GBS Young Infant Disease Burden, Trends and Prevention Strategies: High Income Countries - GBS Young Infant ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

National Center for Immunization & Respiratory Diseases
GBS Young Infant Disease Burden, Trends and
Prevention Strategies: High Income Countries
Stephanie Schrag, D Phil
US Centers for Disease Control and Prevention
FDA Vaccines and Related Biological Products Advisory Committee Meeting,
May, 2018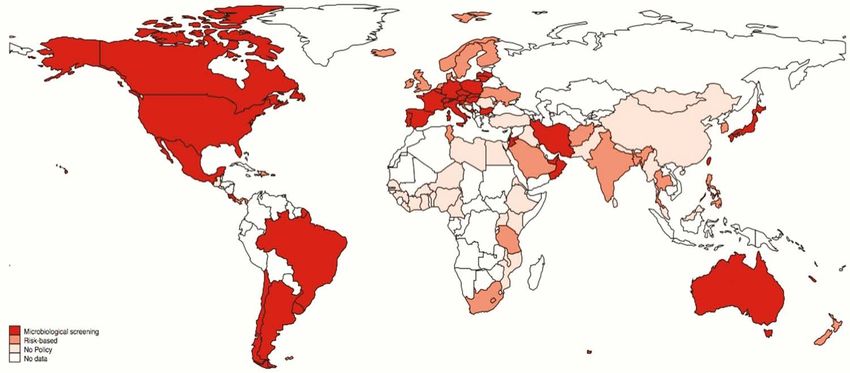
DISCLOSURES
Not involved in any clinical trials involving GBS vaccines sponsored by
either GSK or Pfizer.
Serve on two committees as part of my official Federal duties that are
related to the matter coming before the committee.
1. Chair of the WHO GBS vaccine development working group
2. Member of the World Health Organization/London School of
Hygiene and Tropical Medicine advisory group to develop a value
proposition for vaccines against GBS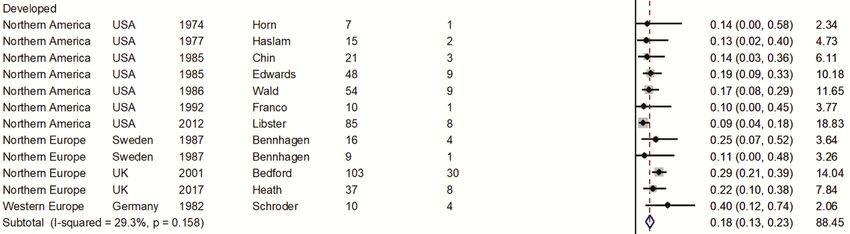
Sixty year anniversary: Emergence of GBS sepsis and
meningitis in infants
1958: Yale Hospital, Connecticut1; Charity Hospital, New Orleans2
1962–3: Boston City Hospital3
1965–72: St Louis Children’s Hospital4
1969–71: Several Colorado Hospitals (incidence: 2/1000 live births) 5
1970–72: Baylor College Affiliated Hospitals, Texas6
UK, 1968: First infant GBS report7; rapid emergence in 1970s
1Nyhan, WL et al. 1958 Pediatrics; 2Hood, M et al, AMHOG 1961; 3Eickhoff, TC et al. 1964. N Engl J Med 1964; 4Barton, LL et al,1973. J Peds; 5Franciosi R. et al. 1973. J
Peds; 6Baker,
CJ et al. 1973. J Peds; Ismail, A. et al. Neonatology, 2011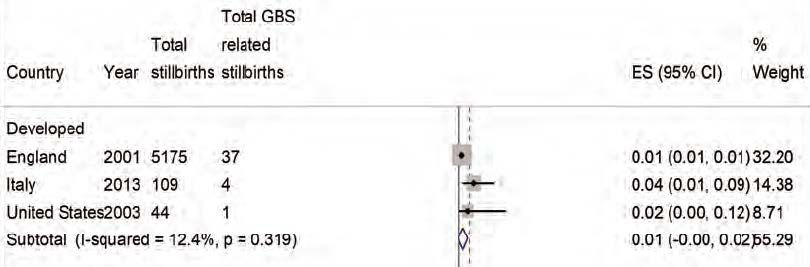
GBS Disease in Infants Before Prevention Efforts
These charts show the age 80distribution of invasive GBS disease in infants
100
Percent of cases
90before prevention
Early-onset efforts, by
(EOGBS): 60
age in months, weeks, or (for early-onset cases
0–6 days of life
80only) days. Approximately 80% of infant infections occur in the first days of
40
Percent of cases
20
70
60life. Late-onset infections occur0 in infants between 1 5week and 89 days of age.
0
1 2 3 4 6
Age (days)
50
40
30 Late onset: 7–89 days of life
20
10
0
< 1 1-3 1 2 3 4 5 6 7 8 9 10 11
wk wk
Age (months)
A Schuchat. Clin Micro Rev. 1998;11:497–513.
Early-onset GBS Risk Factors: Maternal Colonization
~10–30% pregnant women colonized with GBS
– Higher prevalence among African Americans
Can be transient, intermittent or persistent; genitourinary or gastrointestinal tract
serves as reservoir
Acquired vertically
– GBS ascends to amniotic cavity during labor
• Aspiration leads to pneumonia/bacteremia
– Exposure during passage through birth canal
• Colonization of skin/ mucus membranes
– GBS can also cross intact amniotic membranes
Maternal to Infant Transmission (in absence of intervention)
Approximately 10–30% of women~10-30% are colonized with GBS. About half of the
infants born to colonized mothers are themselves colonized. The majority of
GBS colonized mother
colonized infants (98%) are asymptomatic. In the absence of intervention,
about 2% of colonized
50%infants will develop early-onset
50%disease (e.g., sepsis,
pneumonia, meningitis).
Non-colonized Colonized
newborn newborn
98% 2%
Early-onset sepsis,
Asymptomatic pneumonia, meningitis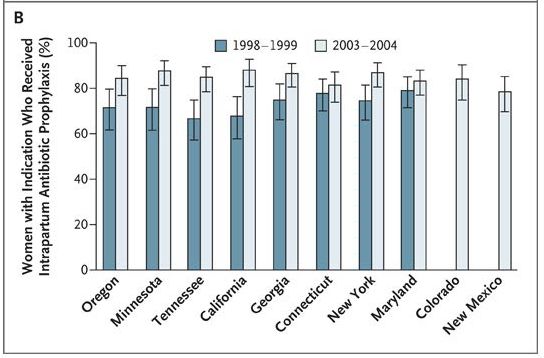
Intrapartum antibiotic prophylaxis (IAP) to prevent GBS disease
in first week of life
Clinical trials and well-designed observational studies (1980s)
– IV penicillin or ampicillin
– Given to GBS-colonized women (+/- additional risk factors)
Efficacy against invasive early-onset disease: 100%
– Effectiveness in observational studies: 86–89%
1970s: Work towards a maternal GBS vaccine launched
Allardice et al. 1982, Am J Obstet Gynecol; Boyer and Gotoff. 1986. N Engl J Med; Lim et al., 1986, J Clin Micro; Tupperainen et al., 1989. Obstet Gynecol ; Garland et al,
1991, Aust NZ J Obstet Gynecol; Matorras et al. 1991 Eur J Obstet Gynecol Reprod Biol.
Debate: How best to target women for IAP
Risk-based strategies
– GBS bacteriuria, prolonged membrane rupture, premature rupture of
membranes, preterm delivery, intrapartum fever, previous infant with GBS
disease
– Flexibility in risk factors considered (narrow vs more comprehensive)
Microbiologic screening for GBS colonization
– 50% more effective than risk-based approach1
– Requires laboratory capacity and cost of antenatal screens
Concerns: Antimicrobial resistance and disruption of newborn microbiome
– Deliveries exposed to IAP, US: 12% pre-prevention; 32% IAP era
– Similar under screening or broad risk-based approach
1Schrag et al. 2002. NEJM 347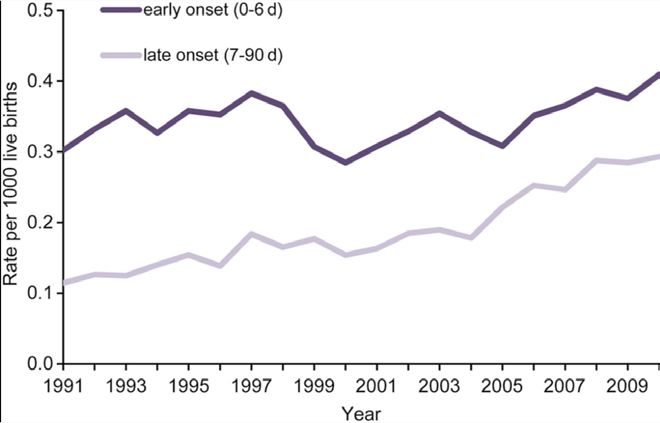
US perinatal GBS disease prevention guidelines In 1996, CDC published “Prevention of Perinatal Group B Streptococcal Disease: A Public Health Perspective,” which recommended either risk-based or microbiologic screening. In 2002, CDC published “Prevention of Perinatal Group B Streptococcal Disease: Revised Guidelines from CDC,” which recommended universal microbiologic screening. The most recent guidelines, “Prevention of Perinatal Group B Streptococcal Disease: Revised Guidelines from CDC, 2010” made small refinements to the 2002 guidelines. 1996: Either risk-based or 2002: Universal 2010: Small refinements microbiologic screening microbiologic screening MMWR, Vol 59(RR-10)
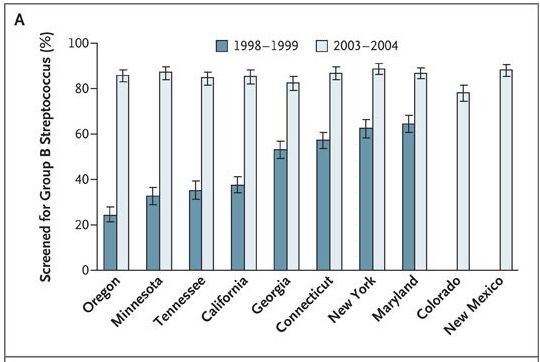
Rapid transition to universal screening: Proportion of women
screened for GBS pre- and post-2002
A bar chart showing how quickly 10 states transitioned to universal screening
after CDC’s guidelines were published in 2002. From 1998 through 1999,
these states screened about 48% of pregnant women. By 2003 through 2004,
this number had increased to 85%.
•Increased from 48% to 85%
•98% had available result at labor
Van Dyke et al., N Engl J Med. 2009Proportion of women with indication receiving IAP increased
under universal screening
A bar chart showing how the proportion of pregnant women with an
indication who went on to receive intrapartum antibiotic prophylaxis (IAP)
increased under universal screening. From 1998 through 1999, 74% of
women with an indication actually received IAP. By 2003 through 2004, this
number had increased to 85%.
•Increased from 74% to 85%
Van Dyke et al., N Engl J Med. 2009Active Bacterial Core Surveillance (ABCs) System
Minnesota
New York
Oregon
Connecticut
Colorado
California Maryland
Tennessee
Georgia
New Mexico
• Surveillance began in 3 sites, 1989
• Live births in 10 current ABCs sites ~10% of US births
• GBS from a normally sterile site, all ages
• Early-onset GBS disease: 0-6 days of life; Late-onset: 7-89 days
www.cdc.gov/abcsInvasive early- and late-onset disease trends, US ABCs
2.00
A line graph showing invasive early- and late-onset disease trends from 1990
1.80
First consensus guidelines
through 2015 from Active Bacterial Core surveillance. In 1990, the incidence
1.60
Cases per 1000 live births
of early-onset disease was more than 1.7 cases per 1,000 live births. The
1.40
incidence decreased dramaticallyUniversal
1.20
through 1999 (a little more than 0.4 cases
screening
Minor guidelines revisions
per 1,000 live births) and continued to decrease gradually through 2015 (a
1.00
little more than 0.2 cases per 1,000 live births). During this same time period,
0.80
late-onset disease incidence has remained relatively stable at around 0.3
0.60
cases per 1,000 live births.
0.40
0.20
Early-onset disease Late-onset disease
0.00
Year
Schrag and Verani. Vaccine 2013; Nanduri S et al. ISSAD 2018GBS disease serotype distribution over time, ABCs
1999–2005 2006–2015 5-valen t 6-valent (+
n=997 n=1743
coverag e t ype IV)
Pie charts showing that GBS serotype distribution has remained relatively
stable over time according to ABCs data. Serotypes Ia93 .2%III cause99.3%
and most early-
onset GBS disease, followed by II and V, then Ib. Serotype III causes about half
Early-onset
of late-onset GBS disease, followed by Ia, V, Ib, and II.
93.6% 99.7%
Late-onset
Ia Ib II III V Other
Phares, C. et al. JAMA 2008; Nanduri, S. et al., ISSAD 2018Antimicrobial susceptibility, young infant GBS disease,
ABCs
Beta-lactam non-susceptibility rare
– 1% of adult invasive isolates non-susceptible to beta-lactams, 2015/16
Resistance to second line agents common in 2015
– Erythromycin: 49% of isolates
– Clindamycin (constitutive): 26% of isolates
Metcalf, BJ et al., Clin Microbiol Infect 2016; Nanduri, S et al., ISSAD 2018; McGee; L. et al ISSAD 2018US remaining infant GBS disease, ABCs, 2006–15
Early-onset , % (n=1277) Late-onset , % (n=1388)
Age at onsetComparison to other US diseases where maternal
immunization is in use or under consideration
Condition (infantsSequelae among GBS infection survivors: 18% have
moderate to severe impairment* post-meningitis
12/18 studies were from high income countries
*Neurodevelopmental impairment assessed at 18 months of follow-up
Kohli-Lynch, M. et al. 2017. CID 65: Suppl 2Additional disease burdens that might be prevented
by a maternal GBS vaccine
Maternal GBS disease: an estimated 175 maternal invasive cases in US per
year1
GBS associated stillbirths: approximately 1% of stillbirths2; limited data
1Phares, C. et al., JAMA 2008; 2Seale, A. et al. Clin Infect Dis 2017Cost-effectiveness of a potential maternal GBS vaccine, US
Healthcare sector perspective, 2013 U.S.$
Screen/IAP prevents EOGBS: $70,275/QALY, compared with no prevention.
Maternal GBS immunization, pentavalent vaccine, 70% effective against
covered serotypes, prevents EOGBS and LOGBS: $56,609/QALY, compared
with no prevention.
BUT … at coverage typical of current maternal vaccines (~50%), GBS
vaccine would prevent fewer cases of disease than Screen/IAP … unless
the vaccine were 90% effective.
A combination strategy, vaccination with Screen/IAP for unvaccinated
women, would prevent more disease than either alone, at costs/QALY
similar to Screen/IAP.
Kim S-Y et al., Vaccine 2017Global adoption of policies for GBS prevention LeDoare, K. et al. 2017. CID 65. Suppl 2.
Trends in early and late-onset disease, United
Kingdom and Ireland
Incidence / 1000 live births 2000–2001 2014–2015
Overall 0.72 0.95
EOD 0.48 0.55
LOD 0.24 0.38
Lamagni, T. et al. 2013. CID O’Sullivan et al., ESPID, 2016Invasive early and late-onset trends, Netherlands
Risk-based IAP
1990 1995 2000 2005 2010
Bekker et al. 2014. Lancet Infect DisMost recent high income country incidence estimate, young
infant GBS disease*: 0.46/1000 live births (EOD: 0.37, LOD: 0.21)
*Invasive disease, day 0-89 of life
Madrid, L. 2017. CID 65; Suppl 2.Global GBS serotype distribution, meta-analysis
Early-onset Late-onset
Madrid, L. et al., CID 2017: 65 (Suppl2). Based on data from 2000-2017 (N=6500 isolates)High income country experience: where are we today?
Remaining disease burden of significance
– US: Despite 80% decline in early-onset disease incidence
– UK, Netherlands: Increasing young infant GBS disease
Further major declines through improved IAP unlikely in US
– Does not prevent late-onset disease
Beta-lactam non-susceptibility has emerged but remains rare
– If it becomes more common it could threaten current prevention and
treatment strategies
Long-term consequences of newborn microbiome disruption due to IAP poorly
understood
– CDC has funded two large observational evaluationsEmerging incidence of invasive GBS disease among
non-pregnant adults, ABCs: 10.9/100,000 in 2016
US estimate: 27,729 cases of invasive GBS disease and 1,541 deaths in 2016
www.cdc.gov/abcsAcknowledgements
• Entire ABCs team
• Srinivas Nanduri
• Paul Heath
The findings and conclusions in this report are those of the
authors and do not necessarily represent the official
position of the Centers for Disease Control and Prevention.
For more information, contact CDC
1-800-CDC-INFO (232-4636)
TTY: 1-888-232-6348 www.cdc.gov
ABCs Surveillance Officers
The findings and conclusions in this report are those of the authors and do not necessarily represent the
official position of the Centers for Disease Control and Prevention.You can also read

















































