Double-J catheter calcification risk factors and management
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ORIGINAL ARTICLE
Double-J catheter calcification
risk factors and management
González-Ramírez MA, Méndez-Probst CE, Feria-Bernal G.
• ABSTRACT • RESUMEN
Objective. To identify risk factors related to double-J Objetivo: Identificar factores de riesgo relacionados para
ureteral catheter calcification and to analyze different la calcificación de catéteres ureterales doble J y analizar
management strategies for catheter extraction. las diferentes estrategias en el manejo para su extracción.
Materials and Methods. A retrospective study from Material y métodos: Estudio retrospectivo de nuestra
information in our data-base from January 2004 to August base de datos de enero del 2004 a agosto del 2007. Se
2007 was carried out. A total of 382 double-J ureteral colocaron 382 catéteres ureterales doble J, 39 (10.2%) pre-
catheters were placed. Catheter calcification occurred sentaron calcificación y 30 (7.8%) de ellos no fue posible
in 39 patients (10.2%) and simple extraction was not su extracción simple, por lo que concluimos que fueron
possible in 30 of them (7.8%) and so we concluded that “retenidos”. En los 39 analizamos distintas variables para
they were “retained”. Different variables were analyzed la identificación de factores litogénicos y el método de re-
in the 39 patients to identify lithogenic factors and tiro. Se realizó estudio comparativo con prueba de Fisher
removal method. A comparative study with the Fisher en dos grupos: calcificación identificada antes de 6 meses
test was carried out in two groups: calcification that was (Grupo 1), y después de 6 meses (Grupo 2). En dos pacien-
identified before 6 months (Group 1) and after 6 months tes no se obtuvo información sobre dicho periodo.
(Group 2). This time interval could not be determined in Resultados: Grupo 1: 12 pacientes (32.4%) y Grupo 2:
2 patients. 25 pacientes (67.6%). Se identificó un factor genético en
Results. There were 12 patients in Group 1 (32.4%) 20.5%, metabólico 69.2%, infeccioso 17.9%, estructural
and 25 patients in Group 2 (67.6%). A genetic factor 15.4%, y farmacológico 25.6%. Al comparar las variables
was identified in 20.5% of patients, a metabolic factor in entre los dos grupos, no se encontró diferencia estadística-
69.2%, an infectious factor in 17.9%, a structural factor mente significativa. En 35 pacientes se requirió de un solo
in 15.4% and a pharmacological factor in 25.6%. No procedimiento para el retiro del catéter. Sólo se presentó
statistically significant difference was found between una complicación (fístula urinaria de la pelvis renal). No
the two groups. The catheter was removed in a single hubo cambio significativo en la función renal global.
Urology Department. Instituto Nacional de Ciencias Médicas y Corresponding author: Manuel Alejandro González Ramírez. medic_
Nutrición “Salvador Zubirán” Mexico City alex@hotmail.com Telephone: (0155) 54 87 09 00 ext 2145. Vasco
de Quiroga # 15, Delegación Tlalpan, CP 14000, México, D.F.
Rev Mex Urol 2009;69(1):7-12 7González-Ramírez MA et al. Double-J catheter calcification risk factors and management
procedure in 35 patients. Only 1 complication presented Conclusiones: La calcificación del catéter ureteral doble
(renal pelvic urinary fistula). There was no significant J es una complicación seria y algunas ocasiones com-
change in over-all kidney function. promete su extracción. La experiencia en el manejo
Conclusions. Double-J ureteral catheter calcification is endourológico hace que sea posible la resolución exi-
a serious complication and its removal can be difficult. tosa en un solo tiempo aun en calcificaciones severas. Es
Successful catheter removal in a single procedure even importante vigilar estrechamente aquellos pacientes con
mayor riesgo litogénico.
in the case of severe calcification is possible when the
surgeon is experienced in endourological management.
It is important that patients at high risk for lithogenesis Palabras clave: litiasis, catéter ureteral, litotricia, hiper-
be under close surveillance. calciuria.
Key words: Lithiasis, Ureteral catheter, Lithotripsy,
Hypercalciuria.
• INTRODUCTION Percuflex or Tecoflex is used in more than 90%
Since the introduction of the double-J ureteral of cases in our department. It is recommended that
catheter by Finney in 1978 (1), its use has taken an these catheters not remain in place longer than 6
important position in the management of obstructive months in order to avoid complications such as urinary
uropathy (urolithiasis, ureteral stenosis and lesions, tract infections, migration, rupture and calcification and
retroperitoneal fibrosis), of postoperative ureteropyelic retention. Despite this recommendation a considerable
stenosis and kidney transplant. The introduction amount of patients are found to present with such
of new materials and modifications has improved complications even though their catheters have been in
mechanical and hydrodynamic characteristics making place for less than 6 months.
these catheters more biocompatible. They are made of Calcification and the potential impossibility to
different polymer-based synthetic materials. The first remove the ureteral catheter are the most serious
polyethylene catheter stopped being used because of complications (2,3), representing a great challenge for
its rigidity, low tolerance and high depolymerization the urologist to opportunely identify the patient most
and high fracture risk. Polyurethane catheters have at risk of presenting with it as well as to successfully
adequate resistance and flexibility and are economic extract it. Crystal aggregation in the ureteral catheter
but have limited biocompatibility and biodurability and takes place due to three mechanisms: a) urea-splitting
are recommended for short periods of time (3 months). bacteria colonization (4-5), b) lithogenic and anti-
Silicon catheters are more biocompatible but their lithogenic factors in the patient even in the absence
retention and tension strength is limited, requiring of bacteria (4) and c) red blood cell, white blood cell,
greater thickness. This results in a smaller internal platelet and fibrin derivative adhesion in the catheter
caliber which limits hydrodynamic characteristics. They that acts as a matrix for crystal aggregation (6).
are more difficult to place because of their high friction The objective of this study was to identify double-J
coefficient and they should not be left in place longer than catheter calcification risk factors and to analyze different
12 months. Catheters made from different copolymers therapeutic strategies for calcified catheter removal.
(Percuflex, Tecoflex, C-Flex, Silitek and Urosoft) such as
silicon and polyurethane have greater tension strength,
their walls are thinner and their internal diameter is • MATERIALS AND METHODS
larger giving them better hydrodynamics. Their flexibility A retrospective analysis of 382 patients in whom double-J
and hydrogel covering let them adapt adequately to the catheter was placed from January 2004 to August 2007
urothelium with greater biocompatibility than those of was carried out. Thirty-nine patients (10.2%) presented
polyurethane. Their biocompatibility is close to those with calcification. Simple extraction was not possible
of silicon but with a lower friction coefficient. They also in 30 of them (7.8%), indicating that the catheters were
have a low propensity to form mineral salt deposits. retained. The following variables were reviewed: sex,
Their recommended period of use is 6 to 12 months. age, body mass index (BMI), ureteral catheter placement
8 Rev Mex Urol 2009;69(1):7-12González-Ramírez MA et al. Double-J catheter calcification risk factors and management
Table 1. Characteristics of 39 patients Table 2. Lithogenic factor description
Variable N: 39 Total Patients with
Variable (%)
mean Age 48.7 years 39 identified factor (N)
Sex
Metabolic Factor (27)
Female 79.5% 31
Male 20.5% 8 Hypercalciuria 66.7% 18
mean BMI 28.12 38 Hyperoxaluria 11.1% 3
Hypocitraturia 14.8% 4
Placement Motive Hyperuricosuria 7.4% 2
Urolithiasis 89.7% 35
Ureteral stenosis 2.6% 1 Genetic Factor (8)
Pyeloplasty 2.6% 1 Urolithiasis 100% 8
Pregnancy 2.6% 1
Infectious Factor (7)
mean Ureteral Catheter Continued Placement 8.4 months
Enterococo faecium 28.6% 2
Metabolic Factor Proteus mirabilis 71.4% 5
Yes 69.2% 27 Structural Factor (6)
No 30.8% 12
Retroperitoneal Fibrosis 33.3% 2
Genetic Factor Pyeloureteral Stenosis 66.7% 4
Yes 20.5% 8 Pharmacological Factor (9)
No 71.8% 28
Tiazides 44.5% 4
ND 7.7% 3
Steroids 11.1% 1
Infectious Factor Salicilates 33.3% 3
Alopurinol 11.1% 1
Yes 17.9% 7
No 76.9% 30
ND 5.1% 2
Structural Factor
Yes 15.4% 6 all kidney function (serum creatinine before and after
No 79.5% 31 ureteral catheter removal).
ND 5.1% 2 When one attempt at simple extraction was successful,
calcification was classified as slight. If cystolitholapaxy,
Pharmacological Factor
extra- or intracorporeal lithotripsy and/or open surgery
Yes 23.1% 9 were required, calcification was classified as moderate
No 71.8% 28 to severe.
ND 5.1% 2 Comparative analysis of lithogenic factors between
ND = not determined the two groups was carried out using the Fisher
BMI = body mass inde exact test with P < 0.05 as statistical significance.
Group 1 was the group in which calcification was
identified before 6 months and Group 2 in which it
was identified after 6 months. Windows SPSS V13
statistical program was employed.
motive, time lapse from catheter placement to
calcification identification, lithogenic factors such
as metabolic factor (lithiasis profile), genetic factor • RESULTS
(family history influencing urolithiasis), infectious Percuflex double-J catheter was used in 38 patients
factor (urea-splitting bacteria), pharmacological factor (94.9%) and silicon double-J catheter was used in 1
(drugs with known risk for urolithiasis), structural factor patient (5.1%). Characteristics and variable analysis of
(anatomical alterations in the urinary system), calcification the 39 patients is shown in Tables 1 and 2. There was
management, complications and modification in over- no information in regard to length of time ureteral
Rev Mex Urol 2009;69(1):7-12 9González-Ramírez MA et al. Double-J catheter calcification risk factors and management
Table 3. Lithogenic factor comparison between Groups 1 and 2
with Fisher exact test
1
Fisher exact test
4
Lithogenic Grup 1 Grup 2
P value
Factors N: 12 (%) N: 25 (%)
Metabolic
7
Yes 10 (83.3%) 17 (68%)
0.28
No 2 (16.7%) 9 (32%)
Genetic
Yes 4 (33.3%) 4 (16%) Laser ureterolithotripsy
No 7 (58.3%) 20 (80%) 0.19 Extracción simple
ND 1 (8.4%) 1 (4%) Cystolitholapaxy
Infectious
Yes 2 (16.7%) 5 (20%)
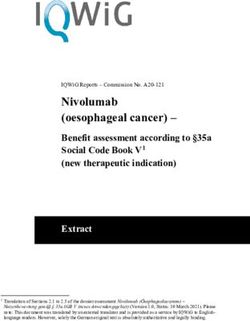
No 10 (83.3%) 19 (76%) 0.5 Figure 1. Group 1 removal method
ND 0 1 (4%) 1
1
Structural 1
Yes 4 (33.3%) 2 (8%) 5
No 8 (66.7%) 22 (88%) 0.08
ND 0 1 (4%)
4
Pharmacological
Yes 3 (25%) 6 (24%)
No 9 (75%) 18 (72%) 0.66
ND 0 1 (4%) 12
ND= not determined
catheter remained in 2 patients. Group 1 was made
up of 12 patients (32.4%) and Group 2 of 25 patients Simple extraction Laser ureterolithotripsy
(67.6%). Comparative analysis between the two groups
Cystolitholapaxy LEOCH/Cystolitholapaxy
is shown in Table 3. Removal method was not known
in 2 patients and a single procedure was required for Ballistic ureterolithotripsy LEOCH/Cystolitholapaxy/
catheter removal in 35 patients. In Group 1 four patients Image 1. Double-J ureteral catheter with incrustation at the medial and
Pielolitotomía
distal end.
presented with slight calcification in the distal segment
and/or body of the catheter in which successful removal
was possible with a simple extraction. Seven patients
presented with moderate to severe calcification in the was carried out in 2. One patient presented with severe
distal segment in which successful removal was possible incrustation in the proximal J that required 1 session of
with cystolitholapaxy. One patient presented with extracorporeal lithotripsy and then simple extraction in
severe incrustation in the body of the catheter a second session. Another patient presented with severe
which was resolved through laser ureterolithotripsy incrustation in the proximal and distal segments requiring
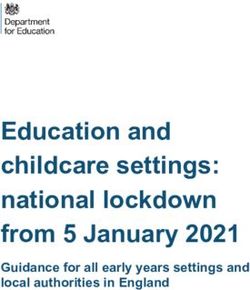
(Figure 1). In Group 2 simple extraction was required extracorporeal lithotripsy of the proximal J in one session
in 5 patients presenting with slight calcification in the and cystolitholapaxy of the distal J (Image 1). Removal
external surface of the catheter. Twelve patients was not possible because there was no response in the
presented with moderate to severe incrustation proximal calcification and so pyelolithotomy had to be
in the distal segment that was resolved through carried out in order to extract the catheter. These two
cystolitholapaxy. Because of severe calcification in patients were the only ones who required more than one
the catheter body mechanical ureterolithotripsy was procedure to resolve calcification. Therapeutic strategy
carried out in 4 patients and laser ureterolithotripsy distribution is shown in Figure 2.
10 Rev Mex Urol 2009;69(1):7-12Laser ureterolithotripsy
Extracción simple
Cystolitholapaxy
González-Ramírez MA et al. Double-J catheter calcification risk factors and management
1 been shown to have an impact on treatment or classification
1 since relatively low volumes (100 to 400 mm3) have
1
required more than one procedure for catheter removal.
5 Slight calcification can be classified as that in which one
attempt at simple extraction is successful. Moderate to
4 severe calcification classification can be that in which
cystolitholapaxy, extra- or intracorporeal lithotripsy and/or
open surgery are required.
A renal metabolic problem was shown in 69.2% of
12 catheters presenting with external surface calcifications.
Of these, 66.7% were related to hypercalciuria although
there was a poor relation to ureolithic germs. In the
comparison between patients identified with calcification
before or after six months (the recommended time for
Simple extraction continued Percuflex double-J ureteral catheter placement),
Laser ureterolithotripsy
32.4% of patients identified with incrustations after 6 months
Cystolitholapaxy LEOCH/Cystolitholapaxy required more complex procedures for catheter removal.
Ballistic ureterolithotripsy LEOCH/Cystolitholapaxy/ There was no statistically significant difference between the
Pielolitotomía two groups probably due to the limited number of patients
compared, motivating us to increase the size of the database
Figure 2. Group 2 removal method and continue the study.
Due to the development of endourological techniques
it is possible to carry out successful removal with a low
incidence of complications in a single procedure even in
Except for the patient requiring open surgery, the rest of cases of severe incrustations and retained catheters.
the patients were managed as out-patients and were able
Of the different endourological strategies used in our
to leave the hospital on the same day of their procedures.
institution we consider laser to be the most versatile
A urinary fistula of the renal pelvis presented in 1 patient
method for managing moderate to severe incrustations in
who then needed to undergo three additional procedures.
the catheter body because incrustation fragmentation is
No significant changes in overall kidney function were
performed with greater technical ease avoiding the use of
documented in any of the cases noting the fact that 2 of the
trident tweezers for fragment extraction in the majority
patients had only one kidney.
of cases. Cystolitholapaxy is sufficient for resolving
important calcifications of the proximal J. If proximal J
• DISCUSSION incrustation is slight to moderate it can initially be managed
Intraluminal calcification development does not have an with extracorporeal lithotripsy. If it is severe and does not
impact on catheter hydrodynamic function since only 4% of respond to extracorporeal lithotripsy, percutaneous or open
such calcifications present clinically significant obstructive surgery must be considered.
uropathy (8). The same does not hold true for extraluminal
calcification which by affecting catheter lateral orifice flow • CONCLUSIONS
significantly reduces ureteral flow. Therefore the more
Double-J ureteral calcification is a serious complication in
proximal the affectation, the less flow will be generated. The
the use of these devices and so the patient at high risk for
same thing takes place when extraluminal calicification is
lithogenesis must be under strict surveillance. Experience
related to a catheter with a wider diameter.
in endourological management provides successful
Crystal aggregation to the catheter surface most calcification resolution in a single procedure even in severe
commonly begins with proteic, cellular and calcium cases.
crystal adhesion. Multiple crystallography studies carried
out on formed crustations have shown that monohydrate
calcium oxalate is the most frequent (up to 80%). Studies BIBLIOGRAPHY
by Vallejo and collaborators have shown that hypercalciuric
1. Finney, RP. Experience with new double J ureteral catheter stent 1978. J
alkaline urine infected with ureolithic germs has the Urol 2002 167:1135-8.
greatest tendency to generate incrustations as opposed to 2. El-Faquih SR, Shamsuddin AB, Chakrabaarti A et al. Polyurethane internal
stents in treatment of stone patients: Morbidity related to indwelling times.
normocalcemic and sterile urine. J Urol 1991;146:1487-91.
3. Mohan-Pillai K, Keeley FX Jr, Moussa SA et al. Endourological manage-
Calcification is a frequent and serious complication that ment of severely encrusted ureteral stents. J Endourol 1999;
can lead to catheter retention. Incrustation volume has not 13:377-9.
Rev Mex Urol 2009;69(1):7-12 11González-Ramírez MA et al. Double-J catheter calcification risk factors and management
4. Bithelis G, Bouropoulos N, Liatsikos EN, Perimenis P. Assessment 7. Burgos Revilla FJ, Vallejo Herrador J, Sáenz Garrido J. Utilidad de los
of encrustations on polyurethane ureteral stents. J Endourol 2004; catéteres endourológicos en el tratamiento de la litiasis urinaria. Arch
6:550-9. Esp Urol 2001;54:895.
5. Stickler DJ, Morris N, Moreno M, Sabbuba N. Studies on the formation 8. Abdul Majid Rana, Abdul Sabooh. Management strategies and re-
of crystalline bacterial biofilms on urethral catheters. Eur J Clin Micro- sults for severly encrusted retained ureteral stents. J Endourol
biol Infect Dis 1998;17:1. 2007;21:628.
6. Tieszer C, Reid G, Denstedt J. Conditioning film deposition on ureteral
stents after implantation. J Urol 1998;160:876.
12 Rev Mex Urol 2009;69(1):7-12You can also read