FRONTLINE AIDS HARM REDUCTION EVALUATION TERMS OF REFERENCE - People
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
FRONTLINE AIDS
HARM REDUCTION
EVALUATION
TERMS OF REFERENCE
1. BACKGROUND
Frontline AIDS is a global network of civil society organisations who have been on the frontline of the world’s
response to AIDS for 25 years, igniting innovations that break through social, political and legal barriers that
stand in the way of a future free from AIDS.
We are on the frontline of harm reduction, ensuring people who use drugs (PWUD) in their diversity can
access the services they need to protect themselves from the risk of contracting HIV and other blood-borne
diseases, as well as the harm associated with drug use. We support community-based organisations with
funding and technical expertise to develop community driven harm reduction services and advocacies.
We advocate for changes to laws, policies and practices to support HIV prevention, treatment and care for
people who use drugs. We also support debates on effective approaches to respond to drug use. We
advocate to national governments and international society to move away from punishing people who use
drugs, encouraging more supportive and humane approaches to deal with drug use and its related social
problems. In addition, we work with community-based organisations, including those led by people who use
drugs to design quality harm reduction and advocacy programmes that meet their specific needs.
Throughout all our programming we intend to achieve gender equality, ensuring our work serves both men
and women who use drugs. This means addressing the extra barriers faced by women who use drugs, at
institutional, societal, cultural, political and personal levels.
1.1 Frontline AIDS Harm Reduction Programming
In 2018, Frontline AIDS developed a Harm Reduction Theory of Change (ToC) to capture the key outcomes
envisioned to end AIDS among people who use drugs, implemented through two programmes, the Integrated
Harm Reduction Program (IHRP) and the Partnership to Inspire, Transform and Connect the HIV response
(PITCH)1. In the past four years the majority of the Frontline AIDS harm reduction work has been
implemented under these two programs. The ToC deploys four strategies to the achieve short-, medium-
and long-term outcomes:
• Strategy 1: Initiate, deliver and expand high-quality HIV and health programmes to people who use drugs;
• Strategy 2: Advocate for an improved policy environment for harm reduction and people who use drugs;
• Strategy 3: Build capacity for harm reduction that involves people who use drugs;
• Strategy 4: Promote and scale-up community-led harm reduction good practices.
1Since early 2019 Frontline AIDS manages the Global Fund regional grant for the Middle East and North Africa region, which
focusses on advocacy for harm reduction and public health- & human rights-based drug policies. This program will not be part of
the evaluation.
Terms of Reference Frontline AIDS Harm Reduction Evaluation 2020 1The Integrated Harm Reduction programme (IHRP) is a 3-year (2018-2020) programme, financed through
core funding from the Dutch Ministry of Foreign Affairs, and focuses on the promotion and scale-up of
community-led harm reduction good practices in six countries (China, India, Indonesia, Myanmar, Nigeria2
and Senegal).
The aim of the IHRP is to demonstrate the effectiveness of person-centred harm reduction services, and to
target national governments and relevant donors to adopt, expand and sustain the harm reduction models,
delivering them at a scale sufficient to tackle the HIV epidemic. The IHRP programme focuses on delivering
the fourth strategy of the Frontline AIDS Harm Reduction ToC: the promotion and scale-up of community-
led harm reduction good practices. It has employed the following activities:
• Develop strong programme models to improve access to and retention in needle and syringe programmes
(NSP), opioid substitution treatment (OST) and HIV-, Hepatitis C- and TB-treatment;
• Document and communicate examples of good practice and innovation;
• Support community action to monitor and improve the quality of services for people who use drugs and
their partners and families;
• Build advocacy messages to influence national policies and practices on our piloted and tested models to be
scaled up.
The Partnership to Inspire Transform and Connect the HIV response (PITCH) is a 5-year (2016-2020) multi-
country programme, led by the Dutch Aidsfonds and Frontline AIDS and funded by the Dutch Ministry of
Foreign Affairs. PITCH enables men who have sex with men, sex workers, transgender people, people who
use drugs and adolescent girls and young women to realise their human rights and improve access to HIV
and sexual and reproductive health services. This programme, focussing on advocacy rather than service
provision, is implemented by partners in Indonesia, Kenya, Mozambique, Myanmar, Nigeria, Uganda,
Ukraine, Vietnam and Zimbabwe and has two regional components (Southern Africa and Eastern Europe &
Central Asia). The programme focuses on delivering the second and third strategies of the Frontline AIDS
Harm Reduction Theory of Change3.
Within PITCH, Frontline AIDS coordinates the harm reduction and drug policy advocacy across the nine
countries, two regions and at global fora, with the following objectives:
• Influence the global agenda for harm reduction and drug policy reform at international advocacy spaces;
• Advocate for decriminalisation of drug use and establishment of harm reduction programmes that include
the WHO recommended interventions;
• Build the capacity of networks of people who use drugs in order to generate evidence, set advocacy
agendas and establish south-to-south collaboration channels.
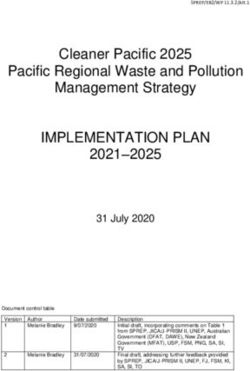
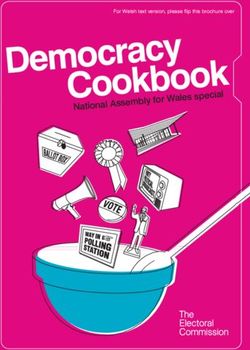
Fig. 1 Countries where PITCH (pink) and IHRP (green) are implemented, with the overlap in the middle
2 In year 1 the IHRP did not implement in Nigeria, but in Kenya. In year 2 the programme in Nigeria started, while the one in Kenya
stopped.
3 Note that the ToC was developed when PITCH was already halfway.
Terms of Reference Frontline AIDS Harm Reduction Evaluation 2020 21.2 Theoretical Pathway of Change
Alongside the HR ToC, Frontline AIDS has designed a theoretical pathway of change that countries are most
likely to go through to end HIV among people who use drugs. While the initial pathway was slightly more
complex (having more stages), the current one dates from late 2019. It is mostly used at Frontline Global4 to
understand and reflect on differences between countries, and to identify needs and ways forward along the
continuum, while Frontline AIDS implementing partners defined their activities based on in-country needs and
the objectives of the two programmes.
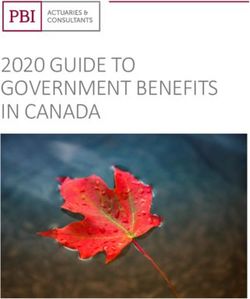
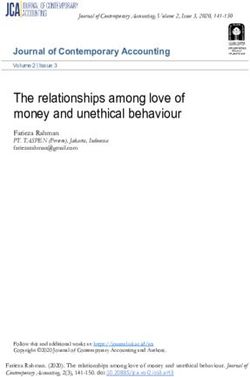
Fig. 2 Theoretical Pathway of Change to end AIDS among people who use drugs
In the theoretical pathway of change countries are divided into three categories:
• Kick-starters: Countries where there is a significant and / or growing need for harm reduction services, but
where current service provision is almost non-existent and where no harm reduction policies exist. Here we
seek to identify new partners, identify or support the establishment of organisations of people who use
drugs and begin small-scale service delivery (as pilots). Countries in this category include Mozambique,
Nigeria, Senegal, Uganda and Zimbabwe.
• Accelerators: Countries where governments have started delivering harm reduction services and are
exploring ways to scale up service coverage. The aim of our investment is mainly to encourage the
governments to expand community-based, peer-led service provision models to new areas and hand over
interventions to the national programme supported by donors and national governments. Countries in this
category include Kenya, Myanmar and Indonesia.
• Multipliers: Countries with an established apparatus of harm reduction programmes at a national level
mainly funded by the government. The aim of our investment is to ensure that the government programmes
reach hard-to-reach people, focus on strengthening the quality and inclusivity of people who use drugs in
decision making and broadening the scope to the regional level. Countries in this category include China,
India, Ukraine and Vietnam.
2. PURPOSE AND OBJECTIVES OF THE EVALUATION
With both programmes contributing to the Frontline AIDS harm reduction work ending in 2020 and the
development of a new harm reduction strategy for the period 2021-2025, we would like to invite consultants
or consulting groups to conduct an evaluation of the overall harm reduction work of Frontline AIDS.
4 Whereas “Frontline AIDS” refers to the whole partnership, “Frontline Global” includes only the offices in Brighton and Cape Town.
Terms of Reference Frontline AIDS Harm Reduction Evaluation 2020 32.1 Evaluation Context Since the start of the IHRP (2018) & PITCH (2016), there have been major internal and external changes in the context of our harm reduction programming. Internally, Frontline AIDS (formerly the International HIV/AIDS Alliance) developed a new brand, a Global Theory of Change and a Global Plan of Action (2020-2025) together with a new partnership model. In the future, the harm reduction programming will be implemented through this new Global Plan of Action and is reflected in the Frontline AIDS Global Theory of Change. A new harm reduction strategy articulating the harm reduction work across the partnership for the coming five years is currently in development. Externally, there has been increased debate on decriminalisation of drug use and possession of drugs for personal use, while decriminalisation and legalisation of (medical) cannabis actually started in various countries and states. At the same time however, we have witnessed an increased focus on the war on drugs in other countries (Philippines, Brazil). Other important developments influencing our work have been the global COVID- 19 pandemic and the 2019 Global Fund replenishment. What we have not seen, unfortunately, is a significant progress towards eliminating AIDS among PWUD; funding for harm reduction has stalled and existing harm reduction programs have not been scaled-up or expanded. 2.2 Evaluation Purpose In this context, Frontline AIDS realises that the way forward cannot be business as usual. Through this evaluation, it is important for us to clearly assess what has worked and what has not; what we need to do better and what we should not invest in during the coming years, as we develop the new strategy for harm reduction. This includes not only what we have planned and achieved in terms of activities (implementation, capacity building, advocacy), but also where we have done it (which countries / regions) and how we have done it (partner choice, coordination, communication with partners, governments and other stakeholders, embeddedness in other programmes). 2.3 Use of evaluation findings Various teams at Frontline AIDS5 will use the lessons and recommendations presented in the evaluation report to do the following: • Shape Frontline AIDS future harm reduction programming; • Inform our strategic donor (NL MoFA) of the achievements of our harm reduction work so far; • Promote our work and the work of our partners to current and prospective donors to open up new streams of funding for harm reduction; • Promote the harm reduction concept to governments, international organisations and policy makers as an alternative to current repressive approaches towards people who use drugs. 2.4 Evaluation Objectives The evaluation therefore has two main objectives: 1. To assess the two harm reduction programmes PITCH & IHRP against the short- and medium-term outcomes of the HR ToC, and the contributions of Frontline Global to this; 2. To draw lessons on what has worked well and what can be improved, which will guide us shaping the Frontline AIDS harm reduction strategy for the coming five years. 5Harm reduction programming, communications, influencing, institutional fundraising and philanthropy teams are expected to draw from the findings of the evaluation. Terms of Reference Frontline AIDS Harm Reduction Evaluation 2020 4
3. SCOPE OF THE EVALUATION
3.1 Geographical scope
The evaluation is expected to cover all global, regional and country outcomes achieved under the harm
reduction approach as articulated in the ToC. The PITCH programme was implemented in two regions and
nine countries while the IHRP was implemented in six countries. The three countries covered by both
programs (Indonesia, Myanmar, Nigeria) are expected to provide the most complete data.
3.2 Programme scope
The evaluation will assess the effectiveness, impact, relevance, coherence and sustainability of the Frontline
AIDS harm reduction work under two programmes: IHRP (implemented from January 2018 till December
2020) and the work related to people who use drugs under PITCH (implemented from January 2016 till
December 2020).
It should be noted that the PITCH programme covers four key and vulnerable populations (sex workers,
adolescent girls & young women, LGBT and people who use drugs). The requested evaluation will focus only
on the work implemented and achievements gained related to people who use drugs. An end term evaluation
(ETE) focusing on the whole PITCH programme is currently underway (see Annex 1) and due to be completed
in October 2020. The evaluation is using an outcome harvesting methodology, with limited focus on
additional OCED-DAC criteria such as coherence for example. To make optimal use of both evaluations and
avoid duplication, the precise scope of the PITCH related work will be further discussed during the inception
phase of the evaluation process.
4. EVALUATION APPROACH
The consultants should consider the following in their proposed evaluation approach:
• The meaningful involvement of people who use drugs in the design, implementation and validation of the
evaluation.
• The contribution of Frontline Global and the Frontline AIDS partnership to the achievement of outcomes
and effectiveness of strategies employed by Frontline.
• Gender equality as an important cross-cutting issue in harm reduction work.
In addition, the indicators and themes emerging in the evaluation should be evaluated according to three
criteria:
• Evidence-based: availability of evidence6 to substantiate claims by evaluation respondents;
• Systematisation: to what extent is the organisation systematic in addressing each theme, is it
institutionalised?
• Outcome-focused: Are processes related to the achievement of each theme designed in a way that leads
to the realisation of outcomes?
6Drawing on the BOND principles for assessing the quality of evidence (October 2013), good quality evidence for Frontline AIDS
means:
• Voice and Inclusion: the perspectives of people living in poverty, including the most marginalised, are included in the evidence,
and a clear picture is provided of who is affected and how.
• Appropriateness: the evidence is generated through methods that are justifiable given the nature of the purpose of the
enquiry.
• Triangulation: the evidence has been generated using a mix of methods, data sources, and perspectives
• Contribution: the evidence explores how change happens, the contribution of the intervention and factors outside the
intervention in explaining change.
• Transparency: the evidence discloses the details of the data sources and methods used, the results achieved, and any
limitations in the data or conclusions.
Terms of Reference Frontline AIDS Harm Reduction Evaluation 2020 55. EVALUATION QUESTIONS The following evaluation questions are proposed based on the OECD-DAC criteria. The specific evaluation questions will be finalised in the inception phase with the selected consultant. 5.1 Effectiveness To what extent has the work under the IHRP and PITCH been successful in promoting high-quality, sustainable, community-based and peer-led harm reduction services to governments and donors, and in securing an enabling environment in which people who use drugs can access those services? Possible topics for assessment: • How is the quality of the interventions implemented under the IHRP (responding to needs of people who use drugs and adapted to the local contexts)? • Which strategies have been useful to convince donors to support the interventions piloted under the programmes? • Which strategies have been useful to promote the WHO-recommended harm reduction model in international fora (such as HIV, law enforcement and drug policy spaces) and at national level in the countries of implementation? • Which strategies have been successful in increasing support for public health- and human rights-based drug policies7 in the countries of implementation and in international fora? • In which ways have people who use drugs strengthened their organisation and collaboration nationally and internationally under influence of the two programmes? 5.2 Impact To what extent have the two programmes generated significant effects on the harm reduction and drug policy landscape in the countries where they were implemented and at global and regional fora that the two programmes have directly engaged with8? Consider positive, negative, intended and unintended effects. Possible topics for assessment: • To what extent have the programmes contributed to an enabling environment for harm reduction in the targeted countries? • To what extent has the work contributed to communities of people who use drugs taking the lead in harm reduction interventions, including in the design and implementation of programming models? • To what extent have the programmes helped partners attract other donors for harm reduction interventions? • To what extent have the programmes contributed to improved health and enjoyment of full rights of people who use drugs in the targeted countries? 7 This includes all policies related to drug use and people who use drugs, such as (de-)criminalisation of drug use and drug possession for personal use & penalties/sentences for this; policies facilitating/impede forced drug treatment; facilitate/impede harm reduction interventions (especially NSP & OST). 8 Such as the UNGASS on Drugs, CND, HLM on Drugs. In other spaces, such as HLM on HIV, HLPFs and the HLM on UHC we have advocated more broadly for issues related to all KPs. Terms of Reference Frontline AIDS Harm Reduction Evaluation 2020 6
5.3 Relevance and Coherence Internal coherence: To what extent have the two programmes strengthened each other and to what extent have they been embedded in or linked to other programmes at Frontline Global and at partner organisations? External coherence: To what extent have the programmes managed to coordinate efforts with other actors working in the HIV & AIDS context in each of the targeted countries and internationally? Possible topic for assessment: • What lessons can we learn from working with partners in loose affiliation (without defined hierarchical structure or collaboration agreement)? • What has been the added value /contribution of Frontline Global in the achievement of outcomes under both programmes? • What can we learn from the management structures used in both programmes? • What are the gaps in the programmes and current needs according to partners involved in the programmes? • Do the definitions of pathways and the change markers help us understand the changes we have seen in the lifetime of the programmes? 5.4 Sustainability To what extent are the positive effects generated by the programmes likely to last without continued funding after 2020? Possible topics for assessment: • To what extent are positive changes in policy environments for harm reduction and people who use drugs expected to last after the end of the programmes in the targeted countries and in the global fora? • To what extent will community-based harm reduction interventions that were supported in the programmes be able to continue after the end of 2020? • For interventions that appear not to be sustainable, to what extent have they positively or negatively impacted the communities of people who use drugs? 6. PROPOSED METHODOLOGY The methodology will be finalised in consultation with Frontline Global staff during the inception phase. As the PITCH programme is being evaluated currently, the evaluation of Frontline AIDS harm reduction work should draw upon information and analysis from the PITCH ETE and collaborate with the consultants carrying out this ETE as much as possible. Due to the global COVID-19 pandemic it is highly unlikely that project visits will be possible. However, we encourage applications that meaningfully involve communities of people who use drugs in the research process. Therefore, consultant(s) should propose suggestions for including communities, implementing partners and beneficiaries in the design and implementation of the study as feasible. It is expected that the consultant(s) employ(s) systematic research methods in answering the evaluation questions. The methods are likely to include (but not limited to): • Desk review of documentation and analysis of data available: a systematic review of all secondary data currently available for the programmes. This includes donor reports, monitoring data and other research products generated by the two programmes, including access to the emerging findings of the PITCH outcome harvest evaluation. Details of available documentation is provided in Annex 2. The desk review should include an analysis of the outcomes achieved and the contribution of Frontline AIDS to these across the nine PITCH and five IHRP programme countries. Terms of Reference Frontline AIDS Harm Reduction Evaluation 2020 7
• In-depth interviews and focus group discussions (FGDs) with key informants. This can be in person or via
skype/phone as is practical:
o Frontline Global staff involved in the IHRP and PITCH;
o Management and staff of partner organisations;
o People who use drugs reached by or involved in the programmes;
o Government representatives reached by or involved in the programmes;
o Global partners involved in the programmes;
o Lead and in-country consultants of the PITCH ETE.
7. EXPECTED DELIVERABLES
• A final inception report: Including the research methods and protocols to collect primary data and analysis
of secondary data to answer the evaluation questions; the data collection tools, sampling and proposed
analysis.
• A draft product containing:
o The results of the evaluation, including lessons learned;
o A minimum of three case studies with a focus on what has worked well and what has not, including
synergies between the two programmes if in countries where they were both implemented;
o Recommendations for future harm reduction work.
• After feedback from relevant Frontline Global staff the consultant will submit a final product and a verbal
presentation. Note that we do not necessarily expect the end-product to be a classic report. We highly
recommend the deliverables to be presented in a format that is easily accessible and that can be adapted
to share with various stakeholders.
8. MANAGEMENT AND GOVERNANCE OF THE EVALUATION
This consultancy will be directly managed by the lead consultant who will assume overall responsibility for
the deliverables. Ancella Voets, Lead: HIV Technical Harm Reduction (avoets@frontlineaids.org) will act as
the first point of contact for the (team of) consultant(s) and will be responsible for overseeing the
implementation of the evaluation. For issues directly related to the IHRP, consultant will contact Revati
Chawla, Lead: Programmes (rchawla@frontlineaids.org), while for issues related to PITCH, consultant will
contact Lucas Hendriksen, Lead: Programmes (lhendrinksen@frontlineaids.org).
Logistic matters will be organised with Caitlin Maslen, Support Officer: Programmes. Payment will be processed
upon completion of the deliverables and submission of a final invoice to Caitlin at
cmaslen@frontlineaids.org and payments@frontlineaids.org.
Frontline AIDS will support all stages of the process including providing relevant documentation, assisting in
the organisation of data collection (providing contact details, facilitating access to interviewees and relevant
data), providing feedback on drafts of all agreed outputs, including the methodology.
The study will be guided by a Frontline AIDS steering committee. They will provide input into the proposed
tools and methodologies and sign off final deliverables
Terms of Reference Frontline AIDS Harm Reduction Evaluation 2020 89. TIMELINE Action Timeline Publish for expressions of interest to find consultant 03/07/20 Expression of interest/proposal submitted to Frontline AIDS 24/07/20 Frontline AIDS selects consultant/s 07/08/20 Contracting: development of Purchase Order and payment terms 14/08/20 Inception report, work plan and methodology agreed 04/09/20 Consultant starts data collection 07/09/20 Consultant starts data analysis and interpretation 21/09/20 Consultant starts drafting evaluation report 05/10/20 First draft evaluation report 19/10/20 Final evaluation report 02/11/20 It is envisaged that this work will take approximately 30 days. 10. PROFILE OF CONSULTANT / CONSULTANCY TEAM The successful bidder will have one or more members who meet the following criteria: Essential • Substantial experience in conducting research/evaluations of HIV strategies and interventions; • Experience in undertaking assessments using quantitative and qualitative methodologies; • Experience working in an international development context; • Understanding of participatory research approaches, including experience with marginalised populations; • Ability to systematically analyse and present complex data and information; • Experience involving PWUD people in research/evaluation processes; • Experience in conducting evaluations of harm reduction programmes in low- and middle-income countries; • Excellent communication and facilitation skills; • Excellent written and spoken English; • Ability and commitment to deliver the expected results within the agreed period of time. Desirable • Witten and spoken French 11. CONFIDENTIALITY & PROPRIETARY INTERESTS The consultant(s) shall not, either during the term or after termination of the assignment, disclose any proprietary or confidential information related to the assignment without prior written consent from Frontline AIDS management. We are looking for a consultant team comprising of those who are independent of Frontline AIDS and the Dutch Ministry of Foreign Affairs (MoFA) i.e. not an employee of either the Dutch MoFA or Frontline AIDS. Previous working experience in either organisation is not an exclusion criteria. Terms of Reference Frontline AIDS Harm Reduction Evaluation 2020 9
12. SUBMISSION OF EXPRESSION OF INTEREST (EoI) Interested consultants should email their expression of interest and CV to: Caitlin Maslen cmaslen@frontlineaids.org no later than 24th July 2020. The submission of EoI need to include a proposed methodology of how the evaluation will be done, how long it will take and how the findings will be validated, presented and shared, and their daily rate. In addition, the chosen evaluator(s) will need to draft/adjust further evaluation questions (as part of the proposed methodology) in consultation with the core team. Given the current circumstances of lock down measures related to the COVID-19 pandemic, the selected evaluator(s) are expected to present a plan that can be implemented, from inception to presentation, through online communication, knowing that such communication may be challenging for some partners, due to limited connection quality. Depending on where the consultant is based and on the severity of lock down measures in that specific time and place, a visit to one of the implementation sites may be possible, but is not assured. Terms of Reference Frontline AIDS Harm Reduction Evaluation 2020 10
ANNEX 1: SUMMARY OF PITCH END TERM EVALUATION
Objectives, themes and questions
1. To assess the outcomes and impact of PITCH, as well as their sustainability, in the context of the
programme’s Theory of Change
a. Which significant advocacy outcomes has PITCH made a measurable contribution to? To what extent
does evidence exist to support these claims of contribution?
b. How has PITCH contributed to any positive or negative unexpected outcomes? What lessons have been
learned, and how have these unexpected outcomes influenced partners’ advocacy planning?
c. Which PITCH advocacy strategies have been most effective in allowing PITCH partners to achieve their
advocacy asks? What lessons can be learned from this?
d. Reflecting on structural and legislative changes, how sustainable are the achievements of PITCH
beyond the programme’s lifetime, and in the absence of significant external funding?
e. To what extent has PITCH measurably and sustainably strengthened the advocacy capacity of PITCH
partners, including the capacity to capture evidence to support their advocacy?
f. To what extent has the capacity of PITCH partners to apply a gender transformative approach to their
work been strengthened? How has this been achieved? What impact has this had on the outcome of
PITCH country level advocacy activities?
g. What lessons can be learned about how gender informs advocacy carried out on behalf of Key
Populations and Adolescent Girls and Young Women?
h. From the perspective of different PITCH stakeholders, including implementing partners, which
programmatic strategies and approaches have partly or entirely failed? What lessons can we learn
from this?
2. To understand the extent to which internal and external PITCH stakeholders have benefited from
collaborating with each other
a. To what extent have country partners and global policy partners benefited from/connected with each
other’s advocacy activities?
b. To what extent have country partners and regional programme partners benefited from/connected
with each other’s advocacy activities?
c. To what extent have regional programme and global policy partners benefited from/connected with
each other’s advocacy activities?
d. To what extent have PITCH partners formed or joined coalitions with other civil society organizations
that have helped to advance their advocacy, raise the profile of the experiences of Key Populations
and Adolescent Girls and Young Women, and to set the advocacy agenda?
e. To what extent can examples of effective collaboration at the country level be demonstrated between
PITCH and other MoFA funded programmes working to address HIV/AIDS?
f. To what extent have working relationships between PITCH, and the Dutch embassies and Permanent
Missions in the PITCH countries, contributed to advocacy outcomes through strategic collaboration?
Methodology
1. Key informant interviews
2. Focus groups discussions
3. Desk-based literature review and comparative analysis of data
4. 2-day reflection meetings using an outcome harvesting methodology to better understand and document
evidence of PITCH partners’ contribution to the most significant, observable changes identified.
Terms of Reference Frontline AIDS Harm Reduction Evaluation 2020 11The intention is to harvest at least 8 most significant outcomes in each country or region and at the global level and substantiate 4 of these outcomes, each by 2 independent persons who are knowledgeable about the harvested outcomes. The intention is to harvest a total of (9 countries + 2 regions + 1 global level) * 8 outcomes = 96 outcomes, half of which will be substantiated. The OH will be used to answer evaluation question 1.1, 1.2 and 1.4; and will involve as much as possible all relevant stakeholders of the PITCH programme. The harvested outcomes, in particular the secton contributions of PITCH to the outcome will further be used by the HIV, gender and SRHR expert evaluators to develop stories of change that will give insight into the process contributing to the outcomes, relevance of the outcomes from diverse perspectives and other relevant changes. Terms of Reference Frontline AIDS Harm Reduction Evaluation 2020 12
ANNEX 2: AVAILABLE DOCUMENTATION
• Frontline AIDS Global Theory of Change (2020-2025)
• Frontline AIDS Global Plan of Action (2020-2025)
• Frontline AIDS Community Responses to HIV Evidence Map (2019)
• Harm reduction theory of change (2018)
• Harm reduction investment case (2018-2020)
• Harm reduction fundraising strategy (2018-2020)
• Documents produced by the PITCH ETE team (probably available by October 2020)
• IHRP M&E tool tracker
• IHRP & PITCH partners’ annual workplans
• IHRP partners’ annual narrative reports and summarised annual results presentations
• PITCH annual narrative reports
• PITCH advocacy logs in DHIS2 database
• Selected PITCH newsletter items
• Selected stories of change from PITCH (partners)
• Publications under the IHRP
o Piloting alternatives to incarceration to address drug use in China
o Harm Reduction programming in Kenya
o How can women who use drugs demand their sexual and reproductive health and rights
o A guide on advancing the sexual and reproductive health and rights of women who use drugs
o Three ways India is making drug use safer
o Understanding why people who inject drugs in Indonesia are disengaged from HIV testing and treatment:
gaps in the HIV treatment cascade
• Report of the Strategic harm reduction meeting of November 2019
Terms of Reference Frontline AIDS Harm Reduction Evaluation 2020 13You can also read