ESMO SUMMIT AFRICA 2020 - Current Advances in Radiation Therapy in Head and Neck Cancer - OncologyPRO
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ESMO SUMMIT AFRICA 2020 Current Advances in Radiation Therapy in Head and Neck Cancer Kevin Harrington The Institute of Cancer Research, London Cape Town 14.2.2020
CONFLICT OF INTEREST DISCLOSURE Research Funding Elekta (MR-Linac Consortium) MSD (investigator-initiated studies of pembrolizumab + radiotherapy) Honoraria/Speaker’s Fees Elekta (MR-Linac Consortium) MSD Pfizer
CHEMO-RT FOR LOCALLY-ADVANCED DISEASE Level I, A evidence
Post-operative Chemo-RT
459 pts 334 pts
Surgery Surgery
231 228 167 167
60-66 Gy/30-33F 66 Gy/33F
60-66 Gy/30-33F 66 Gy/33F
CDDP 100 mg/m2 d1, 22, 43 CDDP 100 mg/m2 d1, 22, 43
• L-R control HR = 0.61 (95% 0.41-0.91) • 5 year PFS = 47% C-RT vs 36% RT
• 2-year L-R control = 82% C-RT vs 72% RT • OS HR = 0.70 (95% 0.52-0.95)
• DFS HR = 0.78 (95% 0.61-0.99) • 5-year OS = 53% C-RT vs 40% RT
• OS HR = 0.84 (95% 0.65-1.09)
RTOG 9501 Cooper et al NEJM 2004; 350: 1937 EORTC Bernier et al NEJM 2004; 350: 1945
Level I, A evidence
Phase III Trial of Cetuximab and RT
- Acneiform rash
- No greater toxic effect (including mucositis) by combined treatment
Bonner et al. NEJM 2006; 354: 567
Level II, B evidence Bonner et al. Lancet Oncol. 2010; 11: 21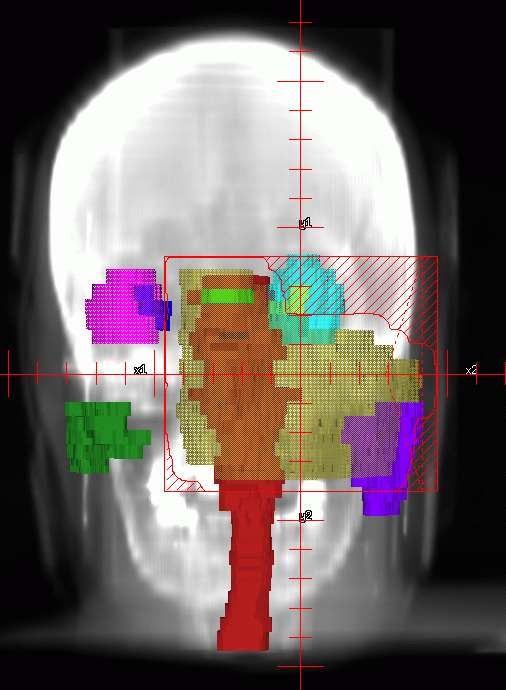
CT Image-Guided RT
RT source
On-board
imaging
CT Planning – Beam’s-Eye-View
CT Planning - Dose Calculation

CT Plan - 3D Plan Evaluation
GOOD FOR
TUMOUR
CONTROL
GOOD FOR
REDUCING
TOXICITYIrradiating Concave Structures
Conventional Intensity-Modulated
Radiotherapy Radiotherapy
Tumour
Dose
TissueDelivery of IMRT
Target
OAR
Intensity
IMB 1Target
OAR
Intensity
IMB 1Target IMB 2 OAR
Target IMB 2 OAR
IMB 4
IMB 3
Target
OAR IMB 5
IMB 2
IMB 1IMB 4
IMB 3
Target
OAR IMB 5
IMB 2
IMB 1PARSPORT Trial Design
Head and neck cancer patients
at risk of radiation-induced xerostomia
(oropharynx/hypopharynx)
Randomisation 1:1
Conventional radiotherapy Parotid-sparing IMRT
(CRT)
65 Gy/30 fractions in 6 weeks - radical and post-operative R1/R2
60 Gy/30 fractions in 6 weeks - post-operative R0
Nutting et al. Lancet Oncol. 2011;12:127-36.3D Conformal RT versus IMRT
Conventional IMRT sparing
radiotherapy parallel left parotid
opposed fields
Nutting et al. Lancet Oncol. 2011;12:127-36.LENT SOM Subjective Xerostomia* rates
p=0.04 p=0.01 p=0.004 p=0.003
86
83
74 71
62 60
CRT
Percentage
IMRT
≥G2 39
29
n=40 n=45 n=36 n=45 n=34 n=38 n=21 n=31
3 6 12 18
Months post treatment * partial but persistent or complete dryness
Nutting et al. Lancet Oncol. 2011;12:127-36.Measurable Sialometry to 12 months
CRT
Percentages of stimulated, measurable sialometry by visit :
IMRT
ipsilateral contralateral
70 70
60 60
50 50
40 40
30 30
20 20
10 10
0 47 47 29 32 33 35 26 33 0 47 47 29 34 34 38 26 34
b/l 3mo 6mo 12mo b/l 3mo 6mo 12mo
Nutting et al. Lancet Oncol. 2011;12:127-36.Overall Survival
1.00
Proportion alive
0.75
1 year overall survival (95% CI):
CRT
CRT (n=47): 90.8% (77.3 – 96.4)
0.50
IMRT
IMRT (n=47): 93.6% (81.5 – 97.9)
0.25
Hazard Ratio (IMRT:CRT) = 1.05 (0.38 to 2.90)
0.00
0 3 6 9 12 15 18
Months from end of treatment
n events/at risk
CRT 0/47 1/44 3/40 3/32
IMRT 0/47 1/47 2/45 5/34
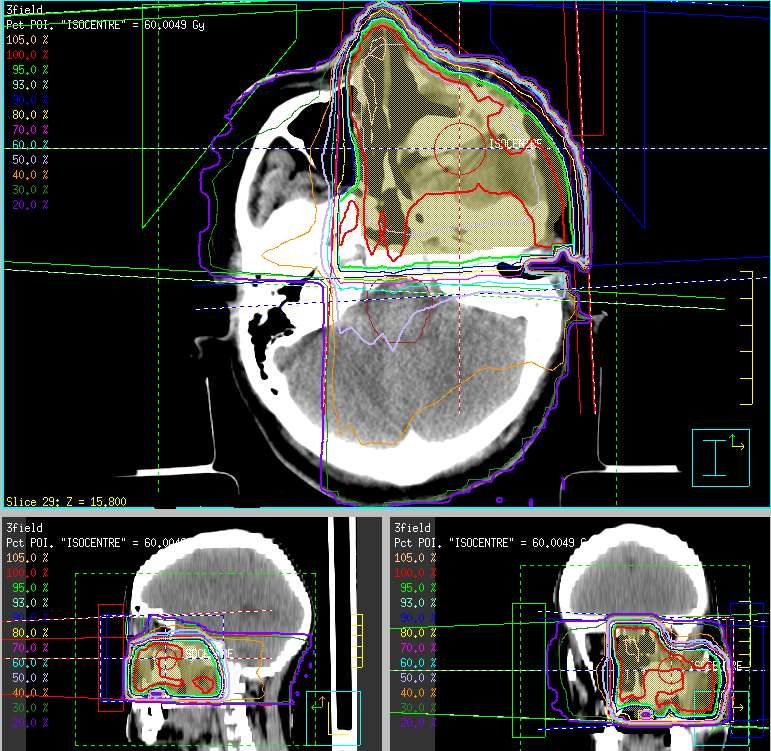
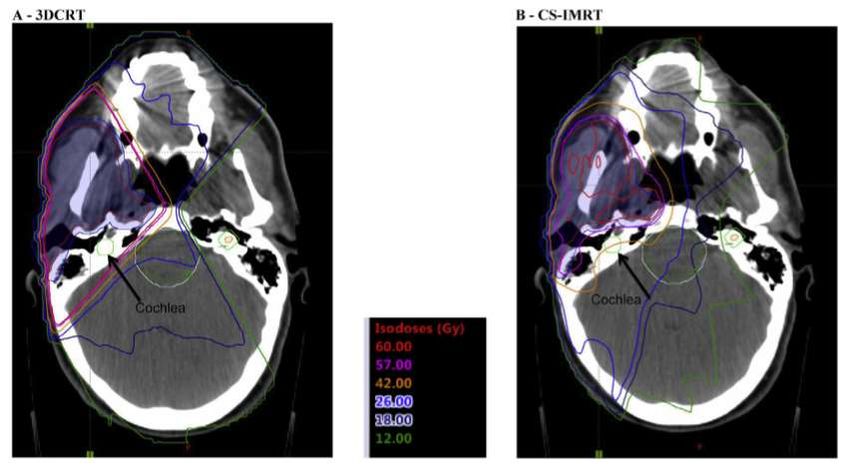
Nutting et al. Lancet Oncol. 2011;12:127-36.• Cochlea inside 95% isodose • Cochlea dose 50 Gy • Excellent target volume coverage • Threshold for sensori-neural loss 40 Gy • Dose to oral cavity and parotid low Nutting et al. European Journal of Cancer 103 (2018) 249e258
Nutting et al. European Journal of Cancer 103 (2018) 249e258
Nutting et al. European Journal of Cancer 103 (2018) 249e258
Results Nutting et al. European Journal of Cancer 103 (2018) 249e258
Results Nutting et al. European Journal of Cancer 103 (2018) 249e258
Results Nutting et al. European Journal of Cancer 103 (2018) 249e258
Results Nutting et al. European Journal of Cancer 103 (2018) 249e258
Quality of Life Outcomes Nutting et al. European Journal of Cancer 103 (2018) 249e258
Dose-escalation by IMRT – Laryngo-Hypopharyngeal Cancer
Radiother. Oncol 2007
IJROBP 2011Phase III Trial Dose-escalated IMRT
DL1 DL2
PTV1: 65 Gy PTV1: 67.2 Gy
2.167 Gy/# 2.4Gy/#
30 fractions 28 fractions
PTV2:
PTV2:
1.8 Gy/#
2.0 Gy/#
CT axial image
primary CTV (green/yellow) and nodal CTV (magenta)
32Phase III Trial Dose-escalated IMRT
DL1 DL2
PTV1: 65 Gy PTV1: 67.2 Gy
2.167 Gy/# 2.4Gy/#
30 fractions 28 fractions
PTV2:
PTV2:
1.8 Gy/#
2.0 Gy/#
REPORTED AT ASCO 2018 – FAILED TO MEET PRIMARY ENDPOINTin partnership with
DARS Trial Schema
102 patients undergoing radiotherapy for cancer in the oropharynx or
hypopharynx, fulfilling all eligibility criteria
Registration
Baseline evaluations
PROs, WST, PSS-HN, toxicity
Videofluoroscopy (VF)
Induction CT Sub Study (limited
(optional by centre)
number of sites) –
Randomisation (1:1) baseline VF
Concomitant CT
(unless contra- Standard Dysphagia-optimised
indicated) IMRT IMRT
Follow up: VF Sub Study
3, 6, 12, 18, 24 months post RT: PROs, WST, PSS-HN, acute and long 12 and 24 months post
term toxicity. RT
3, 4, 5 years post RT: recurrences, new secondary cancers.
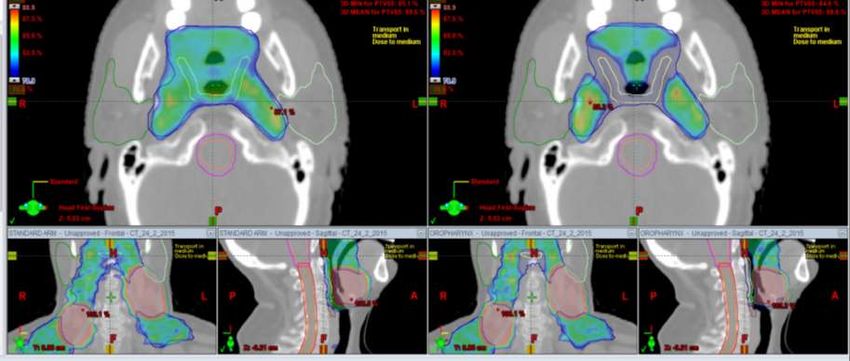
35PTV54 coverage
Standard Arm Experimental Arm
36DARS objectives/endpoints Primary objective: To determine if using dysphagia-optimised IMRT to reduce the radiation dose delivered to the dysphagia/ aspiration related structures (DARS) improves swallowing function compared to standard IMRT Primary endpoint: Difference in mean MDADI composite score at 12 months
The Problem of Margins
Margin
Tumour
Uwe OelfkeMR Image-Guided RT
Accelerator
MRI with ring gantry
MLC
beamMR-Linac at Royal Marsden
The New Gold-Standard?
bladder
GTV primary tumor
rectum
CERVIX
CERVIX
PROSTATE LUNGMR-Linac Consortium
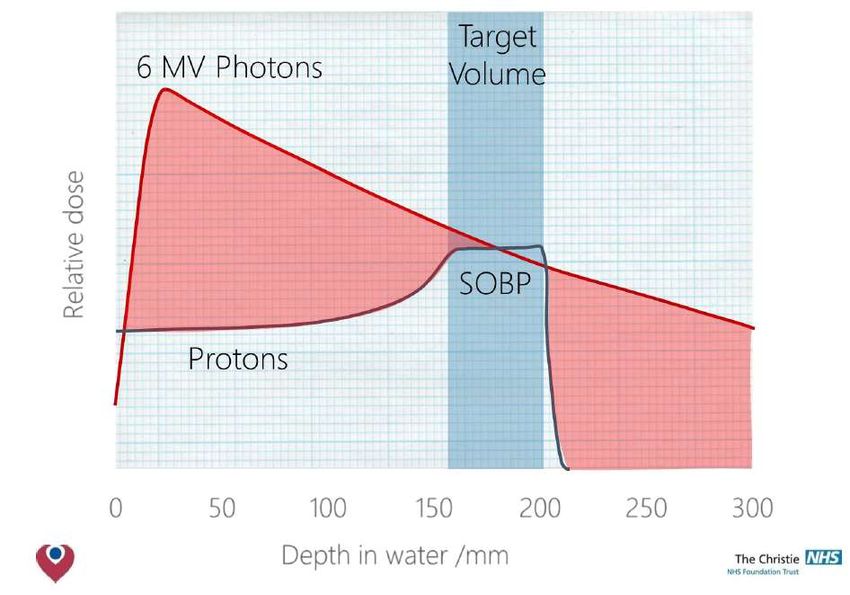
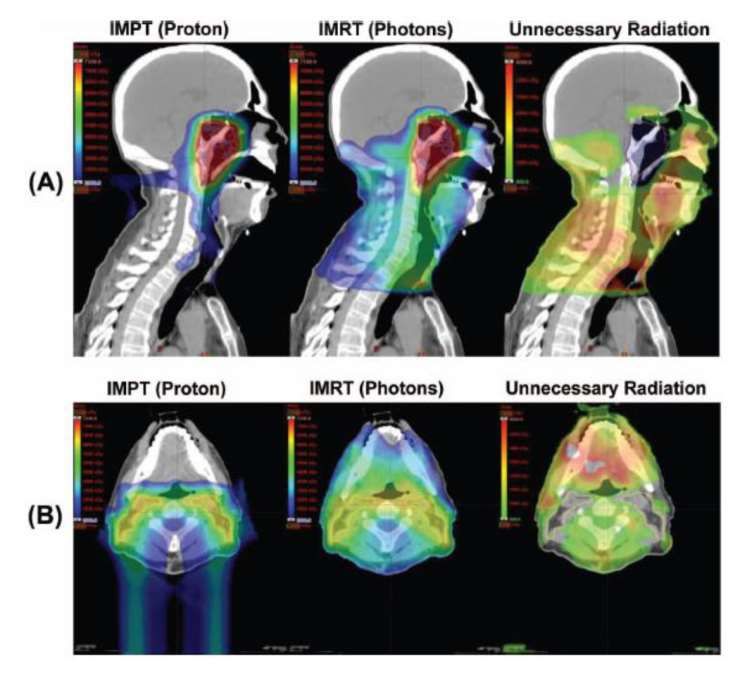
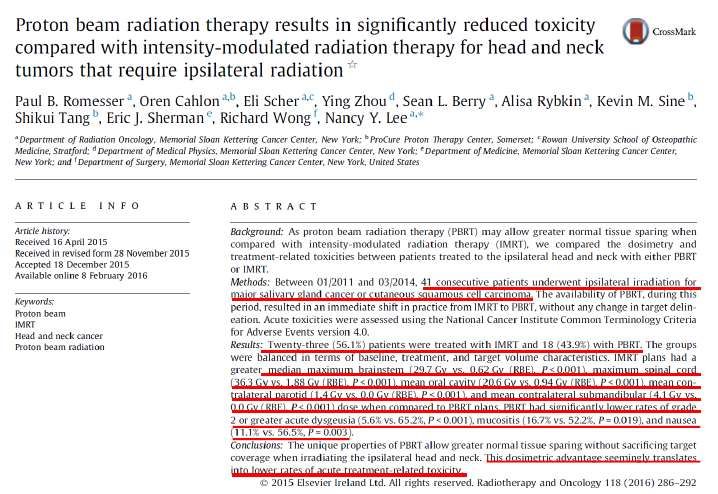
Proton Beam Therapy
LA SCCHN: PD-L1/PD-1 Plus CRT
LEAD-IN TREATMENT MAINTENANCE FOLLOW-
JAVELIN HEAD AND UP
Cisplatin/RT*
NECK 100
AVELUMAB + AVELUMAB
AVELUMAB
(10 mg/kg )
q2w
Eligibility criteria:
• LA SCCHN
R 12 months F/U†
• HPV+ AND HPV- 7 weeks
˗ HPV- STAGE III, IVA, IVB 1:1
˗ HPV+ T4/N2C/N3
Cisplatin/RT Placebo
N = 640 Placebo * q2w
+ Placebo
KEYNOTE-412TAKE HOME MESSAGES 1. Head and neck radiotherapy has changed beyond recognition in the last 3 decades 2. High tech solutions are seductive, but do not always deliver the hypothesised benefits in clinical trials 3. Combinations of optimised radiotherapy technique/technology with biological response modifiers represents the greatest hope of future benefits
Acknowledgements
Chris Nutting
Uwe Oelfke
David Dearnaley
Dow-Mu Koh
Fiona Hemsley, Liz Bishop, Angela McDonald
Consultant Oncologists at RMH
Consultant Radiologists at RMH
MR-Linac Consortium
ElektaYou can also read