DOUBLE BLIND CONTROLLED STUDY OF ADDING FOLIC ACID TO FLUOXETINE IN THE TREATMENT OF OCD
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Psychiatria Danubina, 2019; Vol. 31, No. 1, pp 69-77 https://doi.org/10.24869/psyd.2019.69 Original paper
© Medicinska naklada - Zagreb, Croatia
DOUBLE BLIND CONTROLLED STUDY OF ADDING FOLIC ACID
TO FLUOXETINE IN THE TREATMENT OF OCD
Ümit Tural1, Aytül Çorapçıo÷lu2, ùükriye Boúgelmez2, Gültürk Köro÷lu2, Hatice Ünver3,
Can Duman4 & Emin Önder2
1
Department of Psychiatry, The Nathan S. Kline Psychiatric Research Institute, Orangeburg, New York, USA
2
Department of Psychiatry, Medical Faculty at the University of Kocaeli, Umuttepe Kocaeli, Turkey
3
Department of Child and Adolescent Psychiatry, Medical Faculty at the University of Marmara, Istanbul, Turkey
4
Department of Biochemistry, Medical Faculty at the University of Kocaeli, Umuttepe, Kocaeli, Turkey
received: 17.8.2018; revised: 3.11.2018; accepted: 29.11.2018
SUMMARY
Background: Folate is important for the synthesis of serotonin the neurotransmitter which plays a main role in OCD. We,
therefore, explored the efficacy of folic acid as add on treatment to fluoxetine in a double blind study among patients with OCD.
Subjects and methods: A double blind, 12-week study comparing the efficacy of folic acid as add on treatment and placebo in
patients with OCD was conducted on thirty six (36) patients. Patients were randomly assigned to folic acid (5 mg/day) or placebo
group in addition to fluoxetine (40 mg/day). After the baseline assessment, on week 2, 4, 6, 8 and 12 assessments were performed by
using YBOCS, HAM-D, HAM-A and CGI-S. Serum folate, erythrocyte folate, serum homocysteine and B12 levels were measured both
baseline and the end of study.
Results: A mixed model repeated measures ANCOVA on Y-BOCS scores were used to determine the difference between folic acid
and placebo groups. No significant differences were found in the ratios of gender or in the mean age, serum folic acid level, erythro-
cyte folate level, serum homocysteine level and serum B12 level between the treatment groups at the baseline. Consecutively scores
collected over six measurements on YBOCS, HAM-D, HAM-A and CGI showed non-significant differences between folic acid and
placebo groups.
Conclusion: None of the biological markers of one carbon metabolism were associated with the change in YBOCS scores. It may
be assumed that there is no beneficial effect of folic acid addition to fluoxetine in the treatment of OCD.
Key words: OCD - fluoxetine - serum folate - red cell folate - serum homocysteine - vitamin B12
* * * * *
INTRODUCTION trolled study (Godfrey et al. 1990). Coppen & Bailey
(2000) demonstrated that the co-administration of folic
Low levels of folate and vitamin B12 have been asso- acid substantially and significantly improve the res-
ciated with low levels of serotonin metabolite 5-hydro- ponse to fluoxetine in female depressed patients but not
xyindolacetic acid (5-HIAA) in cerebrospinal fluid in in male. Papakostas and colleagues found a relationship
humans as well as in rats (Botez et al. 1979, Botez et al. between serum folate level and the timing of impro-
1982). Furthermore, low to deficient levels of folate in vement with fluoxetine, resistance to medication, and
serum and erythrocytes have been associated with relapse during the continuation phase of pharmaco-
depressive disorders, greater severity of depression, low therapy (Papakostas et al. 2005, Papakostas et al. 2004,
or delayed response rate to antidepressants, and in- Papakostas et al. 2004).
creased relapse rates (Abou-Saleh et al. 1986, Carney et Folate appears to influence the rate of synthesis of
al. 1990, Fava et al. 1997, Abou- Saleh & Coppen 1989, tetrahydrobiopterin, the cofactor in the hydroxylation of
Bottiglieri et al. 1992, Bottiglieri et al. 2000, Coppen et phenylalanine and tryptophan (Coppen et al. 1989,
al. 1989, Coppen & Bailey 2000, Papakostas et al. 2005, Bottiglieri & Hayland 1994, Hamon et al. 1986). Be-
Papakostas et al. 2004, Papakostas et al. 2004, Tol- cause this is the rate limiting step in the biosynthesis of
munen et al. 2004, Wilkinson et al. 1994). Studies have dopamine, norepinephrine and serotonin, alterations in
been suggesting that folic acid and its derivates can be the rate of synthesis of this important cofactor may be
used in the treatment of depression as add-on treatment relevant to depression or other psychiatric disorders
(Coppen & Bailey 2000, Guaraldi et al. 1993, Di Palma such as obsessive compulsive disorder (OCD). It has
et al. 1994, Alpert et al. 2002). Previously, it was shown hypothesized that OCD may be associated with seroto-
that methyfolate (5-methyltetrahydrofolate- MTHF), a ninergic dysfunction, and the clinical effects of selective
derivate of folate which is actively transportted into serotonin reuptake inhibitors (SSRIs) may suggest an
central nervous system-CNS) significantly improved the indirect role of serotonin in obsessions and compulsions
outcome of depressed patients with definite or just bor- (Lee et al. 2018, Sinopoli et al. 2017, Van Praag 1982,
derline folate deficiency after addition of –to standard Westenberg et al. 2007). Methyltetrahydrofolate has
psychotropic treatment in a double-blind, placebo-con- been shown to bind to presynaptic glutamate receptors,
69Ümit Tural, Aytül Çorapçıo÷lu, ùükriye Boúgelmez, Gültürk Köro÷lu, Hatice Ünver, Can Duman & Emin Önder: DOUBLE BLIND CONTROLLED
STUDY OF ADDING FOLIC ACID TO FLUOXETINE IN THE TREATMENT OF OCD Psychiatria Danubina, 2019; Vol. 31, No. 1, pp 69-77
where it may bind to presynaptic glutamate receptors, checking with the patient and his/her caregiver along
potentially modulate the release of other neurotrans- with a pill count at each visit. Patients were excluded
mitters including the monoamines (Ruck et al. 1980). from study entry for the following reasons: having a
Furthermore, glutamatergic system may be involved in total score on the 17-item Hamilton Depression Rating
the neurochemical disturbances existing in OCD (Baxter Scale (HAM-D) of 12 or higher score, being a woman
2001, Coric et al. 2005). who was currently pregnant or lactating, being diag-
Clinical interventions commonly used for the treat- nosed with cerebrovascular disease, Parkinson’s Disease,
ment of OCD provide symptom improvement in about Alzheimer’s Disease, having a current or past diagnosis
40-60% of patients with OCD; however, there are a of schizophrenia, other psychotic disorders, manic or
considerable number of patients in whom enough hypomanic episode verified with medical records,
symptom reduction (20-40%) can not be obtained that diagnosed with recurrent depression, known poor or
indicate a need for the new pharmacological treatment non-response to previous treatment with fluoxetine,
options (Jenike 2004). Although, folate and B12 defi- having a DSM-IV-TR defined diagnosis of alcohol or
ciencies and disturbance of one-carbon metabolism or substance abuse and/or dependence in the past 6
use of folate and its derivates as an antidepressant or months, having a clinically relevant abnormal labora-
augmentation with folic acid of antidepressant drug tory test including megaloblastic anemia, having an
action are well studied in depression, such studies have unstable or severe physical illness, current ingestion of
not been done in OCD yet. There are a few studies of drugs known to affect homocysteine, B12, and folate
serum folate levels in patients with OCD. In a study, the levels (e.g. antiepileptic, lithium), receiving treatment
authors indicated that serum B12 levels were signi- with a depot neuroleptic within 1 month. Concomitantly
ficantly associated with OCD whereas folate levels did using any psychotropic medication was not permitted
not with OCD and other psychiatric disorders (Hermes other than alprazolam for sleep if needed. All previous
et al. 1988). A more recent study found both lowered psychotropic medications had been withdrawn for at
blood level of folate and increased blood level of least 1 week before sampling. After informed patient
homocysteine in comparison to healthy controls, and consent, baseline fasting blood samples were obtained
both folate and homocysteine were significantly corre- in all patients for examination of full blood count, liver
lated with symptom severity of OCD as assessed with function tests, routine urine tests, thyroid tests (TSH, T3,
Yale-Brown Obsessive Compulsive Scale (YBOCS) T4), serum and red blood cell folate, serum B12, and total
total score (Atmaca et al. 2005). Taken together that serum homocysteine. No dietary restrictions were impo-
strong evidence of benefits of folate in the treatment of sed. At the endpoint (week 12), fasting serum homo-
depression and results from a few studies suggesting a cysteine, B12, folate and RBC folate levels were re-
possibility of impaired one carbon metabolism in OCD, evaluated. At each follow up appointment, the patient
a study of serum homocysteine, B12, folate, and erythro- was questioned about any possible adverse effects of the
cyte folate concentrations in patients with OCD and medication. The study was approved by the local ethics
whether the co-administration of folic acid would aug- committee and registered (143-6/116).
ment the anti obsessive-compulsive action of fluoxetine
has been undertaken. Scales
All patients entering the study were rated on the
SUBJECTS AND METHODS clinical rating scales, the 17-item Hamilton Depression
Rating Scale (HAM-D), Hamilton Anxiety Scale (HAM-
Participants A), Yale-Brown Obsessive Compulsive Scale (YBOCS),
A randomized, double-blind parallel group, placebo Clinical Global Impression-Severity of Illness (CGI-S).
controlled trial completed in outpatient psychiatry clinic Psychometric assessments were performed at baseline,
of Kocaeli University. The participants and clinicians weeks 2, 4, 6, 8, and 12 by using all of the mentioned
were blinded to interventions after assignment. Forty scales. We explored and compared the “response” rates
patients with Diagnostic and Statistical Manual of between the placebo and folic acid group. A response
Mental Disorders, 4th Edition, Text Revision (DSM-IV- was defined as 30% or more drop in the end point
TR) diagnosis of OCD were randomly assigned to YBOCS total score as compared with baseline.
receive either a tablet of 5 mg folic acid or an identical Yale Brown Obsession Compulsion Scale was deve-
looking placebo tablet to take with their fluoxetine. loped to detect the character and severity of obsessive-
Computer based randomization procedure was used. All compulsive symptoms, and consists of two parts (Good-
patients were prescribed 20 mg of fluoxetine as starting man et al. 1989). Questions 1-5 evaluate severity of
dose. After the first week of fluoxetine treatment, the obsessions; questions 6-10 evaluate severity of compul-
dosage of fluoxetine optimized to 40 mg daily. No fur- sions. Validity and reliability in Turkish was made
ther effort was made to balance the samples, for example (Karamustafalıo÷lu et al. 1993).
according to gender or duration and severity of OCD, The Hamilton Anxiety Rating Scale (HAM-A) is a
during randomization process. The medication adhe- 14-item questionnaire to be rated by the clinician,
rence and patient compliance were assessed through assessing severity of generalized anxiety (Hamilton
70Ümit Tural, Aytül Çorapçıo÷lu, ùükriye Boúgelmez, Gültürk Köro÷lu, Hatice Ünver, Can Duman & Emin Önder: DOUBLE BLIND CONTROLLED
STUDY OF ADDING FOLIC ACID TO FLUOXETINE IN THE TREATMENT OF OCD Psychiatria Danubina, 2019; Vol. 31, No. 1, pp 69-77
1969). The validity and reliability of Turkish version difference was found by multivariate F test, then follow
was confirmed (Yazıcı et al. 1998). up univariate ANOVAs with Bonferroni adjustment for
Hamilton Depression Rating Scale was designed as type I error were performed. In the main analysis, the
a tool to measure the severity of illness inpatients diag- outcome (dependent) measure was observed changes in
nosed with depression (Hamilton 1967). The version of the total score of YBOCS, which had been collected
the instrument utilized in the study contains 17 items. over six measurements, between the two treatment
According to the options chosen by rater, each item arms. Because of gender differences, may have an effect
contributes a score of 0, 1, 2, 3, or 4 points toward a on the antidepressant responses (Coppen and Bailey,
HAM-D total. A 17-item HAM-D total score may theo- 2000, Martenyi et al. 2001) gender was added as a
retically range from 0 to 52. Its validity and reliability second “between-subjects factor” to the mixed model
for use with the Turkish population was done (Akdemir repeated measures of ANOVA to test the main
et al. 2001). hypothesis which allows us to evaluate both inclusive
and exclusive of the effects of gender. Preliminary
The Clinical Global Impression was developed and assumption testing for ANOVAs was conducted. All
published by National Institute of Mental Health in analyses were based on the ITT patient sample. The
1976, a brief instrument, comprising of two parts, the significance level was always set at 0.05 (two sided).
first being a clinician’s rating of the severity of the Partial Eta Square (etap2) was reported as an indicator of
disease (CGI-S), and the second for assessing general effect size for ANOVAs.
improvement or deterioration, and side effects of the
drugs (Guy 1976). In this study, we used the first part
that the severity of psychiatric symptoms was clinically RESULTS
assessed by means of CGI-S that gives a score ranging Sample
from 1 (disease free) to 7 (greatest severity possible).
Fifty eight patients were screened. Forty three pa-
tients with OCD were enrolled; however, seven patients
Biologic Assays
dropped out the study because of refusal to give a blood
The blood samples were taken from antecubital vein sample at the time of venipuncture (2 patients) or
between 9 and 11 AM after an overnight fast. Serum incomplete baseline psychiatric assessments (4 patients)
folate, erythrocyte folate and serum B12 levels were or violate the study agreement (1 patient). Therefore,
measured using ECLIA (Roche Diagnostics Elecsys remaining 36 patients were included in further statistical
2010 immune analyzer). Normal range for serum coba- analyses. The mean age of the whole group was
lamin was 197–866 pg/ml (145-637 pmol/L); for serum 32.6±10.9 years. There was no significant difference
folate was 3.1–17.5 ng/ml (7.0-39.7 nmol/L); for ery- between the ages of the two treatment groups (Table 1)
throcyte folate was 176-589 ng/ml (401-1338 nmol/L) or between the mean ages of men (n=14, 32.16±11.41
as established by the kit manufacturer. Plasma total L- yrs) and women (n=22, 31.86±10.71 yrs; t=-0.265,
homocysteine estimation was carried out using FPIA in df=34, P=0.793). Gender distribution was not signi-
the IMx system (Abbott Diagnostic, Abbott Park, IL, ficantly different between the treatment groups. None of
USA). Normal range for plasma total L-homocysteine the baseline psychometric or biochemical parameters
was 4.45-12.42 µmol/L as established by the kit was significantly different between the treatment groups
manufacturer. In the present study we analyzed the (Table 1). The comorbidities in OCD group were as fol-
results according to the standard lower limits of the lows: four patients with panic disorder, 2 patients with
normal range as suggested by the kit manufacturer, social phobia, 1 patient with generalized anxiety dis-
namely 197 pg/ml for cobalamin, 3.1 ng/ml for serum order, 1 patient with post-traumatic stress disorder.
folate, and 176 ng/ml for erythrocyte folate. All results
below these values were considered to be lower than Adverse effects
normal. If the value of plasma totals homocysteine
values higher than 12.42 µmol/L, it was accepted as Twelve out of 18 patients (66.7%) reported adverse
higher than normal. effects of the treatment in fluoxetine plus placebo
group; 6 patients reported a mild increase of anxiety
symptoms, 5 of headache, 2 of nausea, and 3 of in-
Statistical analysis
somnia. Fifteen patients (83.3%) reported adverse
Sociodemographic variables were assessed either effects of the treatment in fluoxetine+folic acid group;
with independent samples t-test for continuous variables 5 patients suffered from nausea, 4 from difficulty
or Chi square test for categorical variables. Yates’ concentrating, 4 from flatulence, 2 from gastrointe-
corrected chi-square or Fisher’s exact test were used stinal discomfort, 2 from reddened skin. Total adverse
when appropriate. Pearson or partial correlations were effects frequency was not significantly different bet-
used to explore the relationship between interested ween the groups (Ȥ2=0.593, df=1, P=0.441). Five (13.9%)
variables and the biochemical markers, MANOVA was of subjects withdrew from the study during follow up
used for comparing. Multivariate sample means period due to adverse effects (2 in flx+placebo, 3 in
between the placebo and folic acid groups. If significant flx+folic acid group).
71Ümit Tural, Aytül Çorapçıo÷lu, ùükriye Boúgelmez, Gültürk Köro÷lu, Hatice Ünver, Can Duman & Emin Önder: DOUBLE BLIND CONTROLLED
STUDY OF ADDING FOLIC ACID TO FLUOXETINE IN THE TREATMENT OF OCD Psychiatria Danubina, 2019; Vol. 31, No. 1, pp 69-77
Table 1. Baseline Comparisons between the Groups
Flx Alone Group Flx+Folic Acid Group Statistic and P value
Age (Mean±SD) 33.44±11.62 31.06±10.18 t=0.656, df=34, p=0.516
Gender (Female n, %) 12 (66.7%) 10 (55.6%) Ȥ2=0.117, df=1, p=0.732
HAM-D Score (Mean±SD) 6.06±3.08 6.17±2.73 t=-0.115, df=34, p=0.909
HAM-A Score (Mean±SD) 16.22±9.15 17.56±9.91 t=-0.419, df=34, p=0.678
Y-BOCS Score (Mean±SD) 24.78±8.41 27.89±5.97 t=1.280, df=34, p=0.209
CGI-S (Mean±SD) 4.44±1.25 4.94±0.873 t=-1.394, df=34, p=0.172
Serum folate, ng/ml (Mean±SD) 8.13±3.19 6.63±1.98
Erythrocyte folate, ng/ml (Mean±SD) 449.13±94.30 461.11±231.90 Pillai’s trace: F(4,31)=1.047,
Serum homocysteine, µmol/L(Mean±SD) 12.35±3.26 15.21±9.09 p=0.399, eta2=0.119
Serum B12, pg/ml (Mean±SD) 286.99±132.36 232.12±69.20
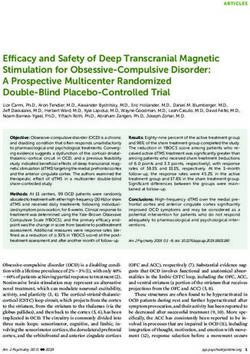
Figure 1. Changes in YBOCS total scores (error bars: 95% CI for mean)
Serum Folate, B12, Homocysteine, other biochemical markers. There was a medium and
and RBC folate levels at baseline negative correlation between blood level of B12 and Y-
BOCS total score (r=-0.396, n=31, P=0.022). However,
All of 36 patients’ serum folate levels were within there were no significant correlations between Y-BOCS
the normal range. However, 4 (11.1%) patients’ ery- total score and serum folate (r=-0.066, n=31, P=0.714),
throcyte folate levels were low, and 7 (19.4%) pa- homocysteine (r=-0.085, n=31, P=0.639), and erythro-
tients’ serum B12 levels were low according to the cyte folate level (r=-0.127, n=31, P=0.482).
reference intervals. Twenty one (58.3%) patients’ se-
rum total homocysteine levels were higher than upper Effect of the treatment on OCD severity
limits. One way between groups MANOVA was
performed to investigate the treatment group (placebo A mixed model repeated measures ANOVA ap-
vs. folic acid) differences in biochemical markers’ proach showed that there was a significant change in
serum levels at baseline. We found no baseline sig- YBOCS total scores collected over six assessments
nificant differences between the groups by means of (F(5,28)=7.683, PÜmit Tural, Aytül Çorapçıo÷lu, ùükriye Boúgelmez, Gültürk Köro÷lu, Hatice Ünver, Can Duman & Emin Önder: DOUBLE BLIND CONTROLLED
STUDY OF ADDING FOLIC ACID TO FLUOXETINE IN THE TREATMENT OF OCD Psychiatria Danubina, 2019; Vol. 31, No. 1, pp 69-77
Table 2. Effect of the treatment on biochemical parameters*
Variable Treatment Baseline Endpoint Comparisons
Group (Mean±SD) (Mean±SD) Within Groups Between Groups
Serum folate Placebo 8.13±3.19 8.04±3.08 F(1,17)=0.47, p=0.832,
(ng/ml) eta2=0.003 F(1,34)=75.962,
Folic acid 6.63±1.98 30.22±10.99 F(1,17)=77.506, pÜmit Tural, Aytül Çorapçıo÷lu, ùükriye Boúgelmez, Gültürk Köro÷lu, Hatice Ünver, Can Duman & Emin Önder: DOUBLE BLIND CONTROLLED
STUDY OF ADDING FOLIC ACID TO FLUOXETINE IN THE TREATMENT OF OCD Psychiatria Danubina, 2019; Vol. 31, No. 1, pp 69-77
ments. Multivariate tests’ results showed that neither met criteria for a lifetime diagnosis of major depression
significant main effect of the groups (F(15,480)=0.883, had folate concentrations in serum and RBCs, but not
P=0.583, etap2=0.027) nor main effect of gender serum total homocysteine concentration, were lower
(F(15,480)=0.295, P=0.996, etap2=0.009) or group x gender than those of subjects who had never been depressed
interaction (F(15,480)=0.614 P=0.864, etap2=0.019) in chan- after adjustment for sociodemographic and biochemical
ge of secondary psychometric scales’ scores (Table 3). factors (Morris et al. 2003). In this area, we can say that
Repeated measures ANCOVA showed that ¨ in the the traditional diets in western region of Turkey contain
biochemical markers (¨folate F(15,465)=1.103, P=0.350, a high proportion of green vegetables and are hence rich
etap2=0.034; ¨erythrocyte folate F(15,465)=0.671, P=0.813, in folate. This may explain why we could not find
etap2=0.021; ¨homocysteine F(15,465)=0.268, P=0.998, serum folate deficiency. Here, we should address the
etap2=0.009; ¨B12 F(15,465)=0.320, P=0.993, etap2=0.010) limitation that the dietary intakes of folic acid were not
were not significantly associated with secondary psycho- controlled in the study. Nevertheless, the present study’s
metric scales’ scores collected over six measurements. design limits us to discuss further on differences bet-
ween healthy group and patients with OCD due to non-
DISCUSSION inclusion of healthy comparison control group.
The biochemical mechanisms through which folate
To the best of our knowledge, there are no previous exerts an influence on neuropsychiatric status are sug-
studies in the literature regarding folate in the treatment gested to be likely to involve the one-carbon cycle, a
of OCD. But, the two studies merely exploring serum pathway essential to many transmethylation reactions
folate, B12 and homocysteine in OCD and found rela- within the CNS, including the metabolism of neuro-
tionship between those substances and symptoms of active substances such as the monoamine neurotrans-
OCD (Hermesh et al. 1988, Atmaca et al. 2005). In this mitters and melatonin, as well as the formation of
trial, we observed similar improvement in symptoms of membrane phospholipids, and the synthesis, repair, and
OCD between each of the two treatment arms (fluo- recombination of nucleic acids (Alpert & Fava 1997,
xetine+placebo vs. fluoxetine+folic acid co-administra- Fenech 2001, Young & Ghadirian 1989). Concordant
tion groups) with no significant superiority each other. with the preclinical research, it is well known that serum
Adding folic acid in fluoxetine had not significantly folate, B12 and homocysteine are strongly associated
better than fluoxetine+placebo group on both efficacy with depressive disorders (Tiemeier et al. 2002), alco-
measures (changes in Y-BOCS total scores and res- holism (De La Vega et al. 2001) and Alzheimer’s
ponse rate) even after adjusting for sex. Many resear- disease (Serot et al. 2001, Serot et al. 2005). We could
ches have been pointing out the beneficial effect of folic not replicate that serum folate deficiency, which have
acid add on treatment in depression (Carney et al. 1990, been previously reported for wide range of psychiatric
Fava et al. 1997, Abou-Saleh & Coppen 1989, disorders, in OCD; however, some of the other distur-
Bottiglieri et al. 1992, Bottiglieri et al. 2000, Coppen et bances (lowered erythrocyte folate level and or serum
al. 1989, Coppen & Bailey 2000, Papakostas et al. 2005, B12 level or increased serum total homocysteine) which
Papakostas et al. 2004, Papakostas et al. 2004, Wilkin- are relevant to one carbon cycle were found. It is
son et al. 1994, Guaraldi et al. 1993, Di Palma et al. interesting to find disturbances in homocysteine and
1994, Alpert et al. 2002, Godfrey et al. 1990, Bottiglieri erythrocyte folate levels whereas normal serum folate
& Hayland 1994), but we could not extend this to OCD. level. An explanation for that is a defective gene of
In the meanwhile, the findings of present study has not methylating enzyme 5, 10-methylenetetrahydrofolate re-
supported the previous study reported that change in ductase (MTHFR). Depressed patients are known to be
RCF is closely tied to response to antidepressant treat- at risk for MTHFR (C677T) polymorphism, which
ment (Levitt et al. 1998). Despite a few previous cross translates into lower serum levels of L-methylfolate and
sectional studies reporting lowered folate, B12 and possibly lower CNS folate, and thus lower monoamine
increased homocysteine levels in OCD (Hermesh et al. and increased homocysteine levels (Yang et al. 2008).
1988, Atmaca et al. 2005), none of our participants had Specific ethnic groups are at higher risk for the less
a baseline lower serum folate than the normal range. functional forms of MTHFR. For example, the T/T
The most reasonable explanation for this might be genotype is present in as many as 10% of whites, and up
culturally or locally defined dietary habits influence the to 22% of samples of Hispanic or Mediterranean popu-
relationship between the folate statuses in different lations (Arinami et al. 1997, Kelly et al. 2004). Although
societies. For example in Chinese patients with depress- many studies including a meta analysis found an asso-
sion had significantly lower serum folate than controls, ciation between MTHFR polymorphism and depression
but no subject in either group had low serum folate (Arinami et al. 1997, Kelly et al. 2004, Hickie et al.
according to their normal range? Conversely, patients 2001, Gilbody et al. 2007) one large (n=6.806) popula-
with depression significantly higher erythrocyte folate tion based cross sectional study examined the risk of
than control subjects (Lee et al. 2003). In a study exa- anxiety, using a validated self-report questionnaire, and
mines associations between depression and folate status found no association between MTHFR gene poly-
indicators in an ethnically diverse general US popu- morphism and anxiety disorders (Bjelland et al. 2003).
lation sample aged 15-39 years found that subjects who Similarly, none of the newly admitted patients with
74Ümit Tural, Aytül Çorapçıo÷lu, ùükriye Boúgelmez, Gültürk Köro÷lu, Hatice Ünver, Can Duman & Emin Önder: DOUBLE BLIND CONTROLLED
STUDY OF ADDING FOLIC ACID TO FLUOXETINE IN THE TREATMENT OF OCD Psychiatria Danubina, 2019; Vol. 31, No. 1, pp 69-77
anxiety disorders had lower serum B12 or folic acid tion groups) with no significant superiority each other.
levels which had been reported from Israel (Lerner et al. Adding folic acid in fluoxetine had not significantly
2006). However, the small number of individuals in the better than fluoxetine+placebo group on both efficacy
study could possibly explain the negative results. measures (changes in Y-BOCS total scores and res-
Homocysteine levels are also particularly high in ponse rate) even after adjusting for sex.
patients with schizophrenia, even in the absence of
dietary deficiency in folate or vitamin B12 (Regland et
al. 1995, Susser et al. 1998). The same is also true for
B12 (Lindenbaum et al. 1988). Similarly, increased post-
Acknowledgements:
prandial levels of homocysteine, but normal fasting This was an investigator-initiated study and partly
levels in depressive patients, were proposed to indicate supported by Lilly ølaç Ticaret A.ù, Turkey, and
some enzymatic defect (Candito et al. 1997). In this I.E.Ulugay. Lilly ølaç Ticaret A.ù. has afforded the
biochemical kits, I.E.Ulugay has offered free drug
point of view, it would be suggested that methylfolate
(folic acid) and matching placebo pills used in the
might be chosen in the future research as active mole- study.
cule for avoiding from confounding affect of MTHFR
polymorphism. Because of both folic acid and dihydro- Conflict of interest:
folate are not biologically active forms of folate, but are
Dr. Ümit Tural have given independent lectures at
essentially pro-drugs, and must undergo enzymatic
educational activities sponsored by Astra Zeneca,
transformation to L-methylfolate in order to be used by Janssen and Abdi øbrahim, companies for which he
cells, and unlike other forms of folate, L-methylfolate as received the honoraria were paid to the Department
bioactive derivate of folate readily crosses the blood- of Psychiatry, Medical Faculty, University of Kocaeli.
brain barrier for use in the CNS. Additionally, it was
previously shown that methylfolate significantly impro- Contribution of individual authors:
ved the outcome of depressed patients with definite or Ümit Tural had the study conception, designed the
just borderline folate deficiency after additions of – to study, performed statistical analyses and interpre-
standard psychotropic treatment in a double-blind, pla- tation of data, drafting of the manuscript and critical
cebo-controlled study (Godfrey et al. 1990). Later, revisions.
lower serum levels of methylfolate have been reported Aytül Çorapçıo÷lu & ùükriye Boúgelmez participated
among depressed subjects, although those levels were in collection and interpretation of data and drafting
not related to severity of depression before treatment of the manuscript.
and values remained markedly low even after a good Gültürk Köro÷lu & Hatice Ünver had literature searches
response to treatment (Wilkinson et al. 1994). and drafting the manuscript.
SSRI antidepressants are thought to work by stop- Can Duman has involved the acquisition and inter-
ping the reuptake of serotonin, thereby enhancing sero- pretation of data.
tonin action within the synapse which results in a thera- Emin Önder made critical revisions, approval of the
final version.
peutic efficacy in many psychiatric disorders. It seems
that the efficacy of folate in psychiatric disorders, es- All authors made important intellectual content to the
manuscript.
pecially depression, can not be simplified as increasing
the rate of serotonin synthesis. If this assumption was
true, then, we might have found that folate had increa-
sed the response rate or fasten the response when we
References
ignored the possible statistical insufficiency. Addi- 1. Abou-Saleh MT, Coppen A: The biology of folate in
tionally, the present study demonstrated that metabolites depression: implications for nutritional hypotheses of the
relevant to one carbon cycle are not associated with the psychoses. J Psychiatr Res 1986; 20:91-101
change in severity of OCD symptoms or treatment 2. Abou-Saleh MT, Coppen A: Serum and red blood cell
response to medication. Finally, limited statistical power folate in depression. Acta Psychiatr Scand 1989;80:78-82
because of the modest sample size in the present study 3. Akdemir A, Turkcapar MH, Orsel SD et al.: Reliability and
(N=36) may have played a role in limiting the signifi- validity of the Turkish version of the Hamilton Depression
cance of some of the statistical comparisons conducted. Rating Scale. Compr Psychiatry 2001; 42:161-165
4. Alpert JE, Fava M: Nutrition and depression: the role of
The readers should note as the limitations that the
folate. Nutr Rev 1997; 55:145-149
study has a relative small sample, not implemented a
5. Alpert JE, Mischoulon D, Rubenstein GE et al.: Folinic
dietary restriction, and not used methylfolate the active acid (Leucovorin) as an adjunctive treatment for SSRI-
metabolite of folate. refractory depression. Ann Clin Psych 2002; 14:33-38
6. Arinami T, Yamada N, Yamakawa-Kobayashi K et al.:
CONCLUSIONS Methylenetetrahydrofolate reductase variant and schizo-
phrenia/depression. Am J Med Genet 1997; 74:526-528
We observed similar improvement in symptoms of 7. Atmaca M, Tezcan E, Kuloglu M et al.: Serum folate and
OCD between each of the two treatment arms (fluo- homocysteine levels in patients with obsessive-compulsive
xetine+placebo vs. fluoxetine+folic acid co-administra- disorder. Psychiatry Clin Neurosci 2005; 59:616-620
75Ümit Tural, Aytül Çorapçıo÷lu, ùükriye Boúgelmez, Gültürk Köro÷lu, Hatice Ünver, Can Duman & Emin Önder: DOUBLE BLIND CONTROLLED
STUDY OF ADDING FOLIC ACID TO FLUOXETINE IN THE TREATMENT OF OCD Psychiatria Danubina, 2019; Vol. 31, No. 1, pp 69-77
8. Baxter LR: Functional imaging of brain systems mediating 27. Guaraldi GP, Fava M, Mazzi F et al.: An open trial of
obsessive-compulsive disorder. In: Charney DS, Nestler methyltetrahydrofolate in elderly depressed patients. Ann
EJ, Bunny BS, eds. Neurobiology of Mental Illness. New Clin Psychiatry 1993; 5:101-105
York: Oxford University Press, 2001; 534-547 28. Guy W: Early Clinical Drug Evaluation until Assessment
9. Bjelland I, Tell GS, Vollset SE et al.: Folate, vitamin B12, Manual for Psychopharmacology. Washington DC: US De-
homocysteine, and the MTHFR 677C->T polymorphism in partment of Health, Education and Welfare, 1976; 76-338
anxiety and depression: the Hordaland Homocysteine 29. Hamilton M: Development of a rating scale for primary
Study. Arch Gen Psychiatry 2003; 60:618-626 depressive illness. Br J Soc Clin Psychol 1967; 6:278–296
10. Botez MI, Young SN, Bachevalier J et al.: Folate 30. Hamilton M: Diagnosis and rating of anxiety. Br J
deficiency and decreased brain 5-hydroxytryptamine Psychiatry. 1969; 3:76–79.
synthesis in man and rat. Nature 1979; 278:182-183 31. Hamon CG, Blair JA, Barford PA: The effect of tetra-
11. Botez MI, Young SN, Bachevalier J et al.: Effect of folic hydrofolate on tetrahydrobiopterin metabolism. J Ment
acid and vitamin B12 deficiencies on 5-hydroxyindo- Defic Res 1986; 30:179-183
leacetic acid in human cerebrospinal fluid. Ann Neurol 32. Hermesh H, Weizman A, Shahar A et al.: Vitamin B12 and
1982; 12:479-484 folic acid serum levels in obsessive compulsive disorder.
12. Bottiglieri T, Hyland K, Laundy M et al.: Folate defi- Acta Psychiatr Scand 1988; 78:8–10
ciency, biopterin and monoamine metabolism in de- 33. Hickie I, Scott E, Naismith S et al.: Late-onset depression:
pression. Psychol Med 1992; 22:871-876 genetic, vascular and clinical contributions. Psychol Med
13. Bottiglieri T, Hyland K: S-adenosylmethionine levels in 2001; 31:1403-1412
psychiatric and neurological disorders: a review. Acta 34. Jenike MA: Clinical practice. Obsessive-compulsive
Neurol Scand 1994; 154(suppl):19-26 disorder. N Engl J Med 2004; 350:259-265
14. Bottiglieri T, Laundy M, Crellin R et al.: Homocysteine, 35. Karamustafalıo÷lu OK, Üçıúık AM, Ulusoy M et al.:
folate, methylation, and monoamine metabolism in depres- Validity and reliability study of Yale-Brown Obsession-
sion. J Neurol Neurosurg Psychiatry 2000; 69:228-232 Compulsion Scale. Poster presented at 29th Congress of
15. Candito M, Aubin-Brunet V, Beaulieu F et al.: Increased National Psychiatry Procedings Book. 1993:86 [Turkish]
postprandial homocysteinemia in a group of depressed 36. Kelly CB, McDonnell AP, Johnston TG et al.: The
patients. Amino Acids 1997; 12:315-321 MTHFR C677T polymorphism is associated with
16. Carney MW, Chary TK, Laundy M et al.: Red cell folate depressive episodes inpatients from Northern Ireland. J
concentrations in psychiatric patients. J Affect Disord Psychopharmacol 2004; 18:567–571
1990; 19:207-213 37. Lee J, Kim BH, Kim E et al.: Higher serotonin transporter
17. Coppen A, Swade C, Jones SA et al.: Depression and availability in early-onset obsessive-compulsive disorder
tetrahydrobiopterin: the folate connection. J Affect Disord patients undergoing escitalopram treatment: A [11C]DASB
1989; 16:103-107 PET study. Hum Psychopharmacol 2018; 33:e2642
18. Coppen A, Bailey J: Enhancement of the antidepressant 38. Lee S, Wing YK, Fong S: A controlled study of folate
action of fluoxetine by folic acid: a randomised, placebo levels in Chinese inpatients with major depression in
controlled trial. J Affect Disord 2000; 60:121-130 Hong Kong. J Affect Disord 1998; 49:73-77
19. Coric V, Taskiran S, Pittenger C et al.: Riluzole augment- 39. Lerner V, Kanevsky M, Dwolatzky T et al.: Vitamin B12
tation in treatment-resistant obsessive-compulsive disorder: and folate serum levels in newly admitted psychiatric
an open-label treatment. Biol Psychiatry 2005; 58:424-428 patients. Clinical Nutrition 2006; 25:60-67
20. De la Vega MJ, Santolaria F, Gonzalez-Reimers E et al.: 40. Levitt AJ, Wesson VA, Joffe RT: Impact of suppression of
High prevalence of hyperhomocysteinemia in chronic thyroxine on folate status during acute antidepressant
alcoholism: the importance of the thermolabile form of the therapy. Psychiatry Res 1998; 79:123-129
enzyme methylenetetrahydrofolate reductase (MTHFR). 41. Lindenbaum J, Healton EB, Savage DG et al.: Neuro-
Alcohol 2001; 25:59-67 psychiatric disorders caused by cobalamin deficiency in
21. Di Palma C, Urani R, Agricola R et al.: Is methylfolate the absence of anemia or macrocytosis. N Engl J Med
effective in relieving major depression in chronic 1988; 318:1720-1728
alcoholics? A hypothesis of treatment. Curr Ther Res Clin 42. Martenyi F, Dossenbach M, Mraz K et al.: Gender diffe-
Exp 1994; 55:559-568 rences in the efficacy of fluoxetine and maprotiline in de-
22. Fava M, Borus JS, Alpert JE et al.: Folate, vitamin B12, pressed patients: a double-blind trial of antidepressants
and homocysteine in major depressive disorder. Am J with serotonergic or norepinephrinergic reuptake inhibition
Psychiatry 1997; 154:426-428 profile. Eur Neuropsychopharmacol 2001; 11:227–232
23. Fenech M: The role of folic acid and Vitamin B12 in 43. Morris MS, Fava M, Jacques PF et al.: Depression and
genomic stability of human cells. Mutat Res 2001; folate status in the US Population. Psychother Psychosom
475:57-67 2003; 72:80-87
24. Gilbody S, Lewis S, Lightfoot T: Methylenetetrahydro- 44. Papakostas GI, Petersen T, Mischoulon D et al.: Serum
folate reductase (MTHFR) genetic polymorphisms and folate, vitamin B12, and homocysteine in major depressive
psychiatric disorders: a HuGE review. Am J Epidemiol disorder, Part 1: predictors of clinical response in
2007; 165:1-13 fluoxetine-resistant depression. J Clin Psychiatry 2004;
25. Godfrey PS, Toone BK, Carney MW et al.: Enhancement 65:1090-1095
of recovery from psychiatric illness by methylfolate. 45. Papakostas GI, Petersen T, Mischoulon D et al.: Serum
Lancet 1990; 336:392-395 folate, vitamin B12, and homocysteine in major depressive
26. Goodman W, Price LH, Steven A et al.: Yale-Brown disorder, Part 2: predictors of relapse during the
obsessive compulsive scale. I. Development, use, and continuation phase of pharmacotherapy. J Clin Psychiatry
reliability. Arch Gen Psychiatry 1989; 46:1006-1011 2004; 65:1096-1098
76Ümit Tural, Aytül Çorapçıo÷lu, ùükriye Boúgelmez, Gültürk Köro÷lu, Hatice Ünver, Can Duman & Emin Önder: DOUBLE BLIND CONTROLLED
STUDY OF ADDING FOLIC ACID TO FLUOXETINE IN THE TREATMENT OF OCD Psychiatria Danubina, 2019; Vol. 31, No. 1, pp 69-77
46. Papakostas GI, Petersen T, Lebowitz BD et al.: The 54. Tolmunen T, Hintikka J, Ruusunen A et al.: Dietary folate
relationship between serum folate, vitamin B12, and and the risk of depression in Finnish middle-aged men. A
homocysteine levels in major depressive disorder and the prospective follow-up study. Psychother Psychosom 2004;
timing of improvement with fluoxetine. Int J Neuro- 73:334-339
psychopharmacol 2005; 8:523-528 55. Van Praag HM: Depression, suicide and the metabolism
47. Regland B, Johansson BV, Grenfeldt B et al.: Homocystei- of serotonin in the brain. J Affect Disord 1982; 4:275-
nemia is a common feature of schizophrenia. J Neural 290
Transm Gen Sect 1995; 100:165-169 56. Westenberg H, Fineberg NA, Denys D: Neurobiology of
48. Ruck A, Kramer S, Metz J, Brennan M: Methyltetrahydro- Obsessive-Compulsive Disorder: Serotonin and Beyond.
folate is a potent and selective agonist for kainic acid CNS Spectr 2007; 12(Suppl 3):14-27
receptors. Nature 1980; 287: 852 57. Wilkinson AM, Anderson DN, Abou-Saleh MT et al.: 5-
49. Serot JM, Christmann D, Dubost T et al.: CSF-folate Methyltetrahydrofolate level in the serum of depressed
levels are decreased in late-onset AD patients. J Neural subjects and its relationship to the outcome of ECT. J
Transm 2001; 108:93-99 Affect Disord 1994; 32:163-168
50. Serot JM, Barbe F, Arning E et al.: Homocysteine and 58. Yang QH, Botto LD, Gallagher M et al.: Prevalence and
methylmalonic acid concentrations in cerebrospinal fluid: effects of gene-gene and gene-nutrient interactions on
relation with age and Alzheimer's disease. J Neurol serum folate and serum total homocysteine concentrations
Neurosurg Psychiatry 2005; 76:1585-1587 in the US: findings from the third national health and
51. Sinopoli VM, Burton CL, Kronenberg S et al: A review of nutrition examination survey DNA bank. Am J Clin Nutr
the role of serotonin system genes in obsessive-compulsive 2008; 88:232-246
disorder. Neurosci Biobehav Rev 2017; 80:372-381 59. Yazıcı MK, Demir B, Tanrıverdi N et al.: Validity and
52. Susser E, Brown AS, Klonowski E et al.: Schizophrenia inter-rater reliability of Hamilton Anxiety Rating Scale.
and impaired homocysteine metabolism: a possible Turk Psikiyatri Derg 1998; 9:114–117 [Turkish]
association. Biol Psychiatry 1998; 44:141-143 60. Young SN, Ghadirian AM: Folic acid and psycho-
53. Tiemeier H, van Tuijl HR, Hofman A et al.: Vitamin B12, pathology. Prog Neuropsychopharmacol Biol Psychiatry
folate, and homocysteine in depression: the Rotterdam 1989; 1 3:841-863
Study. Am J Psychiatry 2002; 159:2099-2101
Correspondence:
Hatice Ünver, MD
Department of Child and Adolescent Psychiatry,
Medical Faculty at the University of Marmara
Istanbul, Turkey
E-mail: drhaticeunver@gmail.com
77You can also read