Enhanced Antitumor Activity of Anti-epidermal Growth Factor Receptor Monoclonal Antibody IMC-C225 in Combination with Irinotecan (CPT-11) against ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
994 Vol. 8, 994 –1003, May 2002 Clinical Cancer Research
Advances in Brief
Enhanced Antitumor Activity of Anti-epidermal Growth Factor
Receptor Monoclonal Antibody IMC-C225 in Combination
with Irinotecan (CPT-11) against Human Colorectal
Tumor Xenografts
Marie C. Prewett, Andrea T. Hooper, Rajiv Bassi, topoisomerase I inhibitors may be an effective therapy
Lee M. Ellis, Harlan W. Waksal, and against chemorefractory colorectal carcinoma tumors.
Daniel J. Hicklin1
Introduction
Department of Immunology, ImClone Systems, Inc., New York, New
York 10014 [M. C. P., A. T. H., R. B., H. W. W., D. J. H.], and Colorectal cancer is the third most common cancer in men
Department of Surgical Oncology, The University of Texas, M. D. and women in the United States with an estimated 130,200 new
Anderson Cancer Center, Houston, Texas 77030 [L. M. E.] cases diagnosed in 2000, including 93,800 patients with colon
cancer and 36,400 with rectal cancer (1). Metastatic colorectal
cancer is the second-leading cause of death from cancer in North
Abstract America, largely because of the poor clinical response of colo-
Colon carcinomas frequently express the epidermal rectal tumors to conventional chemotherapeutics. The topoi-
growth factor receptor (EGFR), and this expression corre- somerase I inhibitor irinotecan (CPT-11) is a water soluble,
lates with more aggressive disease and poor prognosis. Pre- semisynthetic derivative of camptothecin that has shown activ-
vious studies have shown that EGFR blockade by mono- ity against a number of different tumor types in preclinical
clonal antibody IMC-C225 can inhibit the growth of human models and in clinical trials of patients with various human
colon carcinoma tumor cells in vitro and xenografts of these cancers (2). The active metabolite of CPT-11, SN-38, stabilizes
tumors in athymic mice. In this report, we have studied the a ternary complex between the nuclear enzyme topoisomerase I
in vivo activity of IMC-C225 combined with the topoisomer- and double-stranded DNA, which results in replication fork
ase I inhibitor irinotecan (CPT-11) using two models of arrest and chromatid breaks (3). CPT-11 is active clinically in
human colorectal carcinoma in nude mice. IMC-C225 was the second-line treatment of patients with colorectal cancer
tested at a dose of 1 or 0.5 mg administered q3d. CPT-11 was failing or refractory to first-line 5-FU2 and leucovorin therapy
administered at a dose of 100 mg/kg/week or a maximum (4). More recently, CPT-11 administered as a three drug regi-
tolerated dose of 150 mg/kg/week. Treatment with the com- men along with 5-FU and leucovorin has been shown to prolong
bination of IMC-C225 (1 and 0.5 mg) and CPT-11 (100 survival in patients with colorectal cancer that is refractory to
mg/kg) significantly inhibited the growth of established treatment with 5-FU/leucovorin (5). Despite clinical improve-
DLD-1 and HT-29 tumors compared with either CPT-11 or ments attributed to the addition of CPT-11 therapy for meta-
IMC-C225 monotherapy (P < 0.05). Combination therapy static colorectal cancer, nearly all patients will eventually be-
with IMC-C225 (1 mg) and the MTD of CPT-11 (150 mg/kg) come refractory to CPT-11. Thus, new treatment options are
resulted in a regression rate of 100 and 60% of established needed to improve survival in patients with CPT-11 refractory
DLD-1 and HT-29 tumors, respectively. In a refractory colorectal cancer.
tumor model, combined treatment with IMC-C225 and The EGFR and its ligands EGF and TGF-␣ play an impor-
CPT-11 significantly inhibited the growth of CPT-11 refrac- tant role in the growth and survival of human colorectal tumors
tory DLD-1 and HT-29 tumors, whereas either agent alone (reviewed in Refs. 6 and 7). EGF and/or TGF␣ mRNA and
did not control tumor growth. Histological examination of protein are found in a majority of human colorectal tumors and
treated tumors showed extensive tumor necrosis, decreased cell lines, and coexpression of these ligands and EGFR has been
tumor cell proliferation, increased tumor cell apoptosis, and reported, suggesting the potential existence of an autocrine loop.
a marked decrease in tumor vasculature. These results sug- In addition, the expression of EGFR in colorectal cancer corre-
gest that EGFR blockade by IMC-C225 combined with lates with more aggressive disease and poor prognosis. Hence,
blockade of the EGFR receptor may be a useful strategy for
treatment of adenocarcinoma of the colon. IMC-C225 binds the
EGFR with high affinity, competes for ligand binding, and
Received 9/26/01; revised 1/22/02; accepted 2/16/02.
The costs of publication of this article were defrayed in part by the
payment of page charges. This article must therefore be hereby marked
2
advertisement in accordance with 18 U.S.C. Section 1734 solely to The abbreviations used are: 5-FU, 5-fluorouracil; EGFR, epidermal
indicate this fact. growth factor receptor; CPT-11, 7-ethyl-10-[4-(1-piperidino)-1-piper-
1
To whom requests for reprints should be addressed, at ImClone Sys- idino]carbonyloxy-camptothecin (irinotecan); EGF, epidermal growth
tems, Inc., Department of Immunology, 180 Varick Street, New York, factor; TGF, transforming growth factor; MAb, monoclonal antibody;
New York 10014. Phone: (212) 645-1405; Fax: (212) 645-2054; E-mail: MTD, maximum tolerated dose; TUNEL, terminal deoxynucleotidyl
DanH@imclone.com. transferase-mediated dUTP nick end labeling; DAB, diaminobenzidine.
Downloaded from clincancerres.aacrjournals.org on February 13, 2020. © 2002 American Association for Cancer
Research.Clinical Cancer Research 995
down-regulates receptor expression on the cell surface (re- conjugated antiphosphotyrosine MAb (UBI) followed by detec-
viewed in Ref. 8). Several studies have shown that IMC-C225 is tion using the Lumi-GLO method (KPL). Loading equivalence
capable of inhibiting growth of EGFR-expressing tumor cells in of EGFR in each lane was verified by stripping and reprobing
vitro, and treatment with IMC-C225 results in marked inhibition blots with a polyclonal anti-EGFR antibody (Calbiochem, San
of tumor growth in nude mice bearing xenografts of human Diego, CA).
cancer cell lines (8 –10). Moreover, treatment with IMC-C225 in
combination with chemotherapeutic drugs or radiotherapy is Animals
effective in eradicating well-established tumors in nude mice
Female athymic (nu/nu) mice (5– 6 weeks old) were pur-
(8 –11). IMC-C225 is currently in Phases II and III clinical
chased from Harlan Sprague Dawley, Inc. (Indianapolis, IN).
testing in a number of EGFR⫹ malignancies (9). The objective
Mice were housed under pathogen-free conditions in microiso-
of this study was to determine the potential therapeutic utility of
lator cages with laboratory chow and water available ad libitum.
the MAb IMC-C225 when combined with CPT-11 therapy to
All experiments and procedures were performed in accordance
inhibit growth of human colon carcinoma tumor xenografts in a
with the United States Department of Agriculture, Department
nude mouse model.
of Health and Human Services, and NIH policies regarding the
humane care and use of laboratory animals.
Materials and Methods
Cell Lines
Treatment of s.c. Colorectal Carcinoma Xenografts
The colon carcinoma cell lines DLD-1 and HT-29 were
Subcutaneous colon carcinoma tumors were established by
obtained from the American Type Culture Collection (Manas-
injecting 5 ⫻ 106 DLD-1 or HT-29 cells mixed in Matrigel
sas, VA) and maintained in DMEM (DLD-1) or McCoy’s 5A
(Collaborative Research Biochemicals, Bedford, MA) s.c. into
(HT-29) media (Invitrogen, Carlsbad, CA) supplemented with
the left flank of athymic mice. Three separate study designs
10% fetal bovine serum (HyClone, Lenexa, KY) and 2 mM
were used to examine the activity of IMC-C225, irinotecan
GlutaMAX (Invitrogen). Cells were cultured at 37°C in a 5%
(CPT-11; Pharmacia & Upjohn, Kalamazoo, MI), and combi-
CO2 atmosphere and passaged routinely by Trypsin-EDTA (In-
nation therapy.
vitrogen) treatment.
Study Design I. Tumors were allowed to reach 150 –300
mm3 in size, and then mice were randomized into groups of five
Anti-EGFR MAb IMC-C225 animals each. Mice were treated with saline q3d, IMC-C225 at
Clinical grade anti-EGFR MAb IMC-C225 (ERBITUX) 1 mg/dose (q3d), IMC-C225 at 0.5 mg/dose (q3d), CPT-11 at
was produced by the ImClone Systems, Inc. manufacturing 100 mg/kg (q7d), combination treatment with IMC-C225 at 1
facility (Somerville, NJ). mg/dose (q3d) ⫹ CPT-11 at 100 mg/kg (q7d), and IMC-C225 at
0.5 mg/dose (q3d) ⫹ CPT-11 at 100 mg/kg (q7d). Treatment of
Flow Cytometry animals was continued for the duration of the study.
Subconfluent cultures of colon carcinoma cell lines, grown Study Design II. Tumors were allowed to reach 150 –
in 100-mm2 plates, were washed in ice-cold HBSS and detached 300 mm3 in size, and then mice were randomized into groups of
by incubating the monolayers in HBSS with EDTA. Aliquots of 10 animals each. Mice were treated with saline q3d, IMC-C225
106 cells were incubated for 1 h on ice with primary antibody at 1 mg/dose (q3d), CPT-11 at 150 mg/kg (q7d), or combination
(IMC-C225 or control IgG), diluted in PBS with 1% BSA and treatment with IMC-C225 at 1 mg/dose (q3d) ⫹ CPT-11 at 150
0.02% sodium azide (flow buffer). Cells were washed twice mg/kg (q7d). Treatment of animals was continued for the dura-
with flow buffer and then incubated for 30 min on ice with tion of the study.
FITC-labeled goat antihuman IgG Fc-specific secondary anti- Study Design III. Tumors were allowed to reach 150
body (KPL, Gaithersburg, MD) diluted in flow buffer. Cells mm3 in size, and then mice were treated with two cycles of
were washed as above and analyzed for FITC emission intensity CPT-11 (100 mg/kg; days 0 and 7). After two cycles of CPT-11
on an Epics XL (Beckman-Coulter, Hialeah, FL) flow cytome- treatment (day 12), those CPT-11-treated mice with tumor vol-
ter. Dead cells and debris were eliminated from the analysis on umes ⬎ 2-fold the volume on day 0 (“refractory” mice) were
the basis of forward and sideways light scatter. randomized into three groups of seven to eight mice per group.
The frequency of CPT-11 refractory mice was 50 – 60% of the
Phosphorylation Assay total CPT-11-treated group. CPT-11 refractory mice were
Phosphorylation assays were done by seeding DLD-1 or treated with IMC-C225 at 1 mg/dose (q3d), CPT-11 at 100
HT-29 cells at 5 ⫻ 106/150-mm2 tissue culture plate in media mg/kg (q7d), or combination treatment with IMC-C225 at 1
containing 0.5% fetal bovine serum in 5 g/ml IMC-C225 or mg/dose (q3d) ⫹ CPT-11 at 100 mg/kg (q7d). Treatment of
normal human IgG (Jackson Immunoresearch, West Grove, animals was continued for the duration of the study.
PA). After culturing for 24 h, cells were then stimulated with 5 The MTD for CPT-11 therapy was defined as the maxi-
ng/ml EGF or 5 ng/ml TGF-␣ (Sigma Chemical Co., St. Louis, mum dose that did not result in drug-related morbidity and/or
MO) for 20 min at 37°C. Monolayers were than washed with weight loss of ⬎20% of body weight at the beginning of
ice-cold PBS containing 1 mM sodium orthovanadate. Cells therapy. Mice were monitored daily for signs of CPT-11-related
were lysed, immunoprecipitated with IMC-C225, and subjected toxicity (body weight, diarrhea, and lethality).
to Western blot analysis. The phosphorylation patterns were All drug treatments were administered by i.p. injection.
determined by probing the blots with a horseradish peroxidase- Tumors were measured twice each week with calipers, and
Downloaded from clincancerres.aacrjournals.org on February 13, 2020. © 2002 American Association for Cancer
Research.996 IMC-C225 with CPT-11 Inhibits Growth of Colon Tumors
Fig. 1 A, EGFR expression on
DLD-1 and HT-29 colon carcinoma
cells. Flow cytometry analysis histo-
grams of IMC-C225 binding (black)
or a control human antibody (gray).
B, phosphorylation assay showing
IMC-C225 inhibition of EGFR phos-
phorylation. DLD-1 or HT-29 cul-
tures were incubated with IMC-C225
or normal human IgG followed by
stimulation with exogenous EGF or
TGF-␣. Western blotting with an-
tiphosphotyrosine antibody (top pan-
els). Blots were stripped and re-
probed with anti-EGFR antibody
(bottom panels).
tumor volumes were calculated by the formula [/6 (w1 ⫻ successive washes in PBS, sections were coverslipped using an
w2 ⫻ w2)], where “w1” represents the largest tumor diameter, antifade reagent.
and “w2” represents the smallest tumor diameter. For H&E and Ki-67 staining, resected tumors were fixed in
zinc-buffered formalin (Shandon Lipshaw, Pittsburgh, PA)
Histology overnight at 4°C. After paraffin embedding and sectioning at 6
Tumors were harvested from animals at multiple time m, formalin-fixed sections were stained with Mayer’s H&E
points after treatment and snap frozen in liquid nitrogen for (Richard Allen, Kalamazoo, MI). For Ki-67 immunohistochem-
anti-CD31 immunohistochemistry and TUNEL staining. For istry, slides were heated in a water bath at 95°C-99°C in Target
anti-CD31 immunohistochemistry, 6-m cryostat sections were Retrieval Solution (DAKO, Carpinteria, CA) for 20 min, fol-
fixed at room temperature in acetone for 5 min and were lowed by a 20-min cool down period at room temperature. After
postfixed in 10% neutral buffered formalin for 10 s before heat retrieval, sections were rinsed well in PBS and stained with
staining. Endogenous peroxidase activity was blocked by a rabbit antihuman Ki-67 antigen (DAKO N-series, ready to use)
30-min incubation with 0.3% H2O2 in H20. After blocking with per manufacturer’s instructions and were lightly counterstained
5% BSA, 10% normal goat serum ⫹ 0.02% Tween 20, FITC with Mayer’s hematoxylin.
anti-CD31 (clone Mec13.3, BD PharMingen, Franklin Lakes, The Proliferation Index was determined by Ki-67 immu-
NJ), and FITC rat IgG isotype control (PharMingen) were nostaining and calculating the number of DAB-positive pixels
diluted to a final concentration of 1 g/ml in blocking buffer per total number of nuclear pixels (hematoxylin-positive pixels
and were incubated with the tissue sections for 60 min at room plus DAB-positive pixels ⫻ 100) in five fields at ⫻200. The
temperature. Slides were then washed in PBS to remove excess Apoptosis Index, determined by TUNEL staining, is calculated
antibody. Slides were incubated with 1 g/ml horseradish per- from the number of TUNEL-positive pixels per total number of
oxidase-conjugated anti-FITC (Roche Molecular Biochemicals, Hoechst-positive pixels ⫻ 100 in five fields at ⫻200. The
Indianapolis, IN) for 30 min at room temperature and were Apoptosis:Proliferation Ratio equals the Apoptosis Index/Pro-
washed subsequently in PBS. Immunostaining was developed liferation Index ⫻ 1000.
for 4 min using a liquid DAB substrate kit (Zymed, San Fran-
cisco, CA) per manufacturer’s instructions. The reactions were Statistical Analysis
stopped by successive washes in tap and distilled water and Tumor volumes and histological quantitations were ana-
were lightly counterstained with Mayer’s hematoxylin. Sections lyzed using Student’s t test. Antitumor activity of combination
were coverslipped using a permanent mounting medium. therapy with IMC-C225 and CPT-11 in vivo was analyzed by
TUNEL staining was performed using the Apoptosis Detection the fractional product method as described (12). Analyses were
System, Fluorescein (Promega, Madison, WI). Briefly, 6-m computed using the SigmaStat statistical package (v. 2.03; Jan-
cryostat sections were fixed in 4% paraformaldehyde for 10 min del Scientific, San Rafael, CA).
at room temperature and rinsed in PBS with 0.1% Triton X-100.
Sections were then incubated in Equilibration Buffer for 5 min Results
at room temperature followed by incubation in TUNEL Mix, The in vivo effects of IMC-C225 and CPT-11 therapy alone
prepared according to kit instructions, for 1 h at 37°C. After or in combination were tested in a DLD-1 and HT-29 s.c.
Downloaded from clincancerres.aacrjournals.org on February 13, 2020. © 2002 American Association for Cancer
Research.Clinical Cancer Research 997
Fig. 2 Growth inhibition of
DLD-1 and HT-29 colorectal
tumor xenografts in nude mice.
A and B, dose-dependent effects
are shown for treatment of
established DLD-1 (A) and
HT-29 (B) tumors treated with
saline (E), IMC-C225 at 1 mg
(F) or 0.5 mg (‚) per dose/q3d,
CPT-11 at 100 mg/kg/week
(䡺), CPT-11 (100 mg/kg/week)
plus IMC-C225 at 1 mg/dose/
q3d (f), and CPT-11 (100 mg/
kg/week) plus IMC-C225 at 0.5
mg/dose/q3d (Œ). C and D,
combination therapy on estab-
lished DLD-1 (C) and HT-29
(D) tumors treated with saline
(E), IMC-C225 at 1 mg (F),
CPT-11 at 150 mg/kg/week
(䡺), and CPT-11 (150 mg/kg/
week) plus IMC-C225 at 1 mg/
dose/q3d (f). Bars, ⫾SE.
xenograft model in athymic nude mice. DLD-1 and HT-29 cells mice was 150 mg/kg when given q7d (data not shown). The
express moderate levels of EGFR, and IMC-C225 inhibits both MTD of CPT-11 was then used in combination therapy with
EGF and TGF-␣-stimulated EGFR tyrosine phosphorylation in IMC-C225 in the DLD-1 and HT-29 xenograft models (Fig. 2,
both cell lines (Fig. 1, A and B). Three different therapy designs C and D). A total of 17 cycles of IMC-C225 and 7 cycles of
were tested in the DLD-1 and HT-29 tumor models. In therapy CPT-11 was administered. Combination therapy with 1 mg of
schedule I, mice with well-established (⬃200 mm3) DLD-1 or IMC-C225 and 150 mg/kg CPT-11 resulted in a significant
HT-29 tumors were treated by i.p. administration of two differ- inhibition of tumor growth compared with single-agent IMC-
ent doses of IMC-C225 (1 or 0.5 mg; q3d) with or without C225 (P ⬍ 0.002) or compared with single-agent CPT-11 (P ⬍
CPT-11 (100 mg/kg; q7d). A total of 16 cycles of IMC-C225 0.03). In the DLD-1 model, complete inhibition of tumor growth
and 7 cycles of CPT-11 was administered. Treatment with was observed in the majority of animals. In addition, regression
IMC-C225, CPT-11, or the combination was well tolerated for of established DLD-1 tumors was observed in 60% of animals
the duration of therapy. IMC-C225 treatment alone at 1- or treated with the combination of IMC-C225 and CPT-11. The
0.5-mg doses did not significantly inhibit growth of DLD-1 or activity of IMC-C225 and CPT-11 treatment was even more
HT-29 tumors (P ⬎ 0.05; Fig. 2, A and B). Although CPT-11 pronounced in the HT-29 model. Regression of established
treatment alone (100 mg/kg/week) was active against DLD-1 HT-29 tumors was observed in 100% of the animals treated with
(P ⬍ 0.02) tumors, the treatment did not significantly inhibit IMC-C225 and CPT-11 combination therapy. The indices for
growth of HT-29 tumors (P ⬎ 0.05). In contrast, enhanced combination therapy are ⬎1, indicating an enhanced interaction
antitumor activity using combination therapy with IMC-C225 between IMC-C225 and CPT-11. Table 1 summarizes the anal-
and CPT-11 was observed in both DLD-1 and HT-29 tumors ysis of the enhanced combination effect at different time points
compared with mice treated with control, IMC-C225, or CPT-11 during therapy.
alone. The results from studies described above demonstrated that
In the second study design, we attempted to achieve a DLD-1 or HT-29 tumors are poorly responsive to IMC-C225 or
maximal therapeutic effect by increasing the dose of CPT-11 to CPT-11 therapy alone. To further examine the effect of IMC-
the MTD. Pilot studies determined that the MTD of CPT-11 in C225/CPT-11 combination therapy against CPT-11 refractory
Downloaded from clincancerres.aacrjournals.org on February 13, 2020. © 2002 American Association for Cancer
Research.998 IMC-C225 with CPT-11 Inhibits Growth of Colon Tumors
Table 1 Combination therapy with IMC-C225 and CPT-11
Fractional tumor volume (FTV)a relative to control animals
Combination Therapy
Ratio of expected:
Dayb IMC-C225 CPT-11 Expectedc Observed observed FTVd
DLD-1 26 0.577 0.447 0.258 0.254 1.015
29 0.579 0.410 0.237 0.213 1.111
33 0.534 0.365 0.195 0.153 1.272
36 0.506 0.356 0.180 0.133 1.349
HT-29 25 0.481 0.393 0.189 0.162 1.166
28 0.456 0.360 0.164 0.120 1.364
32 0.409 0.310 0.127 0.078 1.638
35 0.411 0.291 0.120 0.054 2.232
a
FTV, calculated as mean tumor volume experimental/mean tumor volume control.
b
Day after start of treatment. Tumor volumes were measured twice weekly (n ⫽ 8 for each group of mice).
c
(Mean FTV of IMC-C225) ⫻ (mean FTV of CPT-11).
d
Obtained by dividing the expected FTV by the observed FTV. A ratio of ⬎1 indicates a more than additive effect, and a ratio of ⬍1 indicates
a less than additive effect.
colorectal tumors, a refractory model was designed and tested. agent alone. Similar findings were observed in DLD-1 tumors.
Animals with established DLD-1 or HT-29 tumors were treated These findings show that the antitumor activity of combined
with two cycles of CPT-11 (100 mg/kg; days 0 and 7). At day treatment with IMC-C225 and CPT-11 is a result of increased
12, tumor volumes were measured, and animals with tumors that tumor cell apoptosis and necrosis compared with treatment with
had increased ⬎2 ⫻ the original tumor volume at the start of either agent alone.
CPT-11 therapy were considered CPT-11 refractory. These mice
were selected and randomized into treatment groups receiving
continued CPT-11 (100 mg/kg; q7d), switched to IMC-C225 Discussion
therapy (1 mg; q3d) or combination therapy on the same sched- EGFR and its ligands EGF and TGF-␣ are important fac-
ule. DLD-1 or HT-29 tumors in animals that continued to tors in the normal physiology of the human gastrointestinal tract
receive CPT-11 grew at similar kinetics before randomization, (for review, see Ref. 13). EGF is a potent epithelial mitogen that
i.e., these tumors did not respond to additional CPT-11 therapy is produced in the Paneth cells of the small intestine and the
(Fig. 3). IMC-C225 therapy alone did not have a significant Brunner’s glands of the duodenum (14). EGF stimulates intes-
antitumor effect on CPT-11 refractory DLD-1 or HT-29 tumors tinal crypt stem cell proliferation in both the small and large
and grew at similar kinetics to those tumors treated with CPT-11 intestine and is an important survival factor for the intestinal
(P ⬎ 0.05 compared with CPT-11-treated mice). In contrast, mucosa (14, 15). EGFR and TGF-␣ expression can be detected
combination therapy with IMC-C225 and CPT-11 significantly in normal epithelial mucosa throughout the gastrointestinal tract
inhibited the growth of CPT-11 refractory DLD-1 or HT-29 (16). The EGFR and its ligands also play an important role in the
tumors (P ⬍ 0.01 and ⬍0.01, respectively) with enhanced growth and survival of human colorectal tumors (6, 7). EGFR is
antitumor activity compared with either agent alone (Table 2). expressed at varying levels in human colorectal tumors and
Histological examination of HT-29 xenografts at day 47 colorectal carcinoma cell lines. Moreover, coexpression of EGF
after treatment showed marked differences in tumors from an- and/or TGF␣ and EGFR has been reported in several human
imals administered the combined IMC-C225/CPT-11 therapy colon tumor cell lines, suggesting the potential existence of an
compared with tumors from animals receiving control or single autocrine stimulatory loop (17–19). In addition, studies have
agent therapy. Extensive tumor necrosis was observed in DLD-1 demonstrated that the EGFR expression level is related to the
and HT-29 tumors treated with a combination of IMC-C225 and progression of the colon cancer disease, as well as survival after
CPT-11 (Fig. 4A). A reduction in tumor cell proliferation (Ki-67 tumor resection (20, 21). The relationship between EGFR ex-
staining), a reduction in tumor vasculature (CD31 staining), and pression and the hepatic metastasis of colon adenocarcinoma
an increase in tumor apoptosis (TUNEL staining) was observed has been reported in a limited number of studies (22). These
in tumors treated with IMC-C225 and CPT-11. Quantitative studies suggest that expression of EGFR in colon carcinoma
analysis of the tumor cell proliferation, apoptosis, and vessel correlates with the ability to produce liver metastases. Hence,
staining showed a significant difference between combination the role of the EGFR signaling pathway in colorectal cancer has
therapy versus control and between combination therapy versus led to considerable interest in the potential therapeutic utility of
single-agent therapy (P ⬍ 0.001 for all comparisons; Fig. 4B). agents that block EGFR function.
In HT-29 tumors, combination treatment resulted in a ⱖ1.4-fold Studies herein were performed to determine the activity
decrease in tumor cell proliferation, a ⱖ2.9-fold increase in of the anti-EGFR MAb IMC-C225 in combination with the
tumor cell apoptosis, and a ⱖ4.3-fold decrease in vessel stain- topoisomerase I inhibitor CPT-11 in colorectal tumor models
ing. The Apoptosis:Proliferation Ratio was increased ⱖ4.5-fold and to provide a rationale for clinical development of this
in IMC-C225/CPT-11-treated tumors compared with either combination. We hypothesized that combining IMC-C225
Downloaded from clincancerres.aacrjournals.org on February 13, 2020. © 2002 American Association for Cancer
Research.Clinical Cancer Research 999
reverse the CPT-11 refractory nature of both HT-29 and
DLD-1 tumors. These results are consistent with a number of
studies demonstrating the same principle; namely, combined
therapy with IMC-C225 and antineoplastic drugs results in a
marked potentiation of antitumor activity compared with
monotherapy. IMC-C225 or its parent murine antibody 225
has been shown to augment the antitumor activity of several
anticancer agents, including cisplatin, doxorubicin, 5-FU,
gemcitabine, and paclitaxel in preclinical models (23–27).
Similar enhancement of activity has been observed in studies
where IMC-C225 is used in combination with irradiation (11,
28, 29). Importantly, the combination of IMC-C225 with
cytotoxic drugs/radiation often results in tumor regression
and, in many cases, eradication of established tumors. It
should be noted that overexpression of EGFR by tumor cells
is not required for the enhanced activity observed when
combining IMC-C225 with chemotherapy and particular in
these studies when combining IMC-C225 with CPT-11. The
two colorectal tumor lines used in our studies express mod-
erate levels of EGFR (⬃1 ⫻ 105) and respond to ligand
stimulation, and receptor activation can be inhibited by treat-
ment with IMC-C225. These findings suggest that the biol-
ogy of the EGFR pathway in tumor cells, rather than the
overall receptor level, is important for the activity of IMC-
C225 when combined with chemotherapeutic agents. The
effectiveness of combining IMC-C225 and chemotherapy or
radiation therapy observed in preclinical studies has been
extended to clinical trials in patients with squamous cell
carcinoma of the head and neck (30, 31).
The activity of IMC-C225 or its parental murine antibody
225 has been demonstrated previously in a number of in vitro
and in vivo preclinical models of human colon adenocarcinoma
(32–34). In these studies, treatment with IMC-C225 inhibited
Fig. 3 Growth inhibition of CPT-11 refractory colorectal tumor xe-
nografts in nude mice. Mice with established DLD-1 (A) or HT-29 (B) the growth of colorectal tumor cells in vitro and growth of s.c.
tumors were treated with two cycles of CPT-11 therapy (100 mg/kg) on tumor xenografts. Combination treatment with IMC-C225 and
days 0 and 7. Mice with tumors that did not respond to CPT-11 therapy other antineoplastic agents or radiation has been shown to
(⬎2 ⫻ initial tumor volume at day 12; shown as dotted vertical line) enhance the antitumor effect against established colorectal tu-
were selected, randomized, and then treated with IMC-C225 at 1 mg/
dose/q3d (F), continued CPT-11 at 100 mg/kg/week (䡺), or combina- mor xenografts (34 –36). Ciardiello et al. (35) tested IMC-C225
tion therapy (f). Bars, ⫾SE. in combination with the topoisomerase I inhibitor topotecan in
the human GEO colon adenocarcinoma xenograft model. Treat-
ment of mice bearing established GEO colon tumors with either
with CPT-11 would enhance the antitumor activity of these IMC-C225 or topotecan alone was ineffective at controlling the
drugs against tumors that are poorly responsive to either drug growth of GEO tumors. However, combined treatment resulted
alone. Our findings show that functional inhibition of EGFR in a significant suppression of tumor growth and almost com-
with IMC-C225 combined with CPT-11 therapy is highly plete tumor regression and a significant survival advantage
effective in two different colorectal tumor models. Impor- compared with animals receiving monotherapy. These results
tantly, HT-29 and DLD-1 colorectal tumor xenografts were are consistent with those obtained in the present study with
found to be poorly sensitive to CPT-11 or IMC-C225 mono- CPT-11. Interestingly, Ciardiello et al. (35) found that sequen-
therapy. However, when IMC-C225 treatment was added to tial treatment with topotecan followed by IMC-C225 therapy
CPT-11 therapy, enhanced tumor growth inhibition was ob- resulted in the most effective antitumor response. In our studies,
served. To further evaluate the enhanced effects of combin- CPT-11 and IMC-C225 was administered to mice simulta-
ing IMC-C225 with CPT-11, we studied the combination of neously during the initial treatment cycle followed by weekly
these two agents in a more rigorous CPT-11 refractory model. CPT-11 treatment with sustained serum levels of IMC-C225
In these experiments, mice with established HT-29 or DLD-1 administered on a q3d schedule. We found no dependency for
tumors that did not respond to CPT-11 therapy were selected sequential treatment with CPT-11 followed by IMC-C225.
and subsequently treated with CPT-11, IMC-C225, or the Moreover, we have found optimal therapeutic effects in animal
combination. Remarkably, IMC-C225 treatment was able to models when CPT-11 and IMC-C225 are administered together
Downloaded from clincancerres.aacrjournals.org on February 13, 2020. © 2002 American Association for Cancer
Research.1000 IMC-C225 with CPT-11 Inhibits Growth of Colon Tumors
Table 2 Response of CPT-11 refractory xenografts to IMC-C225 and CPT-11
Fractional tumor volume (FTV)a relative to control animals
Combination therapy
Ratio of expected:
Dayb Switch to IMC-C225 Continued CPT-11 Expectedc Observed observed FTVd
DLD-1 36 0.566 0.544 0.308 0.269 1.144
40 0.495 0.495 0.245 0.213 1.149
43 0.456 0.475 0.217 0.171 1.268
47 0.404 0.474 0.191 0.143 1.335
50 0.393 0.467 0.184 0.123 1.498
HT-29 36 0.420 0.485 0.204 0.190 1.073
40 0.355 0.439 0.156 0.140 1.115
43 0.345 0.467 0.161 0.120 1.343
47 0.295 0.423 0.125 0.096 1.307
50 0.287 0.405 0.116 0.074 1.562
a
FTV, calculated as mean tumor volume experimental/mean tumor volume control.
Day after start of treatment. Tumor volumes were measured twice weekly (n ⫽ 8 for each group of mice).
b
(Mean FTV of IMC-C225) ⫻ (mean FTV of CPT-11).
c
d
Obtained by dividing the expected FTV by the observed FTV. A ratio of ⬎1 indicates a more than additive effect, and a ratio of ⬍1 indicates
a less than additive effect.
rather than sequentially.3 The discrepancy between our results EGFR⫹ tumors in preclinical models (reviewed in Ref. 8). The
and that of Ciardiello et al. (35) are unclear. These differences direct mechanism responsible for IMC-C225’s activity is inhi-
may be related to drug treatment schedule, pharmacodynamics bition of EGFR tyrosine kinase activation. The outcome of this
of CPT-11 versus topotecan, mechanisms of interaction between blockade is reflected in the disruption of any number of pro-
IMC-C225 and CPT-11 versus topotecan, or differences in the cesses regulated by the EGFR pathway in a given tumor cell.
tumor models. These processes include: (a) regulation of cell cycle progres-
Histological examination of HT-29 and DLD-1 tumors sion; (b) cell survival pathways; (c) tumor cell invasion; and (d)
treated with IMC-C225 and CPT-11 therapy showed marked angiogenesis. Several mechanisms appear to contribute to the
changes in several markers that can be attributed to the antitu- enhanced cytotoxic response observed with combinations of
mor effect of combination therapy. These comprise a decrease in IMC-C225 and chemo/radiation. Genotoxic damage induced by
tumor cell proliferation, an increase in tumor cell apoptosis, and chemotherapy or radiation leads to induction of arrest at the
a reduction in tumor vasculature. The reduction in tumor cell G1-S cell cycle checkpoint or activation of apoptosis; both are
proliferation and tumor vasculature and increase in apoptosis led regulated by the EGFR signaling pathway. Disruption of EGFR-
to extensive tumor necrosis in IMC-C225/CPT-11-treated colo- mediated survival signals and an increase in programmed cell
rectal tumors. The incidence of tumor cell apoptosis suggests death appear to be major mechanisms whereby IMC-C225 syn-
that the effects of IMC-C225/CPT-11 treatment on colon carci- ergizes with cytotoxic agents (8, 11). Changes in the expression
noma tumors in vivo were not merely cytostatic but rather affect or activation of a number of molecules after IMC-C225 treat-
the growth and survival of these tumors. These findings are ment contribute to this response; these include p27 (Kip1),
consistent with those of previous studies that have demonstrated cdk-2, Rb, Bcl-2, and Bax. Studies of sublethal DNA damage
IMC-C225-induced tumor cell apoptosis in other EGFR⫹ hu- repair and potentially lethal damage repair analyses in cultured
man tumor models in nude mice (25, 27, 37). The decreased tumor cells have demonstrated a strong inhibitory effect of
CD31 vessel staining observed in HT-29 and DLD-1 xenografts IMC-C225 on postradiation DNA damage repair (11). These
are also consistent with results of other studies and suggest that studies have also shown that exposure of tumor cells to IMC-
antiangiogenic mechanisms may be associated with IMC-C225 C225 induces a redistribution of DNA-dependent protein kinase
treatment (25, 37, 38). However, given the dramatic antitumor from the nucleus to the cytosol and reduction in proliferating
effect of combination therapy observed in these studies, it is cell nuclear antigen expression, which is known to play a role in
difficult to determine to what extent generalized tumor necrosis DNA repair (39). Hence, IMC-C225 inhibits both survival path-
contributed to the reduction of microvessels in treated tumors. ways and DNA repair mechanisms and, thus, enhances the
We speculate that reduced vasculature in HT-29 and DLD-1 apoptotic potential of chemotherapeutic drugs or radiation that
tumors treated with IMC-C225 and CPT-11 is because of both induce cellular damage and programmed cell death. Finally,
generalized tumor necrosis and a direct effect on neoangio- IMC-C225 may also enhance the response to cytotoxic therapy
genesis. through mechanisms involving reduced angiogenesis and tumor
A number of mechanisms have been identified that char- cell invasion. The mechanisms responsible for the enhanced
acterize the effect of IMC-C225 on the growth and survival of antitumor activity we observed in the present studies have not
been fully defined. Our findings from analysis of HT-29 and
DLD-1 tumors suggest that the enhanced antitumor effects
IMC-C225/CPT-11 therapy are attributable to cell cycle, apo-
3
M. C. Prewett, unpublished data. ptotic, and possibly angiogenic mechanisms of tumor growth.
Downloaded from clincancerres.aacrjournals.org on February 13, 2020. © 2002 American Association for Cancer
Research.Clinical Cancer Research 1001
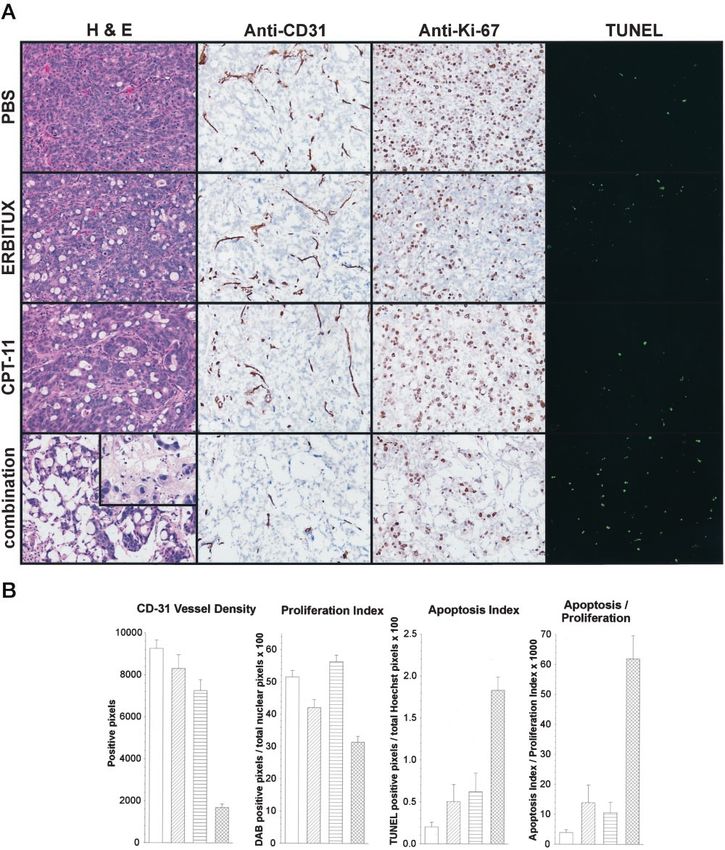
Fig. 4 A, histological examination of HT-29 tumor xenografts (day 47) stained with H&E, anti-CD31 vessel staining (brown), anti-Ki-67 nuclear
antigen (black), and apoptosis by FITC-labeled TUNEL assay (green). (magnification: ⫻200). A higher magnification of combination therapy-treated
HT-29 tumors stained with H&E is shown (inset) to illustrate necrosis in these tumors (⫻400). B, quantitation of CD31 vessel staining, Ki-67
Proliferation Index, Apoptosis Index, and Apoptosis:Proliferation Ratio. Columns, mean number positive pixels in 10 fields. Bars, ⫾SD. Tumors from
mice treated with vehicle (white), IMC-C225 (diagonal hatched), CPT-11 (horizontal hatched), or IMC-C225 plus CPT-11 (cross-hatched).
Downloaded from clincancerres.aacrjournals.org on February 13, 2020. © 2002 American Association for Cancer
Research.1002 IMC-C225 with CPT-11 Inhibits Growth of Colon Tumors
However, additional tumorigenic regulatory processes, such as 13. Chailler, P., and Menard, D. Ontogeny of EGF receptors in the
DNA repair and unknown mechanisms of CTP-11 resistance, human gut. Front. Biosci., 4: D87–D101, 1999.
are likely to play a contributing role. Additional studies will be 14. Reeves, J. R., Richards, R. C., and Cooke, T. The effects of
necessary to fully elucidate the mechanisms contributing to the intracolonic EGF on mucosal growth and experimental carcinogenesis.
Br. J. Cancer, 63: 223–226, 1991.
IMC-C225/CPT-11 antitumor response and determine which
15. Wright, N. A., Pike, C., and Elia, G. Induction of a novel epidermal
molecular pathways are involved in this response. growth factor-secreting cell lineage by mucosal ulceration in human
In conclusion, these results demonstrate enhanced antitu- gastrointestinal stem cells. Nature (Lond.), 343: 82– 85, 1990.
mor activity of IMC-C225 combined with CPT-11 therapy 16. Markowitz, S. D., Molkentin, K., Gerbic, C., Jackson, J., Stellato,
compared with CPT-11 or IMC-C225 treatment alone. This T., and Wilson, J. K. V. Growth stimulation by coexpression of trans-
combination was highly effective against established, CPT-11 forming growth factor-␣ and epidermal growth factor receptor in normal
refractory colorectal tumors. The precise mechanisms responsi- and adenomatous human colon epithelium. J. Clin. Investig., 86: 356 –
362, 1990.
ble for the combined effects of IMC-C225 and CPT-11 in these
colorectal tumor models are still unclear and will require addi- 17. Huang, S. M., Lin, P. F., Fan, D., Price, J. E., Trujillo, J. M., and
Chakrabarty, S. Growth modulation by epidermal growth factor (EGF)
tional studies. Nevertheless, the ability of combination therapy in human colonic carcinoma cells: constitutive expression of the human
to inhibit growth of chemoresistant colorectal carcinoma tumors EGF gene. J. Cell. Physiol., 148: 220 –227, 1991.
suggests that EGFR blockade by IMC-C225 combined with 18. Coffey, R. J., McCutchen, C. M., Graves-Deal, R., and Polk, W. H.,
CPT-11 has potential as a promising therapeutic strategy for Jr. Transforming growth factors and related peptides in gastrointestinal
clinical testing in CPT-11 refractory colorectal cancer. neoplasia. J. Cell. Biochem. Suppl., 16G: 111–118, 1992.
19. Howell, G. M., Sun, L. Z., Ziober, B. L., Wu, S. P., and Brattain,
M. G. The role of growth regulatory aberrations in progression of human
Acknowledgments colon carcinoma. Cancer Metastasis Rev., 12: 275–286, 1993.
We thank Dr. Peter Bohlen for critical review of the manuscript 20. Mayer, A., Takimoto, M., Fritz, E., Schellander, G., Kofler, K., and
and Sarah Michaud for assistance in preparation of the manuscript. We Ludwig, H. The prognostic significance of proliferating cell nuclear
dedicate this work to the memory of our good friend and colleague, antigen, epidermal growth factor receptor, and mdr gene expression in
Angel Santiago. colorectal cancer. Cancer (Phila.), 71: 2454 –2460, 1993.
21. De Jong, K. P., Stellema, R., Karrenbeld, A., Koudstaal, J., Gouw,
A. S., Sluiter, W. J., Peeters, P. M., Slooff, M. J., and De Vries, E. G.
References Clinical relevance of transforming growth factor ␣, epidermal growth
1. Greenlee, R. T., Murray, T., Bolden, S., and Wingo, P. A. Cancer factor receptor, p53, and Ki67 in colorectal liver metastases and corre-
statistics, 2000. CA Cancer J. Clin., 50: 7–33, 2000. sponding primary tumors. Hepatology, 28: 971–979, 1998.
2. Saijo, N. Preclinical and clinical trials of topoisomerase inhibitors. 22. Radinksy, R., Risin, Fan, Dong, Bielenberg, Bucana, C. D., and
Ann. N. Y. Acad. Sci., 922: 92–99, 2000. Fidler, J. Level and function of epidermal growth factor receptor predict
3. Rivory, L. P. Irinotecan (CPT-11): a brief overview. Clin. Exp. the metastatic potential of human colon carcinoma cells. Clin. Cancer
Pharmacol. Physiol., 23: 1000 –1004, 1996. Res., 1: 19 –31, 1995.
4. Rothenberg, M. L., Cox, J. V., DeVore, R. F., Hainsworth, J. D., 23. Baselga, J., Norton, L., Masui, H., Pandiella, A., Coplan, K., Miller,
Pazdu, R., Rivkin, S. E., Macdonald, J. S., Geyer, C.E. J.r, Sandbach, J., W. H., Jr., and Mendelsohn, J. Antitumor effects of doxorubicin in
Wolf, D. L., Mohrland, J. S., Elfring, G. L., Miller, L. L., and Von Hoff, combination with anti-epidermal growth factor receptor monoclonal
D. D. A multicenter, phase II trial of weekly irinotecan (CPT-11) in antibodies. J. Natl. Cancer Inst. (Bethesda), 85: 1327–1333, 1993.
patients with previously treated colorectal carcinoma. Cancer (Phila.), 24. Prewett, M., Rockwell, P., Rose, C., and Goldstein, N. I. Anti-tumor
85: 786 –795, 1999.
and cell cycle responses in KB cells treated with a chimeric anti-EGFR
5. Saltz, L. B., Cox, J. V., Blanke, C., Rosen, L. S., Fehrenbacher, L., monoclonal antibody in combination with cisplatin. Int. J. Oncol., 9:
Moore, M. J., Maroun, J. A., Ackland, S. P., Locker, P. K., Pirotta, N., 217–224, 1996.
Elfring, G. L., and Miller, L. L. Irinotecan plus fluorouracil and leu-
25. Bruns, C. J., Harbison, M. T., Davis, D. W., Portera, C. A., Tsan, R.,
covorin for metastatic colorectal cancer. Irinotecan study group.
N. Engl. J. Med., 343: 905–914, 2000. McConkey, D. J., Evans, D. B., Abbruzzese, J. L., Hicklin, D. J., and
Radinsky, R. Epidermal growth factor receptor blockade with C225 plus
6. Salomon, D. S., Bradt, R., Ciardiello, F., and Normanno, N. Epider- gemcitabine results in regression of human pancreatic carcinoma grow-
mal growth factor-related peptides and their receptors in human malig- ing orthotopically in nude mice by antiangiogenic mechanisms. Clin.
nancies. Crit. Rev. Oncol. Hematol., 19: 183–232, 1995. Cancer Res., 6: 1936 –1948, 2000.
7. Normanno, N., De Luca, A., Salomon, D. S., and Ciardiello, F. 26. Overholser, J. P., Prewett, M. C., Hooper, A. T., Waksal, H. W., and
Epidermal growth factor-related peptides as targets for experimental Hicklin, D. J. Epidermal growth factor receptor blockade by antibody
therapy of human colon carcinoma. Cancer Detect. Prev., 22: 62– 67, IMC-C225 inhibits growth of human pancreatic carcinoma xenografts in
1998. nude mice. Cancer (Phila.), 89: 74 – 82, 2000.
8. Mendelsohn, J. Blockade of receptors for growth factors: an antican- 27. Inoue, K., Slaton, J. W., Perrotte, P., Davis, D. W., Bruns, C. J.,
cer therapy. Clin. Cancer Res., 6: 747–753, 2000. Hicklin, D. J., McConkey, D. J., Sweeney, P., Radinsky, R., and Dinney,
9. Mendelsohn, J. The epidermal growth factor receptor as a target for C. P. Paclitaxel enhances the effects of the anti-epidermal growth factor
cancer therapy. Endocr. Relat. Cancer, 8: 3–9, 2001. receptor monoclonal antibody ImClone C225 in mice with metastatic
10. Waksal, H. W. Role of an anti-epidermal growth factor receptor in human bladder transitional cell carcinoma. Clin. Cancer Res., 6: 4874 –
treating cancer. Cancer Metastasis Rev., 18: 427– 436, 1999. 4884, 2000.
11. Huang, S. M., and Harari, P. M. Modulation of radiation response 28. Saleh, M. N., Raisch, K. P., Stackhouse, M. A., Grizzle, W. E.,
after epidermal growth factor receptor blockade in squamous cell car- Bonner, J. A., Mayo, M. S., Kim, H-G., Meredith, R. F., Wheeler, R. H.,
cinomas: inhibition of damage repair, cell cycle kinetics and tumor and Buchsbaum, D. J. Combined modality therapy of A431 human
angiogenesis. Clin. Cancer Res., 6: 2166 –2174, 2000. epidermoid cancer using anti-EGFr antibody C225 and radiation. Can-
12. Yokoyama, Y., Dhanabal, M., Griffioen, A. W., Sukhatme, V. P., cer Biother. Radiopharm., 14: 451– 463, 1999.
and Ramakrishnan, S. Synergy between angiostatin and endostatin: 29. Milas, L., Mason, K., Hunter, N., Petersen, S., Yamakawa, M., Ang,
inhibition in ovarian cancer growth. Cancer Res., 60: 2190 –2196, 2000. K., Mendelsohn, J., and Fan, Z. In vivo enhancement of tumor radiore-
Downloaded from clincancerres.aacrjournals.org on February 13, 2020. © 2002 American Association for Cancer
Research.Clinical Cancer Research 1003
sponse by C225 anti-epidermal growth factor receptor antibody. Clin. growth factor receptor and protein kinase A. J. Natl. Cancer Inst.
Cancer Res., 6: 701–708, 2000. (Bethesda), 88: 1770 –1776, 1996.
30. Robert, F., Ezekiel, M. P., Spencer, S. A., Meredith, R. F., Bonner, 35. Ciardiello, F., Bianco, R., Damiano, V., De Lorenzo, S., Pepe, S.,
J. A., Khazaeli, M. B., Saleh, M. N., Carey, D., LoBuglio, A. F., De Placido, S., Fan, Z., Mendelsohn, J., Bianco, A. R., and Tortora, G.
Wheeler, R. H., Cooper, M. R., and Waksal, H.W. Phase I study of Antitumor activity of sequential treatment with topotecan and anti-
anti-epidermal growth factor receptor antibody cetuximab in combina- epidermal growth factor receptor monoclonal antibody C225. Clin.
tion with radiation therapy in patients with advanced head and neck Cancer Res., 5: 909 –916, 1999.
cancer. J. Clin. Oncol., 19: 3234 –3243, 2001. 36. Bianco, C., Bianco, R., Tortora, G., Damiano, V., Guerrieri, P.,
31. Shin, D. M., Donato, N. J., Perez-Soler, R., Shin, H. J., Wu, J. Y., Montemaggi, P., Mendelsohn, J., De Placido, S., Bianco, A. R., and
Zhang, P., Lawhorn, K., Khuri, F. R., Glisson, B. S., Myers, J., Clay- Ciardiello, F. Antitumor activity of combined treatment of human can-
man, G., Pfister, D., Falcey, J., Waksal, H., Mendelsohn, J., and Hong, cer cells with ionizing radiation and anti-epidermal growth factor re-
W. K. Epidermal growth factor receptor-targeted therapy with C225 and ceptor monoclonal antibody C225 plus type I protein kinase A antisense
cisplatin in patients with head and neck cancer. Clin. Cancer Res., 7: oligonucleotide. Clin. Cancer Res., 6: 4343– 4350, 2000.
1204 –1213, 2001. 37. Perrotte, P., Matsumoto, T., Inoue, K., Kuniyasu, H., Eve, B. Y.,
32. Karnes, W. E., Jr., Walsh, J. H., Wu, S. V., Kim, R. S., Martin, Hicklin, D. J., Radinsky, R., and Dinney. C.P.N. Anti-epidermal growth
M. G., Wong, H. C., Mendelsohn, J., Park, J. G., and Cuttittal, F. factor receptor antibody C225 inhibits angiogenesis in human transi-
Autonomous proliferation of colon cancer cells that coexpress trans- tional cell carcinoma growing orthotopically in nude mice. Clin. Cancer
forming growth factor ␣ and its receptor. Variable effects of receptor- Res., 5: 257–265, 1999.
blocking antibody. Gastroenterology, 102: 474 – 485, 1992. 38. Petit, A. M. V., Rak, J., Hung, M-C., Rockwell, P., Goldstein, N.,
33. Wu, X., Fan, Z., Masui, H., Rosen, N., and Mendelsohn, J. Apo- Fendly, B., and Kerbel, R. S. Neutralizing antibodies against epidermal
ptosis induced by an anti-epidermal growth factor receptor monoclonal growth factor and ErB-2/neu receptor tyrosine kinases down-regulate
antibody in a human colorectal carcinoma cell line and its delay by vascular endothelial growth factor production by tumor cells in vitro and
insulin. J. Clin. Investig., 95: 1897–1905, 1995. in vivo. Am. J. Pathol., 151: 1523–1530, 1997.
34. Ciardiello, F., Damiano, V., Bianco, R., Bianco, C., Fontanini, G., 39. Hasan, S., Hassa, P. O., Imhof, R., and Hottiger, M. O. Transcrip-
De Laurentiis, M., De Placido, S., Mendelsohn, J., Bianco, A. R., and tion coactivator p300 binds PCNA and may have a role in DNA repair
Tortora, G. Antitumor activity of combined blockade of epidermal synthesis. Nature (Lond.), 410: 387–391, 2001.
Downloaded from clincancerres.aacrjournals.org on February 13, 2020. © 2002 American Association for Cancer
Research.Enhanced Antitumor Activity of Anti-epidermal Growth Factor
Receptor Monoclonal Antibody IMC-C225 in Combination with
Irinotecan (CPT-11) against Human Colorectal Tumor
Xenografts
Marie C. Prewett, Andrea T. Hooper, Rajiv Bassi, et al.
Clin Cancer Res 2002;8:994-1003.
Updated version Access the most recent version of this article at:
http://clincancerres.aacrjournals.org/content/8/5/994
Cited articles This article cites 36 articles, 13 of which you can access for free at:
http://clincancerres.aacrjournals.org/content/8/5/994.full#ref-list-1
Citing articles This article has been cited by 48 HighWire-hosted articles. Access the articles at:
http://clincancerres.aacrjournals.org/content/8/5/994.full#related-urls
E-mail alerts Sign up to receive free email-alerts related to this article or journal.
Reprints and To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Subscriptions Department at pubs@aacr.org.
Permissions To request permission to re-use all or part of this article, use this link
http://clincancerres.aacrjournals.org/content/8/5/994.
Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
Rightslink site.
Downloaded from clincancerres.aacrjournals.org on February 13, 2020. © 2002 American Association for Cancer
Research.You can also read

















































