EULAR 2018 WIN session: What is new in the treatment of myositis? - The University of Manchester
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
EULAR 2018 WIN session:
What is new in the treatment of myositis?
Dr Hector Chinoy PhD FRCP
@drhectorchinoy
Senior Lecturer / Honorary Consultant Rheumatologist
Salford Royal NHS Foundation Trust
Manchester Academic Health Science Centre
The University of Manchester, UK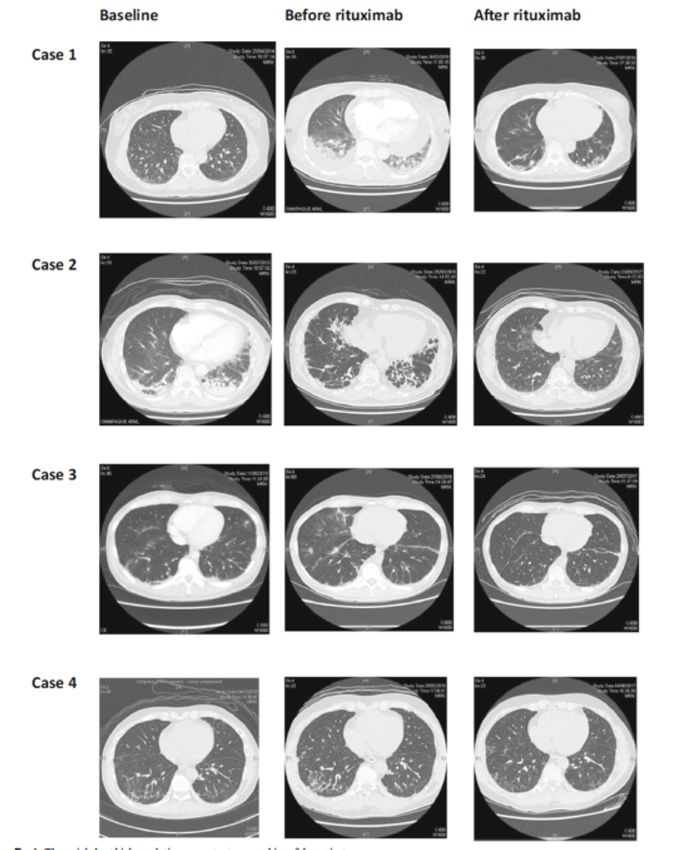
Myositis / idiopathic inflammatory
myopathy (IIM) is an orphan disease
32 incident cases of IIM diagnosed Incidence
in 10 year period in Salford, UK (2007-2016) (1,000,000 person
years)
Whole
18
population
Male 10
Female 25
(A rare disease is defined by the EU as
< 5 in 10,000 general population – raredisease.org.uk)
Parker et al. Increasing incidence of adult idiopathic inflammatory myopathies: a ten-year uk epidemiological study
Ann Rheum Dis, volume 77, supplement Suppl, year 2018, page A757 (Poster - FRI0455)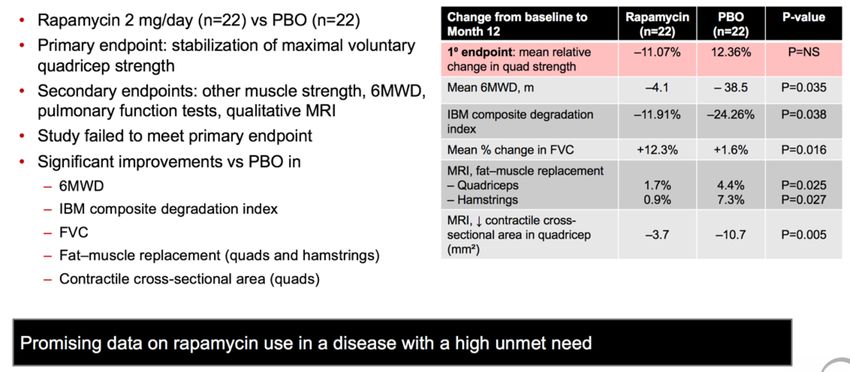
Myositis Spectrum Disease
Creatine
ATP ATP
Creatine Kinase
ADP ADP + H+
Creatine phosphate
IIM: Treating a rare, heterogeneous disease is challenging
Incompletely understood aetiopathogenesis
Few randomized controlled clinical trials, lack of
statistical power - treatment strategies mostly empirical
Multidisciplinary approach, tailored to disease activity
and clinical serotype/phenotype
Goal is to improve muscle strength, suppress extra-
muscular manifestations, minimize risk of complications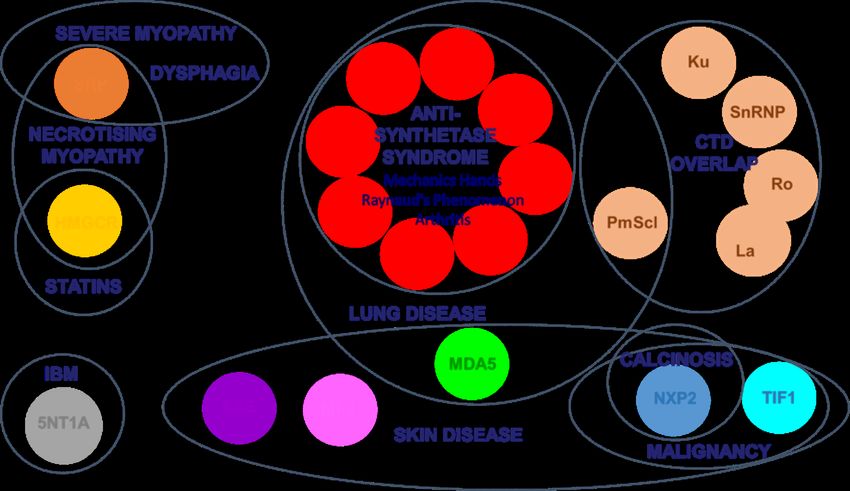
Treatment of IIM is challenging:
diagnosis, assessing disease, treatment success?
Correct diagnosis
• other myopathies may have similar clinical presentation (also PM vs IBM)
• inflammation on biopsy does not exclude other diagnoses
• treatment resistance should prompt reappraisal of diagnosis
Assessing disease
• muscle weakness… is it activity (ongoing immune-mediated process), or damage (fatty replacement/ atrophy)?
• poor prognostic features may direct drug selection/ treatment strategy (lung, cardiac, dysphagia, malignancy)
Treatment success measured as improvement in major manifestations of disease…by
muscle strength & improvement in skin rash or organ involvement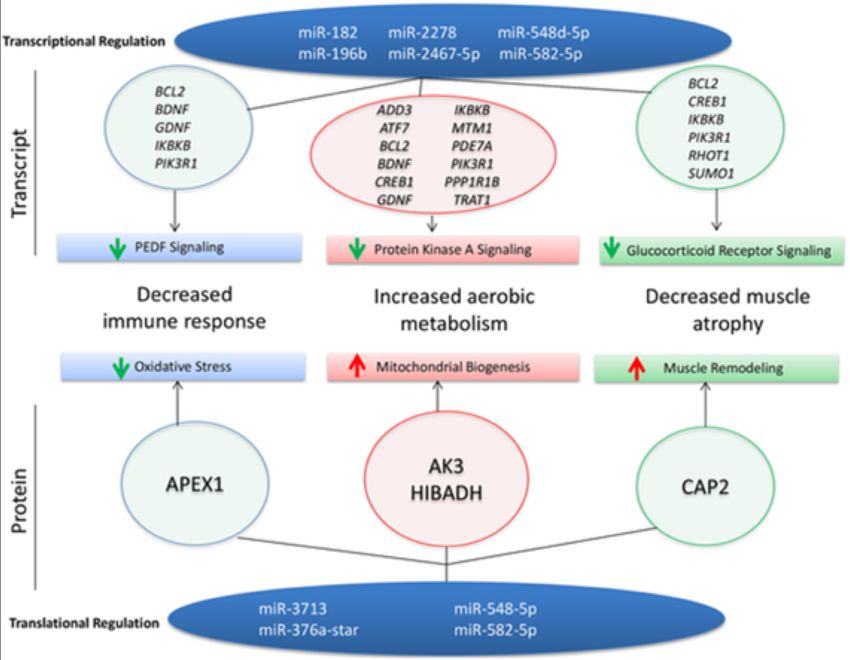
Think about Inclusion Body Myositis…
Inclusion bodies HLA-1 upregulation Protein accumulation
Rimmed vacuoles
• >50, male predominance
• CK < 5x ULN (15 ULN)
• Antibody negative (Ro)
• Fatty atrophy at presentations
• Assymmetrical weakness
• Finger flexor/distal
involvement
• CK but no clinical response
COX negative fibres Endomysial inflammation
Also seen in polymyositis Histopathology courtesy of Dr Daniel DuPlessis, SRFT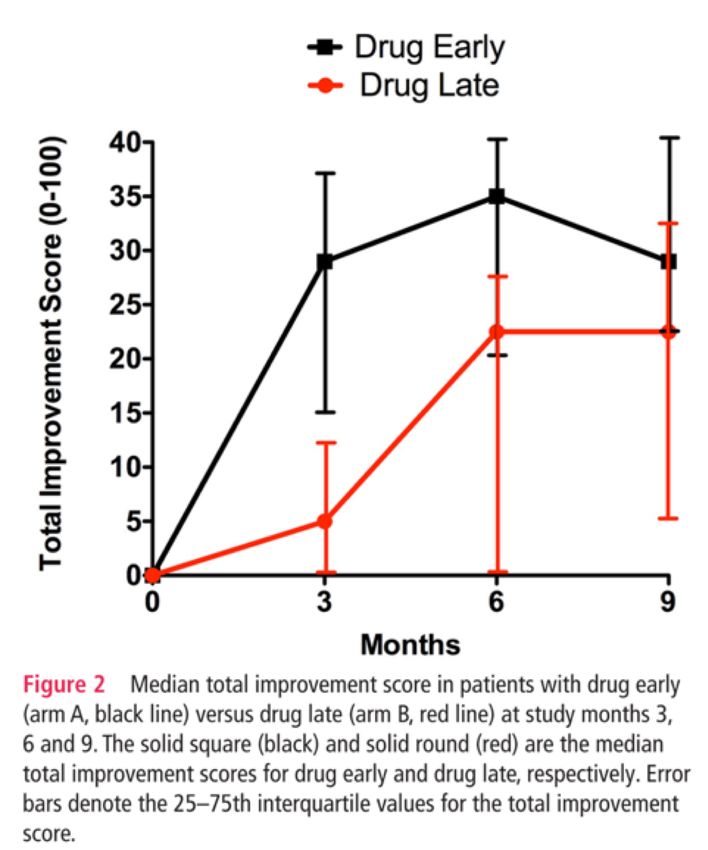
Treatment of IIM is challenging:
diagnosis, assessing disease, treatment success?
Correct diagnosis
• other myopathies may have similar clinical presentation (also PM vs IBM)
• inflammation on biopsy does not exclude other diagnoses
• treatment resistance should prompt reappraisal of diagnosis
Assessing disease
• muscle weakness… is it activity (ongoing immune-mediated process), or damage (fatty replacement/ atrophy)?
• poor prognostic features may direct drug selection/ treatment strategy (lung, cardiac, dysphagia, malignancy)
Treatment success measured as improvement in major manifestations of disease…by
muscle strength & improvement in skin rash or organ involvement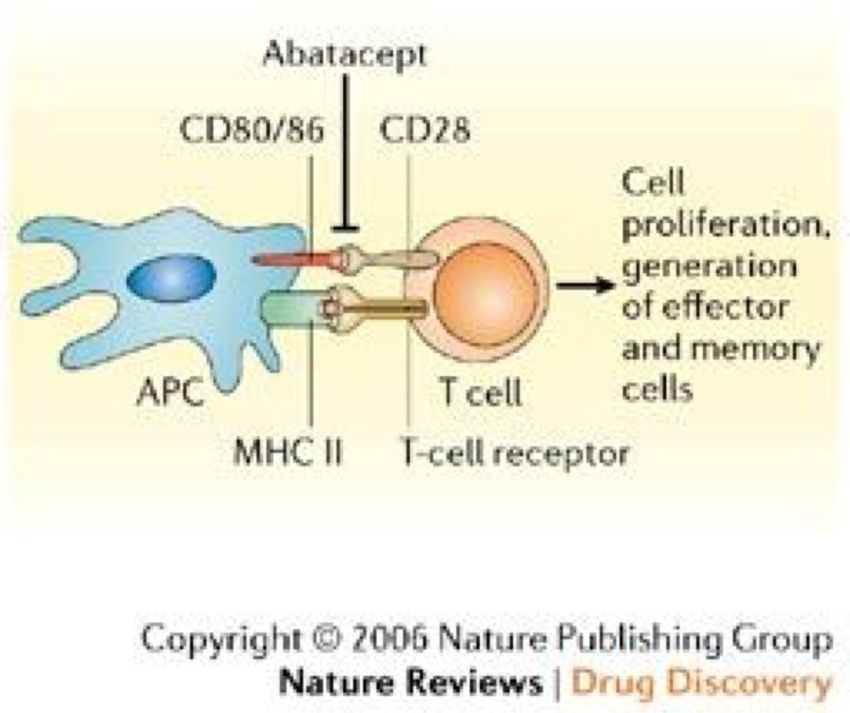
Treatment of IIM is challenging:
diagnosis, assessing disease, treatment success?
Correct diagnosis
• other myopathies may have similar clinical presentation (also PM vs IBM)
• inflammation on biopsy does not exclude other diagnoses
• treatment resistance should prompt reappraisal of diagnosis
Assessing disease
• muscle weakness… is it activity (ongoing immune-mediated process), or damage (fatty replacement/ atrophy)?
• poor prognostic features may direct drug selection/ treatment strategy (lung, cardiac, dysphagia, malignancy)
Treatment success measured as improvement in major manifestations of disease…by
muscle strength & improvement in skin rash or organ involvement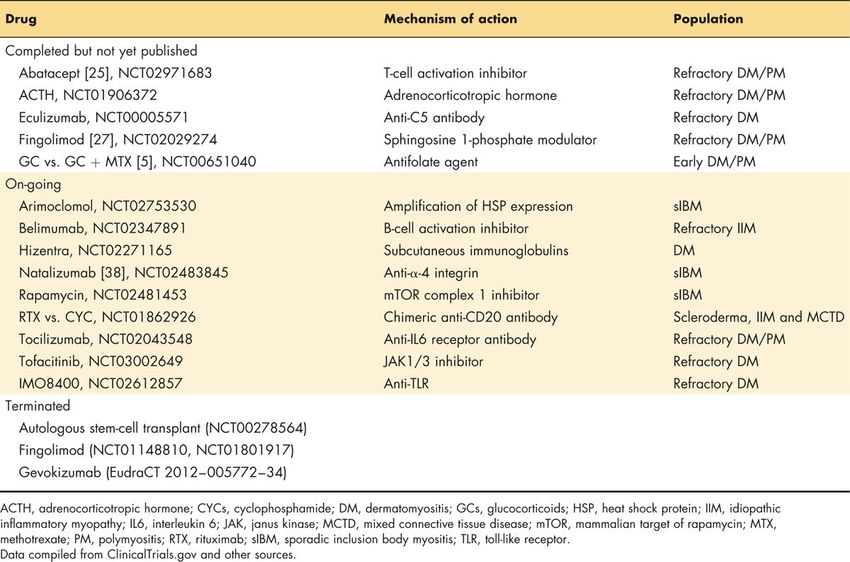
Steroid use still wide since 1950s –retrospective analysis of number and type of
therapies & duration of treatment for 320 patients with JDM enrolled in a North
American registry
Median time to half the initial oral prednisone dose Median time to discontinuation of oral prednisone 41
was shorter in patients diagnosed after 1997 vs months [IQR 24–89], did not differ by diagnosis year
patients diagnosed before 1997
(10 vs. 19 months, PHench PS, Kendall EC, Slocumb CH, Polley HF. Ann Rheum Dis. 1949 Jun;8(2):97-104. PubMed PMID: 18623812
Efficacy and safety of adrenocorticotropic hormone
gel in refractory dermatomyositis (DM) and polymyositis (PM)
• Acthar Gel /repository corticotropin injection (RCI)
– FDA-approved treatment for myositis since 1952, in 2010 FDA retained indication
– long-acting full-sequence ACTH
– includes other pro-opiomelanocortin peptides thought to have anti-inflammatory &
immunomodulatory effects mediated through melanocortin receptors
• Enrolled 10 patients with active & refractory PM/DM
• Study subjects s/c self-administered RCI 80 units (1 mL) twice weekly for 24
weeks
• Primary end point IMACS definition of improvement (DOI): 3 of any of the
6 core set measures improved by ≥20%, with no more than 2 worsening by
≥25% (cannot include MMT)
Aggarwal R, Marder G, Koontz DC, Nandkumar P, Qi Z, Oddis CV.
Efficacy and safety of adrenocorticotropic hormone gel in refractory dermatomyositis and polymyositis.
Ann Rheum Dis. 2018 May;77(5):720-727. PMID: 29237618https://www.niehs.nih.gov/research/resources/imacs/diseaseactivity/
Slide courtesy of Rohit Aggarwal
6 Core Set Measures: Validated and reliable
Domain Core Set Measure Range
Physician Global Activity
Physician global VAS (10 cm scale) 0-10
Patient Global Activity
Patient/Parent global VAS (10 cm scale) 0-10
Muscle Strength Composite score of 8 muscle groups
0-80
( MMT-8 )
Physical Function Health Assessment Questionnaire (HAQ) score
0-3
Laboratory Enzymes Most abnormal enzyme among CK, LDH, AST, ALT, Aldolase Depends on muscle
enzymes
Extramuscular Disease Global extramuscular disease activity VAS (10 cm):
Activity constitutional, cutaneous, articular, GI, pulm, cardiac 0-10
Rider LG, Giannini EH, Harris-Love M, Joe G, Isenberg D, Pilkington C, Lachenbruch PA, Miller FW; International
Myositis Assesment and Clinical Studies Group. Defining Clinical Improvement in Adult and Juvenile Myositis. J
Rheumatol. 2003 Mar;30(3):603-17. PMID: 12610824.Physician global disease activity
Visual Analogue Scale (VAS) 0 – 10 cm
Considering All Aspects of Myositis
Slide courtesy of Rohit AggarwalPatient global disease activity
Visual Analogue Scale (VAS) 0 – 10 cm
Considering all the ways that myositis affects you,
please rate the overall activity of disease today
Slide courtesy of Rohit AggarwalExtra-muscular global disease activity
Visual Analogue Scale (VAS) 0 – 10 cm
uConstitutional
uCutaneous
uPulmonary
uGI
= Extra-Muscular
Disease Activity
uJoints
uCardiac Slide courtesy of Rohit AggarwalHealth Assessment Questionnaire
Without any With some difficulty With much difficulty Unable to do
difficulty
Dressing/Grooming
Arising
Eating
Walking
Hygiene
Reach
Grip
Activities
Slide courtesy of Rohit AggarwalManual Muscle Testing - 8
Total Score = 80 (One side + Axial)
Slide courtesy of Rohit AggarwalKendall Scale
• MRC Scale
– 1976
– Grade 0-5 - blunt
– Informally adapted
with “+” and “-”
designations
• Kendall Scale
– Florence Kendall
– “MRC-plus”
– Grade 0-10Muscle Enzymes • Creatine Kinase (CK) • Aldolase • AST • ALT • LDH
Acthar Gel- results
• 7 / 10 met primary endpoint of efficacy,
median 8 weeks
• Significant decrease in prednisone dose from
baseline → last follow-up
• Muscle strength improved by >10% & physician
global by >40%
• No patient developed significant weight gain
(≥10 kg), cushingoid features, diabetes,
persistent hypertension, hyperglycaemia, or ↑
HbA1c
• RCI was considered safe and tolerable
• 2 – HZV, 1- heart block, 1 – AVN hip
Aggarwal R, Marder G, Koontz DC, Nandkumar P, Qi Z, Oddis CV.
Efficacy and safety of adrenocorticotropic hormone gel in refractory dermatomyositis and polymyositis.
Ann Rheum Dis. 2018 May;77(5):720-727.
doi: 10.1136/annrheumdis-2017-212047. Epub 2017 Dec 13. PubMed PMID: 29237618Step-wise approach to
remission induction & maintenance pharmacotherapy in IIM
Parker MJS, Chinoy H. The treatment approach of idiopathic inflammatory myopathies. EMJ. 2017;2[4]:14-18Poor prognostic features requiring aggressive management
• Severe disease at onset, and/or poor response to initial glucocorticoids
or with delayed initiation of treatment
• Dysphagia, lung, cardiac involvement
• Necrotising myopathy
1. Lilleker JB, Diederichsen ACP, Jacobsen S, Guy M, Roberts ME, Sergeant JC, Cooper RG, Diederichsen LP, Chinoy H.
Using serum troponins to screen for cardiac involvement and assess disease activity in the idiopathic inflammatory myopathies. Rheumatology (Oxford). 2018 Jun 1;57(6):1041-1046. PMID: 29538753
2. Hughes M, Lilleker JB, Herrick AL, Chinoy H.
Cardiac troponin testing in idiopathic inflammatory myopathies and systemic sclerosis-spectrum disorders: biomarkers to distinguish between primary cardiac involvement and low-grade skeletal muscle disease activity.
Ann Rheum Dis. 2015 May;74(5):795-8Myositis Spectrum Disease Antibodies & Clinical Associations in Adult Myositis
Betteridge Z, McHugh N.
Myositis-specific autoantibodies: an important tool to support diagnosis of myositis.
J Intern Med. 2016 Jul;280(1):8-23Myositis Spectrum Disease Antibodies & Clinical Associations in Adult Myositis
POTENTIALLY
POOR
PROGNOSTIC
GROUP
Betteridge Z, McHugh N.
Myositis-specific autoantibodies: an important tool to support diagnosis of myositis.
J Intern Med. 2016 Jul;280(1):8-23Effective induction therapy for childhood anti-SRP associated myositis
Induction
Cyclophosphamide
IVIG
Rituximab
In conjunction with
Intensive physiotherapy
Maintenance
Methotrexate as maintenance
• Anti-SRP myositis distinct from other JIIM
• Important differential to JDM, should
be considered when severe weakness
without rash or CK > 10,000 Binns EL, Moraitis E, Maillard S, Tansley S, McHugh N, Jacques TS,
Wedderburn LR, Pilkington C, Yasin SA, Nistala K;
• Early identification essential to initiate UK Juvenile Dermatomyositis Research Group (UK and Ireland).
aggressive medical & physical therapy Effective induction therapy for anti-SRP associated myositis in childhood:
A small case series and review of the literature.
Pediatr Rheumatol Online J. 2017 Oct 31;15(1):77. PMID: 29089059?Combination therapy with biologics
?When to use biologics
Spencer CH, Rouster-Stevens K, Gewanter H, Syverson G, Modica R, Schmidt K, Emery H, Wallace C, Grevich S, Nanda K,
Zhao YD, Shenoi S, Tarvin S, Hong S, Lindsley C, Weiss JE, Passo M, Ede K, Brown A,
Ardalan K, Bernal W, Stoll ML, Lang B, Carrasco R, Agaiar C, Feller L, Bukulmez H, Vehe R, Kim H, Schmeling H, Gerstbacher D,
Hoeltzel M, Eberhard B, Sundel R, Kim S, Huber AM, Patwardhan A; Pediatric Rheumatologist Collaborators.
Biologic therapies for refractory juvenile dermatomyositis: five years of experience of the Childhood Arthritis and Rheumatology Research Alliance in North America.
Pediatr Rheumatol Online J. 2017 Jun 13;15(1):50. PMID: 28610606Anti-MDA5 (anti-CADM140)
Reported Clinical Associations
ILD (67-100%)
Rapidly Progressing ILD (RP-ILD) (22-100%)
Skin manifestations
DM
Gottron’s Papules
Periungal
Ulceration (skin and mouth)
Hand Swelling
Arthritis
Palmar Papules
Mechanic’s Hands JDM Associations
Panniculitis
Skin and Oral Ulcers
Alopecia
Slide courtesy of Dr Z Betteridge No known association with Periungal, Gottron’s
Papules, Arthritis or Alopecia
Fiorentino et al J Am Acad Dermatol 2011;65:25-34
Sato et al Arthritis Rheum 2005;52:1571-6
Nakashima et al Rheumatol 2010;49:433-40
ILD?
Kobayashi et al J Pediatr 2011;158:675-7So H, Wong VTL, Lao VWN, Pang HT, Yip RML. Rituximab for refractory rapidly progressive interstitial lung disease related to anti-MDA5 antibody-positive amyopathic dermatomyositis. Clin Rheumatol. 2018 Apr 30. doi: 10.1007/s10067-018-4122-2. [Epub ahead of print] PubMed PMID: 29713969.
RECITAL: Cyclophosphamide or rituximab to treat CTD-ILD?
• UK, multicentre, prospective, randomised, double-blind,
double-dummy, controlled trial
• RTX 1 g iv x2 vs monthly iv CYC 600 mg/m2 body surface
area
• ILD due to SSc, IIM (& anti-synthetase syndrome), MCTD
• 116 individuals randomised 1:1, stratification based on
underlying CTD, followed for 48 weeks from first dose
• Primary endpoint: change in forced vital capacity (FVC) at
24 weeks
• Key secondary endpoints: safety, change in FVC at 48
weeks, survival, change in oxygen requirements, total 48-
week corticosteroid exposure, utilisation of health care
resources
Saunders P, Tsipouri V, Keir GJ, Ashby D, Flather MD, Parfrey H, Babalis D, Renzoni EA, Denton CP, Wells AU, Maher TM.
Rituximab versus cyclophosphamide for the treatment of connective tissue disease-associated interstitial lung disease (RECITAL):
study protocol for a randomised controlled trial. Trials. 2017 Jun 15;18(1):275. PMID: 28619061Exercise improves muscle function, aerobic conditioning and
quality of life in IIM patients
• Safe & therapeutic benefits of exercise (active
and/or recent onset disease)
• Several exercise programs based on resistance
training, aerobic exercise or combination, up to 12
weeks duration
• No evidence that exercise has deleterious effects
on disease activity
• Supervised resistance training in combination with
aerobic exercise starting 4 weeks after initiation of
pharmacotherapy, or as soon as patients are able
to perform exercise
Alexanderson H.
Physical exercise as a treatment for adult and juvenile myositis.
J Intern Med 2016;280:75-96.Effect of endurance exercise on microRNAs in myositis
skeletal muscle - a randomized controlled study
• PM/DM, exercising 1 month
• Randomized into two groups at Karolinska University Hospital
• 12-week endurance exercise group (n = 12) or a non-exercised control
group (n = 11)
• Affymetrix microarray, microRNA expression determined in paired
muscle biopsies before/after exercise intervention from 3 patients in
each group
Boehler JF, Hogarth MW, Barberio MD, Novak JS, Ghimbovschi S, Brown KJ,
Alemo Munters L, Loell I, Chen YW, Gordish-Dressman H, Alexanderson H, Lundberg IE, Nagaraju K.
Effect of endurance exercise on microRNAs in myositis skeletal muscle-A randomized controlled study.
PLoS One. 2017 Aug 22;12(8):e0183292. PubMed PMID: 28829792microRNAs may improve disease by decreasing immune
responses and increasing mitochondrial biogenesis
• Endurance exercise altered 39 microRNAs
• Target transcripts had ↓ mRNA expression in
exercised patients
• ↓ in NF-κB regulator IKBKB associated with
an ↑ in target microRNA (miR-196b)
• At protein level, increase in mitochondrial
proteins (AK3, HIBADH) associated with ↓
microRNAs predicted to regulate their
expression
Improvement in disease phenotype after exercise,
associated with ↑ microRNAs that target &
downregulate immune processes at transcript
level, as well as ↓ microRNAs that target /
Boehler JF, Hogarth MW, Barberio MD, Novak JS, Ghimbovschi S, Brown KJ,
upregulate mitochondrial content at protein level.
Alemo Munters L, Loell I, Chen YW, Gordish-Dressman H, Alexanderson H, Lundberg IE, Nagaraju K.
Effect of endurance exercise on microRNAs in myositis skeletal muscle-A randomized controlled study.
PLoS One. 2017 Aug 22;12(8):e0183292. PubMed PMID: 28829792Blood-flow restricted resistance training in patients with sporadic
inclusion body myositis: a randomized controlled trial
Involves cuff application to restrict blood supply to exercising muscles
to generate an ischaemic environment within muscles - combined with
metabolic stress generated when exercising, favours anabolic response
in exercised myofibres
Pearson SJ, Hussain SR. A review on the mechanisms of blood-flow restriction resistance training-induced muscle hypertrophy.
Sports Med. 2015 Feb;45(2):187-200. doi: 10.1007/s40279-014-0264-9. Review. PubMed PMID: 25249278.
Jørgensen AN, Aagaard P, Frandsen U, Boyle E, Diederichsen LP. Blood-flow restricted resistance training in patients with
sporadic inclusion body myositis: a randomized controlled trial. Scand J Rheumatol. 2018 May 18:1-10. doi:
10.1080/03009742.2017.1423109Blood-flow restricted resistance training in patients with sporadic
inclusion body myositis: a randomized controlled trial
Involves cuff application to restrict blood supply to exercising muscles
to generate an ischaemic environment within muscles - combined with
metabolic stress generated when exercising, favours anabolic response
in exercised myofibres
• Primary outcome was the physical function domain of the 36-item
Short Form Health Survey – not met
• In per-protocol analysis, between-group difference in baseline to
follow-up change in knee extensor muscle strength 15.0%
(blood-flow resistance: +5.8%, p = 0.304; control: −9.2%, p = 0.024)
Pearson SJ, Hussain SR. A review on the mechanisms of blood-flow restriction resistance training-induced muscle hypertrophy.
Sports Med. 2015 Feb;45(2):187-200. doi: 10.1007/s40279-014-0264-9. Review. PubMed PMID: 25249278.
Jørgensen AN, Aagaard P, Frandsen U, Boyle E, Diederichsen LP. Blood-flow restricted resistance training in patients with
sporadic inclusion body myositis: a randomized controlled trial. Scand J Rheumatol. 2018 May 18:1-10. doi:
10.1080/03009742.2017.1423109Myostatin pathway – Bimagrumab, an activin receptor-IIb
inhibitor
http://mmcneuro.wordpress.com/2013/08/23/bym338-bimagrumab-for-inclusion-body-myositis-new-cure-or-next-dud/Google image search: Myostatin animals Shuelke et al. N Engl J Med 2004;350:2682-8.
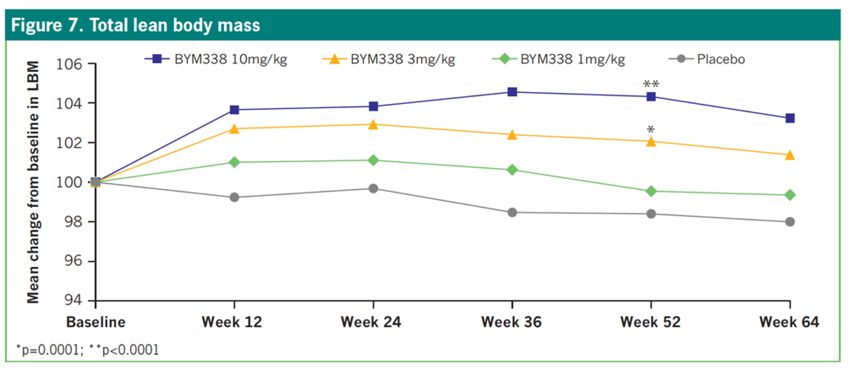
RESILIENT: A randomized, double-blind, placebo-controlled, phase IIb/III
study to evaluate efficacy, safety and tolerability of intravenous BYM338
at 52 weeks on physical function, muscle strength, and mobility in
patients with sporadic inclusion body myositis
Amato et al. A Randomized, Double-Blind, Placebo-Controlled Study
of Bimagrumab in Patients with Sporadic Inclusion Body Myositis.
ACR 2016 Washington DC Abstract 8L
44RESILIENT: A randomized, double-blind, placebo-controlled, phase IIb/III
study to evaluate efficacy, safety and tolerability of intravenous BYM338
at 52 weeks on physical function, muscle strength, and mobility in
patients with sporadic inclusion body myositis
Study did not
achieve primary endpoint
Amato et al. A Randomized, Double-Blind, Placebo-Controlled Study
of Bimagrumab in Patients with Sporadic Inclusion Body Myositis.
ACR 2016 Washington DC Abstract 8L
45At Week 52, bimagrumab 3 and 10 mg/kg treatments resulted in
statistically significant changes in lean body mass compared with placebo
Amato et al. A Randomized, Double-Blind, Placebo-Controlled Study
of Bimagrumab in Patients with Sporadic Inclusion Body Myositis.
ACR 2016 Washington DC Abstract 8LFollistatin Gene Therapy for Sporadic Inclusion Body Myositis
Improves Functional Outcomes
rAAV1.CMV.huFS344, 6x 1011 vg/kg
delivered to R/L quads of 6 sIBM subjects.
Primary outcome : distance travelled
for the 6-min walk test
Mechanisms:
- binds to activins inhibiting pro-inflammatory cytokines
- downregulation of fibrosis markers
- ability to stimulate myoblasts to express myogenic
transcription factors that promote muscle regeneration Mendell JR, Sahenk Z, Al-Zaidy S, Rodino-Klapac LR, Lowes LP, Alfano LN, et al. Follistatin Gene Therapy for
Sporadic Inclusion Body Myositis Improves Functional Outcomes. Mol Ther. 2017 Apr 5;25(4):870-879. PMID: 28279643Lack of evidence on orthotic devices for the management of
knee instability related to inflammatory myopathy
Design
Systematic review of primary studies
Setting
Community
Participants
Adults with neuromuscular disorder/
CNS disorder & impaired walking
ability due to instability of knee
Interventions
Orthoses with aim of controlling
knee instability, eg
knee-ankle-foot orthoses,
ankle-foot orthoses, knee orthoses
McDaid C, Fayter D, Booth A, O'Connor J, Rodriguez-Lopez R, McCaughan D, Bowers R, Iglesias CP, Lalor S, O'Connor RJ, Phillips M, Ramdharry G.
Systematic review of the evidence on orthotic devices for the management of knee instability related to neuromuscular and central nervous system disorders.
BMJ Open. 2017 Sep 5;7(9):e015927. PMID: 28877943
Bernhardt K, Oh T, Kaufman K. Stance control orthosis trial in patients with inclusion body myositis. Prosthet Orthot Int. 2011 Mar;35(1):39-44. PMID: 21515888Other non-pharmacotherapeutic measures
• Physical therapy & rehabilitation to begin early in treatment course
• Pulmonology collaboration in patients with associated lung disease
• Speech therapy & aspiration precautions for patients with pharyngeal
and oesophageal involvement
• Osteoporosis prevention and treatment
• Appropriate immunizations prior to initiation of immunosuppressive
therapy and pneumocystic prophylaxis in patients receiving high dose
glucocorticoids & other immunosuppressants
• Counselling, psychological and social work support.
Mann & Vencovsky. Treatment of Idiopathic Inflammatory Myopathies (Chapter) in
Chinoy H. & Cooper R.G. (ed). Myositis - Oxford Rheumatology Library. (Oxford University Press) 2017Innate immune mechanisms of muscle damage in myositis
Rayavarapu S, Coley W, Kinder TB, Nagaraju K.
Skelet Muscle. 2013 Jun 7;3(1):13. doi: 10.1186/2044-5040-3-13.Rapamycin (Sirolimus)
• Rapamycin is a mTOR inhibitor used in organ transplantation
• Potentially, rapamycin can deplete T effector cells, preserve T
regulatory cells and induce protein degradation - all parameters
impaired during IBMRAPAMI: Rapamycin Vs. Placebo for the Treatment of Inclusion Body Myositis:
Improvement of the 6 Min Walking Distance, a Functional Scale, the FVC and Muscle
Quantitative MRI
• Prospective, randomized, controlled, double blind, monocentric, phase
IIb trial evaluating efficacy of rapamycin against placebo
(NCT02481453)
• Primary endpoint: stabilization of maximal voluntary quadriceps
isometric strength assessed by dynamometry
• 44 patients treated with oral rapamycin (2 mg/d, n=22) or placebo
(n=22) for 12 months
1. Benveniste O, Hogrel JY, Annoussamy M, Bachasson D, Rigolet A, Servais L, Salem JE, Hervier B,
Landon Cardinal O, Mariampillai K, Hulot JS, Carlier P, Allenbach Y. Arthritis Rheumatol. 2017; 69 (suppl 10)
2. Lilleker JB, Bukhari M, Chinoy H. Rapamycin for inclusion body myositis: targeting non-inflammatory mechanisms.
Rheumatology (Oxford). 2018 Feb 26. doi: 10.1093/rheumatology/key043Rapamycin vs. Placebo for the Treatment of Inclusion Body Myositis: Improvement of
the 6 Min Walking Distance, a Functional Scale, the FVC and Muscle Quantitative MRI
-
Benveniste O, Hogrel JY, Annoussamy M, Bachasson D, Rigolet A, Servais L, Salem JE,
Hervier B, Landon Cardinal O, Mariampillai K, Hulot JS, Carlier P, Allenbach Y.
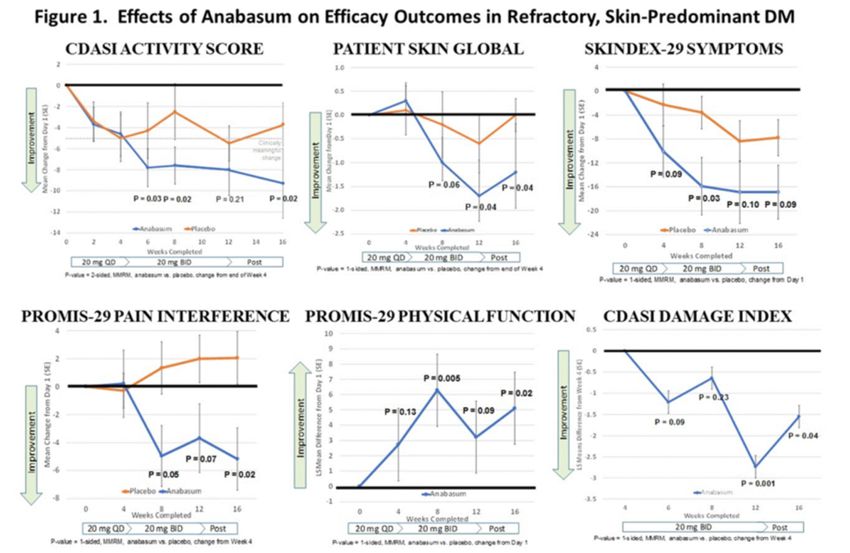
Arthritis Rheumatol. 2017; 69 (suppl 10).A Phase 2 Study of Safety and Efficacy of Anabasum (JBT-101), a Cannabinoid
Receptor Type 2 Agonist, in Refractory Skin-Predominant Dermatomyositis (DM)
• Anabasum
• non-immunosuppressive, synthetic, oral preferential CB2 agonist
• triggers resolution of innate immune responses
• reduces cytokine production by PBMC from DM patients.
• To test safety / efficacy of anabasum in DM subjects with refractory, moderate-to-
severely active skin disease
• Double-blind, randomized placebo-controlled 16-week study
• Enrolled adults with documented DM and Cutaneous Dermatomyositis Disease
Area and Severity Index (CDASI) activity score ≥ 14, minimal active muscle
involvement, failure/intolerance to HCQ & immunosuppressants
Werth VP, Hejazi E, Pena SM, Haber JS, Okawa J, Feng R, Gabre K, Concha J, Cornwall C, Dgetluck N, Constantine S, White B.
Arthritis Rheumatol. 2017; 69 (suppl 10)Cutaneous dermatomyositis
disease area and severity index
(CDASIv2)
Useful to use as outcome measure
in patients with predominant
skin involvement
1: Yassaee M, Fiorentino D, Okawa J, Taylor L, Coley C, Troxel AB, Werth VP.
Modification of the cutaneous dermatomyositis disease area and severity index,
an outcome instrument.
Br J Dermatol. 2010 Mar;162(3):669-73. PubMed PMID: 19863510
2: Anyanwu CO, Fiorentino DF, Chung L, Dzuong C, Wang Y, Okawa J, Carr K, Propert KJ, Werth VP.
Validation of the Cutaneous Dermatomyositis Disease Area and Severity Index: characterizing
disease severity and assessing responsiveness to clinical change.
Br J Dermatol. 2015 Oct;173(4):969-74. PubMed PMID: 25994337;Anabasum and dermatomyositis
Immune-related potential
therapeutic targets in myositis
Oddis, C. V. & Aggarwal, R. (2018) Treatment in myositis
Nat. Rev. Rheumatol. doi:10.1038/nrrheum.2018.42Functional role for co-receptor blockade in muscle inflammation?
§ CTLA-4, CD28, CD86 and CD40
demonstrated on inflammatory cells
infiltrating muscle tissue in patients with
DM & PM
§ Expression of BB-1 (counter-receptor
for CTLA-4 & CD28)
§ on MHC-1-expressing muscle fibres from
PM muscle tissue
§ BB-1+ fibres bind strongly to CLTA-4 and
CD28 on invasive CD8+ T cells
Nagaraju K, Raben N, Villalba ML, et al. Costimulatory markers in muscle of patients
with idiopathic inflammatory myopathies and in cultured muscle cells. Clin Immunol1999;92:161–9.
Murata K, Dalakas MC. Expression of the costimulatory molecule BB-1, the ligands
CTLA-4 and CD28, and their mRNA in inflammatory myopathies. Am J Pathol 1999;155:453-60Co-receptor blockade: Abatacept in the treatment of adult
dermatomyositis and polymyositis:
a randomised, phase IIb treatment delayed-start trial
§ 20 with DM (n=9) or PM (n=11) with refractory disease enrolled to receive
either immediate active treatment with intravenous abatacept or 3 month
delayed-start
§ Primary endpoint was number of responders, defined by the International
Myositis Assessment and Clinical Studies Group definition of improvement
(DOI), after 6 months of treatment.
§ Secondary endpoints included number of responders in early treatment arm
compared with delayed treatment arm at 3 months
§ Repeated muscle biopsies investigated for cellular markers and cytokines
Tjärnlund A et al. Abatacept in the treatment of adult dermatomyositis and polymyositis:
a randomised, phase IIb treatment delayed-start trial.
Ann Rheum Dis. 2017 Oct 9. pii: annrheumdis-2017-211751Trial design
Tjärnlund A et al. Abatacept in the treatment of adult dermatomyositis and polymyositis:
a randomised, phase IIb treatment delayed-start trial.
Ann Rheum Dis. 2017 Oct 9. pii: annrheumdis-2017-211751• 8/19 patients included in analyses achieved
DOI at 6 months
• 3 months: 5 (50%) patients responders
after active treatment, 1 (11%) patient in
delayed treatment arm
• 8 adverse events (AEs) regarded as drug-
related: 4 mild; 4 moderate; 4 serious AEs -
none drug-related
• Significant increase in regulatory Foxp3+ T
cells (Tregs), other markers unchanged in
repeated muscle biopsies
Tjärnlund A et al. Abatacept in the treatment of adult dermatomyositis and polymyositis:
a randomised, phase IIb treatment delayed-start trial.
Ann Rheum Dis. 2017 Oct 9. [Epub ahead of print] PubMed PMID: 28993346.Completed, on-going or terminated clinical trials in inflammatory myopathy
Leclair V, Lundberg IE.
Recent clinical trials in idiopathic inflammatory
myopathies.
Curr Opin Rheumatol. 2017 Nov;29(6):652-659.
doi: 10.1097/BOR.0000000000000430.
PMID: 28763333Conclusions • Tailor treatment according to clinical phenotype / serotype /severity • Importance of exercise intervention • Future targets involving the innate immune system • Possible licensed drugs on the horizon • New exciting times in myositis!
You can also read

















































