EMERGENCY! PROMP CARDS! - MEDICAL EMERGENCIES SEC0ON
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Emergency!
Promp✚ Cards!
Medical Emergencies Sec0on
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020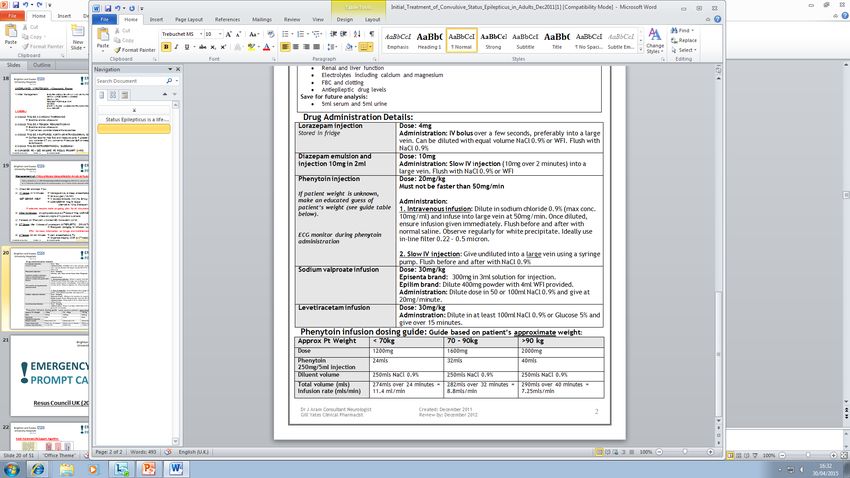
Suspected Sepsis
Could this be sepsis? RED FLAG
• NEWS ≥5 • Lactate ≥ 2
1 AND/OR • Heart rate >130
• Does the pa5ent look sick • Altered mental state (V/P
on AVPU)
If yes • Systolic Blood Pressure
• Ensure full set of observa5ons 25
• Get senior review ST4+ • Oxygen required to
maintain SpO2 > 92% (88%
• Senior Doctor review iden5fies presence of one or more red flag
in COPD)
symptoms
• Urine – not passed in 18
3 OR hours or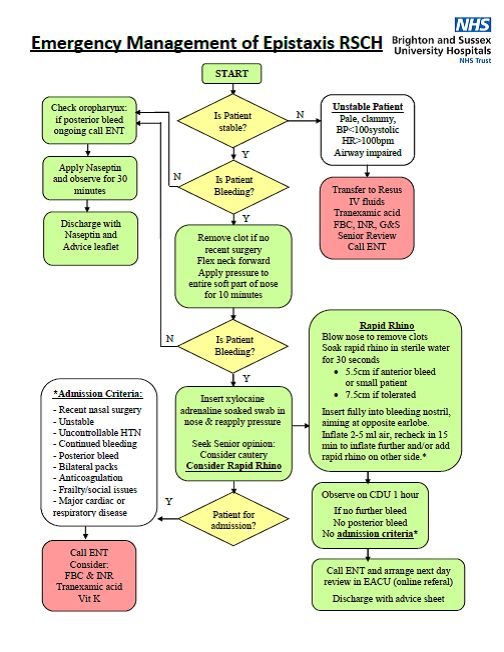
Treatment of Hyperkalemia
Mild: 5.5-5.9mmol/L Moderate: 6-6.4mmol/L Severe: >6mmol/L
• Bloods: Bloods (U&Es, Mg2+, HCO3-, CK)
1 • ECG
• If K >6mmol/L ensure cardiac monitoring
If K >6.5mmol/L Or ECG changes give
2 • 10mL 10% Calcium Gluconate IV over 3 minutes
Temporary reduc0on of K+
3 • 10 units of Actrapid Insulin in 50mL 50% dextrose IV over 15minutes
• If K+ >6.5mmol/L this will only reduce K+ for 4 hours
Consider:
4 • 10mg of nebulised salbutamol
• Cau5on if IHD or tachycardic
If HCO3-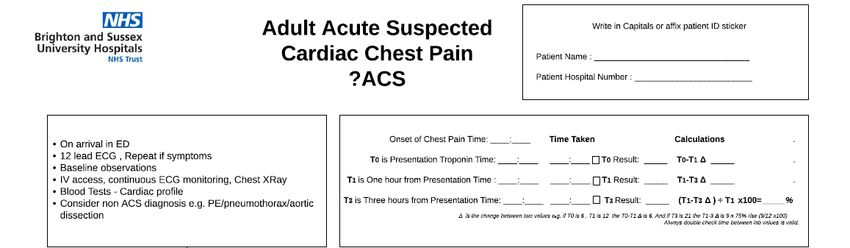
MASSIVE Pulmonary Embolus (PE)
Unstable pa5ent with likely PE diagnosis/proven massive PE (BPDiabe0c Ketoacidosis
Diagnos5c Criteria all 3 required Fluids
• Blood ketones >3 1L 0.9% sodium chloride with potassium as per
• Blood glucose >11mmol/L or known Diabetes (T1 and 2) below box
• 1L over next 2 hours
• Serum bicarbonateLife Threatening Asthma
1 ABCDE assessment – Urgent senior ED and Urgent ITU review if life threatening features
Life threatening asthma is severe asthma with any one feature of life threatening;
Severe Asthma (any 1 of) Life Threatening Clinical Signs Life Threatening Measurement
• PEF 33-50% best/predicted • Altered conscious level • PEFAcute Chest Pain Pathway
On arrival in A&E
1 12 lead ECG
2 IV access
3 Baseline observa5ons
4 Con5nuous cardiac monitoring un5l 1st troponin result
5 Blood tests (FBC, U&E, LFTs, Troponin, INR, lipids, glucose)
6 Medical clerking and drug chart to be completed in A&E
7 Ini5a5on of ACS treatment when diagnosis confirmed
8 Medical assessment confirms Cardiac chest pain (SPR or above)
9 Follow pathway on next page
6
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020Acute Chest Pain Pathway
a
6
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020Acute Chest Pain Pathway
b
6
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020Unexplained Hypotension- Diagnos0c Prompt
Ini0al management THINK and Consider following Diagnosis
Could this be CARDIAC TAMPONDE?
1 ABCDE Assessment → Examine and ultrasound
Could this be TENSION PNEUMOTHORAX?
2 Ensure Large bore IV access → Examine and ultrasound
→ If periarrest consider bilateral thoracotomies
3 Send VBG Could this be a RUPTURED AORTA/INTRA ABDOMNIAL
BLEED?
4 Request portable CXR → Perform a FAST Scan
→ Measure Aorta (>4.5cm consider AAA and CT)
→ If any concerns contact Vascular SpR bleep 8004,
5 Do an ECG OOH via switchbored
Could this be RETROPERITONEAL BLEEDING?
6 Start IV fluids unless contraindicated → Examine and ultrasound
CONSIDER PULMONARY EMBOLISM
7 Inform Senior → See massive PE Prompt card
7
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020Management of PROLONGED 8
SEIZURES/STATUS EPILEPTICUS
Status Epilep0cus is a life threatening medical emergency defined as;
• Seizure las5ng ≥5 minutes
OR
• ≥ 2 seizures without return of consciousness
OR
• ≥ 3 tonic clonic seizures within 1 hours
REVIEW DUE APR 2020
Check BM and Treat if low and get senior help
1st stage 0-10 minutes
• Manage airway and contact anesthe5cs if concerns 8235
• Give oxygen 15L/min
• Gain IV Access and bloods (incl. Na, B-HCG, alcohol, drug levels)
Give
VERSION 5.0
• Lorazepam 4mg IV bolus at 4-5 minutes
Alterna0ve if no IV access
• Diazepam 10mg PR
If pa0ents seizures resolve make Treatment
IMPLEMENTED APR 2019
•
management plan for
• Monitoring • Infusions if required
• Determine cause
Ongoing seizure aXer 10 minutes give
• Second dose of Lorazepam 4mg IV (Unless cyano5c/hypoxic)
2nd Stage: an0epilep0c drug therapy (aXer 2x 4mg dose of lorazepam)
• Phenytoin 20mg/kg IV infusion (on cardiac monitor)
• If already on phenytoin contact consultant – consider valproate or leve5rcetam
3rd Stage 30-60 minutes
• Contact anesthe5cs and ITU
• Organise imaging CT head and CXRDrug Administra0on Guide in Status Epilep0cus
Review following points before
administra0ng Phenytoin
• Do you have pa5ents correct
weight?
• Have you sent a Phenytoin
level?
• Have you used the correct
diluent?
• What is the concentra5on of
your final solu5on?
• Is the infusion rate correct?
• Is a filter in place?
• Are you infusing with an
incompa5ble drug?
• Are you giving a loading or
maintenance dose?
Phenytoin Infusion Dosing Guide: Based on approximate weight
• Monitor for side effects
If in doubt, consultant with a
pharmacist and/or local
guidance
a
8
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020Adrenal Insufficiency/ Addisonian Crisis Emergency
Management
Pa0ents at Risk Clinical Features
• Pre-exis5ng Addison’s disease (primary adrenal insufficiency) • Hypotension
• Pituitary Disease (secondary adrenal insufficiency) • Dizziness
• Pa5ents on chronic steroid treatment ≥7.5mg prednisolone OD (or • Collapse
equivalent dose of other steroids) for ≥3 weeks in the last 3 months • Hypovolemic shock
• Fa5gue
• Confusion
Precipitants • Vomi5ng • Trauma
• Infec5on • Diarrhoea • Stress • Delirium
• Dehydra5on • Major Stress • Impaired level of consciousness
• Abdominal pain/cramps
• Nausea/vomi5ng
Diagnos5c measures should not delay treatment, if suspected treatment • Weight loss
should commence without delay
Closely monitor for biochemical There are no adverse consequences
abnormali5es of ini5a5ng life-saving hydrocor5sone
• Hypoglycemia • Hyperkalemia treatment.
• Hyponatraemia • AKI
If the diagnosis is unclear, it can be
safely and formally established when
Immediate Management the pa5ent has clinically recovered.
→ Hydrocor5sone 100mg IV/IM STAT (cont 50mg QDS regularly)
→ IV fluids 1L 0.9% NaCl in the first hour Contact an Endocrinologist for urgent
→ Further IV hydra5on (4-6L over 24 hours) Monitor for fluid overload in review.
elderly, cardiac and renal impairment Report all incidents of Addisonian crisis for
→ Monitor capillary blood glucose and treat hypoglycemia pa5ents with known adrenal insufficiency or
hypopituitarism on the DATIX system
9
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020Management of Malignant Hypertension
BP ≥180/120mmHg
Symptoms Signs General Measures
• Headache • BP ≥180/120mmHg • Contact on-call
• Blurred vision • Grade III/IV re5nopathy Cardiologist/ Renal/
• Confusion • Re5nal Haemhorrage/exudates HDU
• NONE AT ALL • Papillioedema
• Consider arterial line
Consider Secondary Causes inser5on
• Intracranial Haemhorrage • Renal Artery Stenosis
• Aor5c Dissec5on • Cocaine • Close monitoring of
• Acute Glomerulonephri5s • Eclampsia haemodynamics and
• Phaemochromocytoma fluid balance
Inves0ga0ons
• FBC • Coagula5on
• U&E • 12 lead ECG
Acute Phase Management
• Target to reduce diastolic BP to 100-110mmHg over 6 hours
• MAXIMUM DECREASE of 25% from baseline in 24 hours
Labetalol
→ IV infusion at at rate of 15-120mg/hr (5trate upwards un5l adequate response- see
prompt card for guidence)
→ GTN infusion as per trust protocol
Sodium Nitroprusside (under specialist advice only)
→ IV infusion star5ng at a rate of 0.3microgram/kg/min
→ Increase by 0.5 microgram/kg/min every 5 minutes to 8 microgram/kg/min
0
1
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020Severe Pre- Eclampsia Defini5on Features of severe pre-eclampsia: • BP of ≥160/110 alone • Severe Headache OR • Blurred vision • BP
Eclamp0c Seizures
• Dial 2222 state OBSTETRIC EMERGENCY
1
• If s5ll pregnant state NEONATAL EMERGENCY
2 Administer high flow oxygen and maintain airway
3 Place in the leX lateral posi5on
IV access
4
Send FBC, U&E, LFT’s, Urate, INR, G&S
5 Con5nuous BP and oxygen satura5on monitoring
6 Commence Magnesium immediately (see below for dose)
7 Commence Labetalol as necessary
8 Fetal monitoring and delivery planning
Loading Dose Maintenance Dose
4g MgSO4 (8mls of 50% 10g MgSO4 (20mls)
solu5on)
Mixed with 12 ml N.Saline/5% Mixed with 30mls water for
Dextrose for injec5on injec5on to total volume 50ml
I.V over 5 mins Infusion to DUE
runAPRat2020a rate of
2
1
IMPLEMENTED APR 2019 VERSION 5.0 REVIEWIni0al management of Gastrointes0nal Haemorrhage
Resuscitate Pa5ent
1
• ABCDE assessment
2
Gain bilateral large bore IV access Correct Clolng
• Send FBC, U&E, LFT’s, Cloyng, G&S
• Stop an5coagulants
• Start IV fluids
3 • Shocked pa5ent need four units of cross matched RBC
• Pa5ents with liver disease may require more • Stop an5platelet
4 Hourly fluid balance calcula5on and urine output • If on NOAC, contact haematologist
High risk for variceal bleed OR previous variceal bleed
→ Terlipressin 2mg IV (QDS) (1mg if ischemic heart/
• If renal impairment contact renal
5 vascular disease) team
→ Tazocin 4.5g IV
→ In penicillin allergic gentamycin and metronidazole • If platelets 70g/dL • Consider FFP
7 Unless advanced liver disease (jaundice, ascites,
coagulopathy) • If recent coronary stentEndoscopy Referral
a
3
1
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020Emergency Laparotomy Risk Assessment
High Risk Criteria
2 or more of • Lactate >2
• RR >20 • NEWS >5
• WBC 12 • Age >70
• HR >90 • Age >50 and significant comorbidity
• Temp 38
And Organ Dysfunc5on
• Systolic BP 90%
If any of the above- inform A&E consultant
1
Obtain senior surgical review/discussion within 30 minutes
A&E Team
• Oxygen
• Large bore cannula & fluid resuscita5on
2
• Catheterise and fluid balance chart
• Bloods FBC, U&E, LFT, Cloyng, G&S 2X, Lactate, Amylase
• Administer an5bio5cs as per microguide
Surgical Team
• Ensure above is complete
• CT scan (state emergency laparotomy on form) within 2 hours
3 • Inform anesthe5st (bleep 8224)
• Next available slot on emergency theatre list
• Calculate and document P-Possum mortality score
(www.riskpredic5on.org.uk)
4
1
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020Emergency Management of Epistaxis
5
1
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020General Approach to Managing Overdose
Assess airway
A Contact Anesthe5c team if required
• RR – If depressed and suspicious for opioid toxicity consider Naloxone 400mcg ini5al dose (see
Naloxone prompt card)
B • O2 satura0ons – Aim satura5ons 94-98% in all pa5ents
• Carbon monoxide poisoning suspected- High flow Oxygen (15L non-re-breather mask)
• BP – Hypotensive 250ml - 500ml 0.9% NaCl IV boluses, assess response.
• Hypertensive + tachycardia – consider Beta blockers
• HR – Bradycardic - 500mcg atropine / external pacing.
• For tachyarrhythmia - consider Metoprolol 2.5 – 5mg IV, consider magnesium sulphate 2g IV
C • VBG / ABG – If elevated lactate give IV fluids, and replace electrolytes as appropriate
• Venous bloods – Toxicology screen, paracetamol / salicylate levels, U+E’s, LFT’s, coagula5on, FBC
• ECG – Assess QT interval, tachy/brady-arrhythmias, ischaemic changes – consider Magnesium
Sulphate and Calcium Gluconate.
• NB: Remember Sodium Bicarbonate for TCA overdose.
• GCSDrug Overdose - Toxidromes
Toxidrome Vitals Pupils Other Symptoms Drugs
• Temp Hyperalert, agita5on, hallucina5ons Cocaine, amphetamines,
Sympathomime5c • HR Mydriasis Diaphoresis, tremors, hyper-reflexia, seizures ephedrine, pseudoephedrine,
• RR theophylline, caffeine
• BP
• Temp Hypervigilanve, agita5on, hallucina5ons, coma An5histamines, tricyclics, an5-
An5cholinergic • HR Mydriasis Dry, flushed skin, dry mucous membranes, Parkinson agents,
• RR decreased bowel sounds, urinary reten5on, an5spasmodics, phenothiazines
• BP myoclonus, seizures (rarely) (an5-psycho5cs), atropine
• Temp Hallucina5ons, agita5on Phencyclidine, LSD, MDMA
Hallucinogenic • HR
Mydriasis Nystagmus ("Ecstasy“)
• RR
• BP
• Temp Tremor, myoclonus, hyper-reflexia, clonus, MAOIs alone or with SSRIs,
Serotonin Syndrome • HR Mydriasis diaphoresis, flushing, rigidity, diarrhoea TCAs, L-tryptophan
• RR
• BP
• Temp CNS depression, coma Opioids e.g. heroin, morphine,
Opioid • HR Miosis Hypo-reflexia, pulmonary oedema, needle methadone, oxycodone
• RR marks
• BP
• Temp CNS depression, confusion, coma Benzodiazepines, barbiturates,
Seda5ve / Hypno5c • HR
Miosis / Hypo-reflexia alcohols
• RR Mydriasis
• BP
• Temp Confusion, coma Organophosphate and
Cholinergic • HR
Miosis Saliva5on, incon5nence, diarrhoea, emesis, carbamate insec5cides, nerve
• RR diaphoresis, lacrima5on, GI cramps, agents, nico5ne, pilocarpine,
bronchoconstric5on, muscle fascicula5on / edrophronium,
• BP
weakness, seizures
7
1
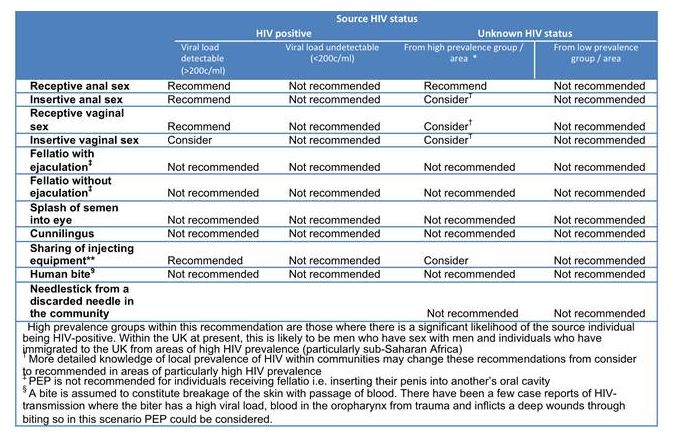
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020Post Exposure Prophylaxis (PEP)
Ensure all discussions, prescrip5ons and dispensing is with maximum privacy
Indicated when poten5al high risk exposure in the last 72 hours
• Ideally to start within 24 hours of exposure
Considera5ons
• Drug interac5on
Complete the relevant referral form of the intranet. Search ‘PEP’
• Pregnant?
Complete up to date PEP proforma • Breas|eeding?
• Separate forms for sexual and occupa5onal exposure • Is emergency
contracep5on
Take PEP baseline bloods- HIV serology, crea5nine, ALT and ALP (Group on symphony) required?
• Sexual assault?
Prescribe PEP on symphony (search ‘post’ in drug name)
• 5 day packs available SHAC East (Claude Nicol
• Remind pa5ents it is a 28 day course Centre), Eastern Road,
Brighton, BN2 5BE Tel:
Counsel pa5ent on how to take PEP and inform them of the PEP passport (in the box) 01273 523388
Sexual exposure pa5ents must contact the Claude Nicol center for follow up ASAP
If there is a complicated risk assessment, known HIV posi5ve source or you are unsure-
contact HIV SPR on 8075/via switch OOH
• Complete PEP referal form hmps://nww.bsuh.nhs.uk/clincal/teams-and-departments/hiv/pep-referal
• Link can be found on microguide under ‘post exposure prophylaxis’
• Occupa0onal Health MUST be no0fied of all occupa0onal exposures
8
1
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020Post Exposure Prophylaxis (PEP)
a
8
1
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020Care of the Dying Pa0ent
Have you recognised your pa5ent may day in the Ensure you:
coming hours or days? • Have considered poten5ally reversible causes which
• Deliver the five priories for the care of the dying may be appropriately treated
• Assess symptoms and prescribe appropriate
Recognise medica5on
1 • The possibly that a person may die within the • Assess need for clinically assisted hydra0on and
next few hours or days nutri0on
• Clarify any prior expressed wishes/review any
Communica5on
advance care plans
• Sensi5ve communica5on between staff, the
2
dying person and those iden5fied as important Remember:
to them • Involve senior decision maker
• Refer to pallia5ve care on bamboo
Involve
• The dying person and those iden5fied as • RSCH EXT 3021 Bleep 8420, OOH Martlets hospital
important to them are involved in decisions • PRH EXT 3021, bleep 8420 OOH St Peter & St James
3
about treatment and care Hospital
• If admission NOT wanted and discharge feasible
• To the extent the dying person wants
contact pallia5ve care team urgently
Support
4 • Ac5vely explore the needs of pa5ent and those AXer assessment and conversa5ons, use these
iden5fied as important to them documents found on microguide:
1. Individualised care plan (doctor to complete -
Plan and deliver follow prompts on chart)
• An individual care plan 2. Symptom observa5on chart for a dying person
5 • Including food &drink 3. Nursing care plan for a dying person
• Symptom control 4. Drug chart with appropriate symptom control
• Psychological, spiritual and social support medica5on
9
1
IMPLEMENTED APR 2019 VERSION 5.0 REVIEW DUE APR 2020End of Life Care Prescribing
• All pa5ents reconised as dying must have pre-emp5ve medica5on prescribed PRN for control of common
symptoms
• Ensure a dose is administered if symptoma5c
• If PRN not controlling symptoms (≥3 doses in 24 hour period) seek specialist advice or consider syringe pump
• See Microguide for further prescribing guidance under pallia5ve care sec5on
Symptom Drug Dose Frequency Contacts
Pallia5ve care Team
1st line: Diamporphine Pain Dyspnoea
9-5 Mon-fri
Pain/ breathlessness 2.5-5mg SC 1 hourly 4 hourly • Bleep 8420
2nd line: Morphine 1 hourly 4 hourly • Ext 3021
5mg SC
Known severe reanl faliure eGFR Alfentanil RSCH OOH – Martlets
• 01273964164You can also read