Epileptic Encephalopathy With Continuous Spike And Wave During Sleep: Caratterizzazione clinica, neurofisiologica e neuropsicologica - Valentina ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Epileptic Encephalopathy With Continuous
Spike And Wave During Sleep:
Caratterizzazione clinica, neurofisiologica e
neuropsicologica
Valentina De Giorgis, MD PhD
Martina Zanaboni, Spec. in Neuropsicologia e Psicoterapia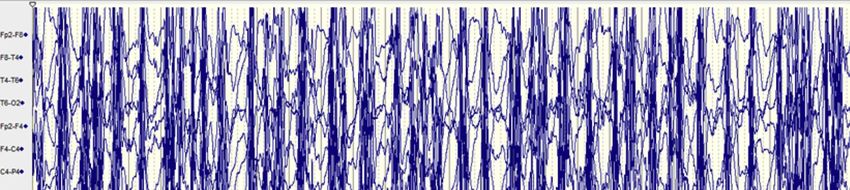
DEFINITION the «TRUE EPILEPTIC ENCEPHALOPATHY»
The cognitive and behavioural difficulties are the direct result of the underlying
epileptic activity and any targeted treatment
Clinic
Sublinical Electric Status Epilepticus induced by sleep
Patry et al., 1971
EEG Encephalopathy related to status epilepticus during slow sleep (ESES)
Tassinari et al., 1977
Epilepsy with continuous spikes and waves during slow sleep (ECSWS)
NPS Tassinari et al., 1985 – Palayiotopoulos, 2005
characterization
Continuous spikes and waves during sleep (CSWS)
Commission on Classification and Terminology of ILAE, Engel 2006
Treatment
Epileptic Encephalopathy with Continuous Spike and Waves during Sleep
(ESES)
Commission on Classification and Terminology of ILAE, Berg et al., 2010
Clinical
Study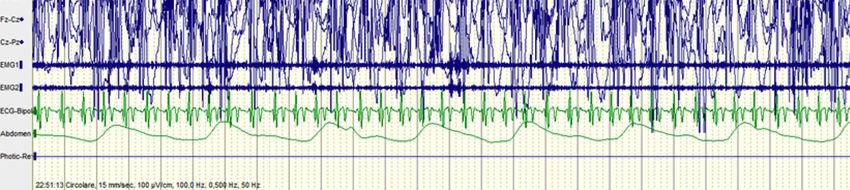
DEFINITION CSWS: TYPICAL SYMPTOMS
Hallmark: a significant increase in EEG abnormalities during sleep with
Clinic presence of neurocognitive impairment
EEG
++ Neuropsychological impairment
Global or Selective cognitive or Language regression
NPS
characterization
++ Typical EEG pattern
continuous epileptiform activity in NREM sleep
+ Epilepsy, with focal or generalized seizures
Treatment clonic; tonic–clonic; absence; focal-motor; focal-complex; negative myoclonus
+/- Motor deterioration
ataxia, dyspraxia, dystonia or unilateral deficits
Clinical
Study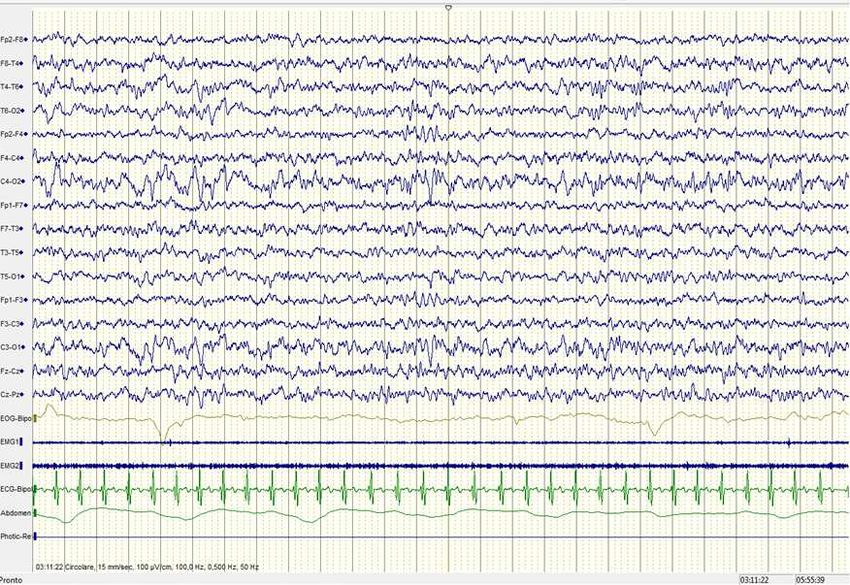
Definition ETIOLOGY
A complex interplay between brain development, maturation processes and
susceptibility genes
CLINIC
Structural
Perinatal infarction, Brain malformation, Thalamic injury, Shunted
Hydrocephalus, POLYMICROGYRIA
EEG
Genetic
GRIN2A: cognitive disability, focal epilepsy, ESES, autistic-like disability
CNKSR2: epilepsy-aphasia spectrum
NPS
characterization
SRPX2: RE, verbal dyspraxia, and intellectual disability, autism
CNVs: 15q13.3, 15q11.2, 16p13.11, 1q21.1, 16p11.2, 22q11.2, 16p11.2
Idiopathic – Self limited
Treatment
Regular development before epilepsy onset, no brain lesions
ECTS (Rolandic) – Atipical ECTS – Panayiotopoulos - Gastaut
Unknown – Cryptogenic
Developmental delay before epilepsy onset, dysmorphic features, comorbilities
Clinical
Study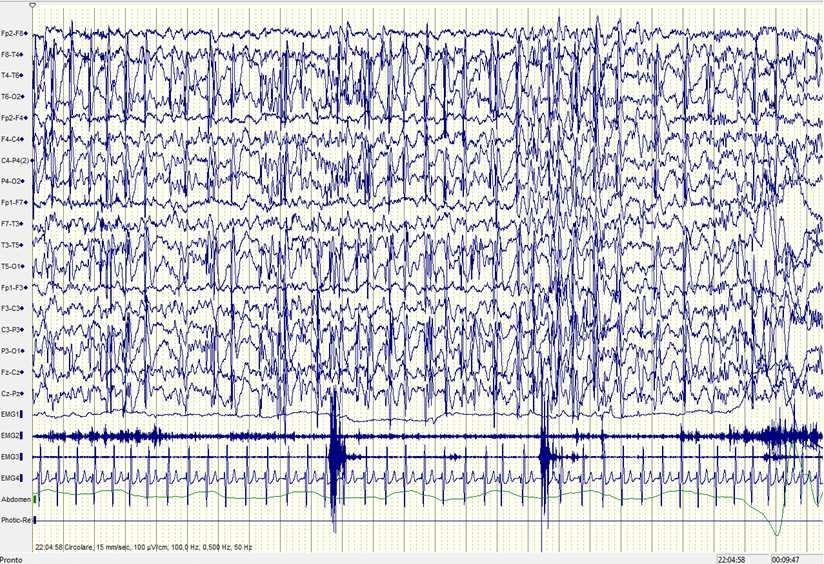
Definition CSWS
Encephalopathy with SES
different seizure types, combinations of cognitive, motor, and behavioural
CLINIC disturbances, and CSWS EEG pattern
Landau-Kleffner Syndrome
acquired aphasia, seizures, neuropsychological deficit, behavioural disturbances
EEG and CSWS
Acquired epileptiform opercular syndrome
oro-facio-lingual deficits, focal motor seizures involving the face and
NPS
characterization occasionally rolandic, partial complex, or atypical absences, neuropsychological
deficit and CSWS
Atypical Benign epilepsy with centro-temporal spikes (BECTS)
Treatment early age at onset, frequent spikes or spike-wave discharges in awake,
severe neuropsychological impairment and CSWS pattern
Clinical
Study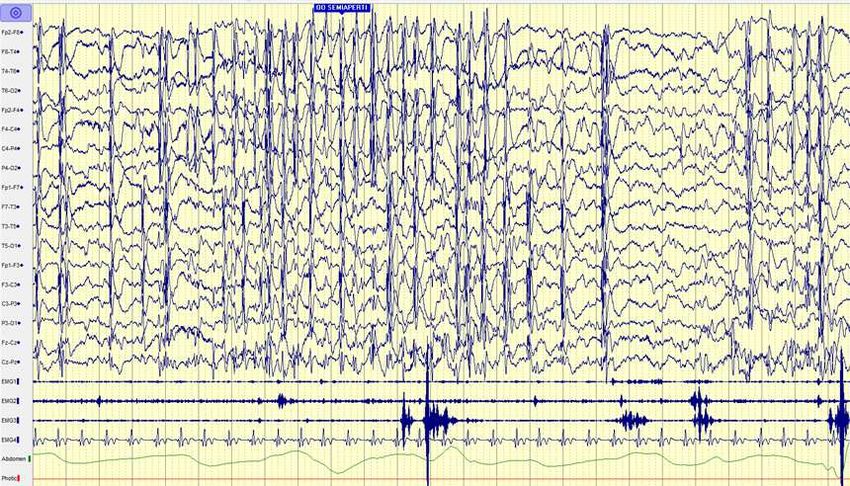
Definition CSWS – 3 MAIN GROUPS
Static frames of an evolutive multifactorial age-related condition
PERVASIVE
CLINIC Language, memory, spatial orientation, ADHD, autistic-like behaviours
COMBINED – multiple concomitant disfunctions
Temporal (language in LKS), frontal, occipital, parietal dysfunction, spatio-
EEG temporal or motor disturbances (negative myoclonus, dyspraxias, gait disorders)
SELECTIVE
Unique specific impairment restricted to a limited number of cortical columns
NPS
characterization
Treatment
Clinical
Study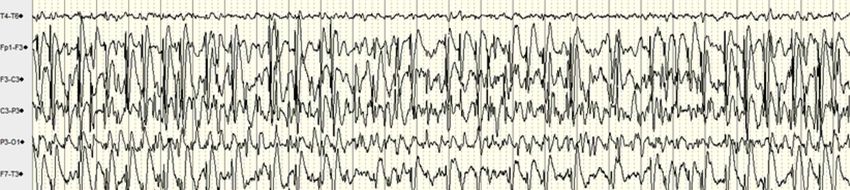
Definition
CLINIC
EEG
NPS
characterization
Treatment
Clinical
Study
Definition CSWS - EVOLUTION
2y 6y (4-8) 12y (8-16)
CLINIC
II STAGE
I STAGE CSWS period
Frequent seizures
Pre-CSWS period Absences, Myoclonic, Atonic, Clonic III STAGE
Infrequet nocturnal motor focal EEG:
EEG seizures CSWS evolution
Abnormal background Seizures remit
EEG: Widespread spikes of higher
nonREM potentiation of EEG:
amplitude Normalization of interictal activity
spiking SWI >85%
focal-multifocal SW (CT-F- Cognitive, Language improvement
Cognitive, Language, Behavior, (but not normalization)
PO) Motor deterioration
NPS
characterization
OUTCOME AND PROGNOSIS
CSWS disappear after 11-12y
Seizures usually disappear with puberty
Treatment Residual moderate to severe neurocognitive impairments persist
Poor prognosis when:
Symptomatic/structural
Early onset seizures
Resistance to AEDs CRITICAL PERIOD
Clinical DURATION OF CSWS & PLASTICITY
Study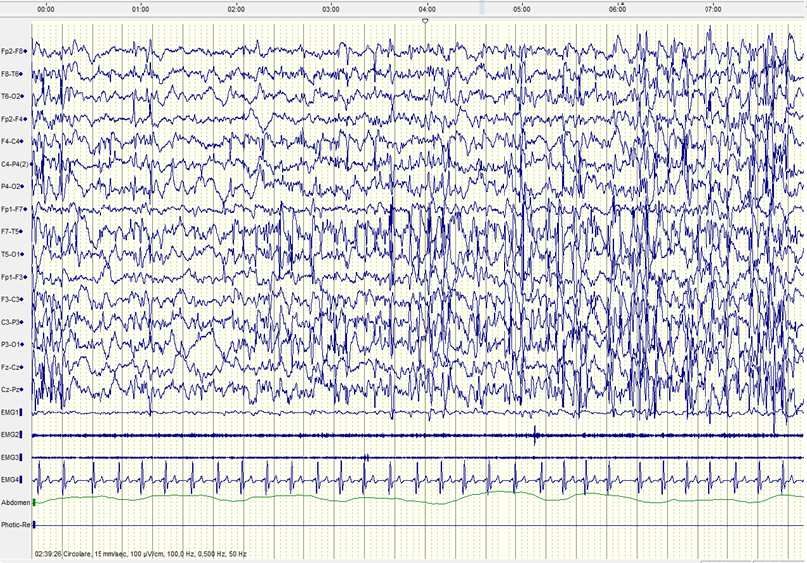
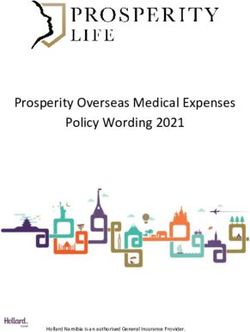
Definition CSWS: TYPICAL EEG pattern
Clinic
diffuse bilateral
and/or unilateral or focal localization
rhythmic high-amplitude spikes and waves
EEG
NPS
characterization
Treatment
Clinical occurring in slow sleep (NREM)
study
persisting on 3 or more recordings over a period of at least 1 month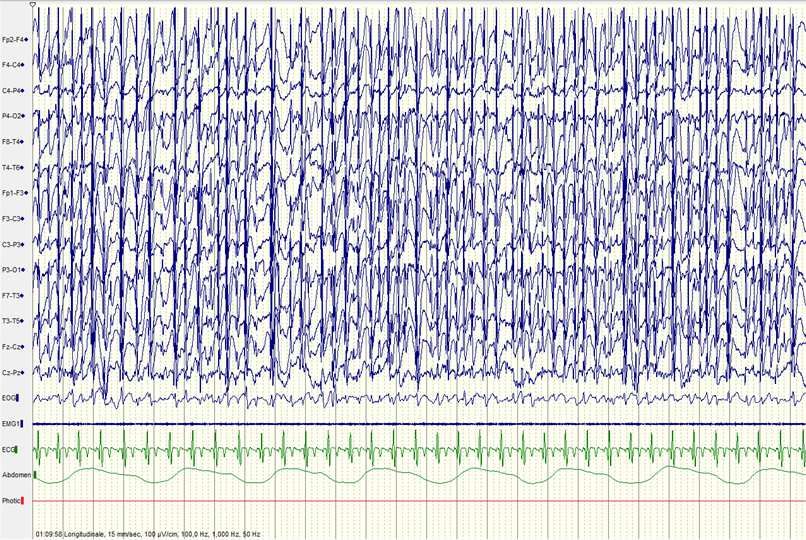
Definition CSWS: EPILEPTIFORM ACTIVITY
Morfology
Parameters for a syndromic and/or etiological assessment
Clinic
Amplitude
EEG Before ESES: FC – CT – T – P – O – Vertex
Topography During ESES: migration to frontal regions
ESES offset: moving back to the original topography
NPS
characterization
Developmental Stages
AEDs
Treatment
Clinical
studyDefinition CSWS: EPILEPTIFORM ACTIVITY
Morfology
Parameters for a syndromic and/or etiological assessment
Clinic
Amplitude
EEG Before ESES: FC – CT – T – P – O – Vertex
Topography During ESES: migration to frontal regions
ESES offset: moving back to the original topography
NPS
characterization
Developmental Stages
AEDs
Treatment
Clinical
studyDefinition CSWS: EPILEPTIFORM ACTIVITY
Morfology
Parameters for a syndromic and/or etiological assessment
Clinic
Amplitude
EEG Before ESES: FC – CT – T – P – O – Vertex
Topography During ESES: migration to frontal regions
ESES offset: moving back to the original topography
NPS
characterization
Developmental Stages
AEDs
Treatment
Clinical
studyDefinition CSWS: EPILEPTIFORM ACTIVITY
Morfology
Parameters for a syndromic and/or etiological assessment
Clinic
Amplitude
EEG Before ESES: FC – CT – T – P – O – Vertex
Topography During ESES: migration to frontal regions
ESES offset: moving back to the original topography
NPS
characterization
Developmental Stages
AEDs
Treatment
Clinical
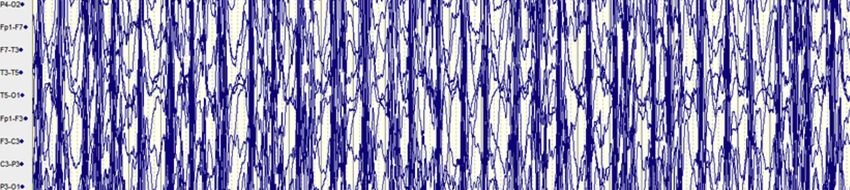
studyDefinition CSWS: TYPICAL EEG pattern
WAKEFULNESS:
Focal Slow Activity reflecting the main epileptic focus
Clinic
Burst of diffuse SW (abesences) +/-diffuse PoliWS (atonic – myoclonic)
EEG
NREM:
- SW slower and more rhythmic during slow sleep (from a secondary
bilateral/unilateral synchronization of the focal / multifocal SW)
NPS - Transition between diffuse, hemisferic and focal pattern
characterization
- Fragmented EEG
Treatment REM:
- Focal SW (similar to wakefulness)
- Brief bursts of diffuse SW (arousal)
Clinical
studyDefinition CSWS: TYPICAL EEG pattern
WAKEFULNESS:
Focal Slow Activity reflecting the main epileptic focus
Clinic
Burst of diffuse SW (abesences) +/-diffuse PoliWS (atonic – myoclonic)
EEG
NREM:
- SW slower and more rhythmic during slow sleep (from a secondary
bilateral/unilateral synchronization of the focal / multifocal SW)
NPS - Transition between diffuse, hemisferic and focal pattern
characterization
- Fragmented EEG
Treatment REM:
- Focal SW (similar to wakefulness)
- Brief bursts of diffuse SW (arousal)
Clinical
studyDefinition CSWS: TYPICAL EEG pattern
WAKEFULNESS:
Focal Slow Activity reflecting the main epileptic focus
Clinic
Burst of diffuse SW (abesences) +/-diffuse PoliWS (atonic – myoclonic) pagine
galeone / Martini
EEG
NREM:
- SW slower and more rhythmic during slow sleep (from a secondary
NPS bilateral/unilateral synchronization of the focal / multifocal SW)
characterization
- Transition between diffuse, hemisferic and focal pattern
- Fragmented EEG Mettere esempio di sincronizzazione in sonno
Treatment
REM: mettere esempio di sonno REM
- Focal SW (similar to wakefulness)
- Brief bursts of diffuse SW (arousal)
Clinical
studyDefinition CSWS: TYPICAL EEG pattern
WAKEFULNESS:
Focal Slow Activity reflecting the main epileptic focus
Clinic
Burst of diffuse SW (abesences) +/-diffuse PoliWS (atonic – myoclonic)
EEG
NREM:
- SW slower and more rhythmic during slow sleep (from a secondary
bilateral/unilateral synchronization of the focal / multifocal SW)
NPS - Transition between diffuse, hemisferic and focal pattern
characterization
- Fragmented EEG
Treatment REM:
- Focal SW (similar to wakefulness)
- Brief bursts of diffuse SW (arousal)
Clinical
studyDefinition CSWS: TYPICAL EEG pattern
WAKEFULNESS:
Focal Slow Activity reflecting the main epileptic focus
Clinic
Burst of diffuse SW (abesences) +/-diffuse PoliWS (atonic – myoclonic)
EEG
NREM:
- SW slower and more rhythmic during slow sleep (from a secondary
bilateral/unilateral synchronization of the focal / multifocal SW)
NPS - Transition between diffuse, hemisferic and focal pattern
characterization
- Fragmented EEG
REM: mettere esempio di sonno REM
Treatment - Focal SW (similar to wakefulness)
- Brief bursts of diffuse SW (arousal)
Clinical
studyDefinition CSWS: TYPICAL EEG pattern
WAKEFULNESS:
Focal Slow Activity reflecting the main epileptic focus
Clinic
Burst of diffuse SW (abesences) +/-diffuse PoliWS (atonic – myoclonic)
EEG
NREM:
- SW slower and more rhythmic during slow sleep (from a secondary
bilateral/unilateral synchronization of the focal / multifocal SW)
NPS - Transition between diffuse, hemisferic and focal pattern
characterization
- Fragmented EEG
REM:
Treatment - Focal SW (similar to wakefulness)
- Brief bursts of diffuse SW (arousal)
Clinical
studyDefinition CSWS: TYPICAL EEG pattern
WAKEFULNESS:
Focal Slow Activity reflecting the main epileptic focus
Clinic
Burst of diffuse SW (abesences) +/-diffuse PoliWS (atonic – myoclonic)
EEG
NREM:
- SW slower and more rhythmic during slow sleep (from a secondary
bilateral/unilateral synchronization of the focal / multifocal SW)
NPS - Transition between diffuse, hemisferic and focal pattern
characterization
- Fragmented EEG
Treatment REM:
- Focal SW (similar to wakefulness)
- Brief bursts of diffuse SW (arousal)
Clinical
studyDefinition CSWS: TYPICAL EEG pattern
WAKEFULNESS:
Focal Slow Activity reflecting the main epileptic focus
Clinic
Burst of diffuse SW (abesences) +/-diffuse PoliWS (atonic – myoclonic)
EEG
NREM:
- SW slower and more rhythmic during slow sleep (from a secondary
bilateral/unilateral synchronization of the focal / multifocal SW)
NPS - Transition between diffuse, hemisferic and focal pattern
characterization
- Fragmented EEG
REM:
Treatment - Focal SW (similar to wakefulness)
- Brief bursts of diffuse SW (arousal)
Clinical
studyDefinition CSWS: MEASURES
SPIKE AND WAVE INDEX: percentage of NREM sleep occupied by spikes
Clinic and waves (time occupied by epileptiform activities)
Methods Visual estimtion
EEG Computer-aided spike detection
Cut off 85/90% - 50% - 25%
Lack of the accepted criteria for the diagnosis of ESES
NPS
characterization
Fluctuating In the same patient during the course of ESES
Within the same night (++ firt part of night)
Treatment
Clinical
studyDefinition CSWS: MEASURES
SPIKE AND WAVE INDEX: percentage of NREM sleep occupied by spikes
Clinic and waves (time occupied by epileptiform activities)
Methods Visual estimtion
EEG Computer-aided spike detection
Cut off 85/90% - 50% - 25%
Lack of the accepted criteria for the diagnosis of ESES
NPS
characterization
Fluctuating In the same patient during the course of ESES
Within the same night (++ firt part of night)
Treatment
Clinical
studyDefinition CSWS: MEASURES
SLEEP STRUCTURE
Clinic
Presence/absence of sleep graphoelements
Alternating NREM/REM stages
EEG
Markers of fragmentation/instability
in sleep microstructure
NPS
characterization
SPINDLES Consolidation of memory – maintenance of cognitive functions –
EXECUTIVE FUNCTIONS
Treatment
(working memory – cognitive flexibility – problem solving)
Chatburn, 2013
Astill et a., 2014
Clinical Vermeulen et al., 2018
studyDefinition CSWS: MEASURES
SLEEP STRUCTURE
Clinic
Presence/absence of sleep graphoelements
Alternating NREM/REM stages
EEG
Markers of fragmentation/instability
in sleep microstructure
NPS
characterization
SPINDLES Consolidation of memory – maintenance of cognitive functions –
EXECUTIVE FUNCTIONS
Treatment
(working memory – cognitive flexibility – problem solving)
Chatburn, 2013
Astill et a., 2014
Clinical Vermeulen et al., 2018
studyDefinition CSWS: MEASURES
SLEEP STRUCTURE
Clinic
Presence/absence of sleep graphoelements
Alternating NREM/REM stages
EEG
Markers of fragmentation/instability
in sleep microstructure
NPS
characterization
SPINDLES Consolidation of memory – maintenance of cognitive functions –
EXECUTIVE FUNCTIONS
Treatment
(working memory – cognitive flexibility – problem solving)
Chatburn, 2013
Astill et a., 2014
Clinical Vermeulen et al., 2018
studyDefinition CSWS: MEASURES
SLOW WAVES DOWNSCALING
Absence of progressive renormalization (downscaling) of synaptic strength
Clinic occurring during sleep – Altered onvernight decrease of slow wave slope
EEG
Wakefulness Learning Process Synchronization of large cortical areas
NPS High synaptic strength
characterization
Overnight Synaptic weaking/elimination decrease of the SWA slope
Treatment
Physiologic sleep-related synaptic downscaling
Tononi & Cirelli., 2014
Esser et al., 2007
Clinical Riedner et al., 2007
study Bolsterli et al., 2017Definition
NEW NEUROIMAGING TECHNIQUES AND BEYOND
EEG-fMRI
DIFFUSION TENSOR
IMAGING TRACTOGRAPHY
Clinic age-dependent difference and heritability
of the perisylvian language network,
altered white matter connectivity,
motor networks related to behavior,
EEG cognitive and motor tasks
Parlatini et al., 2017
Budisavljevic et al., 2014
NPS
characterization
EEG COHERENCE STUDIES
functional brain connectivity as a measure of functional
association between 2 brain regions
Treatment
Clinical
study
Mott et al., 2019Definition CSWS: COGNITION
Congnitive regression/Stagnation (>12pts)
Language regression
Clinic Learning disabilities
Behavioural disturbances (ADHD)
EEG Geographical Prominence of SWA
Temporal: LKS
Fronto-Central: Rolandic
Occipital: visuo-spatial
NPS
characterization
Common-to-all basic diagnostic assessment
Intelligence
Language
Treatment Memory
Attention
Visuo-spatial
Executive Functions
Clinical Arzimanoglou & Cross., 2019
studyDefinition
Clinic
EEG
Avoid:
PB, PHT, CBZ, OXC
NPS
characterization
TREATMENT
treatment goals include not only the improvement in seizure control, but even
more important a reduction in EEG abnormalities and consequently
Clinical neuropsychological deficits
studyDefinition
Intravenous methylprednisolone
pulse therapy
15–30 mg/kg/day
Clinic for 3 consecutive days, once a
month, for 4 months
Case/sex Epilepsy Neurological Neurological Outcome after PT
syndrome problems problems at the
before epilepsy start of PT
EEG
1/F ESES Minimum Severe mental No change Significant reduction
motor retardation (TIQ 38) (pDefinition
RETROSPECTIVE EVALUATION OF THE
ESES/CSWS POPULATION
Clinic AIM OF THE STUDY
To find possible correlations between clinical variables and ESES/CSWS
outcome, with the aim to identify possible factors involved in a worse long-term
cognitive and behavioral outcome in patients affected by ESES/CSWS with a
SWI ≥ 50
EEG
RESULTS
71 patients (36 males and 35 females)
Mean follow-up: 6.1 years (range 2-11).
NPS Mean age at first seizure onset: 3.9 years (range 0-12)
characterization Mean age at ESES/CSWS onset: 5.7 years (range 2-14)
Mean ESES/CSWS duration: 1.84 years (range 0.4-4)
Treatment 17 pt: ischemic birth injuries
(porencephaly, periventricular leukomalacia)
4 pt: brain infections
(3 congenital cytomegalovirus infections, 1 meningitis),
3 pt: focal or diffuse cortical dysplasia,
1 pt: ganglioloma,
1 pt: thalamic cavernous angioma
1 pt: Leber Congenital Amaurosis
CLINICAL 5 genetic alterations
(cromosomic translocation, del4q13.1, dup-inv 15q)
STUDYDefinition SEIZURE DISTRIBUTION
At T0 most patients presented seizures
during night sleep (47.9%)
At T1 both in daytime and sleep
Clinic (49.2%)
At T2 seizure freedom 59.1% (7pt night,
9pt day, 7 pt both)
EEG
SWI was measured through a nocturnal polygraphic monitoring EEG recording in all
NPS
patients during ESES/CSWS period (t1) and we found a mean SWI of 78% on our patients
characterization with a range from 50% to 95%.
Treatment
CLINICAL
STUDYDefinition FOCAL SLOW ACTIVITY IN SLEEP
73.4% of patients
even if this pattern apparently
Clinic doesn’t correlate with ESES outcome
(seizures, neuropsycological and motor
findings, drug-resistance)
EEG
Example of a focal slow activity in sleep (frontal-central left) Example of a focal slow activity in sleep (central-occipital right)
NPS
characterization
Treatment
CLINICAL
STUDYDefinition WHAT’S NEW
Clinic Patients who presented sleep disorder before ESES/CSWS onset were those
who showed worst cognitive outcome (pDefinition TREATMENT EFFICACY
Steroids 48%
Clinic Benzodiazepine 20%
Sulthiame 18%
VPA
Levetiracetam 8%
Etosuximide 6%
EEG
NPS
characterization
DRUG-RESISTANCE
Prevalent in lesional patients, not in idiopatic ones (p=0.002)
Treatment In patients who had a developmental delay before ESES/CSWS (P=0.04)
CLINICAL
STUDYDefinition
Clinic
16 «Idiopathic» Patients (8 M, 8 F) Area Test
Parameter
to be assessed
Borderline Patological
EEG
Mean Age at onset 6,25 Cognitive assessment WISC-IIIa Cognitive profile
QItot 85-71
QIP 85-71
QItot 2
DDEb (task 10 – word dictation)
Writing
Accuracy 1< z-score < 2 z-score > 2
Detailed DDEb (task 11 – non word dictation)
BDE (foreward and backword
neuropsychological Calculation
enumeration, number reading, Numerical competence
number dictation, number repetition,
weighted score 5-7 weighted scoreRESULTS
ESES Duration of Sex T0 T0 T0 T0 EEG T0 Diagnosis ESES T0 T1
Patient onset Follow-up
Comorbilities Comorbilities Seizures discharge SWI Therapy Intelligence Intelligence
(year)
(year) Quotient Quotient
#1 5 6 M delayed speech behavioral problems motor focal Temporal left 80 Atypical HC + VPA + TIQ 76 TIQ 101
BECTS ETS VIQ 78 PIQ 79 VIQ 112 PIQ 113
#2 6,6 3 M delayed speech emotional social atonic Temporal 50 LKS HC + CLB + TIQ84 TIQ82
emot social probl problems right VPA VIQ75 PIQ96 VIQ72 PIQ93
#3 5,5 6 M delayed speech hyperactivity tonic Temporal left 80 LKS HC + LEV + ETS TIQ 79 TIQ 94
hyperactivity VIQ 74 PIQ 90 VIQ 85 PIQ 104
#4 9 10 F delayed speech behavioral problems myoclonic Frontal 70 ESES STH + VPA + TIQ74 TIQ64
behavioral problems bilateral CLB VIQ77 PIQ77 VIQ65 PIQ72
#5 8,08 4 F anxiety anxiety motor focal Frontal 75 Atypical HC +VPA TIQ68 TIQ81
bilateral BECTS VIQ59 PIQ85 VIQ67 PIQ100
#6 6,3 3 M emotional-social emotional-social motor focal Temporal 80 Atypical HC +VPA TIQ 75 TIQ70
problems problems right BECTS VIQ 71 PIQ 84 VIQ63 PIQ85
#7 2,4 6 F no no tonic–clonic Central 50 ESES ETS + CLB TIQ 88 TIQ 67
bilateral VIQ 86 PIQ 92 VIQ 80 PIQ 62
#8 4,11 8 M delayed speech motor focal Central 90 ESES VPA + CLB TIQ 87 TIQ 91
hyperactivity hyperactivity left VIQ 74 PIQ 103 VIQ 79 PIQ 103
#9 4,5 9 F no behavioral problems motor focal Temporal left 80 ESES STH + ETS TIQ 99 TIQI106
VIQ 84 PIQ 116 VIQ 90 PIQ 120
#10 4,5 12 F delayed speech no tonic–clonic Temporal left 80 ESES ETS + CLB TIQ 59 TIQ 80
VIQ 56 PIQ 72 VIQ 65 PIQ 100
#11 6,25 16 F delayed speech behavioral problems motor focal Frontal right 80 ESES VPA + CLB TIQ 101 TIQ 94
behavioral problems VIQ93 PIQ 103 VIQ 82 PIQ 107
#12 6,4 9 F no no no Central 70 ESES HC + VPA +ETS TIQ 63 TIQ 53
right VIQ 52 PIQ 52 VIQ62 PIQ61
#13 6,5 12 F behavioral problems behavioral problems motor focal Central 75 ESES STH + CLB TIQ93 TIQ 91
hyperactivity hyperactivity bilateral VIQ81 PIQ107 VIQ80 PIQ102
#14 8,4 8 M hyperactivity hyperactivity motor focal Temporal left 80 Atypical VPA + HC TIQ34 TIQ64
BECTS VIQ40 PIQ42 VIQ54 PIQ56
#15 11 5 M emotional-social emotional-social motor focal Temporal 70 Atypical STH + VPA TIQ35 TIQ32
problems problems right BECTS +LEV VIQ43 PIQ42 VIQ43 PIQ36
#16 6,25 5 M no behavioral problems motor focal Central 80 Atypical HC +ETS + VPA TIQ69 TIQ60
right BECTS VIQ72 PIQ72 VIQ47 PIQ83Definition
Wechsler scales
Clinic
EEG
NPS
characterization
T0 Baseline – T1 Remission
Treatment VIQ ↓ : da 71.84 a 68.55
PIQ ↑ : da 77 a 85
p-value 0.004
CLINICAL
STUDYDefinition Cognitive evolution and age at onset
Clinic
Group 1: early onset
( < 6 aa)
Group 2: mid-onset
EEG (età 6-7 aa)
Group 3: late onset
(> 8 aa)
NPS
characterization
Scores: TIQ: Group 1: 61 to 62; Group 2: 72 to 75; Group 3: 85 to 95
VIQ: Group 1: 63 to 59; Group 2: 75 to 73; Group 3: 82 to 75
PIQ: Group 1: 66 to 69; Group 2: 73 to 83; Group 3: 92 to 106
Treatment
Early Onset group had lower IQ values during follow-up
(p value 0,02)
CLINICAL
Verbal scores were worse than Performance scores in all groups
STUDYDefinition Attention – Visuomotor skills - Memory
Clinic
EEG
NPS
characterization
Treatment Visuo-spatial attention: range values (83% with better performance during follow-up
Speed from 50° to 65°p - Accuracy from 50° to 75°p
Visuo-motor skills: scores in range in almost all patients
Improvement during follow-up (T0-T1) froml 45° to 64° p
Short term memory: scores in range in all patients
CLINICAL
STUDYDefinition Academic Skills
Clinic
EEG
NPS
characterization
Writing accuracy
improved from pathological to borderline in non-word (standard deviation mean values: T0 = -2.5 and T1 = -1.5)
Stayed significantly pathological with respect to words (standard deviation mean values: T0 = -6.5 and T1 = -4)
Treatment
Reading speed
non-word reading performance remained borderline during the follow-up (standard deviation mean values: T0= -1.8 and T1= -1.3)
word performance passed from borderline to normal scores (standard deviation mean values: T0= -1.9 and T1= -0.9).
Reading accuracy
non-word reading improved from pathological to normal (standard deviation mean values: T0 = -2 and T1 = -0.6)
CLINICAL word reading accuracy improved from pathological to borderline (standard deviation mean values: T0 = -1.9 andT1 = -1.3).
STUDYDefinition Lexical semantic route
(word writing accuracy)
Clinic
temporo-occipital region next to fusiform gyrus
medial and inferior temporal gyrus
EEG
NPS
characterization
Treatment
CLINICAL
STUDYDefinition
AGE OF CSWS ONSET
Worst evolution in early onset patients
Clinic
in whom the disease develops in a critical period of
brain and synaptic maturation
EEG
At the end of follow-up the Neuropsychological
picture did not refert to a deterioration
NPS
characterization
Verbal IQ has the worst evolution but
after an accurate evaluation of cognitive subtest decline
is not seen but a
Treatment
DEVELOPMENTAL HINDRANCE
CLINICAL
STUDYDefinition Whole Exome Sequencing
GENETICS IN CSWS PATIENTS
GRIN2A: cognitive disability, focal epilepsy,
ESES, autistic-like disability
Clinic SRPX2: RE, verbal dyspraxia, and intellectual
disability, autism
CNVs: 15q13.3, 15q11.2, 16p13.11, 1q21.1,
16p11.2, 22q11.2, 16p11.2
EEG
Trios of
NPS
9 patients with
characterization Idiophatic ESES
selection of potential interesting variants for
Treatment Sanger validation and Segregation Analysis
none of the them were de novo variants
CLINICAL
STUDY#1 Classical ESES evolution
Chr:Pos PubMed/OMIM Inheritance Sanger seq Gene Names Sequence Ontology (Combined)
Effect (Combined)
6:52318896{Epilepsy, juvenile absence, susceptibility to, 1} AD EFHC1 missense_variant Missense
Kainic acid-induced F-344 rat model of mesial temporal lobe epilepsy: gene expression and canonical pathways.
Sharma AK, Searfoss GH, Reams RY, Jordan WH, Snyder PW, Chiang AY, Jolly RA, Ryan TP.
3:124215182
Toxicol Pathol. 2009 Oct;37(6):776-89. doi: 10.1177/0192623309344202. Epub 2009 Aug 21. ? Validated KALRN missense_variant Missense
Regulation of mTORC1 by PI3K signaling.
Dibble CC, Cantley LC.
16:2257300Trends Cell Biol. 2015 Sep;25(9):545-55. doi: 10.1016/j.tcb.2015.06.002. Epub 2015 Jul 6. Review. ? Paternal MLST8 frameshift_variant LoF
Juvenile Leigh syndrome, optic atrophy, ataxia, dystonia, and epilepsy due to T14487C mutation in the mtDNA-ND6 gene: a
mitochondrial syndrome presenting from birth to adolescence.
Leshinsky-Silver E, Shuvalov R, Inbar S, Cohen S, Lev D, Lerman-Sagie T.
MT:14552 J Child Neurol. 2011 Apr;26(4):476-81. doi: 10.1177/0883073810384615. Epub 2010 Dec 31. ? ND6 missense_variant Missense
#2 ESES - mild cognitive impairment (IQ 67), no behav disturbances - pyneal gland cystis - seizure onset 2.1 years - ESES onset 5.16 years
Chr:Pos PubMed/OMIM Inheritance Sanger seq Gene Names Sequence Ontology (Combined)
Effect (Combined)
Chang et al. (2006) found that mice heterozygous for Hdac7 deletion were normal, but Hdac7 knockout was embryonic lethal. By
embryonic day 11, all Hdac7 -/- embryos showed widespread vascular rupture, pericardial effusion, and enlarged dorsal aortae.
Electron microscopy showed a lack of tight junctions between adjacent endothelial cells in dorsal aortae and cardinal veins prior to
death. Endothelial cell-specific Hdac7 deletion was also embryonic lethal. Hdac7 -/- embryos showed a dramatic upregulation of
Mmp10 in the perivascular region and downregulation of Timp1 in endothelial cell. Expression of class II HDACs in two mouse models of
temporal lobe epilepsy.
Jagirdar R, Drexel M, Bukovac A, Tasan RO, Sperk G.
12:48189171
J Neurochem. 2015 Nov 25. doi: 10.1111/jnc.13440. [Epub ahead of print] lesions HDAC7 splice_region_variantOther
MT:12346 MELAS SYNDROME ? ND5 missense_variant Missense
MT:13105 MELAS SYNDROME ? ND5 missense_variant Missense
#3 ESES - mild impairment of scholar performances (dislexia) - seizure onset 8 years - ESES onset 9 years
Chr:Pos PubMed/OMIM Inheritance Sanger seq Gene Names Sequence Ontology (Combined)
Effect (Combined)
5:89953800?Febrile seizures, familial, 4 ADGRV1 missense_variant Missense
The in vivo roles of STEF/Tiam1, Rac1 and JNK in cortical neuronal migration.
Kawauchi T, Chihama K, Nabeshima Y, Hoshino M.
6:155450373
EMBO J. 2003 Aug 15;22(16):4190-201. ? Maternal TIAM2 frameshift_variant LoF
Chang et al. (2006) found that mice heterozygous for Hdac7 deletion were normal, but Hdac7 knockout was embryonic lethal. By
embryonic day 11, all Hdac7 -/- embryos showed widespread vascular rupture, pericardial effusion, and enlarged dorsal aortae.
Electron microscopy showed a lack of tight junctions between adjacent endothelial cells in dorsal aortae and cardinal veins prior to
death. Endothelial cell-specific Hdac7 deletion was also embryonic lethal. Hdac7 -/- embryos showed a dramatic upregulation of
Mmp10 in the perivascular region and downregulation of Timp1 in endothelial cell. Expression of class II HDACs in two mouse models of
temporal lobe epilepsy.
Jagirdar R, Drexel M, Bukovac A, Tasan RO, Sperk G.
12:48189142
J Neurochem. 2015 Nov 25. doi: 10.1111/jnc.13440. [Epub ahead of print] lesions Maternal HDAC7 missense_variant Missense
The PHR proteins: intracellular signaling hubs in neuronal development and axon degeneration.
Grill B, Murphey RK, Borgen MA.
Neural Dev. 2016 Mar 23;11:8. doi: 10.1186/s13064-016-0063-0. Review. Pam and its ortholog highwire interact with and may
negatively regulate the TSC1.TSC2 complex.
Murthy V, Han S, Beauchamp RL, Smith N, Haddad LA, Ito N, Ramesh V.
13:77780968
J Biol Chem. 2004 Jan 9;279(2):1351-8. Epub 2003 Oct 14. ? MYCBP2 splice_region_variantOther
A novel serine racemase inhibitor suppresses neuronal over-activation in vivo.
Mori H, Wada R, Takahara S, Horino Y, Izumi H, Ishimoto T, Yoshida T, Mizuguchi M, Obita T, Gouda H, Hirono S, Toyooka N.
17:2227977Bioorg Med Chem. 2017 Jul 15;25(14):3736-3745. doi: 10.1016/j.bmc.2017.05.011. Epub 2017 May 11. ? SRR,TSR1 splice_region_variantOther
#4 Autism disorder, cognitive disability. No epileptic seizures (recognised by parents) but during EEG we found an epileptiform activity with a tipical picture of CSWS, confirmed during two-three
nocturnal EEG polisonnographic registrations
Chr:Pos PubMed/OMIM Inheritance Sanger seq Gene Names Sequence Ontology (Combined)
Effect (Combined)
SPIN90 phosphorylation modulates spine structure and synaptic function.
Cho IH, Kim DH, Lee MJ, Bae J, Lee KH, Song WK.
3:48719811PLoS One. 2013;8(1):e54276. doi: 10.1371/journal.pone.0054276. Epub 2013 Jan 14. ? NCKIPSD missense_variant Missense
8:68423813Epilepsy, familial temporal lobe, 5 AD, AR CPA6 missense_variant Missense
TULIP1 (RALGAPA1) haploinsufficiency with brain development delay.
Shimojima K, Komoike Y, Tohyama J, Takahashi S, Páez MT, Nakagawa E, Goto Y, Ohno K, Ohtsu M, Oguni H, Osawa M, Higashinakagawa T,
Yamamoto T.
14:36125071
Genomics. 2009 Dec;94(6):414-22. doi: 10.1016/j.ygeno.2009.08.015. Epub 2009 Sep 3. ? Maternal RALGAPA1 missense_variant Missense
. Changes in FCHO1/2 expression levels correlated directly with numbers of CCV budding events, ligand endocytosis, and synaptic
19:17889043
vesicle marker recycling. ? FCHO1 splice_region_variantOther#5 ESES - maternal familiarity for Epilepsy (cousins and uncles) - mild cognitive impariment (IQ 63), learning disorder, attention deficit, memory disturbances - seizure onset 7.25 y - ESES onset 10.5 years
Chr:Pos PubMed/OMIM Inheritance Sanger seq Gene Names Sequence Ontology (Combined)
Effect (Combined)
2:25976466Shashi-Pena syndrome AD ASXL2 missense_variant Missense
The Novel Membrane-Bound Proteins MFSD1 and MFSD3 are Putative SLC Transporters Affected by Altered Nutrient Intake.
Perland E, Hellsten SV, Lekholm E, Eriksson MM, Arapi V, Fredriksson R.
8:145736182
J Mol Neurosci. 2017 Feb;61(2):199-214. doi: 10.1007/s12031-016-0867-8. Epub 2016 Dec 16. ? MFSD3 frameshift_variant LoF
#6 ESES - from 2 to 4 year language disorder (word's articulation) - seizure onset 2,25 years - ESES onset 5.5 years - moderate cognitive impairment, severe language disturbance (landau kleffner)
Chr:Pos PubMed/OMIM Inheritance Sanger seq Gene Names Sequence Ontology (Combined)
Effect (Combined)
1:210977302
Temple-Baraitser syndrome AD KCNH1 splice_region_variantOther
A new locus regulating MICALL2 expression was identified for association with executive inhibition in children with attention deficit
hyperactivity disorder.
Yang L, Chang S, Lu Q, Zhang Y, Wu Z, Sun X, Cao Q, Qian Y, Jia T, Xu B, Duan Q, Li Y, Zhang K, Schumann G, Liu D, Wang J, Wang Y, Lu L.
7:1474775 Mol Psychiatry. 2017 Apr 18. doi: 10.1038/mp.2017.74. [Epub ahead of print] MICALL2 missense_variant Missense
Loss-of-function mutation of the AF9/MLLT3 gene in a girl with neuromotor development delay, cerebellar ataxia, and epilepsy.
Pramparo T, Grosso S, Messa J, Zatterale A, Bonaglia MC, Chessa L, Balestri P, Rocchi M, Zuffardi O, Giorda R.
9:20414311Hum Genet. 2005 Oct;118(1):76-81. Epub 2005 Oct 28. AD Paternal MLLT3 disruptive_inframe_insertion
Missense
Balschun et al. (1999) concluded that RYR3 has a functional role in hippocampal synaptic plasticity, specifically on the adaptation of
15:34135758
acquired memory in response to external changes or stimuli. ? RYR3 missense_variant Missense
#7 ESES - mother´s uncle with unknown EPILEPSY , mother´s cousin with ABSENCE, son of a mother´s cousin with ABSENCE - Seizure onset 4.5 years - ESES onset 7.4 years - metaphonological disorder,
attention deficit, (IQ98) - mild learning disorder, IQ 104
Chr:Pos PubMed/OMIM Inheritance Sanger seq Gene Names Sequence Ontology (Combined)
Effect (Combined)
A genome-wide association study and biological pathway analysis of epilepsy prognosis in a prospective cohort of newly treated
epilepsy.
Speed D, Hoggart C, Petrovski S, Tachmazidou I, Coffey A, Jorgensen A, Eleftherohorinou H, De Iorio M, Todaro M, De T, Smith D, Smith PE,
Jackson M, Cooper P, Kellett M, Howell S, Newton M, Yerra R, Tan M, French C, Reuber M, Sills GE, Chadwick D, Pirmohamed M, Bentley D,
Scheffer I, Berkovic S, Balding D, Palotie A, Marson A, O'Brien TJ, Johnson MR.
9:8331575 Hum Mol Genet. 2014 Jan 1;23(1):247-58. doi: 10.1093/hmg/ddt403. Epub 2013 Aug 19. ? PTPRD splice_region_variantOther
GRINL1A colocalizes with N-methyl D-aspartate receptor NR1 subunit and reduces N-methyl D-aspartate toxicity.
Roginski RS, Goubaeva F, Mikami M, Fried-Cassorla E, Nair MR, Yang J.
15:57924690
Neuroreport. 2008 Nov 19;19(17):1721-6. doi: 10.1097/WNR.0b013e328317f05f. ? GCOM1,MYZAPmissense_variant Missense
A novel ubiquitin-specific protease, synUSP, is localized at the post-synaptic density and post-synaptic lipid raft.
Tian QB, Okano A, Nakayama K, Miyazawa S, Endo S, Suzuki T.
16:23093775
J Neurochem. 2003 Nov;87(3):665-75. ? Maternal USP31 disruptive_inframe_deletion
Missense
Gene expression profile analysis in epilepsy by using the partial least squares method.
Wang D, Song X, Wang Y, Li X, Jia S, Wang Z.
ScientificWorldJournal. 2014;2014:731091. doi: 10.1155/2014/731091. Epub 2014 May 1Genetic disorders associated with postnatal
microcephaly.
Seltzer LE, Paciorkowski AR.
22:41489105
Am J Med Genet C Semin Med Genet. 2014 Jun;166C(2):140-55. doi: 10.1002/ajmg.c.31400. Epub 2014 May 16. Review. ? EP300 splice_region_variantOther#8 ESES - maternal familiarity for migraine; paternal familiarity for dyscalculia - seizure onset 8.5 years - ESES onset 9.4 years - Impaired reading and perceptual visual disorder, visual agnosia
(IQ80) - mild learning disorder (IQ116)
Chr:Pos PubMed/OMIM Inheritance Sanger seq Gene Names Sequence Ontology (Combined)
Effect (Combined)
Approximately 25% of the mutant mice showed signs of neurologic dysfunction, including ataxia and seizures. Imaging studies detected
6:32191659cerebral arteriovenous malformations. ? NOTCH4 disruptive_inframe_insertion
Missense
p600 regulates spindle orientation in apical neural progenitors and contributes to neurogenesis in the developing neocortex.
Belzil C, Asada N, Ishiguro K, Nakaya T, Parsons K, Pendolino V, Neumayer G, Mapelli M, Nakatani Y, Sanada K, Nguyen MD.
1:19480259Biol Open. 2014 May 8;3(6):475-85. doi: 10.1242/bio.20147807. ? UBR4 splice_region_variantOther
This gene is a member of the neuroblastoma breakpoint family (NBPF) which consists of dozens of recently duplicated genes primarily
located in segmental duplications on human chromosome 1. This gene family has experienced its greatest expansion within the human
lineage and has expanded, to a lesser extent, among primates in general. Members of this gene family are characterized by tandemly
repeated copies of DUF1220 protein domains. Gene copy number variations in the human chromosomal region 1q21.1, where most
DUF1220 domains are located, have been implicated in a number of developmental and neurogenetic diseases such as microcephaly,
macrocephaly, autism, schizophrenia, mental retardation, congenital heart disease, neuroblastoma, and congenital kidney and urinary
tract anomalies. Altered expression of some gene family members is associated with several types of cancer. This gene family contains
1:145296404
numerous pseudogenes. Alternative splicing results in multiple transcript variants. [provided by RefSeq, Oct 2014] ? NBPF10 missense_variant Missense
N-Acetyl-D-Glucosamine Kinase Promotes the Axonal Growth of Developing Neurons.
Islam MA, Sharif SR, Lee H, Moon IS.
Mol Cells. 2015 Oct;38(10):876-85. doi: 10.14348/molcells.2015.0120. Epub 2015 Oct 15. N-acetyl-D-glucosamine kinase interacts with
dynein light-chain roadblock type 1 at Golgi outposts in neuronal dendritic branch points.
Islam MA, Sharif SR, Lee H, Seog DH, Moon IS.
2:71297867Exp Mol Med. 2015 Aug 14;47:e177. doi: 10.1038/emm.2015.48. ? Paternal NAGK splice_acceptor_variant
LoF
AD/incomplete
13:111117759
Porencephaly 2 penetance COL4A2 missense_variant Missense
BET protein Brd4 activates transcription in neurons and BET inhibitor Jq1 blocks memory in mice.
Korb E, Herre M, Zucker-Scharff I, Darnell RB, Allis CD.
19:15367992
Nat Neurosci. 2015 Oct;18(10):1464-73. doi: 10.1038/nn.4095. Epub 2015 Aug 24. ? BRD4 splice_region_variantOther
Whole-exome sequencing identifies a variant of the mitochondrial MT-ND1 gene associated with epileptic encephalopathy: west
syndrome evolving to Lennox-Gastaut syndrome.
Delmiro A, Rivera H, García-Silva MT, García-Consuegra I, Martín-Hernández E, Quijada-Fraile P, de Las Heras RS, Moreno-Izquierdo A,
Martín MÁ, Arenas J, Martínez-Azorín F.
MT:3394 Hum Mutat. 2013 Dec;34(12):1623-7. doi: 10.1002/humu.22445. Epub 2013 Oct 10. ? ND1 missense_variant Missense
#9 ESES - mild perinatal sufference - seizure onset 5 years - ESES onset 10.5 years - mild cognitive impariment (IQ 65), learnign disability, attention deficit
Chr:Pos PubMed/OMIM Inheritance Sanger seq Gene Names Sequence Ontology (Combined)
Effect (Combined)
MINK is a Rap2 effector for phosphorylation of the postsynaptic scaffold protein TANC1.
Nonaka H, Takei K, Umikawa M, Oshiro M, Kuninaka K, Bayarjargal M, Asato T, Yamashiro Y, Uechi Y, Endo S, Suzuki T, Kariya K.
Biochem Biophys Res Commun. 2008 Dec 12;377(2):573-8. doi: 10.1016/j.bbrc.2008.10.038. Epub 2008 Oct 18. Regulation of dendritic
spines, spatial memory, and embryonic development by the TANC family of PSD-95-interacting proteins.
Han S, Nam J, Li Y, Kim S, Cho SH, Cho YS, Choi SY, Choi J, Han K, Kim Y, Na M, Kim H, Bae YC, Choi SY, Kim E.
2:160031597
J Neurosci. 2010 Nov 10;30(45):15102-12. doi: 10.1523/JNEUROSCI.3128-10.2010. ? Paternal TANC1 missense_variant Missense
Electrophysiologic studies indicated that Camk4 contributes to synaptic potentiation. Stimulation of brain slices induced significant
synaptic potentiation in the anterior cingulate cortex, insular cortex, and somatosensory cortex of wildtype mice, but reduced or
5:110560350
blocked potentiation in Camk4 -/- mice. ? CAMK4 splice_region_variantOther
DSCAM and DSCAML1 regulate the radial migration and callosal projection in developing cerebral cortex.
Zhang L, Huang Y, Chen JY, Ding YQ, Song NN.
11:117299189
Brain Res. 2015 Jan 12;1594:61-70. doi: 10.1016/j.brainres.2014.10.060. Epub 2014 Nov 4. DSCAML1 disruptive_inframe_deletion
Missense
Altered Expression of Intersectin1-L in Patients with Refractory Epilepsy and in Experimental Epileptic Rats.
Yang X, Xu X, Zhang Y, Wang S, Li M, Wang X.
21:35144379
Cell Mol Neurobiol. 2015 Aug;35(6):871-80. doi: 10.1007/s10571-015-0181-y. Epub 2015 Mar 18. ? Maternal ITSN1 inframe_deletion Missense
Recurrent Alternate-Sided Homonymous Hemianopia Due to Mitochondrial Encephalomyopathy with Lactic Acidosis and Stroke-Like
Episodes (MELAS): A Case Report.
Krysko KM, Sundaram AN.
Neuroophthalmology. 2016 Sep 23;41(1):30-34. doi: 10.1080/01658107.2016.1224256. eCollection 2017 Feb. Genetic and biochemical
findings in Chinese children with Leigh syndrome.
Ma YY, Wu TF, Liu YP, Wang Q, Song JQ, Li XY, Shi XY, Zhang WN, Zhao M, Hu LY, Yang YL, Zou LP.
MT:10277 J Clin Neurosci. 2013 Nov;20(11):1591-4. doi: 10.1016/j.jocn.2013.03.034. Epub 2013 Aug 13. ? ND3 missense_variant Missense
Increased Cell Proliferations and Neurogenesis in the Hippocampal Dentate Gyrus of Ahnak Deficient Mice.
Shin JH, Kim YN, Kim IY, Choi DH, Yi SS, Seong JK.
11:62289498
Neurochem Res. 2015 Jul;40(7):1457-62. doi: 10.1007/s11064-015-1615-0. Epub 2015 May 26. AHNAK missense_variant Missense
Increased Cell Proliferations and Neurogenesis in the Hippocampal Dentate Gyrus of Ahnak Deficient Mice.
Shin JH, Kim YN, Kim IY, Choi DH, Yi SS, Seong JK.
11:62300105
Neurochem Res. 2015 Jul;40(7):1457-62. doi: 10.1007/s11064-015-1615-0. Epub 2015 May 26. AHNAK missense_variant MissenseDefinition
#1 PATIENT
SEIZURES
inconstant deviation of the head
and eyes to the right shoulder,
gasps, staring eyes, tightening the 4
Clinic limbs, vomiting and loss of
consciousness, lasting between 3 to
10 minutes, followed by
drowsiness and severe headache
and nausea
EEG
NEUROPSYCHOLOGICAL PROFILE
deficiency in the decoding processes of
the written code with severely impaired
visually-cognitive skills
NPS
characterization
bilateral parieto-occipital epileptic foci CSWS pattern during sleep
Treatment
CLINICAL
STUDYDefinition
#2 PATIENT
SEIZURE
at age 9.5 years
on waking, while in bed with her parents,
the girl presented loss of contact with
glare, generalized tremor and hypertone
guttural sounds and light scalpel with
upper limbs and hands claw, lasting
about 4-5 minutes, then followed by a
Clinic long period of general hypotonia with
persistence of fiery look and absence of
contact
NEUROPSYCHOLOGICAL PROFILE
borderline cognitive level (WISC-III TIQ 80,
VIQ 103, PIQ 60)
EEG a significant reading impairment (-2 SD)
insufficient comprehension
deficit in organizational and planning skills
slowness in writing in italics
lacking speed in arithmetic skills
deterioration in visual-perceptive disorder
with very severe visual agnosia and a
NPS disturbance of spatial orientation
characterization
Temporo-occipital epileptic foci. CSWS pattern during sleep
Treatment
CLINICAL
STUDYADEQUATE IQ
IED-related BOLD changes (discrepancy between PIQ and VIQ)
Pt# Pt#
1 2 visuo-spatial
visuo-motor impairment
during ESES/CSWS period
SEVERE VISUAL-PERCEPTIVE DISORDER
VISUAL AGNOSIA
+
DISTURBANCE OF SPATIAL ORIENTATION
A linear relationship was observed
between the number of IEDs and
positive BOLD signal changes in the
left postcentral gyrus (BA3)
(global maximum),
the left fusiform gyrus (BA37), and
the right lingual gyrus (BA 18)
No significant correlation was
found with the age at seizure onset
or epilepsy duration
Single-subject result. Single-subject IED-related BOLD findings in the 2 ICOE patients. The hemodynamic changes have been warped to the
PALS-B12 atlas in Caret, bottom and lateral view. Results are displayed using a threshold of p < 0.05 corrected for FWE for both.
No decreases in BOLD signal were detected in any patient.Definition CLINICAL RELEVANCE
Clinic EXTRASTRIATE VISUAL SYSTEM
selective impairment of functions
limited number of cortical columns
EEG
posterior ventral occipito-temporal cortex
(faces, objects, and letters)
NPS
characterization
EEG paroxysms interfere with physiological functions,
and possibly, with neuroplasticity processes involved in
higher cortical functions [Tassinari and Rubboli, 2006]
Treatment
need for appropriate neuropsychological
testing, individually tailored to specific deficits
and interpreted in the light of the
CLINICAL neurophysiology and functional neuroimaging
STUDYDefinition CSWS: COGNITION
Cognitive regression/Stagnation (>12pts)
Language regression
Clinic Learning disabilities
Behavioural disturbances (ADHD)
Geographical Prominence of SWA
EEG Temporal: LKS
Fronto-Central: Rolandic
Occipital: visuo-spatial
NPS
characterization Common-to-all basic diagnostic assessment
Intelligence
Language
Memory
Treatment Attention
Visuo-spatial
Executive Functions
Clinical
Practices that may beed a consensual attitude
study Repet at regular intervals (once a year?) a core battery of neurocognitive test
Arzimanoglou% Cross., 2019CORNICE TEORICA Karmiloff-Smith,1992 Sviluppo neuropsicologico : Specializzazione cerebrale progressiva delle funzioni Plasticità= Cambiamenti funzionali e strutturali cerebrali che permettono lo svilupparsi delle funzioni (Johnson,2009)
NEUROPSICOLOGIA ED EPILESSIA Anomalie epilettiformi, crisi epilettiche e il substrato neuronale anomalo SNC dinamico, plasticità cerebrale, ambiente Mancato sviluppo Rallentamento Regressione di una funzione Disfunzioni più generali e diffuse (Smith,2010)
EPILESSIA DI SISTEMA (Avanzini, 2012) La spiegazione patofisiologica dell'impatto negativo dell'attività epilettica dipende dall’organizzazione del cervello Pruning costruzione dei network corticosubcorticale Le anomalie epilettiche compromettono questi processi Mantiene connessioni non più utili (in base all’età del bambino e alla richieste dell’ambiente) Impedisce consolidamento di nuove connessioni sinaptiche tra le regioni (Maquet et al., 1995) EE precoce (pruning precoce): precoce specializzazione cerebrale - sistema che elabora troppi tipi di input o perde capacità acquisite in precedenza (ritardo globale/regressione) EE con esordio in età scolare= pruning impedito o aberrante _ no specializzazione cerebrale e ciò potrebbe influire sulla capacità del sistema di multitasking e di integrare le abilità di base in funzioni superiori (Karmiloff-Smith, 2012)= intelligenza normale ma con disturbi specifici, come il linguaggio, le funzioni esecutive, la memoria e l'apprendimento (lettura, scrittura e aritmetica).
VALUTAZIONE Quando? All’esordio controlli 6-9 mesi Come? «minimum routine screening for cognitive and behavioral difficulties» Perché? Ritardo nello sviluppo di competenze Caratterizzazione delle funzioni Follow up Supporto
NEUROPSICOLOGIA E ENCEFALOPATIA EPILETTICA "l'attività epilettica stessa può contribuire a gravi deficit cognitivi e comportamentali al di sopra e al di là di quanto ci si potrebbe aspettare dalla sola patologia sottostante (ad esempio malformazione corticale), così come il fatto che tali menomazioni possono peggiorare nel tempo. ” (Bergel,2010)
onse
t
Durata Tipo di sd
ESES elettroclincia
Fattori
psicosociali eziologi
e a
ambientali
Risposta al Pattern
trattament
o/farmaci EEG
Crisi
epilettiche
tipo e
frequenzaESES «maladaptive plasticity» Issa,2014
ESES= maladaptive plasticity durante i «periodi critici/ sensibili
nello sviluppo» = deficit indotti dalla riorganizzazione di nuovi
circuiti neuronali disadattivi
I disturbi cognitivi osservati sembrano fortemente collegati a periodi
critici/sensibili dello sviluppo.
1) i disturbi iniziano e finiscono quasi nello stesso momento in cui
iniziano e finiscono i periodi critici.
2) L’attività epilettica durante il sonno guida la plasticità in senso
disadattivo durante il periodo critico e la fine del periodo critico
cementa quei cambiamenti disadattivi deficit nps persistenti
3) ll sonno non REM è importante per plasticità del periodo critico e
quindi potrebbe spiegare perché l'interruzione del sonno non
permette i nuovi apprendimentiGruppo 1°: BECTS IEDs NREM sleep 85% 100% di rischio di sviluppo di deficit verbali e disturbi dell’apprendimento Disturbo dell’apprendimento rappresenta un deficit legato ad un processamento di alto livello che coinvolge l’integrazione tra le abilità cognitive di base (memoria, attenzione, linguaggio, percezione) Conclusione: Lo sviluppo ed il mantenimento dei deficit nps dipende dalla frequenza di IED durante il sonno NREM perché non permettono di consolidare gli apprendimenti
Soggetti: ECTS all’esordio, drug naif, QI norma Domini: Linguaggio, EF, apprendimenti scolastici, abilità visuomotorie e visuospaziali, memoria a breve termine Risultati: Deficit: linguaggio, EF, apprendimenti scolastici Ipotesi: Deficit delle FE
EPILESSIA E FE
● Alta frequenza di disfunzioni delle FE in questa
popolazione
● Deficit nelle FE predicono una scarsa qualità della vita
(MacAllister,2014) Deficit nelle FE
Politerapia
Earlier age of
epilepsy onset
Higher seizure
frequency
Bassa qualità della
(Sherman, Slick, & Eyrl, 2006) vitaFE E VITA QUOTIDIANA
Apprendimento di
Monitoraggio e
nuove azioni e Pianificazione e
modifica
comportamenti presa di decisioni
dell’azione
non automatici
Letto-scrittura
Relazioni sociali
Linguaggio
Qualità della vita
successo
Status economico
scolasticoEXECUTIVE FUNCTION «Le funzioni esecutive rappresentano le abilità necessarie per programmare, mettere in atto e portare a termine con successo un comportamento finalizzato a uno scopo»
CONCLUSIONE ESES = esempio paradigmatico dell’EE “Estrema attivazione di anomalie epilettiche durante il sonno NREM causa deficit nelle funzioni neurocognitive e comportamentali al di là di altri fattori intervenienti ((i.e., structural lesions, abnormal preexisting cognitive and behavioral background). Le anomalie epilettiche protratte in un Sistema in via di sviluppo e l’alta plasticità causano deficit nps e comportamentali anche in bambini sani o peggioramento nei bambini con deficit preesistente Importante: EEG- diagnosi, identificazione del focus,IEDs NREM Nuove tecnologie diagnostiche: tecniche di neuroimmagine (fMRI,PET,MEG) Valutazione neuropsicologica – rischio adattamento qualità della vita
NPI
Epilepsy Group
Responsabile: Valentina De Giorgis
Specializzande: Costanza Varesio
Ludovica Pasca
Elisa Salmin
Martina totaro
Epilepsy Nurse: Flavia bocchino
TNFP: Grazia Papalia
Marco Fasce
CHIARA TOTARO
Neuropsicologa Martina Paola Zanaboni
Dietologa Anna Tagliabue
DIETISTE Claudia Trentani
Cinzia Ferraris
MONICA GUGLIELMETTIYou can also read