"Documentation Proliferation" Effect in Electronic Medical Records
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

“Documentation Proliferation” Effect in Electronic
Medical Records
Adele Towers, MD and Mark Morsch, MS
DISCLAIMER: The views and opinions expressed in this presentation are those of the author and do not necessarily represent official policy or position of HIMSS.
Conflict of Interest Disclosure
Adele Towers, MD, MPH
• Salary: N/A
• Royalty: N/A
• Receipt of Intellectual Property Rights/Patent Holder: N/A
• Consulting Fees (e.g., advisory boards): N/A
• Fees for Non-CME Services Received Directly from a Commercial Interest or their Agents (e.g.,
speakers’ bureau): N/A
• Contracted Research: N/A
• Ownership Interest (stocks, stock options or other ownership interest excluding diversified mutual
funds): N/A
• Other: UPMC has a financial interest in the Optum Clinical Documentation Improvement Module
2 © 2013 HIMSS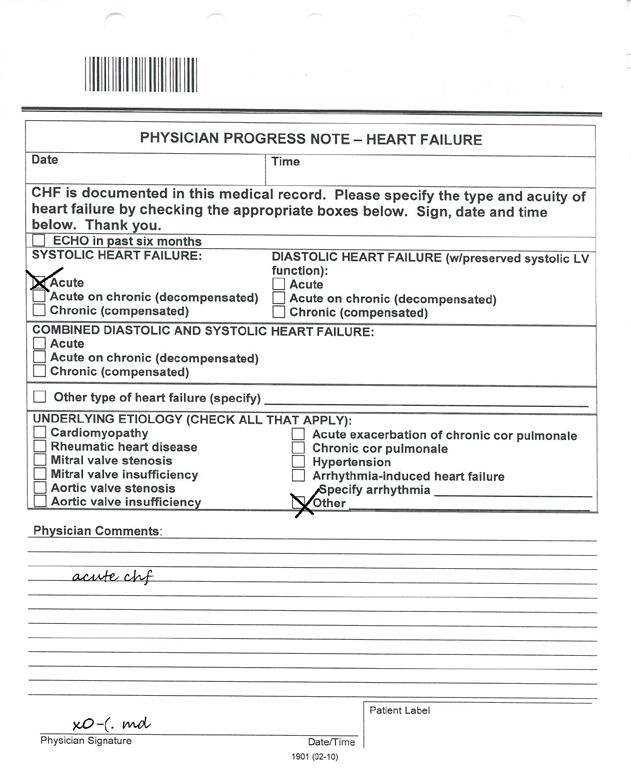
Conflict of Interest Disclosure
Mark Morsch, MS
• Salary: OptumInsight
• Royalty: N/A
• Receipt of Intellectual Property Rights/Patent Holder: N/A
• Consulting Fees (e.g., advisory boards): N/A
• Fees for Non-CME Services Received Directly from a Commercial Interest or their Agents (e.g.,
speakers’ bureau): N/A
• Contracted Research: N/A
• Ownership Interest (stocks, stock options or other ownership interest excluding diversified mutual
funds): United Health Group
• Other: N/A
3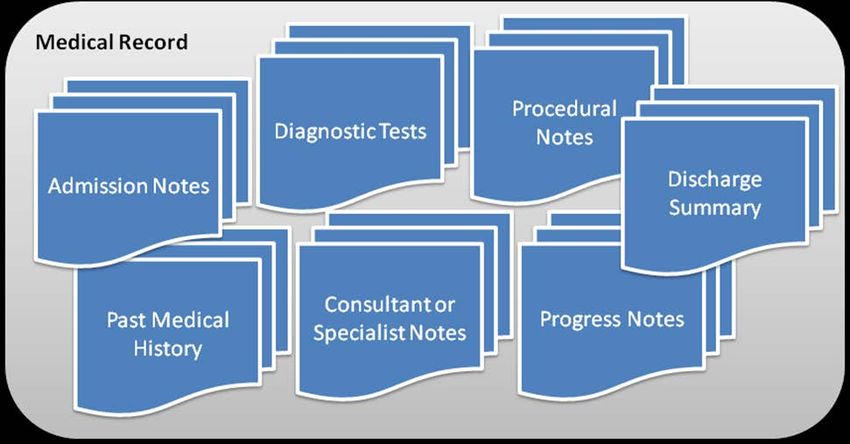
Learning Objectives • Define the challenge of documentation proliferation in electronic medical records (EMR) • Describe how Natural Language Processing (NLP) technology parses and analyzes the medical record and recognizes components of ICD-9 and ICD-10 codes • Explain how natural language processing can help organizations find EMR documentation deficiencies before patient discharge 4
About University of Pittsburgh Medical Center
• UPMC is one of the leading nonprofit health
systems in the United States, headquartered in
Pittsburgh, Pennsylvania.
• UPMC’s unique strategy of combining clinical and
research excellence with business-like discipline
translates into high-quality patient care.
• UPMC is Pennsylvania’s largest employer,
with more than 55,000 employees.
UPMC Quick Facts
Hospitals 20
Average Daily Census PUH: 626
SHY: 392
Inpatient Discharges Per Year PUH: 34,267
SHY: 24,980
Surgeries Per Year PUH: 23,540
SHY: 20,126
ED Visits Per Year PUH: 57,804
SHY: 39,686
5
EMR Environment at UPMC
• Cerner, HPF, MARS
• Cerner PowerNotes –
– 100% electronic at one facility
– 50% electronic at other 2 facilities
• CAC since Sept 6, 2008
• Medipac billing system
6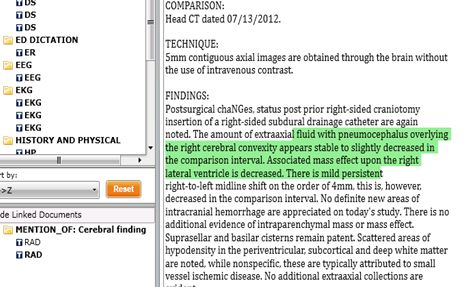
Documentation Gaps in the EMR • Cut & paste phenomenon – new information often buried • When doctors type – they don’t include much information • Symptoms not diagnosis are documented • Doctors can’t find correct diagnosis from pick-list • Need to communicate with physician in their workflow 7
Financial Impact • UPMC captures $12 million per year from retrospective review of medical records • 2011 external documentation audit of UPMC’s records showed that the system was losing $17.8 million per year despite best effort of current retrospective process • Audit confirmed that since the system had moved from paper to electronic records, the case mix index (CMI) had decreased • Typically means hospitals aren’t getting paid as much due to lower documented severity of illness. 8
Clinical Documentation Improvement (CDI) • Seeks to improve the quality of provider documentation to more accurately reflect services rendered. • Important consideration in the transition to ICD-10. • Address potential gap between the content of clinical documentation and the required specificity for ICD- 10 coding. • Concurrent CDI is a proactive approach, identifying and correcting potential documentation deficiencies during the patient’s stay. 9
Case Finding is Often a Wasted Effort
ACDIS CDI Staffing Survey*:
• CDI specialists conduct 8-12 new reviews per day.
• Each CDI specialist spends between 33 and 48 minutes per initial review.
• Average salary for CDI Specialist $60K/yr. ($28.84/hour) Source: Simply Hired
Percent of Reviews Resulting
in a Query Percent of Respondents
0–10% 7%
87% of respondents
11–20% 22%Transforming CDI with NLP
• Natural language processing (NLP) is transforming HIM
& coding with computer-assisted coding (CAC) solutions
– Benefits - Productivity, accuracy, efficiency, transparency,
manageability
– CDI programs shares these same goals
– Harness the power of CAC to drive CDI
• However CAC is not the same as CDI
• Not limited to finding only “code-able” facts, but clinically
significant events that are evidence of an information
gap
11Natural language processing and CAC
Computer
Science
Medical
Linguistics
Coding
12Natural language processing and CAC
NLP for
CAC NLP
Computer
Science
Medical
Linguistics
Coding
13Natural language processing and CDI
NLP for
CAC
CDI NLP
Computer
Science
More
General Medical
Linguistics
Coding
Medical
Knowledge
14Factors Aligning NLP with CDI 1. Accurate abstraction of medical evidence to automate case-finding 2. Clinical information model that supports consistent query decisions 3. Compositional approaches to NLP to recognize complex query scenarios 15
Case Finding Automation with NLP
• NLP can extract the clinical evidence that indicate gaps in
documentation
• Like in CAC, recall and precision are important measures of accuracy
– Goal is high recall and high precision
– High recall ensures that a high proportion of relevant clinical events
are captured
– Capture important facts that can escape manual processes
– High precision means CDI specialists don’t waste time reviewing
cases that don’t have gaps
• Comparing CDI evidence to CAC results provides automated validation
16Alpha Testing – NLP Case Finding Precision
n=308 cases with 387 total markers
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
17CDI Information Model
• Consistent results require a well-defined set of policies
with training and audit programs
• Use evidence-based criteria and national definitions to
create markers
• Ensure information is abstracted and interpreted
following standard guidelines
• Standardized information model for CDI
– Sound basis to construct queries
– Reduce variability in interpretation of potential CDI scenarios
– Drive requirements for NLP abstraction and business rules to
combine data elements
18Three Tier Information Model
Marker
Marker •Marker Source=CDI
•Marker Label = Condition or Procedure
•Marker Type = Type of Marker
•Strength = High, Medium, Low
•SNOMED Concept ID = simple or complex
SNOMED representation
Scenario Scenario
Scenario – a group of indicators that
indicate the reason for the Marker
•Scenario Label
•Strength
Indicator Indicator Indicator •SNOMED Concept ID
Indicator
•Indicator Label
•Indicator Type
•Finding or lab or vital or meds or supplies with full inherited output
•SNOMED Concept ID
19Compositional Approach to NLP
• NLP for CDI cannot solely rely on narrative text
• Lab orders or results, radiology reports, medication
orders, and vital signs are all important sources of CDI
evidence that are often structured data
• CDI markers are formed by logical combinations of
indicators
• Two advanced forms of linguistics are important
– Pragmatics to recognize how context contributes to
meaning
– Discourse analysis to synthesize meaning from
multiple sources
20Pragmatics
What is the context?
- Low sodium value
-Patient completed
marathon today
21Discourse Analysis
What are the broader meanings?
Current New or Existing Problem?
Symptoms
Findings Relevant or
Medical Incidental?
History
Diagnosis Complicated by
Findings Chronic Condition?
Which Symptoms Related
Diagnosis to Final Diagnosis?
How is the Treatment
Treatment Supported by Medical
Evidence?
22Two types of CDI opportunities NLP must be
able to handle
Example 1: Specificity Example 2: Clinical Clarity
Physician documents “CHF improving.” Physician documents “fluid retention and
shortness of breath improving.”
NLP Identifies NLP Identifies
• “CHF” in History and Physical • Pulmonary Vascular Congestion in CXR
• “CHF” in progress note • Ejection Fraction ofWorkflow
Concurrent CDI Case Finding
Business Rules Logic
Continuous
processing of the If a case is marked for CDI, Passive Query Building
ensure it conforms to business
EMR data through rules for presentation to a user:
Query passively built with
NLP to both code Financial Class Revenue Code
minimal (if any) additional
Physician Service Location
and apply case editing and update required
finding rules to each How should it be routed? by CDIS
admission. Directly to physician? Peer Advisor
CDI Specialist CDI Manager Presentation to physician
Specific User Coder
either interfaced to EMR,
Inbox or via PQRT Portal.
Query Response Returned to NLP
24System Built Queries vs.
Manually Built
Dear Dr.
What kind
of CHF is
being
treated?
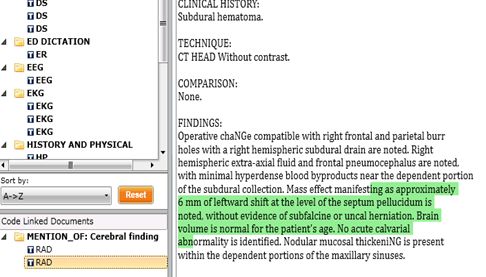
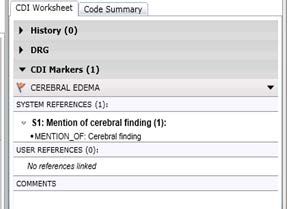
25EMR Case Example
CEREBRAL EDEMA
26CDI Marker – Mention of Cerebral Finding 27
First Radiology Finding 28
Second Radiology Finding 29
Swelling Noted in Operative Note 30
Code Selection Financial Impact
Original Post NLP/Rules Engine
DRG 27 25
CC/MCC NA 348.5
Reimbursement $12,912.58 $29, 798.65
Severity of Illness 1 2
31Conclusions
• Challenges of EMR documentation
• Clinical Documentation Improvement programs can
address documentation gaps
• Three key factors aligning NLP and CDI
– Case finding automation
– Clinical information model
– Compositional NLP
• Concurrent CDI workflow integrated with electronic
physician query
• Encouraging early results from alpha testing
32Thank You!
• Contact Information
– Adele Towers - TowersAL@upmc.edu
– Mark Morsch - mmorsch@alifemedical.com
33You can also read