe spaces for
female adolescents. Boys and men are excluded in order
that the young women feel free to talk about their doubts
and wishes, their fears and hopes. These opportunities for
exchange help them to understand that they are not alone
with their questions. They seek answers and advise each
other with the help of trained female volunteer mentors.
They discuss their parents’ and aunties’ perceptions of fe-
mininity, expectations of boyfriends and male family mem-
bers, and take more control over their lives. They feel safer The strength of the approach is also its weakness: The ra-
as a community. Many of these young women learn to parigaBIZ approach targets girls and young women. It is not
speak out, to articulate what they expect and what they for boys or young men. Although girls and young women are
want. They learn what sexual harassment is, and that they learning that early pregnancy and dependency on men limit
can denounce it. They learn to ask questions confidently, their personal freedom, the effectiveness of this program
with their head raised and their may be limited as long as men
eyes directed to the teacher or consider that these women are
other respected-person in front of breaking long-standing “traditions”.
them.
RaparigaBIZ is financed by the There are some other gender-
Swedish government and is im- mixed volunteer networks focus-
plemented by several local and sing on youth health. These can be
national NGOs under the um- seen as a first step in the right di-
brella of the youth organisations rection.
network Coalizão, for example in
Zambezia province. Its aim is the
“full realisation of sexual and re-
productive rights of girls and During this field mission, the issue
young women through empower- was raised and some PGB stake-
ment for informed choices and holders are now aware that there
provision of access to SRH ser- is a need for a boys program – let’s
vices”. In Zambezia, the project call it rapazBIZ – to strengthen
has reached about 4,900 girls equal opportunity.
aged between 10 and 24 years
old since its beginning in 2016.
Girls aged between 10 and 14
years old are its largest cohort.
16Lídia coordinates young
girl volunteers.
Testimony
Lídia
Leading the girl volunteers
L ídia coordinates 300 girl Each mentor
volunteers. 135 of them are active meets every Sa-
mentors, the others are waiting for turday and Sunday with their group water, or at least receive some-
their initial training. The 19-year-old of up to thirty girls and young women. thing to eat, instead of just atten-
is in the 11th class. She supports the They are between 11 and 19 years ding our meetings.” But slowly, also
selection and training of the volun- old, mostly around 16. They talk the parents are seeing the advan-
teers from several schools around about what they learned about them- tages of the meetings.
Mocuba, a small city in Mozam- selves, as well as family incidents: for
bique’s central region. example about the uncle who always “I don’t even want to tell what I did
gives compliments to his niece; on the weekends in the past”, says
Until two years ago, she was a volun- about their boyfriends expecting one of Lídia’s mentors. Night-life, al-
teer in Hulene, a township close to them to get pregnant; or the com- cohol and young men promising ex-
the airport in Mozambique’s capital ments of teachers, who expect pensive presents were their escapes
Maputo. In 2016 she moved to her sexual favours in return for good from everyday life – bringing some
brother’s apartment in Mocuba. A few grades. They learn to speak-out and hope for a better future, or at least
months later, a flyer circulated calling how to solve difficult situations. The some pleasure. Today they know
for participants in the raparigaBIZ mentors also visit families and try to more clearly what they want – and
movement. She applied, like hun- convince parents of the advantages fight for their dreams against old-
dreds of other youth. She was selec- of young women finishing school and fashioned rules and perceptions.
ted and soon became a coordinator. further education, as well as avoiding Lídia is their role model, self-confi-
early marriage and pregnancies. dent, taking care of herself without
Every month she meets her girl vo- Those needing more help, are refer- being in conflict with her family, going
lunteers to train and advise them on red to the nearest youth health facility to school, and leading so many vo-
becoming a mentor for other girls. (SAAJ). lunteers.
She imparts her knowledge of ado-
lescent reproductive health, youth “When we invite girls to our advo-
rights, contraception and family plan- cacy sessions, parents often ask:
ning. The girl mentors take that ‘What will she bring back for
knowledge to their communities. us?’”, says Lídia. “They believe it
They motivate girls to join in and dis- would be better for the girls to
cuss. help in the household, to fetch
17Good Practice
School Approach
Volunteers support young mothers,
and convince them to
return to school.
Young mothers back at school
“W e have brought eight girls back to school this approach”, where training sessions are used to sensitise
participants on healthy and good social behaviour.
year”, says Célia happily. These young women aged bet-
ween 15 and 17 were pregnant – “some from teachers,
some from their community”. They had left school when
they found out that they were pregnant. Regularly, the volunteers visit neighbouring communities.
They perform improvised plays and hold small discussions.
Through such gatherings they get into contact with other
Célia is one of the more than twenty school girls and boys youth and identify those who may have personal difficulties
who joined the Namagoa Secondary School Youth Club. A and/or have left school too early. The volunteers will then
third of them have already received some training and are visit them and offer basic counselling, sometimes together
passing their newly gained knowledge on to their peers: fa- with the parents. Through their activities in the communities,
mily planning is the most talked about subject, but also ha- they are also able to build trust with young women who had
rassment and abuse, health prevention, as well as “rights dropped out of school in the previous year and encourage
and duties of children”. Some of the school club members them to return. The husband of one young mother was
visit school during the morning, others in the afternoon, be- strictly against the idea that she could return to school. He
cause in Mozambique school is organised in shifts. “That’s believed she would be better off to take care of the house-
how we reach pupils in both groups.” hold. In the end, the 17-year-old left him.
The club is supported by a local NGO named RESA. The “Unfortunately, there is no youth health centre around
local community leader is also involved in the project. The here”, laments Célia. And the nearest normal health centre
school club members can count on his support when they is still far away. “We would like to distribute condoms,
implement their activities in the communities. This is be- but there are never enough,” Célia continues. The geo-
cause he is also the president of the school council and pre- graphical isolation makes it difficult to refer youth to health
sident of the co-management committee of the local health services or to get there regularly to obtain condoms. Howe-
facility. The coordinator of the club is the sports teacher, who ver, the school club volunteers continue advocacy in the
is also the school’s HIV Focal Person. The young male tea- communities, seeking to bring young mothers back to
cher started a football club with the volunteers. He applies school.
elements similar to the “youth development through sports
18Teachers may be reprimanded
for sexual abuse.
Testimony
Josina
Favours for good marks
J osina* cries. She was
late for the Portuguese language
test. The teacher still let her partici-
pate, but gave her a bad grade. Du-
ring a moment when he was alone
with her he said: “How can I sup- For the harassed girls, the mentor would be “culturally inappropriate”.
port your promotion to the next volunteers and cantinho nurses are However, they let the story circulate.
[school] year, if you don’t want to extremely important. They may not Without any direct talk between the
be with me?”** Ashamed, Josina be able to take action against the tea- students and the director, the director
tells her closest friends about the chers, but at least they advise the summons Josina’s teacher and ad-
threat. One of them is a volunteer girls on how to tackle the situation monishes him. A few days later, the
mentor. She advises her to not follow and how to reject such men. The girls school council convened a meeting
the teacher’s demand. learn that no man, teacher or not, has to discuss the matter and publicly re-
any right to claim favours. This primand the teacher. Josina receives
Many teachers are young, about contrasts with the beliefs of many pa- a better test result and will be promo-
twenty years old, when they start rents and students, who still consider ted to the next year. But she will still
their career. In remote areas, they such behaviour as inevitable, some- have to continue lessons with that
are the most respected person with a thing that can’t easily be changed. A teacher…
regular salary. At the same time, they majority of men as well as women
are a stranger, since they are often also believe that short skirts are an
transferred from other provinces. invitation for sexual advances.
Despite the law and the teacher’s
union code of conduct prohibiting There is only one female teacher at
sexual relations between teacher and Josina’s school, the other twenty are
student, teachers demand favours men. The female teacher is known as
from female students again and rigorous and distanced, usually lea-
again. Consequences are rare. ving the school quickly after her les-
There may be some small note in the sons. Today she is not at school.
personnel record, or a teacher might
get transferred to another school. The school director sits under a tree
Some administration staff say they beside his office together with some
prefer to educate the teacher, instead teachers. None of the girls nor the * not real name
of demotivating them through punish- volunteer mentor dare to mention the ** in Mozambican Portuguese:
ment. incident. They consider that doing so “…namorar comigo”
19Good Practice
Clinical Approach
Girls accompanied by a mentor-
volunteer have priority access
to youth health facilities.
SAAJ — the safe health alternative
444 is the number of SAAJ in Mozambique. In Zambe-
zia province, about 55 SAAJ offer their services for youth
aged up to about 24 years. SAAJ stands for Youth Friendly
Health Services, which are specialised units in health faci-
lities. SAAJ offer health services ranging from counselling
to health tests. In case of positive results, the patient com-
mences treatment immediately – irrespective of whether it
is a sexually transmitted disease, malaria, or diabetes. The
basic concept is to offer services for youth in a separate
space, usually in the backyard of a health facility. This ap-
proach reduces waiting times for the target group, and uti-
lises specially trained staff. It also reduces fear of being
seen by other, often older, relatives or neighbours. There-
fore, the inauguration or rehabilitation of a SAAJ itself, can
be considered a good practice, as this facilitates the use of These partners generally rehabilitate and equip SAAJ
medical services by youth. rooms, with PEPFAR funds. The Mozambican Association
for Family Development (AMODEFA) is the only organisa-
tion that provides a privately run specific SAAJ in Zambezia
There are two types of SAAJ: specific and alternative. While province.
the specific SAAJ is an independent physical ward in a
health facility, the alternative SAAJ may refer to just a room,
or the availability of specifically trained staff during opening The SAAJ provide youth with improved access to adoles-
hours within the health facility building. Currently, there are cent-oriented health information and care, especially in re-
some alternative SAAJ being upgraded and equipped to be- gard to sexual and reproductive health. There are many
come specific SAAJ. examples that demonstrate that the existence of the cantin-
hos (school health corners) strengthen the demand for and
existence of SAAJ.
This clinical approach is implemented by the health sector
with the support of four partners: Friends in Global Health
(FGH); International Center for AIDS Care and Treatment
Program (ICAP); and Family Health International (FHI 360).
20Nurse Digna explains
monitoring forms.
Testimony
Digna
SAAJ in action
D igna smiles when she only 24 years old,” she
talks. Her questions are focused and won’t question them, Digna
direct. When she listens, she holds confides with a twinkle in
the gaze of the person speaking. Be- her eye. “Young women are much have to wait. An old poster warning
fore answering a question, she re- more likely than men to come to against tuberculosis is peeling off the
peats it to make sure she understood the SAAJ”, Digna continues. Most of main door.
correctly. She has been working as a them heard about family planning
nurse, mostly with youth, for around and come wanting to know more SAAJ-visitors who only ask for coun-
thirty years. About three years ago about it, and what contraception op- selling are not even counted. Digna
Digna became responsible for two tions there are. Among the young records only the patients who ask for
youth health facilities, called SAAJ, in women seeking advice are those contraception, who receive tests, or
a small district almost 150 kilometres who work during the weekends who are ill. In case of positive results,
north of Quelimane. More than one around the small bars, right in front of the patient commences treatment im-
hundred 12 to 24 year olds pass by the health centre. They come be- mediately irrespective of whether it is
here every day. “Actually, we cause of STIs and ask for condoms a sexually transmitted disease, ma-
should open the SAAJ every day – “If they actually use the laria or blood pressure. Drugs and
until 7 pm, not just until 3 pm,” she condoms, I don’t know”, says test kits are always available. There
says. “That’s too early for many Digna. are only shortages of Salferoso, used
school students.” But the public to treat anaemia, from time to time.
system cannot pay for the extra Her small SAAJ consists of a desk, Digna records the patients in a list,
hours, nor can the U.S. American on it a stack of papers and some disaggregated by gender and age.
university, which contributed equip- condom bulk-packs, there are four These lists are the SAAJ’s reports,
ment to the youth health facility. simple chairs, a small empty refrige- collected in large folders. Up until one
rator for medicines, a locker, and two year ago, the only person who ever
The youth come individually or in rubbish bins. No computer, no tablet. came to collect the lists, was so-
groups of five to ten. “Last Monday, The white-washed walls show traces meone from the international organi-
a group of 15 girls came here,” of people who have leaned on it. The sation that funded the SAAJ
Digna reports. “They wanted to door of the three by seven-meter equipment. What they do with the
know what sexually transmitted room leads directly outside to the hot monitoring papers – nobody in the
diseases are.” Teachers frequently sun. This is where the young women administration knows. Nowadays,
send students to the SAAJ to wait. Those wanting to go to the main since Clotilde has been working in
research various health topics. clinic need to go around the building the provincial health administration,
and through a narrow corridor, with Digna uses WhatsApp to send pho-
The SAAJ is limited to youth up to the similar basic treatment rooms on tographs of the monitoring lists. The
age of 24 years to keep waiting times both sides. On every door hangs an provincial health administration then
short. Although “some come here A4-sized printed document announ- has to transfer the data into Excel
with three babies and say they are cing that coughing patients do not sheets.
21Good Practice
Clinical Approach
Some SAAJ only provide limited
space for nurses, administration
and examination.
Testimony
Feliciana
Schools revitalise
Youth Health Facilities
mentors
“O
come from a
ur SAAJ was revita- school, ac-
lised because of the cantinhos”, companying
says Feliciana. “It practically did a girl”,
not exist anymore.” Since nurses usually urgent cases. The SAAJ friends, who do not consider it ne-
started working in schools counsel- and the cantinhos have agreed that cessary for young, healthy people to
ling the students and referring them priority will be given to mentor-ac- attend health facilities. They may
for services, many more youth have companied young women. Every trigger rumours about their “bad
been taking advantage of the youth month Feliciana meets with nurses health state” which may then lead to
friendly health service in Coalane’s who work in school cantinhos. They discrimination.
health centre. exchange observations and discuss
Sometimes young women them-
important issues, such as how they
Feliciana worked for several years selves do not know what exactly to
can convince the young girls to
in the main patient reception. Youth expect from their visit to the SAAJ.
avoid early pregnancies.
had to wait there as long as any- “Often we have to convince the
body else. From 2016 more and mothers how important it is that
Most visitors are young women,
more adolescents started to come, their daughters come to the
many of them seeking information
sent from the cantinhos in the near- SAAJ and receive advice regar-
about menstruation, family planning
by schools. That’s how she was ding reproductive health”, says
advice and methods. Others are
able to convince the directors – and Miranda, Feliciana’s colleague. It is
pregnant, and many of them come
those higher up– to provide a dedi- important to delay the age at which
with their babies. “15 minutes are
cated space for a specific SAAJ. girls have their first sexual relations-
not enough for most of the
hip in order to avoid early pregnan-
cases”, states Feliciana.
“Most people come in the mor- cies.
ning”, says Feliciana and points to Young men come usually around
the terrace in front of the SAAJ’s midday or in the early afternoon. During the afternoon the visitor
entry. There is space for about fifty They mostly come for HIV tests. numbers reduce. Feliciana uses the
visitors to wait. Others have sought This gives hope for a behaviour time to prepare reports. Her col-
a shady place under the trees bet- shift: traditionally men avoid HIV leagues count the vouchers, often
ween the one-storey-buildings. Be- tests, while women are tested as called referral slips: adolescents
hind the door of the SAAJ stands an part of pre-natal care. This often who were referred from schools
old table, covered with registration causes conflicts at home when a usually bring a kind of referral vou-
forms. Blood samples are taken pregnant woman receives a positive cher. The SAAJ nurses sign a copy,
here before meeting the doctor in test result, but the man continues to which the student should return to
the room behind. The room of less consider himself HIV negative. the school’s nurse. Another is used
than twenty square meters contains by the SAAJ for record keeping. Fe-
a folding privacy screen, a kind of a Many of young women feel asha- liciana completes the list, which she
stretcher, another large table, a few med to be seen in a health centre. will bring to the district health admi-
chairs, and a tiny wooden bench. They worry that aunts, other family nistration. In her case, that’s not far.
Two nurses work here with the doc- members, or neighbours may see If the photocopy machine works,
tor; one to two patients may be them. They are afraid of uncomfor- Feliciana will also keep a copy for
handled at a time. “Sometimes table questioning by relatives or the hospital’s reporting.
22You can also read