Development Update on RSV Vaccine - Fernando P. Polack, MD Fundacion INFANT
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Update on RSV Vaccine
Development
Fernando P. Polack, MD
Fundacion INFANT
Topics for review
RSV Epidemiology
• New morbidity and mortality estimates from GEN
• Mortality at the hospital in industrialized and developing countries
• Mortality in the community
• Recurrent wheezing and asthma
RSV vaccines and monoclonal antibodies
• Maternal immunization to protect infants
• Monoclonal antibodies for infants
• Pediatric vaccines
• Vaccines for the elderly
Other considerations
• Standardization of neutralizing antibody assays
• Considerations about enhanced RSV disease
• PPC and Roadmap documents
2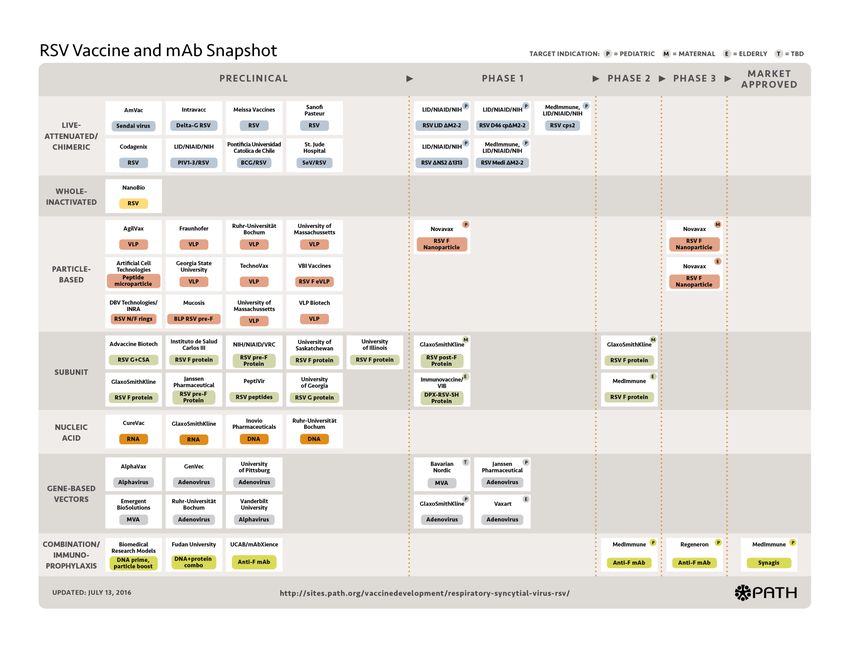
RSV Epidemiology New Global Burden Estimates
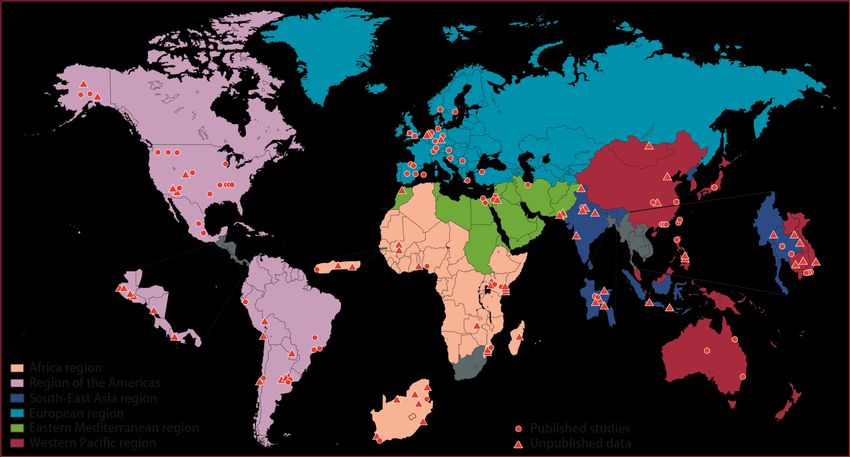
RSV Global Epi Network (RSV
GEN)
Second meeting -
First meeting -
Jun 2015
Nov 2013
71 sites (76 unpublished 4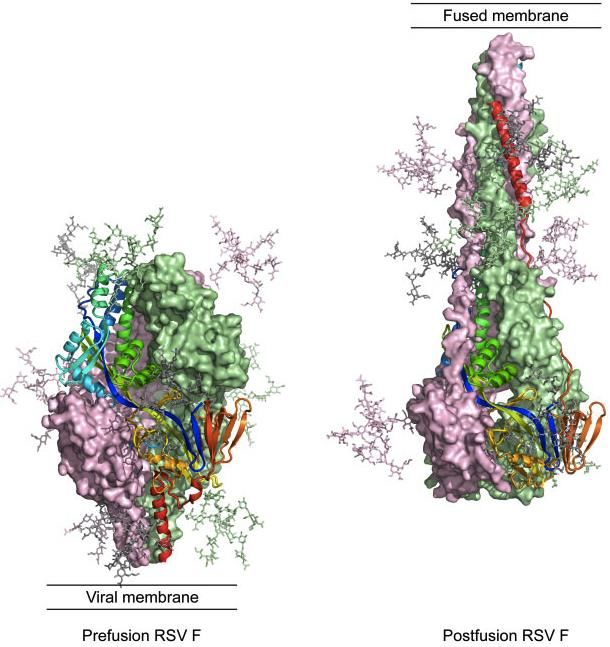
Location of incidence and hospital
mortality studies (n=157)
Funded by Bill & Melinda Gates Foundation 5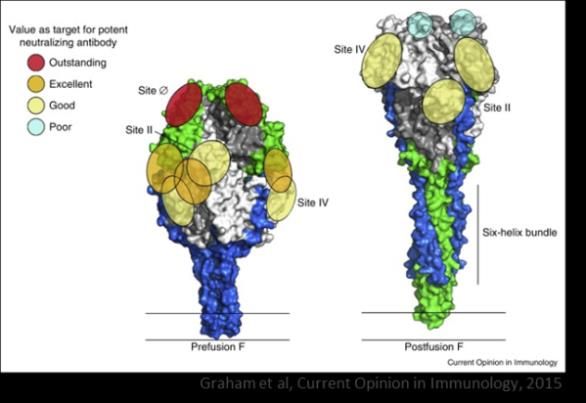
15)
RSV Global Burden Estimates (2005)
30.5
33.8(95%
(95%CI,
CI,19.5-47.9)
193-46.2) million episodes of RSV LRI annually in children < 5
years (22% of all ALRI episodes)
3.4 million episodes requiring hospitalization
2.8
95,000-149,000
66,000-199,000 deaths in 2005, 99% in developing countries
Updated estimates for RSV ALRI, severe ALRI (community based and
hospitalized) and deaths in press by the RSV Global Epidemiology Network
(RSV-GEN) . Publication expected this year
6
Lancet, in press
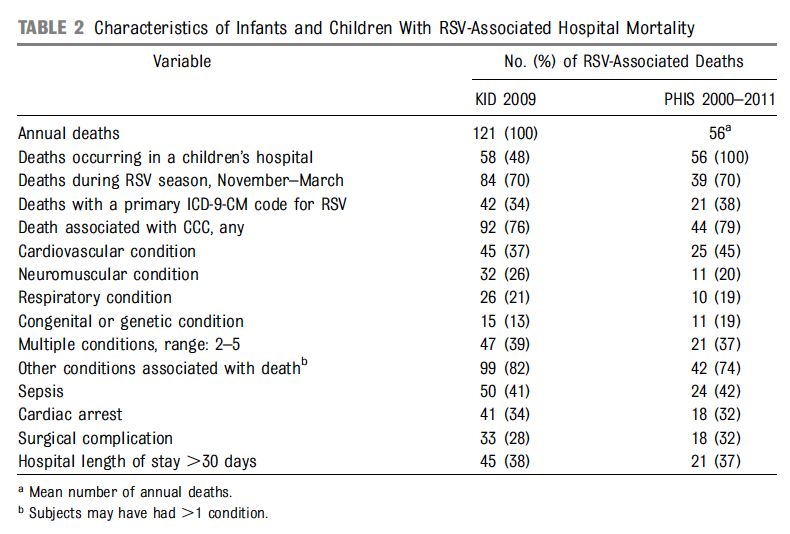
RSV Epidemiology Hospital-based mortality

Byinghton CL et al. Pediatrics 2015
Funded by Bill & Melinda Gates Foundation Geogeghan S et al, AJRCCM 17
Geogeghan S et al, AJRCCM 17
Geogeghan S et al, AJRCCM 17
Geogeghan S et al, AJRCCM 17
Geogeghan S et al, AJRCCM 17
Geogeghan S et al, AJRCCM 17
Mortality at the hospitals
• RSV is the most frequent viral pathogen
associated with post-neonatal infant mortality.
• The virus was detected in 16% of all-cause
hospital deaths; 57% of LRTI deaths where tests
were performed.
• Its CFR was lower than that of non-RSV LRTI
cases. Its importance relied on its dominating
role as an agent of severe LRTI (65%), rather
than on its specific lethality.
Geogeghan S et al, AJRCCM 17Mortality at the hospitals • In contrast to industrialized countries, RSV killed term, previously “healthy” infants. • Deaths had a strong association with bacterial sepsis (GPC) and pneumothoraxes. • The role of co-morbidities, young age, and other factors was less ostensible.
RSV Epidemiology Mortality in the community
Community deaths in infants Funded by Bill & Melinda Gates Foundation
DOES THE AGE DISTRIUBTION OF DEATHS
IN THE COMMUNITY RESEMBLE RSV DEATHS OR HOSPITALIZATIONS?
Hospitalizations
Community deaths
19Community deaths (May-August 2016)
15
RSV
percentage from the total
RV
10 H1N1
MPV
PIV 3
5
0
st
ne
ay
ly
Ju
gu
M
Ju
2016 Au
20RSV was detected in 22% of all-cause home fatalities during
the respiratory season.
40
number of nasal swabs
30
17/37
20 (46%)
8/17
(47%)
10
0
Total Positives RSV
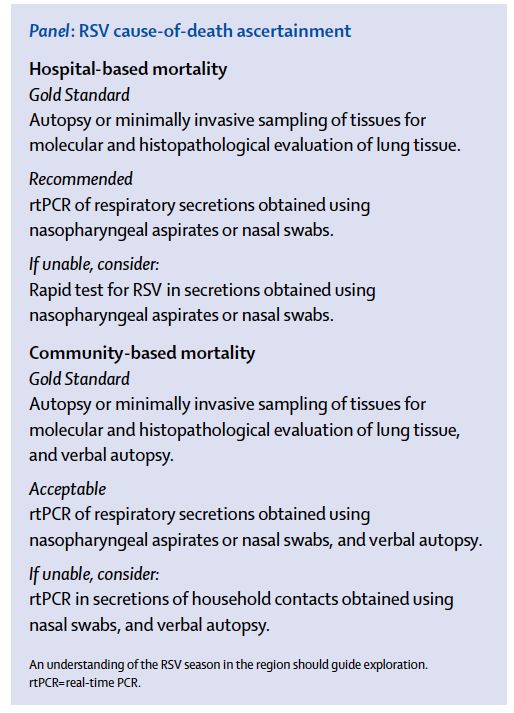
21RSV mortality
• Is a significant problem, particularly due to the
overwhelming dominance of RSV as an agent of LRTI in the
winter.
• Needs, at least, a second factor:
in industrialized countries: co-morbidities.
in developing countries
-at hospitals: suboptimal medical care
(pneumothoraxes) and secondary bacterial infections (and
those factors predisposing to them).
-in the community: social, cultural, infectious
and/or logistical factors affecting access to health care.Zanone S. Lancet Resp Med 2016
RSV Epidemiology Recurrent wheezing and asthma
Blanken MO et al. NEJM 2013
Palivizumab and recurrent wheezing
• 444 late preterm infants until age 6 years
(349 vs 95).
• Recurrent wheezing: 15.3% vs. 31.6%
(p=0.003)
• Physician diagnosed asthma: 15.3% vs.
18.2%
*Asthma defined as RW+ high IgE and/or family history of allergy
Mochizuki H et al. AJRCCM 2017Other interesting topics • Replacement and competition (Hartert TV. J Infect Dis 2017) • Subgroups of healthy infants with increased susceptibility for severe LRTI (Caballero MT. J Clin Invest 2015)
RSV LRTI Prevention
RSV vaccines and monoclonal
antibodies
Maternal immunization to protect infantsNovavax– post-F nanoparicles (alum) • RCT, placebo-controlled, group sequential: pregnant women 28-36 weeks of pregnancy to prevent symptomatic RSV- associated LRTI with hypoxemia for 90 days in infants • Follow up: mothers until 6 months post-delivery, infants follow up for 12 months. • Minimum of 4,600 women. Entering Y3. • US, Mexico, Argentina, Chile, New Zeland, Australia, South Africa, Spain, UK, Philippines. • First interim analysis for efficacy in Q1/Q2 2018.
Glaxo Smith Kline – preF antigen • Active immunization of pregnant women during the 3rd trimester of pregnancy to prevent RSV- associated LRTI in infants • Single dose to boost pre-existing immune response • Immunization in the third trimester • Recombinant subunit PreF antigen • First study in pregnant women will be launched this year – Phase III planned for 2019.
RSV vaccines and monoclonal
antibodies
Monoclonal antibodiesMedimmune – preF mAb
Characteristics
• MEDI8897: Passive RSV vaccine strategy using RSV F mAb
• Fully human, high potency IgG1 mAb derived from human B-cells
• YTE half-life extension technology
• Targets site on RSV prefusion F
• Neutralizes all RSV A and B clinical isolates tested
• Single fixed IM dose given; expected to protect up to 6 months
• Given at birth or at onset of RSV season
Program Status
• Phase 1a adult FTIH complete (N=136)
• Phase 1b/2a in 32-35 week gestational age infants (N=89); complete.
• Phase 2b clinical efficacy in 29-35 week gestational age infants planned
for 2016 (N=1,500)
• FDA fast track designation granted, study endpoints agreed with EMA-
PDCO, FDA.
36Regeneron • Extended half life mAb against RSV preF. • Completed phase III RCT in premature infants – data analysis in progress (coming months). • Planning phase III efficacy RCT in full term infants.
Biosimilar palivizumab (post-F) – WHO
and University of Utrecht
• Palivizumab off patent in 2015
• Plan to develop a ‘biosimilar’ of palivizumab and reduce costs through
– Using latest technologies (i.e. high expression cell line)
– A novel development and financing plan1
• Coordinated by the Utrecht Center of Excellence for Affordable Biotherapeutics for Public
Health
• Funded through a consortium of manufacturers
– Agreement signed on 9 March 2016
– Estimated price $US 250 per child for full 5 courses
– First market authorization expected end 2017
– Roll out the product in LMICs
1http://www.uu.nl/en/news/first-consortium-of-local-manufacturers-to-make-affordable-biosimilars-available-for-low-income
38RSV vaccines and monoclonal
antibodies
Infant vaccinesJanssen RSV junior Vaccine: Ad26.RSV.preF
Vector Antigen Administration
Replication-incompetent RSV fusion protein from the RSV A2 Begin immunization
human type 26 strain at 2 month of age
adenovirus
Ad26.RSV.FA2: prototype vaccine IM, 2 to 3-doses
Elicits Th1 response expressing native F protein
Co-administered
Expected to be similar Ad26.RSV.preF: lead vaccine with other childhood
to natural infection and candidate expressing optimized vaccines
live attenuated vaccines prefusion stabilized F protein
which do not predispose
to ERD in humans FA2 and preF protein sequences differ
by only 5 amino acids
41Janssen RSV Vaccine Phase 1 studies in
adult and elderly subjects
Prototype Ad26.RSV.FA2 in adults
Safety Immunogenicity
Ad26.RSV.FA2 was shown to be safe Ad26.RSV.FA2 increased humoral
and well tolerated (59 subjects) and cellular immunity that was
durable for 6 months.
No serious adverse events, no
adverse events that led to Ad26.RSV.FA2 enhanced the Th1-
withdrawal from study vaccine type responses with no increase in
Th2-type responses (CD4 ICS)
Ad26.RSV.preF in elderly
• Study ongoing in 72 older adults, > 60 years of age
• Preliminary data suggest favorable safety profile
• Ad26.RSV.preF showed better immunogenicity compared to Ad26.RSV.FA2 in pre-
clinical models 42Glaxo Smith Kline Pediatric Program • Active immunization of infants for the prevention of RSV- associated LRTI • Two-dose regimen from 6 wks onwards (min 1 year protection) • Co-administration with routine paediatric vaccines • Chimpanzee Adenovirus (ChAd155) encoding three RSV antigens (F, N and M2.1) • Phase I: complete in adults. Toddlers 12-24 months ongoing.
Bavarian Nordic - MVA • Based on the MVA-BN vector approved in EU& Canada, encoding FA, GA+GB, N and M2 • Phase I (63 healthy subjects) – no unexpected adverse reactions, immunogenic (boosted humoral responses durable for 6 months and T cell responses). • Phase II: enrolled 421 subjects ≥55 years old (identify optimal dose). • Optimal group(s) carried forward into 2017 RSV season with a booster dose
Sanofi- NIAID • The program continues to characterize live attenuated RSV vaccines based on two families of attenuating mutations: one with deletion of the M2-2 gene, and one with deletion of the interferon antagonist NS2. These candidates have been evaluated singly and shown promising results (see NCT01893554, and NCT03102034) • Head-to-head studies of lead candidates using the 2 approaches expected in the near future
RSV vaccines and monoclonal
antibodies
Elderly vaccinesRSV Vaccines for the Elderly
Novavax (NCT02608502)
RSV postfusion F 135 mcg
Endpoints: 10 mod-severe RSV-LRTD*, 20 RSV-
LRTD, any RSV- ARD
MedImmune/Astra Zeneca (NCT02508194)
RSV soluble postfusion F with GLA (TLR4
agonist)
Endpoint: any acute RSV respiratory illness
47
.Other important considerations
• Harmonizing neutralization assays (WHO/
NIBSC/PATH) – there are currently ~10 PRNT
assays (cell lines-virus-methods). Provide
standards.
• Pediatric vaccines and risk for ERD (VRBPAC,
FDA in May 2017).
• 2017 Roadmap and PPC for RSV Vaccines
(WHO) available.
WHO strategic vision for RSV vaccinesAcknowledgements • Ruth Karron (Johns Hopkins University) • Harish Nair (University of Edimburgh) • Greg Glenn (Novavax) • Ilse Dieussaert (GSK) • Myra Widjojoatmodjo (Janssen) • Eduardo Forleo Neto (Regeneron) • Fernando Maellas (mAbxience) • Nathalie Samy (Bavarian Nordic) • Johan Vekemans (WHO)
You can also read