Hospitalizations Due to Respiratory Syncytial Virus (RSV) Outside of the Typical Season
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
PEDIATRIC ALLERGY, IMMUNOLOGY, AND PULMONOLOGY ORIGINAL ARTICLE
Volume XX, Number X, 2011
ª Mary Ann Liebert, Inc.
DOI: 10.1089/ped.2011.0114
Hospitalizations Due to Respiratory Syncytial Virus (RSV)
Outside of the Typical Season
Rachel D. Quick, R.N., C.N.S.,1 Christine A. Jesser, Sc.D.,2 Anna C. Bell, M.D.,3
Marisol Fernandez, M.D.,1 Wm Brendle Glomb, M.D.,4 Bennie C. McWilliams, M.D.,4
Jennifer L. Murray, R.N., M.S.N., C.P.N.P.,5 and Sarmistha B. Hauger, M.D.1
Objective: Respiratory Syncytial Virus (RSV) is the most common cause of bronchiolitis and viral lower respi-
ratory tract infections in children. It is associated with annual winter epidemics across the United States,
typically October through April. Our objective is to describe the clinical characteristics of children hospitalized
outside the typical RSV season and to compare them with those admitted during the season.
Methods: A retrospective chart review was conducted of all patients who were hospitalized at Children’s
Hospital of Austin from May 2000 to September 2006 and had a positive RSV antigen test. Descriptive statistics,
tests of differences, and associations between patients diagnosed in the off-season versus typical season were
conducted.
Results: A total of 850 charts of RSV-positive cases were reviewed. Of these, 45 patients (5.3%) were admitted
during the off-season. The following variables were statistically significantly associated with diagnosis in the off-
season versus typical season: mean birth weight (2704 g vs. 3204 g respectively, p = 0.0001); gestational age at
birth less than 36 weeks (OR = 4.35; 95% CI: 2.2, 8.6); history of neonatal intensive care unit (NICU) admission at
birth (OR = 6.04; 95% CI: 2.9, 12.5); and multiple birth (OR = 3.38; 95% CI: 1.2, 9.2).
Conclusions: Infants with RSV infection outside of the typical season were more likely to have been premature,
of lower birth weight, the products of multiple births, and admitted to the NICU at birth.
Introduction Methods and Materials
Patients
R espiratory Syncytial Virus (RSV) is the most common
cause of bronchiolitis and viral lower respiratory tract
infections in children. It accounts for approximately 91,000
Charts for 850 patients hospitalized at Children’s Hospital
of Austin between May 2000 and September 2006 for labo-
hospitalizations and 500 deaths of infants and children each ratory-confirmed RSV infection were included in the study.
year in the United States.1,2 The risk of severe RSV illness is
highest among children who are premature or have underlying Study design
medical disorders. It is associated with annual winter epidemics
across the nation, typically October through April (hereafter, A retrospective chart review was performed on all RSV-
‘‘typical season’’). In temperate climates, this infection can per- related hospital admissions that occurred at Children’s
sist and spread year-round. Little data are available about the Hospital of Austin from May 2000 to September 2006. The
nature of RSV illness that occurs during the summer months. study was approved by the Austin Multi-Institutional Re-
Our institution observed a portion of all RSV-related ad- view Board. RSV hospitalizations were identified using dis-
missions to occur between May and September, usually charge diagnosis, in addition to laboratory records of a
considered to be the off-season. Our objective is to describe positive RSV test. Codes established by the International
the clinical characteristics of children hospitalized during the Classification of Diseases, Ninth Revision (ICD-9) were used
typical RSV season and to compare them to those admitted for discharge diagnoses, which included RSV bronchiolitis
in the off-season. (466.11), RSV pneumonia (480.1), and RSV unspecified
1
Pediatric Infectious Diseases, Dell Children’s Medical Center, Seton Family of Hospitals, Austin, Texas.
2
Office of Research Administration, Seton Healthcare Family, Austin, Texas.
3
Children’s Medical Group, Austin, Texas.
4
Austin Children’s Chest Associates, Dell Children’s Medical Center, Austin, Texas.
5
Comfort, Pain, and Palliative Care Program, Children’s Hospital Los Angeles, Los Angeles, California.
12 QUICK ET AL.
(079.6). Only patients with confirmed RSV tests were in- 16
cluded in the study.
RSV testing was done by either enzyme immunoassay 14
(EIA) or by culture. Our laboratory utilized the Kallestad 12
Pathfinder EIA (Sanofi Diagnostics Pasteur Inc, Chaska, MN)
and the Directigen EIA (Becton Dickinson Microbiology 10
Systems, Cockeysville, MD) kits during the study period.
8
Data collection forms were utilized that included demo-
graphic information in addition to hospitalization data. De- 6
mographic information included gender, race, gestational
age at birth, chronologic age, NICU admission at birth, birth 4
weight, multiple versus singleton birth, and status of RSV
2
prophylaxis (Palivizumab). Information regarding RSV hos-
pitalization included admission date, discharge date, ad- 0
mission less than 24 hours, RSV test performed, test type, test May June July August September
result, date of test, discharge diagnoses, outcome of death,
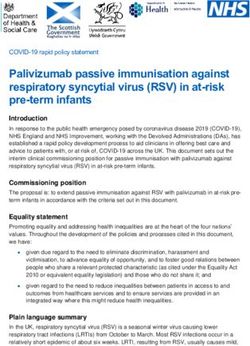
greatest absolute lymphocyte count, oxygen requirement, FIG. 1. Off-season distribution of RSV-confirmed hospital-
izations at Children’s Hospital of Austin, May 2000 to Sep-
ICU admission for a respiratory condition, and duration of
tember 2006, total count by month of admission. RSV,
ICU stay. respiratory syncytial virus.
Study end points
There were two deaths, both with a history of a NICU
This study aimed to describe the population of children in admission and comorbidities. One patient was admitted
Central Texas hospitalized with RSV according to personal during the off-season, had received prophylaxis during the
and hospitalization characteristics. Furthermore, this study previous RSV season, and the primary cause of death was
was performed to compare characteristics of patients ad- identified as respiratory failure. The other patient was ad-
mitted during the typical season to those admitted in the off- mitted in January, did not receive prophylaxis, and the pri-
season. mary cause of death was multiple organ failure.
Statistical analysis Off-season patient characteristics
Patient and clinical characteristics were summarized and A total of 45 (5.3%) patients were admitted during the
presented by season of diagnosis for 850 patients who met off-season. There was no difference noted for patient gender
study inclusion criteria. Comparison of patient characteris- or race when comparing the two seasons. Patients admitted
tics by season were performed using t-tests for equality of during the off-season tended to be of younger gestational
means, chi-square tests for categorical variables, Poisson re- age; 33% were 36 weeks gestational age or less compared to
gression to compare number of admissions by year, and lo- 10% during the typical season. There was a statistically
gistic regression to examine the association of patient significant difference (chi-square, p < 0.001) between the
characteristics with season of diagnosis. distribution of gestational age categories by season of di-
agnosis. Gestational age categories included babies born at
less than 32 weeks gestation, between 32 and 36 weeks,
Results and more than 36 weeks. During the off-season, 22.2% of
Patient characteristics admissions were born at less than 32 weeks gestation
Most patients admitted were aged less than 6 months
12
(53% off-season versus 62% typical season). The majority
(n = 637) were term infants (i.e., ‡ 36 weeks gestation). Ad-
missions occurred in each month of the off-season through- 10
out the study period with the greatest number of cases (31%
of off-season admissions) occurring in September, as shown 8
Number of cases
in Figure 1. Although the number of admissions in the off-
season varied from year to year from 3 to 10 admissions, 6
cases occurred without statistically significant differences in
incidence each year (Fig. 2). Additional characteristics of the 4
patient population are described in Table 1.
2
Hospitalization characteristics
0
A full admission ( ‡ 24 hours) was required for 786
2000 2001 2002 2003 2004 2005 2006
(92.5%) patients. The primary reasons for hospitalization
Year
were cough and respiratory distress (Table 1). Categorical
observed characteristics of the hospital course due to RSV FIG. 2. Off-season distribution of RSV-confirmed hospital-
illness are listed in Table 1. An ICU admission was needed izations at Children’s Hospital of Austin, May 2000 to Sep-
for 79 (9.3%) patients. tember 2006, total count by year of admission.RSV OUTSIDE THE TYPICAL SEASON 3
Table 1. Patient Demographics of RSV-Confirmed Hospitalizations
at Children’s Hospital of Austin, May 2000 to September 2006
Total n (%) Typical season n (%) Off-season n (%) p-value
Sex 0.43
Male 486 (57.2) 462 (57.4) 24 (53.3)
Female 344 (40.5) 323 (40.1) 21 (46.7)
Missing/Unknown 20 (2.4) 20 (2.5) 0 (0)
Gestational Age < 0.001
0 to < 32 weeks 47 (5.5) 37 (4.6) 10 (22.2)
32–35 weeks 49 (5.8) 44 (5.5) 5 (11.1)
> 36 weeks 637 (74.9) 611 (75.9) 26 (57.8)
Missing/Unknown 117 (13.8) 113 (14.0) 4 (8.9)
Race/Ethnicity 0.85
Hispanic 364 (42.8) 343 (42.6) 21 (46.7)
Caucasian 271 (31.9) 259 (32.2) 12 (26.7)
African American 62 (7.3) 59 (7.3) 3 (6.7)
Other Race 134 (15.8) 125 (15.5) 9 (20.0)
Missing/Unknown 19 (2.2) 19 (2.4) 0 (0)
NICU* admission < 0.001
No 554 (65.2) 539 (67.0) 15 (33.3)
Yes 118 (13.9) 101(12.5) 17 (37.8)
Unknown 178 (20.9) 165 (20.5) 13 (28.8)
Prior prophylaxis 0.14
No 745 (87.6) 709 (88.1) 36 (80.0)
Yes 25 (2.9) 24 (3.0) 1 (2.2)
Unknown 80 (9.4) 72 (8.9) 8 (17.8)
Comorbidities (Yes)
Asthma 50 (5.9) 45 (5.6) 5 (11.1) 0.85
Congenital Heart Disease 40 (4.7) 36 (4.5) 4 (8.9) 0.06
Chronic Lung Disease 20 (2.4) 16 (2.0) 4 (8.9) 0.01
Down syndrome 15 (1.8) 13 (1.6) 2 (4.4) 0.28
Cerebral palsy 3 (0.4) 3(0.4) 0 (0) 0.67
History of pneumonia 41 (4.8) 37 (4.6) 4 (8.9) 0.20
History of RAD** 17 (2.0) 16 (2.0) 1 (2.2) 0.58
Risk factors for RSV hospitalization (Yes)
Breastfed (current or previous) 259 (30.5) 268 (33.3) 11 (24.4) 0.45
Exposure to tobacco 163 (19.2) 155 (19.3) 8 (17.8) 0.60
Daycare 131 (15.4) 124 (15.4) 7 (15.6) 0.98
Discharge Diagnosis (Yes)
RSV Bronchiolitis 723 (85.0) 693 (86.1) 30 (66.7) 0.001
RSV pneumonia 49 (5.8) 45 (5.6) 4 (8.9) 0.56
RSV other 74 (8.7) 67 (8.3) 7 (15.6) 0.23
Primary reason(s) for RSV hospitalization (Yes)
Cough 670 (78.8) 641 (79.6) 29 (64.4) 0.001
Respiratory distress 598 (70.4) 565 (70.2) 33 (73.3) 0.05
Fever 475 (55.9) 449 (55.8) 26 (57.8) 0.31
Wheezing 399 (46.9) 380 (47.2) 19 (42.2) 0.28
Hypoxemia 341 (40.1) 323 (40.1) 18 (40.0) 0.78
Dehydration 204 (24.0) 192 (23.9) 12 (26.7) 0.007
Apnea 72 (8.5) 64 (8.0) 8 (17.8) 0.007
Characteristics of hospital course
Oxygen requirement 475 (55.9) 454 (56.4) 21 (46.67) 0.11
Positive chest x-ray*** 292 (34.4) 280 (34.8) 12 (26.7) 0.08
< 24-hour admission 247 (29.1) 234 (29.1) 13 (28.9) 0.84
ICU admission 79 (9.3) 73 (9.1) 6 (13.3) 0.42
Mechanical ventilation 28 (3.3) 24 (3.0) 4 (8.9) 0.05
Outcome of death 2 (0.2) 1 (0.1) 1 (2.2) 0.009
RSV, respiratory syncytial virus. *NICU: neonatal intensive care unit; **RAD: reactive airway disease; ***Includes findings for pneumonia
or bronchiolitis. p-value calculated using Pearson chi-square test.
compared with only 4.6% of cases in the typical season with continuous variables, between seasons is illustrated in
(Table 1). Although not statistically significant, patients Table 2. Babies who were premature ( < 36 weeks gestation
admitted during the off-season were chronologically older at birth) were 4.35 times more likely than term infants to be
upon admission; mean of 8 vs. 10 months respectively. A admitted during the off-season (95% Confidence Interval
comparison of notable patient characteristics, measured [CI]: 2.2, 8.6). Patients with a history of multiple birth were4 QUICK ET AL.
Table 2. Comparison of Off-Season Table 3. Logistic Regression of Patient
(May to September) Patient Characteristics Characteristics on Likelihood of RSV Diagnosis
to Typical Season, Children’s Hospital in the Off-Season, Children’s Hospital
of Austin, May 2000 to September 2006 of Austin from May 2000 to September 2006
Off-season Typical season Outcomes* Odds ratio
n = 45 n = 805 (n) (95% CI)
mean (SD) mean (SD) p value
Sex
Gestational age, weeks* 35.2 (4.7) 38.7 (14.2) 0.12 Male 24 1.00 (Reference)
Birth weight, grams* 2704.9 (844.7) 3204.3 (789.7) < 0.001 Female 21 1.25 (0.69, 2.29)
Hospital length 3.9 (6.4) 3.0 (4.7) 0.26 Race/ethnicity
of stay, days* Caucasian 12 1.00 (Reference)
ICU length of stay, 9.8 (8.2) 5.0 (5.7) 0.06 African American 3 1.10 (0.30, 4.01)
days*,** Hispanic 21 1.32 (0.64, 2.73)
Age at admission, 9.8 (12.5) 8.0 (14.7) 0.42 Other/Unknown 9 1.72 (0.70, 4.19)
months* Age category
Days on a 10.2 (8.5) 6.2 (4.6) 0.16 0 to < 3 months 16 1.00 (Reference)
ventilator*,*** 3 to < 6 months 8 1.31 (0.55, 3.13)
6 to < 12 months 8 1.3 (0.54, 3.11)
*comparison of means using t-test. **Calculated for patient 12 + months 13 1.86 (0.87, 3.96)
population admitted to ICU. ***Calculated for patient population Birth weight
requiring mechanical ventilation. 2,500 + grams 25 1.00 (Reference)
1,500 to < 2,500 grams 10 3.97 (1.82, 8.66)
0 to < 1,500 grams 5 4.50 (1.59, 12.70)
3.38 times more likely to be admitted in the off-season (95% Missing 5
CI: 1.24, 9.22; Table 3). Gestational age
A greater percentage of patients from the off-season had a 36 + weeks 26 1.00 (Reference)
history of NICU admission at birth. Patients with a history of < 36 weeks 15 4.35 (2.2, 8.56)
NICU admission were 6.05 times more likely to have been Missing 4
admitted in the off-season (95% CI: 2.9, 12.5) when compared Multiple birth
No 37 1.0 (Reference)
to those with no history of NICU admission (Table 3). Length
Yes 5 3.38 (1.24, 9.22)
of stay in the NICU was not statically significantly different Missing 3
by season. Prior prophylaxis
A statistically significant difference was found between No 36 1.0 (Reference)
the two groups for birth weight. The data were categorized Yes 1 0.82 (0.11, 6.24)
into very low birth weight, weighing less than 1,500 grams at Missing 8
birth and low birth weight babies, weighing 1,501 grams to NICU admission
less than 2,500 grams at birth. Chi-square tests showed sta- No 15 1.0 (Reference)
tistically significant differences in both groups between the Yes 17 6.05 (2.93, 12.50)
typical season and the off-season. The larger difference was Unknown 13 2.82 (1.29, 6.15)
seen in the very low birth weight group. In the off-season, *Outcome defined as RSV diagnosis during off-season.
11.1% of babies admitted had a history of birth weigh less
than 1,500 grams compared to only 3.2% in the typical-
season. Additional variables listed in Table 1 were not found
to be statistically significant.
data showed no significant difference between degrees of
Discussion illness. In Florida, Halstread et al. reported a persistent RSV
epidemic between July 1993 and December 1996.6 They
RSV infections in the United States typically occur during concluded that RSV is endemic in that region and can be
annual community outbreaks at regular, predictable inter- detected consistently during the summertime months. Simi-
vals in the late fall, winter, and early spring.3 Based on the larly, Light studied Southwest Florida over a 4-year period
definition of widespread RSV activity used by the National and found RSV detected above epidemic levels in all but 6
Respiratory and Enteric Virus Surveillance System out of the 48 months studied. RSV cases were still present
(NREVSS), RSV outbreaks are rapid in onset and last 2–5 during those 6 months, but did not reach the threshold
months. However, studies from South Texas and South- considered by the NREVSS to be epidemic.4 However, there
eastern Florida have found considerable variability in the is little data in the literature regarding these off-season ill-
RSV season from year to year.3,4 Between 1996 and 2007 in nesses.
South Texas, Fergie et al. found that only one RSV season Our goal is to compare RSV illness, which occurs dur-
lasted 16 weeks (the average duration for the southern ing the typical winter epidemics, to the illness that occurs
United States), with the median duration being 21 weeks.5 more sporadically during the off-season. Our data demon-
There are two reports from regions in the southern United strate that particular infants may be at risk for admission for
States of increased RSV illness during summertime months. RSV illness during the off-season. These infants were more
In 1992, Washburn et al. reported a 21% incidence of RSV likely to have been premature, have had low birth weights,
infection among children with respiratory symptoms during have been the products of multiple births, or have a history
the summer in Louisiana over two consecutive years.5 Their of NICU admission. Severe RSV-related respiratory illnessRSV OUTSIDE THE TYPICAL SEASON 5
was observed during the off-season in our study, including may circulate at low levels in certain geographic areas.8
the need for mechanical ventilation and prolonged ICU stay. These infants were more likely to have been premature,
Of note, among children admitted to the ICU, those admitted have had low birth weights, have been the products of
during the off-season remained in the ICU twice as long as multiple births, or have a history of NICU admission. Pe-
those admitted during the typical season. diatricians should be aware of the possibility of infection in
These results suggest that a group of children may remain at such patients who present with a consistent clinical pre-
risk for RSV infection during the off-season, at a time that the sentation.
virus is circulating at low levels. In an attempt to correlate RSV
activity in relation to geographic climate, humidity, and Acknowledgments
weather patterns, Welliver found that RSV activity is nearly
continuous throughout the year in subtropical regions with We would like to thank Carey Bush, Olivia Hauger, Re-
warm weather and high humidity.7 Our institution is in a becca Wren, and Jaquelyn Marroquin who assisted with data
geographic locale that may predispose to such activity. collection. Financial support was provided by a grant from
Weather conditions that affect the viability of the virus may also MedImmune, Inc.
explain the variability of off-season cases among the years.8
A review of the RSV testing data over 10 years has been Author Disclosure Statement
conducted to help define the variability in community RSV SBH and WG have received unrestricted grants from
season timing. During the years 1990–2000, it was observed MedImmune, Inc. SBH has been a speaker for MedImmune,
that the RSV seasons in the South began significantly earlier Inc regarding vaccines and RSV immunophrophylaxis. No
and lasted longer than seasons in the rest of the nation.9 competing financial interests exist for the other authors.
Beginning in 1999, mention is made regarding sporadic de-
tections reported throughout the year to the National Re-
References
spiratory and Enteric Virus Surveillance System.10–13
Texas has been compiling data from major centers pro- 1. Shay DK, Holman RC, Newman RD, Liu LL, Stout JW, Ander-
viding care to children since 2004 regarding the results of son LJ. Bronchiolitis-associated hospitalizations among US chil-
RSV testing to attempt to define RSV epidemiology in our dren, 1980–1996. JAMA 1999; 282:1140–1146.
state. Our institution contributes to this. Although we do not 2. Shay DK, Holman RC, Roosevelt GE, Clarke MJ, Anderson LJ.
Bronchiolitis-associated mortality and estimates of respiratory
have complete data for the period of time in this study, data
syncytial virus-associated deaths among US children, 1979–1997.
from 2002 to 2006 show percent positive RSV test rates J Infect Dis 2001; 183:16–22.
during the off-season ranging from 0 to 11%.14 However, the 3. Fergie, J, Purcell, K. Respiratory syncytial virus laboratory sur-
relatively low total number of tests performed during the off veillance and hospitalization trends in south Texas. Pediatr In-
season months may artificially inflate the percent positive. fect Dis J 2007; 26:S51–S54.
This study is subject to several limitations. Our study is 4. Light, M. Respiratory syncytial virus seasonality in southeast
retrospective in nature, and limited to patients who were ill Florida: results from three area hospitals caring for children.
enough to be admitted; we do not have information re- Pediatr Infect Dis J 2007; 26:S55–S59.
garding patients who may have had similar symptoms and 5. Washburn JF, Bocchini JA, Jamison RM. Summertime respiratory
were not admitted. We also do not have information about syncytial virus infection: epidemiology and clinical manifesta-
tions. South Med J 1992; 85:579–583.
other viral infections that may have been circulating during
6. Halstead DC, Jenkins SG. Continuous non-seasonal epidemic of
the study period, and caused co-infection in the identified respiratory syncytial virus infection in the southeast United
patients with RSV infection. States. South Med J 1998; 91:433–436.
Another limitation of the study is the possibility of in- 7. Welliver, RC. Temperature, humidity, and Ultraviolet B radia-
creased false positive diagnostic test results during a period tion predict community respiratory syncytial virus activity. Pe-
of low prevalence of infection. This phenomenon is well diatr Infect Dis J 2007; 26:S29–S35.
described.15 Due to the retrospective nature of the study, we 8. Centers for Disease Control and Prevention. Respiratory syncy-
do not have the benefit of a more complete evaluation for tial virus activity—United States, 2008–2009 season. MMWR
viral infection in these patients; rather, tests were as ordered 2010; 59:230–233.
by physicians based on clinical judgment. 9. Mullins JA, Lamonte AC, Bresee JS, Anderson LJ. Substantial
variability in community respiratory syncytial virus season
Diagnostic methods for RSV infection include viral cul-
timing. Pediatr Infect Dis J 2003; 22:857–862.
ture, rapid antigen capture assay, immunofluorescent stain- 10. Centers for Disease Control and Prevention. Respiratory syncy-
ing, and polymerase chain reaction. The laboratory at our tial virus activity—United States, 1999–2000 season. MMWR
institution used RSV EIA as the most frequently used diag- 2000; 49:1091–1093.
nostic method of testing during the study period, with 11. Centers for Disease Control and Prevention. Respiratory syncy-
proper procedures for result positive and negative controls. tial virus activity—United States, 2000–01 season. MMWR 2002;
RSV culture may be insensitive and has been called into 51:26–28.
question for diagnosis.16,17 Methods of diagnosis such as 12. Centers for Disease Control and Prevention. Brief report: respi-
polymerase chain reaction may be more sensitive, but were ratory syncytial virus activity—United States, 2003–04. MMWR
not widely available at our institution during the study 2004; 53:1159–1160.
13. Centers for Disease Control and Prevention. Brief report: respi-
period.
ratory syncytial virus activity—United States, 2004–05. MMWR
2005; 54:1259–1260.
Conclusions 14. Sánchez PJ, Murphey D, Hauger S, Brown O, Gaglani M,
Leach C, Siegel J, Pennfield S, Texas Pediatric Society Com-
We found that particular infants may present with sig- mittee of Infectious Disease & Immunizations. Sentinel Site
nificant RSV infection in the off-season, at a time when RSV Surveillance of Respiratory Virus (RSV) Infections in Texas:6 QUICK ET AL.
Implications for Prophylaxis. Poster session presented at PAS Address correspondence to:
2008. Honolulu, HI. Sarmistha B. Hauger, M.D.
15. Feinstein AR. Principles of Medical Statistics. Boca Raton, FL: Pediatric Infectious Diseases
CRC Press, 2002. Dell Children’s Medical Center
16. Ohm-Smith MJ, Nassos PS, Haller BL. Evaluation of the Binax
1301 Barbara Jordan Blvd. ste 200
NOW, BD Directigen, and BD Directigen EZ Assays for Detec-
Austin, TX 78723
tion of Respiratory Syncytial Virus. J Clin Microbiol 2004;
42:2996–2999.
17. Slinger R, Milk R, Gaboury I, et al. Evaluation of the QuickLab E-mail: shauger@sfcaustin.com
RSV Test, a new rapid lateral-flow immunoassay for detection of
respiratory syncytial virus antigen. J Clin Microbiol 2004; 42: Received for publication October 18, 2011; accepted after
3731–3733. revision October 22, 2011.You can also read