DIAGNOSIS 2017/2018 - Analysing the key trends in the medical schemes industry from 2000 to 2016 - Alexander Forbes
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

DIAGNOSIS
2017/2018
Analysing the key trends in the medical schemes industry from 2000 to 2016
Alexander Forbes Health Technical and Actuarial Consulting Solutions
HEALTH
ALEXANDER FORBES HEALTH
INTRODUCTION
Alexander Forbes Health’s Technical and Actuarial
Consulting Solutions team is proud to present this
year’s Diagnosis.
This publication will give you a comprehensive view of the performance of the South
African medical schemes industry as well as some of the changes and challenges
facing the industry.
This analysis covers key statistics and trends over the 17-year period from 2000 to
2016, based largely on the consolidated financial results for all registered medical
schemes, with specific focus on the 10 largest open and the 10 largest restricted
medical schemes by principal membership.
The final demarcation regulations and the gazetted National Health Insurance White
Paper have resulted in much debate in the medical schemes industry in 2017. The
expected consolidation process of both schemes and benefit options in 2018 has
resulted in some uncertainty for many schemes. If you would like to discuss any of
the issues addressed in more detail, please speak to your Alexander Forbes Health
consultant or contact one of the specialists listed at the end of this publication.
2
DIAGNOSIS 2017/2018
CONTENTS
1. Key industry developments 5
2. Performance indicators 9
2.1 Size and scale 9
2.2 Market share 12
2.3 Membership profile 13
2.4 Contributions 20
2.5 Inflationary trends 21
2.6 Healthcare expenditure 23
2.7 Non-healthcare expenditure 25
2.8 Financial performance 28
2.9 Investments 32
2.10 Solvency levels 34
3. Alexander Forbes Health Medical Schemes Sustainability Index 37
4. Conclusion 41
3
ALEXANDER FORBES HEALTH 4

DIAGNOSIS 2017/2018
KEY INDUSTRY DEVELOPMENTS
Industry consolidation
At the Board of Healthcare Funders A National Health Insurance (NHI)
conference in July 2017 the acting Implementation Committee on
registrar of the Council for Medical Consolidation has been established and
Schemes (CMS) indicated in his tasked with restructuring the current
presentation that the CMS would healthcare financing arrangements in the
consider the consolidation of risk lead-up to the creation of a central NHI
pools across smaller medical schemes fund. This is to be achieved through five
in South Africa. According to the transitional arrangements covering the
Medical Schemes Act 131 of 1998 following segments of the population:
(as amended), the registration of a new ■■the unemployed
medical scheme requires a minimum ■■the informal sector
membership of 6 000 principal ■■the formal sector comprising large
members per scheme and 2 000 businesses
principal members per scheme option. ■■the formal sector comprising small
and medium-sized businesses
The CMS has issued Circular 51 ■■the public sector
of 2017, clarifying its approach to
consolidation and reiterating its The unemployed and the informal sector
commitment to improving financial will be covered through the creation of
protection for medical scheme members new funding arrangements. The formal
through effective risk pooling. This sectors would see the consolidation
circular sets out the Council’s approach of existing medical schemes into one
to consolidation as a consultative fund with mandatory coverage in which
process involving key stakeholders PMBs will be replaced with a more
and focusing only on the 31 medical comprehensive benefit package. The
schemes that currently have fewer than public sector would see similar funding
6 000 members. However, the review changes to the formal sector along
will also include schemes servicing local with changes to current government
government and state-owned entities healthcare subsidies.
as well as civil servants at a national or
provincial level.
5
ALEXANDER FORBES HEALTH
INDUSTRY TIMELINE
1998 2000
■■The Medical Schemes Act is signed into law. ■■The Medical Schemes Act comes into
It introduces prescribed minimum benefits effect and the Council for Medical
(PMBs), community-rated contributions and Schemes (CMS) is established.
open enrolment.
2004 2003 25%
■■A Competition Commission ruling bans the system of collective tariff setting ■■The National Health Act gives a
between schemes and healthcare providers. framework for a structured and uniform
■■Single exit price (SEP) is implemented for pharmaceutical manufacturers. health system.
■■The National Health Reference Price List (NHRPL) is first published by the ■■Personal medical savings accounts are
Department of Health. limited to 25% of gross contributions.
■■Medical schemes must maintain a 25% solvency level.
2005 2006
■■The Government Employees Medical ■■The Council for Medical Schemes takes
Scheme (GEMS) is registered. over publication of the National Health
■■The Children’s Act Reference Price List, a guideline for
stipulates the age of consent for minors healthcare service tariffs.
to medical and surgical treatment.
2009 2008
■■The Competition Amendment Act is signed into law, providing ■■The Medical Schemes Amendment Bill is proposed,
a legal framework and giving formal powers to the Competition providing for the risk equalisation fund, low-income
Commission to conduct market enquiries. benefit options, improved governance, and an
■■The Protection of Personal Information Bill is published to amendment of the definition of the business of a
protect personal information processed by public and private medical scheme.
bodies, including medical schemes and industry stakeholders. ■■The Health Professions Council of South Africa
scraps ethical tariffs, used by providers as a ceiling
for patient accounts.
2010 2011
■■Dispensing fee regulation is introduced for pharmacists and ■■The Consumer Protection Act comes into
licensed health professionals. effect, supporting a culture of consumer
■■The High Court rules the National Health Reference Price List rights and responsibilities.
invalid and sets it aside. ■■The Green Paper on the National Health
■■The High Court dismisses the Board of Healthcare Funders’ court Insurance Policy is published.
application to seek clarity on the meaning of Regulation 8(1).
■■The Council for Medical Schemes publishes the prescribed
minimum benefits code of conduct to ensure compliance with
Regulation 8(1) – ‘pay in full’.
6
DIAGNOSIS 2017/2018
2017
■■The revised National Health Insurance (NHI) White Paper is gazetted on 30 June 2017. This version does
not provide updated estimates of the NHI costs, but identifies additional potential sources of funding,
including the removal of medical aid tax credits as well as the public sector medical aid subsidies.
■■The findings and recommendations of the Competition Commission’s Health Market Inquiry are delayed to
30 November 2017.
■■The Constitutional Court overturns the Supreme Court’s ruling that required schemes to hold medical
savings account assets separately from the rest of the scheme’s assets. This means that:
●●medical savings account assets will now form part of the scheme’s assets
●●assets can be invested in investment classes other than cash
●●interest on medical savings account assets can accrue to the scheme
■■An NHI Implementation Committee on Consolidation is established to oversee the restructuring of the
industry before the full implementation of NHI. This process includes:
●●consolidating those schemes with fewer than 6 000 members into larger schemes
●●merging public sector schemes
●●reducing the number of benefit options offered by the remaining schemes
2016
■■The Competition Commission Inquiry into Private Healthcare is delayed, with the draft report not being published
by August 2016 as proposed in the revised timelines.
■■The Council for Medical Schemes releases a proposed risk-based solvency framework to replace the controversial
25% statutory minimum that has been in place since the introduction of the Medical Schemes Act.
■■Final demarcation guidelines are published in a joint statement by the Department of Health
and National Treasury. These guidelines allow hospital cash plans and gap cover to continue, but prohibit primary healthcare
insurance products which will fall under the CMS and require exemption from the Medical Schemes Act.
2015
■■The Competition Commission Inquiry into Private
‘ 2014 – the Financial
Services Board introduces
Treating Customers
‘
Healthcare continues, with medical schemes and Fairly (TCF)
administrators being requested to provide claims
and tariff information for the last 17 years.
■■The Minister of Health publishes a draft
2014
amendment to Regulation 8. Medical schemes are ■■The 12-member board of the newly established Office
no longer required to pay for prescribed minimum of Health Standards Compliance is named.
benefits at cost, but rather at either a contracted ■■The Competition Commission Inquiry into Private
rate or the 2006 guideline tariff plus inflation. Healthcare begins.
■■The Council for Medical Schemes approves the ■■The Draft Road Accident Fund Benefit Bill provides
framework for exemption and allows low-cost for a no-fault benefit scheme and a new administrator
benefit options to be introduced from 1 January to replace the Road Accident Fund.
2016. The framework is then withdrawn soon ■■The Financial Services Board introduces Treating Customers
afterwards. Fairly, a market conduct framework of regulatory reform.
■■The National Health Insurance White Paper is ■■The National Department of Health publishes a National Health
published on 10 December 2015. It proposes a Insurance booklet.
‘
single payer system with no option to opt out
and medical schemes being limited to offer
complementary cover.
2013 – the Protection ‘
of Personal Information
Act came into law
2012 2013
■■The Taxation Laws Amendment Act provides ■■The Financial Services Laws General Amendment Act amends the Medical
for a new medical tax credit system to Schemes Act by widening the definition of the business of a medical scheme.
replace medical tax deductions. The ■■Schemes must hold members’ medical savings account (MSA) contributions
definition of a dependant is widened in the separate from scheme reserves and allow interest to accrue to positive
Income Tax Act to be the same as that in the MSA balances.
Medical Schemes Act. ■■The National Health Amendment Act provides for the establishment of the
■■Draft demarcation regulations propose the Office of Health Standards Compliance (OHSC), a key building block of
removal of most gap cover products and National Health Insurance.
hospital cash plans. ■■The Competition Commission Inquiry into Private Healthcare is announced.
■■The Protection of Personal Information Act is signed into law.
7
ALEXANDER FORBES HEALTH 8

DIAGNOSIS 2017/2018
PERFORMANCE INDICATORS
This section analyses the key statistics ■■Membership growth: Increasing ■■Financial results: The trend in a
influencing the performance of membership reduces the volatility of scheme’s financial results illustrates
medical schemes. a scheme’s claims, and improves the the adequacy of their pricing.
profile, as new members tend to claim ■■Solvency levels: Although the
When evaluating the performance less than the average member in their current statutory solvency level of
of medical schemes, key factors to first year of membership. 25% of gross contribution income
consider are as follows: ■■Membership profile: Claims may be inappropriate, each scheme
■■Size and scale: Larger schemes experience will be more favourable should have sufficient reserves after
tend to have more stable and more for younger populations with lower considering each of the previous factors.
predictable claims experience. They chronic prevalence.
should also have greater negotiating
power when setting prices.
2.1 Size and scale
Medical schemes in numbers
6 000 000 100
90
5 000 000
80
70
4 000 000
Number of medical schemes
Number of beneficiaries
60
3 000 000 50
40
2 000 000
30
20
1 000 000
10
0 0
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Beneficiaries in open medical schemes Beneficiaries in restricted medical schemes
Number of open medical schemes Number of restricted medical schemes
9
ALEXANDER FORBES HEALTH
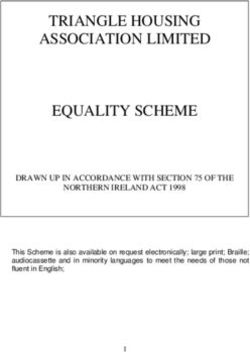
At the end of 2016 there were and particularly for restricted medical since 2000. The 82 medical schemes
82 registered medical schemes in schemes, by the significant amount of operating in South Africa at the end
South Africa, reducing from 83 schemes management time needed to manage an of 2016 served a total of 3.99 million
at the end of 2015 because LMS employer-based restricted scheme. principal members and 8.88 million
Medical Fund (previously Liberty Medical beneficiaries. The number of principal
Scheme) amalgamated with Bonitas Momentum Health and Metropolitan members covered on medical schemes
Medical Fund with effect from 1 October Medical Scheme amalgamated increased by 1.0% in 2016, while the
2016. From the end of 2000 to the end with effect from 1 July 2017, while total number of beneficiaries under
of 2016 the number of medical schemes Discovery Health Medical Scheme cover increased by 0.8%, with
in existence reduced from 144 to 82, and the University of Witwatersrand greater growth in beneficiaries being
which represents a 43% decrease in the Staff Medical Aid Fund are expected observed on restricted medical
number of registered medical schemes to merge on 1 January 2018. The schemes. A total of 58.8% of principal
over 16 years, mainly as a result of Community Medical Aid Scheme members participated in open medical
amalgamations among the smaller, less (COMMED) was liquidated in 2017, schemes at the end of 2016 with
sustainable schemes. The number of with Bonitas Medical Fund agreeing to the balance of 41.2% participating
open medical schemes has decreased take on the existing COMMED members in restricted medical schemes. This
by 25 (53%) compared to a decrease with no underwriting. compares to 58.9% and 41.1%
of 37 (38%) restricted medical respectively at the end of 2015.
Despite the observed decrease in
schemes over the 16-year period. This
the number of medical schemes, the The graph below shows the percentage
consolidation appears to be driven
industry has grown by 1.45 million change in medical scheme membership
mainly by the difficulty in maintaining
principal members (57.0%) and over the last 16 years.
the financial sustainability of small
2.29 million beneficiaries (34.7%)
schemes in the current environment
Annual percentage growth in membership
30%
25%
20%
Percentage annual growth rate
15%
10%
5%
0%
-5%
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
All schemes Open schemes Restricted schemes
10DIAGNOSIS 2017/2018
There is a significant difference members. The open schemes with the current environment where schemes
between the trends in the annual membership below this threshold are are required to pay in full for the cost
growth rate of open and restricted Cape Medical Plan (5 463 principal of prescribed minimum benefits,
medical schemes, with the divergence members), Makoti Medical Scheme regardless of the rates charged.
in the trend beginning in 2006 with (2 427 principal members) and
the registration of the first members Suremed (1 364 principal members). Despite these risks, a fair number of
on GEMS. Following the significant restricted schemes are still performing
increase in restricted scheme A large membership base allows well. Of the 31 schemes referred to
membership attributable to GEMS in for lower claims volatility and helps earlier that have fewer than 6 000
2006 and 2007, the annual growth in schemes, or their administrators, members, only nine achieved a surplus
restricted schemes reduced each year, negotiate more competitive before investment income in 2016,
with very little growth being observed reimbursement rates and fees with the down from 16 in 2015, which indicates
in the restricted schemes from 2013 to various healthcare service providers. the severity of claims in 2016 as well as
2015. In 2016 principal membership This ensures that medical scheme the volatility to which smaller schemes
of open medical schemes grew by members have lower shortfalls are exposed.
0.9% while membership of restricted or copayments when using these
designated service providers. The graph below ranks the top 10 open
schemes grew by 1.3%, with net growth
schemes and top 10 restricted schemes
of 41 175 members across the industry
A small membership base generally according to the number of principal
during the year.
results in a more variable claims members at 31 December 2016.
The minimum membership requirement experience which increases the risk This represents 88.2% of all principal
set by the Council for Medical Schemes of contributions not being set at an members participating on a registered
for registering a new medical scheme appropriate level to cover all claims medical scheme, or 95.7% and 77.4%
is 6 000 principal members. At the end and expenses. This variability is of open and restricted medical scheme
of 2016 there were three open medical compounded further by the negative membership respectively.
schemes and 28 restricted schemes impact of high cost claims, especially in
with fewer than 6 000 principal
Membership by medical scheme
1 600 000 30%
1 400 000
20%
1 200 000
Percentage growth from 2015 to 2016
10%
Number of lives covered
1 000 000
800 000 0%
600 000
-10%
400 000
-20%
200 000
– -30%
ry
s
m
ed
p
d
lth
e
lth
ed
S
ed
ed
lth
lth
ED
ed
ed
p
ed
ita
zw
el
l
ou
M
ve
tu
ie
tm
m
lm
km
sm
m
lm
ea
ea
ea
ea
M
ih
GE
n
sh
Si
gr
co
en
os
of
Bo
U
ed
dh
yH
Po
H
H
so
s
an
n
ed
ed
Be
s
Pr
om
H
W
Ba
Sa
Di
LA
um
M
Fe
Ke
Tr
N
M
M
M
SA
in
at
Pl
2016 principals 2016 dependants Growth in principal members Growth in dependants
11ALEXANDER FORBES HEALTH
Bonitas amalgamated with LMS Medical Umvuzo Health Medical Scheme and cover when they need medical attention.
Fund in 2016, resulting in growth the Chartered Accountants (SA) Medical This anti-selective risk is greatest
of 17.8% in the number of principal Aid Fund (CAMAF) are the 11th and 12th for those schemes with the fewest
members during the year. As a result largest restricted schemes at underwriting controls, as they are most
of that amalgamation, Hosmed Medical 31 December 2016, with 26 319 and 24 vulnerable to these high claimers.
Aid Scheme is a new entrant to the 957 principal members respectively.
top 10 open medical schemes in
Five of the open schemes and six of
2.2 Market share
2016 with 25 528 principal members.
Topmed Medical Scheme and the restricted schemes considered here The industry’s net growth of 68 558
Resolution Health Medical Scheme are experienced positive growth in 2016, principal members over the 2016
the 11th and 12th largest open schemes with the remaining nine experiencing a financial year was driven by the growth
at 31 December 2016, with 22 355 and reduction in membership numbers. on Discovery Health Medical Scheme
17 956 principal members respectively. (Discovery) which experienced net
growth of 29 589 principal members,
The top 10 restricted medical schemes The number of beneficiaries with
as well as the Government Employees
by principal membership have remained medical scheme cover grew by 0.8% in
Medical Scheme (GEMS) which grew by
unchanged in 2016. However, LA Health 2016, after the net loss of lives observed
19 589 principal members.
Medical Scheme is now the fourth in 2015. The number of principal
largest restricted scheme as a result of members covered increased by 1.0%, Discovery’s total market share based
the 8.9% growth in principal members which again resulted in the average on the number of principal members
over the year, with Platinum Health family size in the industry reducing from has increased from 16% in 2001 to
down to fifth place because of a loss 2.23 at 31 December 2015 to 2.22 at 33% at the end of 2016, compared to a
of 5.2% of its membership. Transmed 31 December 2016, which may indicate decrease in market share for the rest of
continued to lose membership, with financial pressures resulting in fewer the open schemes from 54% in 2001 to
an 11.9% and 17.7% reduction in dependants being added to cover. There 26% in 2016.
the number of principal members and is also a tendency in the market for
dependants respectively during the year. members to only add beneficiaries to
12DIAGNOSIS 2017/2018
This decline in open medical scheme the past was assisted by continued 2.3 Membership profile
membership (excluding Discovery) new member growth, stimulated by an
is due to many members choosing attractive employer subsidy. However, One of the most important contributing
to move from their current medical that employer subsidy was not increased factors to a scheme’s performance is the
scheme to join Discovery Health and for a number of years from 2011, which risk profile of its members, with some of
the movement of eligible public sector may have contributed to the slowdown the key statistics being:
employees from the open scheme in membership growth. The increase ■■average age of beneficiaries
market to GEMS since its inception. in the public sector subsidy with effect ■■pensioner ratio (defined as the
from 1 January 2016 is likely to have percentage of beneficiaries over the
In 2016 GEMS’s total market share was contributed towards the growth in lives age of 65 years)
17%, compared to 2% in 2006 when covered on GEMS during the year. The ■■average family size
the first members joined. The rapid total market share of the balance
growth in membership includes eligible of the restricted schemes has This section considers the trends in each
government employees transferring from decreased from 30% to 24%, driven of the above factors.
other open schemes, the amalgamation by a number of amalgamations of
with Medcor in 2010 and the transfer restricted schemes into the open
of a group of 16 000 pensioners from medical schemes environment.
Medihelp to GEMS early in 2012. The
increase in GEMS’s market share in
Market share by principal membership
GEMS Discovery
2010: Medcor 2004: AngloGold
2016
2012: Pre-92 Medihelp pensioners 2010: Afrisam, Umed
2012: Edcon
2013: Nampak, IBM
2011 33% 2014: Altron, Afrox, PG Bison
17%
2006 29%
2%
16%
27%
2001
16%
28% 30%
54%
43%
25% 30%
24%
26%
All restricted medical schemes All open medical schemes
(excluding GEMS) (excluding Discovery)
2001 to 2016 2001 to 2016
Net reduction of 37 schemes Net reduction of 27 schemes
13ALEXANDER FORBES HEALTH
Average age of beneficiaries
35
34
Average age of beneficiaries
33
32
31
30
29
28
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
All schemes Open schemes Restricted schemes
Note: Average age was recorded in the CMS Annual Reports from 2005 only.
The average age of beneficiaries in From 2006 to 2010 the average age of As a scheme ages, we expect the
the medical schemes industry has beneficiaries in the restricted scheme average claims per member to increase,
remained fairly constant since 2005, environment reduced consistently each with a generally accepted benchmark
with a marginal increase from year. This was due to the rapid growth of a 2% increase in average claims per
32.3 years in 2015 to 32.5 years in of GEMS, with significant numbers of year increase in average age. A typical
2016. The average age of both open younger members joining the scheme claims curve is shown on page 16.
and restricted schemes increased during the early years. From 2011 the
slightly in 2016, with a slightly bigger growth driven by GEMS slowed down,
increase experienced by open schemes. and this has resulted in the average
The average age of beneficiaries on age of restricted scheme beneficiaries
open schemes increased by 0.2 years increasing from that point.
to 34.0 years, while the average age on
restricted schemes increased from 30.5
to 30.6 years at the end of 2016.
AVERAGE AGE OF
2015 BENEFICIARIES 2016
32.3 All schemes 32.5
33.8 Open schemes 34.0
30.5 Restricted schemes 30.6
14DIAGNOSIS 2017/2018
15ALEXANDER FORBES HEALTH
A typical claims curve over a member’s lifetime
Young and single Family with children Middle-aged Retired or retiring
■■ Hospital cover ■■ Hospital cover ■■ Hospital cover ■■ Hospital cover
■■ Limited or no ■■ Day-to-day cover ■■ Higher day-to-day cover ■■ Comprehensive
day-to-day cover ■■ Maternity benefits ■■ Chronic benefits day-to-day cover
■■ Limited chronic benefits ■■ Higher chronic benefits
■■ Cover for joint
Average claim per member
replacements and other
age-related conditions
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70+
Age
Individual claims Family claims
16DIAGNOSIS 2017/2018
The following graph considers the average age of beneficiaries for each scheme included in this year’s analysis. It also includes
the change in the average age of each scheme from 31 December 2013 to 31 December 2016.
Average age of beneficiaries
55 7
50 6
45 5
40 4
35 3
Change in age
Average age
30 2
25 1
20 0
15 -1
10 -2
5 -3
0 -4
y
s
m
ed
p
ld
lth
e
lth
ed
S
ed
ed
lth
lth
ED
ed
ed
p
ed
er
ta
zw
el
ou
M
tu
ie
m
m
lm
m
m
m
lm
ea
ea
ea
ea
ov
ni
M
ih
GE
sh
Si
gr
en
st
os
nk
ns
of
Bo
U
ed
dh
yH
Po
H
H
so
sc
ed
ed
Be
Pr
om
H
W
a
Ba
Sa
Di
LA
um
M
Fe
Ke
Tr
N
M
M
M
SA
in
at
Pl
Average age 2016 Three-year change
While the absolute age of a scheme’s an extremely high pensioner ratio, in
membership is important and indicative part because membership is voluntary.
of the likely claims profile, the change Transmed’s average age has also
in this figure serves as an indicator of increased significantly over the last
a change in the profile that would result three years as a result of the loss of a
in the medical scheme needing to significant number of younger, healthier
take corrective action in its pricing beneficiaries. LA Health’s average age
of benefits, especially if the age were has reduced significantly over the last
to increase. three years as a result of the high rate
of growth from younger and healthier
Of the 20 schemes included in this members. Momentum and Bankmed
year’s Diagnosis, KeyHealth has the also experienced decreases in the
highest average age of beneficiaries in average age of beneficiaries over the
the open schemes, whereas Transmed three-year period. As in previous years,
has the highest average age in the Polmed has the lowest average age of
restricted schemes. In addition to a all the schemes considered.
high average age, Transmed also has
17ALEXANDER FORBES HEALTH
Pensioner ratio
10%
9%
8%
Pensioner ratio
7%
6%
5%
4%
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
All schemes Open schemes Restricted schemes
Note: Pensioner ratios were recorded in the CMS Annual Reports from 2005 only.
The average pensioner ratio across the industry increased from 7.7% to 7.9% in 2016. Open schemes have experienced
a greater increase in the pensioner ratio than restricted schemes, with an increase from 8.8% to 9.2% from 2015 to 2016
compared to the increase from 6.1% to 6.3% on restricted schemes.
2015 PENSIONER RATIO 2016
7.7% All schemes 7.9%
8.8% Open schemes 9.2%
6.1% Restricted schemes 6.3%
18DIAGNOSIS 2017/2018
Average family size
2.8
2.7
2.6
Average family size
2.5
2.4
2.3
2.2
2.1
2.0
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
All schemes Open schemes Restricted schemes
In 2016 the average family size for absence of employer subsidies. Those In addition, as members’ dependent
restricted medical schemes increased beneficiaries who have been removed children become self-supporting, they
slightly from 2.38 to 2.39. This was from cover may be added back on become ineligible for membership as
driven by the growth in dependants to the membership when they need dependants on their parents’ medical
covered on GEMS over the year. medical cover, for example during a scheme and in turn become principal
pregnancy, and medical schemes may members themselves. This has a direct
However, the average family size for use waiting periods to try to control this impact on the average family size in
the entire medical schemes industry anti-selective behaviour. two ways:
has declined over the last 16 years, ■■Dependants being removed from
and this trend continued in 2016. Those beneficiaries who have been a medical scheme will reduce the
This indicates that fewer dependants removed from cover may be added back average family size.
per principal member are being on to the membership when they need ■■Individuals joining a medical scheme
registered with medical schemes each medical cover, for example during a as single members will also reduce the
year. This may be due to affordability pregnancy, and medical schemes will average family size.
constraints of members who can no use waiting periods to try to control this
longer afford to provide medical cover anti-selective behaviour.
for their entire family, particularly in the
2015 FAMILY SIZE 2016
2.23 All schemes 2.22
2.12 Open schemes 2.11
2.38 Restricted schemes 2.39
19ALEXANDER FORBES HEALTH
2.4 Contributions investment income is then added to the excess of the statutory requirements.
reserves of the scheme and serves to However, this would not be sustainable
Medical schemes work on the concept of increase its solvency levels. However, in the long term, as over time the
risk pooling, where the risk contribution where investment income is not sufficient scheme would become underpriced
charged to members depends on a to cover this shortfall, the scheme is and would ultimately need to adjust
combination of these factors: forced to use its existing reserves, which its pricing with larger contribution
■■Claims: the expected medical expenses results in decreasing solvency levels. A increases in future years.
of the entire membership group scheme may decide to use investment
income to cover claims or expenses for a The graph below considers the
■■Non-healthcare expenses: the costs
number of reasons, including increasing allocation of contribution income for
associated with any administration of
claims costs, short-term adverse claims the top 10 open schemes and top 10
claims and day-to-day operations
experience and cross-subsidisation restricted schemes, together with the
■■Investment income: the interest
between benefit options. totals for open and restricted schemes
or returns expected from the
and the industry as a whole. Where the
scheme’s assets
Some schemes may intentionally set contribution to reserves sits below the
Where the scheme’s claims and contributions to use part or all of the 0% line, schemes have used part or all
expenses exceed the contributions, investment income to subsidise claims of their investment income to fund for
investment income is required to and expenses, particularly schemes claims and expenses.
subsidise this shortfall. Any remaining which have significant reserves in
In simple terms, the financial
operations of a medical scheme can be
described by four main factors, shown contributions + investment income ≥ claims + expenses
in the equation:
Allocation of contribution income in 2016
110%
100%
90%
80%
Percentage of gross contribution income
70%
60%
50%
40%
30%
20%
10%
0%
-10%
ry
s
m
ed
lp
ld
th
e
lth
ed
S
ed
ed
um lth
lth
ED
ed
ed
p
ed
en
d
try
ta
zw
ou
te
M
ve
tu
e
ie
al
m
m
lm
m
sm
m
lm
Op
us
ea
ea
ea
ni
M
ih
ric
GE
sh
Si
gr
e
o
en
st
os
nk
of
Bo
U
d
ed
dh
yH
Po
H
H
so
sc
an
ed
st
ed
Be
In
Pr
om
H
W
Ba
Sa
Di
LA
M
Fe
Re
Ke
Tr
N
M
M
M
SA
in
at
Pl
Medical savings account Healthcare expenditure Non-healthcare expenditure Contribution to reserves
20DIAGNOSIS 2017/2018
In some cases, where investment income 2.5 Inflationary trends the average contribution per principal
has not been sufficient, schemes have member per month, and allow for
had to use their existing reserves, placing The graph below compares medical normal medical scheme contribution
pressure on solvency levels. scheme contribution inflation, along increases, as well as buy-ups and
with medical care and healthcare buy-downs to other benefit options.
In 2016, 13 of the 20 schemes expense inflation trends, to consumer Changes in contributions as a result of
considered did not have sufficient price index (CPI) inflation over the last family size or family composition are
contribution income to cover both their 17 years, where: also taken into account.
claims and non-healthcare expenses in ■■CPI inflation is the weighted average ■■Medical care and health expense
full and so used investment income and price inflation in different sectors inflation is measured by Statistics
in some cases their existing reserves to and indicates the general level of South Africa and is based on that
subsidise the cost incurred. Two open price increases. Viewed in isolation, it component of CPI which relates to
schemes, Discovery and Bestmed, and doesn’t necessarily give an accurate doctors’ fees, nurses’ fees, hospital
five restricted schemes, LA Health, reflection of cost pressures in a fees, nursing home fees, medical
Platinum Health, SAMWUMED, particular sector. Individual sectors and pharmaceutical products and
Transmed and Sasolmed, had sufficient may experience cost increases that therapeutic appliances.
contribution income to add to their differ from CPI inflation, as is the case
reserves during the year. in the healthcare sector.
■■Medical scheme contribution inflation
In the following sections we consider
is calculated for all medical schemes
each component of the medical
who submit annual financial returns
scheme pricing equation in more detail.
to the Registrar of Medical Schemes.
However, we will first look at some of the
Percentage increases are based on
inflationary trends that we have seen in
the industry over the past 17 years.
AVERAGE INFLATION OVER 17 YEARS
Medical care and health
expenses inflation
Registered medical scheme
contribution inflation 7.6% per year
7.5% per year
Rebased CPI inflation
5.8% per year
21ALEXANDER FORBES HEALTH
Average annualised The general observation in the industry buy-downs to lower cost benefit options,
is that medical inflation (medical care new entrants joining low-income options,
contribution increases and health expenses inflation) will and changes to family size, possibly
2007 to 2018 be approximately 2% to 3% higher through the removal of dependants as a
than CPI inflation over the long term. result of affordability constraints.
However, increases in a particular year
may be significantly higher because The graph on the left provides a
of adverse claims experience. The high-level summary of the average
deviation from CPI is mainly due to: headline contribution increases
12%
■■high increases in healthcare service announced by medical schemes since
Bestmed 11.0% provider fees 2007 and compares this to average CPI.
■■a rising burden of disease Note that we have taken an arithmetic
■■increasing hospital admission rates average for illustrative purposes and have
Fedhealth 10.1% ■■more use of benefits only included the medical schemes where
■■new medical technologies this information is available. Also note that
Medshield 9.5% these increases are based on the headline
■■the requirement to maintain
reserves of at least 25% of gross increases announced by individual
Bonitas 9.3% schemes and the method of calculation
Medihelp 9.3% contribution income
Momentum 9.3% ■■certain benefit enhancements may vary. It does, however, provide some
Discovery 9.2% useful information on real contribution
CPI inflation has averaged 5.8% over increases faced by members.
the last 17 years, while medical care
and health expenses inflation has been The average contribution increases for
on average 7.6% per year, resulting the top nine open medical schemes
Sizwe 7.8% since 2007 have far exceeded average
in a gap of 1.8% per year. Over the
same period, average medical scheme CPI. The margin between the level of
contribution inflation was 7.5% per CPI and the industry’s contribution
CPI 6.2% year, resulting in actual increases in rate was highest from 2008 to
medical scheme contributions per 2011. Since 2012 the contribution
principal member exceeding CPI increases have tended to be closer
inflation by at least 1.7% per year. to CPI as schemes have aimed to
limit increases in contributions to
The gap between medical scheme increase competitiveness and minimise
contribution inflation and CPI inflation membership losses as a result of
has reduced in recent years, most affordability constraints. Increases
likely as a result of efforts by medical announced for 2017 were higher than
schemes in managing the costs in prior years because of a significant
charged by providers. While this would increase in the use of in-hospital
have a direct impact on medical benefits reported by many schemes.
scheme contribution increases, the However, the contribution increases for
further reduction in the gap between 2018 are lower again, in part because of
average medical scheme contribution the lower level of CPI inflation in 2017.
0% inflation and CPI inflation indicates the
extent of member
22DIAGNOSIS 2017/2018
2.6 Healthcare expenditure
One of the main components benefit year, open medical schemes towards risk claims than open medical
influencing the performance of a had an overall risk claims ratio of 89.3% schemes. This trend is illustrated in the
medical scheme is its healthcare compared to the 95.6% experienced graph below.
expenditure, or claims experience. In by restricted medical schemes. The
this section we consider the claims ratio industry as a whole experienced a The graph below also shows a cyclical
as well as the actual level of claims that higher claims year in 2016 than in trend. This is most likely caused by the
are paid by medical schemes. 2015, with the average claims ratio lag effect of medical schemes’ annual
increasing for the third successive year. pricing exercises. Where a scheme has
Healthcare expenditure includes all The noticeable increase in the claims experienced adverse claims during the
payments made for claims incurred ratio from 2014 to 2015 was in part due year, it would usually only correct that
by members. The risk claims ratio is to the inclusion of managed care fees in experience through higher contributions
defined as the ratio of risk claims to healthcare expenditure from 2015. or benefit reductions (and therefore
risk contributions (the proportion of lower relative claims) in the next
contributions that are used to fund Many restricted schemes do not incur financial year, and this corrective action
claims, excluding any allowance for certain non-healthcare expenditure often needs to take place over at least
medical savings accounts). items such as distribution costs, two years.
marketing expenses and broker fees.
The risk claims ratio for all medical As a result, they can often afford to use
schemes increased from 91.4% in a higher percentage of risk contributions
2015 to 92.1% in 2016. For the 2016
Trend in claims ratios
120%
110%
Managed care fees were included with
healthcare expenditure from 2015
Risk claims as a % of risk contributions
100%
90%
80%
70%
60%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
All medical schemes Open medical schemes Restricted medical schemes
23ALEXANDER FORBES HEALTH
Medical schemes usually finalise their surplus (contributions less claims
benefits and contributions reviews in and expenses) while containing non-
September each year, without the full healthcare expenses below the Council
membership and claims experience of Medical Schemes’ generally accepted
data of that year. Where experience guideline of 10% of contributions and
has been worse than expected in the building reserves to a sustainable level.
first part of the year and is therefore
included in the data used for pricing, Although 85% is the generally accepted
allowances can be made for this benchmark for the claims ratio, the ideal
experience in the next financial year. ratio for a particular scheme will depend
on its current circumstances, such as:
However, where the adverse experience ■■the current adequacy of contributions
occurs in the second half of the year, ■■the level of non-healthcare expenses
it cannot be allowed for in the pricing ■■the need for reserve building
of benefits into the next year, and so ■■the scheme’s long-term strategy
this adverse experience must be made
up in the following year. In addition, The graph below illustrates the average
the adverse experience in the second claims paid per beneficiary per month
half of the year has a direct impact on (PBPM), as well as the risk claims ratio
the reserves and solvency levels of the in 2016, for the 20 schemes included
scheme going into the next year. in the Diagnosis this year. These claims
ratios all include any managed care fees
In general, medical schemes with a incurred by the schemes.
risk claims ratio of above 85% face the
challenge of achieving an operating
Claims and contributions by scheme
R2 200 100%
R2 000 95%
Average contribution/claim per beneficiary per month (PBPM)
R1 800 90%
R1 600 85%
R1 400 80%
Risk claims ratio
R1 200 75%
R1 000 70%
R800 65%
R600 60%
R400 55%
R200 50%
R0 45%
ry
s
m
ed
p
ld
lth
e
lth
ed
S
ed
ed
lth
lth
ED
ed
ed
p
ed
ta
zw
el
ou
M
ve
tu
ie
m
m
lm
km
sm
m
lm
ea
ea
ea
ea
ni
M
ih
GE
sh
Si
gr
co
en
st
os
of
Bo
U
ed
dh
H
Po
H
H
so
an
n
ed
ed
Be
s
Pr
om
H
W
y
Ba
Sa
Di
LA
m
M
Fe
Ke
Tr
N
M
M
u
M
SA
in
at
Pl
Average contributions PBPM Average claims PBPM 2016 claims ratio
24DIAGNOSIS 2017/2018
While the claims ratios show the (age profile and pensioner ratio), the to use some of those reserves, while
adequacy of contribution levels, incidence and distribution of disease a scheme which does not meet the
the actual average claims paid per (often called disease burden) and statutory solvency requirements may
beneficiary indicate the level of benefits advances in diagnostic technology have higher contributions than their
provided by a scheme. The graph on and biological drugs. The actual demographic and claims profile would
the previous page shows that KeyHealth cost of claims can be influenced by require to build reserves.
paid the highest amount in claims the negotiating power of a particular
per beneficiary in 2016, and also had medical scheme or its administrator. 2.7 Non-healthcare
the highest contribution income per
beneficiary during the year. Nedgroup The level of the average claims and expenditure
experienced the highest claims ratio of contributions per beneficiary for a
Non-healthcare expenditure (NHE)
these schemes, with a claims ratio of particular scheme will depend on a
includes administration fees, broker
99.4% for the 2016 year. Transmed had number of factors, including the richness
commission, distribution costs, bad
a high claims ratio of 105.3% in 2015, of benefits offered, the split of members
debts, and reinsurance costs. Up to
but managed to reduce this to 85.2% between high-cover and low-cover
2014 managed care fees were reported
for 2016. LA Health had a claims ratio options as well as the demographic
as part of non-healthcare expenditure.
of 82.9% for 2016, the lowest claims profile of the scheme in terms of average
However, since 2015 managed care
ratio of the 20 schemes considered. age and chronic prevalence. The
fees have been recognised as part of
relationship between contributions and
healthcare expenditure, which means
The actual healthcare costs funded by claims for a particular medical scheme
that there is a marked reduction in the
medical schemes are driven largely by will depend on the pricing philosophy
proportion of gross contribution income
the use of services as well as the actual followed by that scheme. A scheme
spent on NHE from 2014 to 2015.
cost of claims. The use of services is with a significant level of reserves might
influenced by demographic factors intentionally price for an operating deficit
25ALEXANDER FORBES HEALTH
Trend in non-healthcare expenditure
20%
18%
Managed care fees were
excluded from non-healthcare
expenditure from 2015.
16%
14%
12%
NHE as a % of GCI
10%
8%
6%
4%
2%
0%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
All medical schemes Open medical schemes Restricted medical schemes 10% line
Total non-healthcare expenditure, as a Restricted schemes are expected paid to NHE to decrease over time,
proportion of gross contribution income, to have lower non-healthcare costs irrespective of whether additional cost
increased marginally in 2016 for the primarily because they have lower or control measures are introduced. In
medical schemes industry as a whole. no distribution expenses or broker fees addition, broker fees paid each year
This increase was driven by an increase and certain operating expenses may may not increase at the same rate as
from 6.0% to 6.3% in the proportion be subsidised by their participating contributions because of the cap in place
of gross contribution income spent on employers. Some restricted schemes, that does not increase at healthcare cost
non-healthcare expenditure by restricted for example Profmed and GEMS, do inflation, which also contributes to the
medical schemes. For open schemes, compete with the open market to a decreased NHE percentage. As a result,
the NHE proportional spend reduced certain extent, and as a result will a more suitable measure of NHE is the
from 10.4% to 10.2%. The lower level budget for marketing expenses and absolute cost per member.
of non-healthcare expenditure within possibly broker fees.
restricted schemes is driven to a The graph on the next page illustrates
large extent by GEMS whose As we assume that NHE increases with the components of NHE for the top 10
non-healthcare expenditure was 5.6% CPI while contributions increase with open and top 10 restricted schemes for
of gross contribution income in 2016, medical inflation, which is usually 2% 2016, as well as for open and restricted
up from 5.0% in 2015. to 3% more than CPI on average each schemes, and the medical schemes
year, we would expect the proportion industry as a whole.
26DIAGNOSIS 2017/2018
Non-healthcare expenditure by scheme
R500 20%
R450 18%
R400 16%
R350 14%
NHE per member per month
NHE as a % of GCI
R300 12%
R250 10%
R200 8%
R150 6%
R100 4%
R50 2%
R0 0%
y
s
m
ed
p
ld
lth
e
lth
ed
S
ed
ed
lth
lth
ED
ed
ed
p
ed
en
d
ry
er
ta
zw
el
ou
te
M
st
tu
ie
m
m
lm
m
m
m
lm
Op
ea
ea
ea
ea
ov
ni
M
ih
ric
GE
du
sh
Si
gr
en
st
os
nk
ns
of
Bo
U
ed
dh
yH
Po
H
H
so
sc
ed
st
ed
Be
In
Pr
om
H
W
a
Ba
Sa
Di
LA
um
M
Fe
Re
Ke
Tr
N
M
M
M
SA
in
at
Pl
Administration expenses Broker and marketing fees Bad debts or other operating expenses NHE as a % of GCI
The marked difference between There is no fixed definition for
non-healthcare expenses of open which expenses can be included as
and restricted medical schemes is administration fees, and this contributes
evident from the graph above. Even to the varied level of administration fees
after excluding broker fees, the across the market. Some administrators
pure administration costs of open may include services other than pure
and restricted medical schemes are administration, for example actuarial
significantly different. This may be due services, which will affect the overall
to the sponsoring employers of the profile of administration expenses.
restricted schemes taking on some of the
expenses incurred in the running of the
medical scheme through the corporate
entity, and so reducing the costs borne
by the medical scheme itself.
27ALEXANDER FORBES HEALTH
The figure below shows the breakdown of non-healthcare expenditure into its different components across the industry in 2016.
84.2%
administration fees
R
Breakdown of
non-healthcare 1.7% 14.1%
expenditure bad debts broker fees (and marketing)
2.8 Financial performance
One of the key factors used to measure 2016, with the industry as a whole
the performance of a medical scheme experiencing an operating deficit of
is the scheme’s operating result. R2.390 billion in 2016. Restricted
A scheme’s operating result is an schemes incurred an operating deficit
indication of its financial soundness after of R1.435 billion while open schemes
claims and non-healthcare expenditure incurred an operating deficit of R0.956
are deducted from contribution income. billion. In 2014 the industry ended
It shows the surplus or deficit before the year with an operating deficit
investment income. of R464.51 million, with restricted
schemes attaining an overall operating
Drivers of strong financial performance deficit of R504.58 million and open
by medical schemes include: medical schemes achieving a small
■■appropriate benefit pricing operating surplus of R40.07 million. The
■■adequate risk management and industry ended 2015 with a significant
claims control operating deficit of R1.219 billion, with
■■favourable age and risk profile of the open schemes recording a deficit of
membership base R565.63 million at an operational level
■■low non-healthcare expenditure and restricted schemes showing a
deficit of R653.78 million.
The trend of deteriorating financial
results that we have observed in the
industry since 2014 continued in
28DIAGNOSIS 2017/2018
Trend in operating results
R3 000
R2 000
R1 000
Operating result (R million)
R0
-R1 000
-R2 000
-R3 000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Open medical schemes Restricted medical schemes All medical schemes
29ALEXANDER FORBES HEALTH
The longer-term trend in operating In 2015, 8 of 23 open schemes and overall net surplus of R1.391 billion
results since 2000 has been driven in 26 of 60 restricted schemes achieved (2015: R1.353 billion) and restricted
large part by the prevailing regulations. an operating surplus. In 2016, 5 of 22 schemes achieved an overall net
Medical schemes were priced to target open schemes and 23 of 60 restricted surplus of R 0.751 billion (2015:
significant surpluses in the years prior schemes achieved an operating surplus. R1.164 billion).
to 2004 in order to meet the regulatory
solvency requirements by 2004. During Schemes incurring operating deficits In 2015, 17 of 23 open schemes and
the years following 2004 many schemes have to rely on investment income 50 of 60 restricted schemes achieved
had met the solvency requirements to achieve a breakeven result on a a net surplus, compared to 12 of 22
and so no longer had to price for larger net level. In 2016, with the addition open schemes and 45 of 60 restricted
surpluses. They were, however, then of investment and other income, the schemes in 2016.
faced with significant increases in industry achieved a net surplus of
claims over the following years as a R2.142 billion, compared to the overall
result of a change in service provider net surplus of R 2.517 billion achieved
charging habits with the requirement to in 2015. Open schemes achieved an
pay PMBs at costs.
Trend in net surplus
R6 000
R5 500
R5 000
R4 500
R4 000
R3 500
Net surplus (R million)
R3 000
R2 500
R2 000
R1 500
R1 000
R500
R0
-R500
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Open medical schemes Restricted medical schemes All medical schemes
30DIAGNOSIS 2017/2018
The graph below shows the financial performance of the top 10 open schemes and top 10 restricted schemes in 2016.
Of the 20 schemes considered in this year’s Diagnosis, 13 did not attain a surplus at an operating level in 2016 and therefore had
to rely on investment income to subsidise claims and non-healthcare expenditure. Four of the 10 open schemes and one of the
10 restricted schemes also did not attain a surplus at a net result level, and so were net disinvestors for the 2016 benefit year.
Schemes' financial performance for 2016
R1 500
R1 000
Operating or net result (R million)
R500
R0
-R500
-R1 000
y
s
m
ed
p
ld
lth
e
lth
ed
S
ed
ed
lth
lth
ED
ed
ed
p
ed
er
ta
zw
el
ou
M
tu
ie
m
m
lm
m
m
m
lm
ea
ea
ea
ea
ov
ni
M
ih
GE
sh
Si
gr
en
st
os
nk
ns
of
Bo
U
ed
dh
yH
Po
H
H
so
sc
ed
ed
Be
Pr
om
H
W
a
Ba
Sa
Di
LA
um
M
Fe
Ke
Tr
N
M
M
M
SA
in
at
Pl
Operating result Net result
31ALEXANDER FORBES HEALTH
2.9 Investments
Where medical schemes do not achieve This strategy is not sustainable unless
operating surpluses, they become investment returns are able to keep
reliant on the investment returns earned pace with, and preferably exceed,
over the year to fund part of their claims claims inflation. At present, however,
and non-healthcare expenditure. In most medical schemes follow very
2016, 54 of 82 medical schemes conservative investment strategies
failed to achieve an operating surplus as shown in the following graph.
and therefore had to draw on their The graph shows the asset allocation
investment returns, placing additional for the 20 schemes under consideration
pressure on solvency levels. in this publication.
Asset allocation at 31 December 2016
100% 60%
90%
50%
80%
70% 40%
60%
Asset allocation
30%
Solvency
50%
20%
40%
30% 10%
20%
0%
10%
0% -10%
y
s
m
ed
p
ld
lth
e
lth
ed
S
ed
ed
lth
lth
ED
ed
ed
up
ed
er
ta
zw
el
M
tu
ie
m
m
lm
m
sm
m
lm
o
ea
ea
ea
ea
ov
ni
M
ih
GE
sh
Si
gr
en
st
os
nk
of
Bo
U
ed
dh
H
Po
H
H
so
sc
an
ed
ed
Be
Pr
om
H
W
y
Ba
Sa
Di
LA
um
M
Fe
Ke
Tr
N
M
M
M
SA
in
at
Pl
Cash and money market Bonds Equities Property Collective investment vehicles Foreign assets Other Solvency
32DIAGNOSIS 2017/2018
In 2016 open schemes held 18.7% of In particular, claims expenditure tends
assets in equites, with 33.7% being held to grow faster than CPI. To maintain
in bonds and 40.1% of assets being solvency year on year, the accumulated
held in cash. In the restricted scheme funds need to increase in line with the
environment, schemes held 22.1% of increase in contributions. If investment
assets in equities, 20.6% in bonds and returns cannot keep pace with the
50.7% in cash or cash equivalents. increase in claims inflation and
The balance is held in property mainly, accumulated funds increase at a rate
with some exposure to debentures and less than contributions, then solvency
insurance policies. levels will decrease, resulting in a need
to either increase contributions further –
There are asset class limits placed on which would exacerbate this issue – or
medical schemes in Annexure B of the reduce benefits.
Regulations to the Medical Schemes
Act, but most schemes are operating As a result, for schemes failing to
well inside the limits for riskier asset meet the solvency requirement, low
classes. The limit on equities is 40%, investment returns as a result of
while the limit on property is 10%. This conservative asset allocations may in
implies that schemes could have up fact be increasing risk for the scheme.
to 50% of their investments in these For schemes meeting the solvency
higher-risk asset classes, whose returns threshold, this can be eroded over time
are generally expected to exceed CPI if returns are below claims inflation, and
inflation. The allowable exposure to they may be missing an opportunity
conservative asset classes, such as to maintain affordable contribution
cash, money market instruments and increases in the future.
bonds, is unlimited. The only restrictions
on these asset classes are on the Where a scheme already has sufficient
exposure to specific issuers, to ensure reserves, there is a strong argument to
some level of diversification. invest at least some of the reserves in
more risky asset classes as allowed by
Medical schemes’ preference for cash Regulation B. Conversely, schemes that
in particular appears to be driven by a are not adequately funded can increase
preference for liquid assets, given the their expected return by investing
short-term nature of medical scheme in more risky assets, which will then
liabilities, as well as concerns about increase the reserves held and thereby
risks related directly to the investments the solvency ratio. This also depends on
(the possibility of making negative the absolute value of the asset base.
returns or losing scheme assets).
However, for the long-term sustainability
of the scheme, average returns below
medical inflation may pose a greater
risk, especially for schemes that rely
on investment returns when they fail to
achieve an operating surplus.
33You can also read