Development of live attenuated pediatric RSV vaccines
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Development of live attenuated pediatric
RSV vaccines
Laboratory of Infectious Diseases, NIAID, NIH
(Ursula Buchholz, Peter Collins)
Center for Immunization Research, JHU
(Ruth Karron)
Infant with RSV disease
Division of Clinical Research, NIAID, NIH
IMPAACT, NIAID and NICHD, NIH
(Betsy McFarland, Coleen Cunningham)
MedImmuneWhy a live RSV vaccine?
• Needle-free, adjuvant-free; a single dose is substantially immunogenic
• Broad stimulation of innate, cellular, humoral immunity
• Direct stimulation of respiratory tract immmunity
• Attenuated RSV strains provide all of the viral antigens
• IN immunization avoids immune suppression by maternal antibodies
• Live vaccines induce broader, more effective immunity than subunits in
virus-naïve recipients (e.g. influenza vaccines)
★ Killed and subunit RSV vaccines prime for enhanced RSV disease in
RSV-naïve recipientsWhy a live RSV vaccine?
• Needle-free, adjuvant-free; a single dose is substantially immunogenic
• Broad stimulation of innate, cellular, humoral immunity
• Direct stimulation of respiratory tract immmunity
• Attenuated RSV strains provide all of the viral antigens
• IN immunization avoids immune suppression by maternal antibodies
• Live vaccines induce broader, more effective immunity than subunits in
virus-naïve recipients (e.g. influenza vaccines)
★ Killed and subunit RSV vaccines prime for enhanced RSV disease in
RSV-naïve recipients
Immunization of infants against RSV requires a live vaccinePlanned timing of a live RSV vaccine
1 or 2 doses beginning
Boost at 12-15 months
at 4 or 6 months
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 age
(months)
The present study examines a single, primary immunization,
evaluated in RSV-seronegative infants 6-24 months of agePhase I clinical studies of live RSV vaccines:
Stepwise evaluation in increasingly vulnerable populations
Adults (unscreened), n = ~10-15
RSV Seropositive Children 15-60 Months, n = ~15 (V:P = 2:1)
Present * RSV Seronegative Children 6-24 Months, n = ~30 to 51
population:
(V:P = 2:1)
* Testing in naïve recipients is restricted to April-OctoberThree key study objectives:
1. Tolerability/reactogenicity: Frequency of vaccine-related solicited events
Studies are conducted in the RSV off-season (April 1to mid-October)
Findings can be obscured by background respiratory infections,
even in the off-season
2. Magnitude of vaccine virus replication: Measure the amount of vaccine virus shed
This gives a second, more quantifiable measure of attenuation
In initial phase I studies, this necessitates extensive nasal wash sampling;
subsequent studies have less sampling
Virus recovery is complicated by the labile nature of RSV
We historically use plaque titration, and are introducing qPCR to measure replication
3. Immune response to RSV: Quantify the serum antibody response
ELISA antibody against RSV-F; RSV-neutralizing antibodies
Historically, nasal wash antibodies have been difficult to quantify reliably
and will not be measured
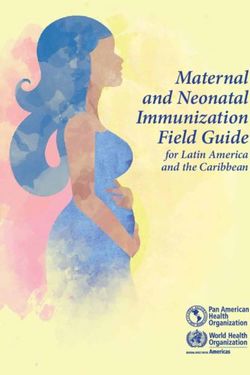
Labwork is done at the Center of Immunization Research, JHU.3 attenuated RSV vaccine candidates with different properties in clin. studies
Mutations in red are temperature sensitive
RSV cps2 NS1 NS2 N P M SH G F M2 L
cp cp cp cp cp
SH 248 1030
404
(P1114) stabilized
• Multiple point mutations + 1 gene deletion = 5 independent attenuating loci
• Highly temperature sensitive, provides further restriction in LRT
• Tendency for some of the population to lose 1 attenuating locus
RSV ∆NS2/ NS1 NS2 N P M SH G F M2 L
∆1313/
NS2
I1314L ∆1313 I1314L
• Deletion of IFN antagonist may provide increased immunogenicity
(CIR-288) • Deletion L residue 1313 confers a moderate ts phenotype
• Expect gene deletion to be highly stable
RSV ∆M2-2 NS1 NS2 N P M SH G F M2 L
• Deletion of RNA regulatory protein:
RSV LID M2-2: Increased antigen expression may increase immunogenicity
IMPAACT • Expect gene deletion to be highly stable
2000 • Not temperature sensitive
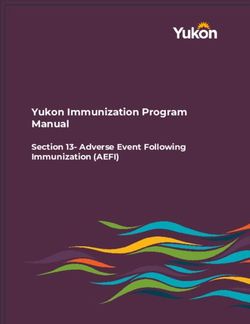
• We are evaluating two slightly different versions: RSV MEDI-∆M2-2 and RSV LID-∆M2-2Lead live-attenuated RSV strains under clinical evaluation
2013 2014 2015/2016
RSV cps2 P1114 Projected studies:
seroneg. 6‐24 mo
1. Expanded study with
lead
RSV MEDI ∆M2‐2 CIR RSV LID ∆M2‐2 candidate identified from
IMPAACT 2000 the 2013/2014 studies
seroneg. 6‐24 mo
seroneg. 6‐24 mo
2. Modified RSV candidate
3. Bovine/human PIV3
RSV ∆NS2∆1313 CIR RSV ∆NS2∆1313 CIR vector expressing RSV F
seropos. 12‐59 mo seroneg. 6‐24 moSummary Immunization of infants requires a live RSV vaccine. Several candidates are being evaluated. This is because they may differ in (i) attenuation and tolerability, (ii) immunogenicity, and (iii) stability. This is assessed in small numbers of infants and children, which is challenging. RSV is a labile virus, and considerable care is needed in preparing vaccine and in processing nasal washes. We hope to have information on 3 different candidates by the end of 2014. This may identify a lead candidate that will be taken to a larger study in 2015/2016.
Summary
Immunization of infants requires a live RSV vaccine.
Several candidates are being evaluated. This is because they may differ in
(i) attenuation and tolerability, (ii) immunogenicity, and (iii) stability.
This is assessed in small numbers of infants and children, which is challenging.
RSV is a labile virus, and considerable care is needed in preparing vaccine
and in processing nasal washes.
We hope to have information on 3 different candidates by the end of 2014.
This may identify a lead candidate that will be taken to a larger study in 2015/2016.
It also is possible that:
• We may identify a promising candidate but decide a different version
(e.g., more attenuated) should be evaluated in 2015. A number of
modified versions are being developed as back-ups.
• Some of the initial testing may be inconclusive and require further
confirmatory evaluation (e.g., to evaluate tolerability)
We also anticipate evaluating a B/HPIV3 vector expressing RSV-F in 2015.You can also read