Global architecture for the nutrition training of health professionals: a scoping review and blueprint for next steps - BMJ Nutrition ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Open access Review
Global architecture for the nutrition
BMJNPH: first published as 10.1136/bmjnph-2021-000354 on 16 February 2022. Downloaded from http://nutrition.bmj.com/ on June 23, 2022 by guest. Protected by copyright.
training of health professionals: a
scoping review and blueprint for
next steps
Breanna Lepre ,1,2 Helena Trigueiro,1 Jørgen Torgerstuen Johnsen ,1
Ali Ahsan Khalid,1 Lauren Ball ,1,3 Sumantra Ray 1,4,5
To cite: Lepre B, Trigueiro H, ABSTRACT
Johnsen JT, et al. Global What this paper adds
Background This paper provides an overview of
architecture for the nutrition capacity-building efforts in the context of nutrition
training of health professionals: ► This paper provides a critical synthesis of capacity-
education for medical and healthcare professionals.
a scoping review and building efforts in the context of nutrition education
Methods Content analysis of eighteen reports related to
blueprint for next steps. BMJ for medical and health care professionals to high-
Nutrition, Prevention & Health nutrition education and capacity building, and interviews
light gaps and opportunities for improvement in
2022;0:e000354. doi:10.1136/ with key personnel from the WHO and NNEdPro Global
the wake of the UN Decade of Action on Nutrition
bmjnph-2021-000354 Centre for Nutrition and Health were synthesised.
(2016-2025).
1 Recommendations to improve nutrition education and
NNEdPro Global Centre for ► Ongoing data collection on the nutrition education
Nutrition and Health, Cambridge, subsequent nutrition capacity of healthcare professionals
and training of medical and healthcare professionals
UK were identified based on policy guidance and interviews.
is likely to facilitate improvements in nutrition ca-
2
School of Medical, Indigenous Findings Most included documents noted the importance
pacity building, with subsequent benefits to popu-
and Health Sciences, University of nutrition education and capacity building for medical
lation health.
of Wollongong, Wollongong, and healthcare professionals. Healthcare professionals and
► Key recommendations include: 1) the establishment
NSW, Australia the ‘health sector’ were positioned as central to achieving
3
Menzies Health Institute, of a national curricula for nutrition education across
improved public health, and the promotion of nutrition
Queensland, Griffith University - all healthcare sectors, including the development
knowledge and awareness in the general population.
Gold Coast Campus, Southport, and expansion of online resources, 2) Organisational
Conclusion Increased focus on nutrition education and
Queensland, Australia and government pledges for the adoption of nutri-
4 capacity of the health workforce are key to improvements
School of Biomedical Sciences, tion education in community and healthcare and 3)
Ulster University, Coleraine, UK in population health and well-being. The WHO is well
Improved global data collection mechanisms and
5
School of Humanities and placed to support global nutrition education.
validated indicators to assess and measure capacity
Social Sciences, University of Recommendations Key recommendations from the
and progress.
Cambridge, Cambridge, UK literature review and interviews include improved global
data collection mechanisms, a pledge from governments
Correspondence to to prioritise nutrition education and capacity building,
Breanna Lepre, NNEdPro Global along with implementation of standardised nutrition
Decade of Action on Nutrition (2016–2025)
Centre for Nutrition and Health,
curricula for all healthcare sectors. This would include the (Nutrition Decade) is a commitment of
Cambridge CB4 0WS, UK; Member States to undertake sustained imple-
development and expansion of on-line resources.
b.lepre@nnedpro.org.uk and
mentation of policies and interventions to
Professor Sumantra Ray; address the double burden of malnutrition.5 6
s.ray@n nedpro.org.uk INTRODUCTION The response of member states to the Nutri-
Good health is required for prolonged tion Decade has the potential to influence
Received 16 August 2021
economic and social development.1 Nutrition public health outcomes internationally. The
Accepted 17 January 2022 plays a major role in promoting both good Second International Conference on Nutri-
health and overall quality of life.1 Globally tion (ICN2) Framework for Action and
each year, 11 million deaths are attributable the 2030 Agenda for Sustainable Develop-
to dietary factors, placing poor diet ahead of ment provide an architectural blueprint for
any other risk factor for death.2 Worldwide, action.7 8
690 million people do not have enough to eat, Multiple international efforts are occur-
while 1.9 billion adults are overweight and ring that aim to improve health outcomes
© Author(s) (or their of these 650 million are obese.3 4 This coex- through more favourable diet quality, as well
employer(s)) 2022. Re-use istence of undernutrition along with over- as policy-driven actions at a population-level.9
permitted under CC BY-NC. No
commercial re-use. See rights
weight and obesity and non-communicable As the specialised agency of UN concerned
and permissions. Published by disease is referred to as the double burden with world public health, the WHO has made
BMJ. of malnutrition.1 The United Nation (UN) universal health coverage (UHC) a major
Lepre B, et al. bmjnph 2022;0:e000354. doi:10.1136/bmjnph-2021-000354 1 BMJ Nutrition, Prevention & Health
component of health reform and the overall goal of the education to inform a global approach to medical and
BMJNPH: first published as 10.1136/bmjnph-2021-000354 on 16 February 2022. Downloaded from http://nutrition.bmj.com/ on June 23, 2022 by guest. Protected by copyright.
General Programme of Work 13, thus a priority objective health professional nutrition education. This critical
of the agency.10 The priority encompasses the need for content analysis paper aims to appraise capacity-building
equitable access to high-quality health services and the efforts in the nutrition education of medical and health-
delivery of evidence-based, people-centred care by compe- care professionals to identify current provision supported
tent healthcare professionals.11 These organisations have by the WHO and related standard setting organisations as
a role to play in nutrition education and capacity of the well as highlighting gaps and opportunities for improve-
health workforce. ment in the wake of the UN Decade of Action on Nutri-
Health professionals are well placed to initiate and tion (2016–2025).
support nutrition care as part of routine practice, and
this is recognised as an essential part of usual care by
institutions such as the American Dietetic Association, METHODS
the American Medical Association, the National Academy It was initially identified that this review would take a
of Sciences and the Society of Teachers of Family Medi- pragmatic approach to search and identify literature.
cine.12–16 In order to provide nutrition care, healthcare Therefore, this literature review encompasses both tradi-
professionals need to develop requisite nutrition knowl- tional search methods as well as extensive consultation
edge in addition to capacity and adequate confidence. with experts to iteratively identify relevant documents. A
However, medical doctors have insufficient exposure review of the literature and interviews with key personnel
to nutrition in their medical education regardless of from the WHO Department of Nutrition and Food Safety
geographical region, setting or year of training.17 18 (NFS) took place over a year from December 2018 to
Similar scenarios are reported in other healthcare profes- December 2019. For the purposes of this study, we have
sions.19 For example, nurses require nutrition knowledge defined key concepts below based on published defini-
to improve patient outcomes but report lacking suffi- tions and author experience (table 1).
cient education and training at an undergraduate level,
and limited opportunities for continuing education to Literature review
support high-quality care.20–22 Clearly, there is an oppor- First, all policy outputs from the WHO NFS related to
tunity to enhance nutrition education provided to all nutrition education and capacity were compiled for
medical and healthcare professionals. screening and review. Additionally, consultation with the
Coherent and sustained efforts to enhance the nutri- WHO NFS Office of the Director was used to identify
tion capacity of the health workforce through improved other relevant documents for inclusion. A total of 353
nutrition education may lead to sustained benefits for documents were screened for inclusion by the primary
population health and will, therefore, likely be effective in investigator (SR). Documents published up to 2018 by a
reducing the double burden of malnutrition.23 In order global multilateral organisation such as the WHO related
to improve the nutrition capacity of the health workforce, to education for the health workforce were included.
there is a need to establish consensus on global nutrition Inclusion and exclusion criteria are provided in table 2. In
standards as a benchmark for universities.17 First, there is total, eighteen policy guidance documents were selected
a need to synthesise existing global guidance on nutrition for inclusion (box 1).
Table 1 Definitions of key concepts used within this paper
Concept Definition
Nutrition capacity Capacity at the human, institutional, organisational and infrastructural levels to implement nutrition
programmes and strengthen nutrition governance.60
Dietitian-nutritionist A professional who applies the science of food and nutrition to promote health, prevent and treat
disease to optimise the health of individuals, groups, communities and populations.61 We recognise that
these terms may have different definitions across countries.
Food system The food system includes all interrelated activities involving the production, processing, transport and
consumption of food.62
Food industry The food industry encompasses a series of industrial activities directed at the processing, conversion,
preparation, preservation, and packaging of foodstuffs.63
Nutrition care Any practice that aims to improve the dietary intake of a patient to improve health outcomes.64
Nutrition science Nutrition science deals with all aspects of the interaction between food and nutrients, life, health and
disease, and the processes by which an organism ingests, absorbs, transports, uses and excretes food
substances.65
Clinical nutrition The discipline that deals with the prevention, diagnosis and management of nutritional and metabolic
changes related to acute and chronic diseases and conditions caused by a lack or excess of energy and
nutrients across the life course.65
2 Lepre B, et al. bmjnph 2022;0:e000354. doi:10.1136/bmjnph-2021-000354BMJ Nutrition, Prevention & Health
capacity of the health workforce. A qualitative descrip-
BMJNPH: first published as 10.1136/bmjnph-2021-000354 on 16 February 2022. Downloaded from http://nutrition.bmj.com/ on June 23, 2022 by guest. Protected by copyright.
Table 2 Inclusion and exclusion criteria for eligible
documents tive approach was taken as it enables rich description of
recommendations to improve nutrition education and
Inclusion criteria Exclusion criteria
capacity of the health workforce. A mix of purposive and
Published up to 2018 Published after 2018 convenience sampling was used to recruit participants
Published by a global multilateral Region specific guidance for interviews. The WHO NFS were included given their
organisation role in global nutrition education and capacity building.
Related to education in regard Not related to education Furthermore, many WHO interns were currently under-
to scope of synthesis or taking a form of medical education, and therefore, this
recommendations was seen as an additional capacity-building opportunity.
Relevant to the global health Not related to the health An invitation to participate in an interview was sent to
workforce (as defined in broad workforce all members of the WHO NFS. All who expressed interest
terms) were invited to participate in an interview. Written notes
were taken during the interviews based on responses
to three key questions: (1) Where do you see a role for
Three reviewers independently analysed all full- text medical/healthcare nutrition education within the
documents. A content analysis approach was used to iden- Nutrition Decade efforts and the work of NFS/WHO?;
tify capacity-building efforts in the context of nutrition (2) What do you perceive as the main barriers to policy
education for the health workforce. formulation and implementation around medical/
healthcare capacity building in this area? and (3) Can you
Interviews
identify any current or emerging opportunities to embed
Semistructured face-to-
face interviews were conducted
medical/healthcare nutrition education into primary
with key personnel from the WHO NFS to provide insight
and/or secondary prevention initiatives?
to recommendations to improve nutrition education and
Survey
Box 1 Key policy guidance included in the review NNEdPro networks were engaged to consider regional
implications in countries other than the UK, including
1. Strengthening nutrition action: a resource guide for countries the Australia/New Zealand network. An email about
based on the policy recommendations of the Second International the study was sent to members of the NNEdPro Virtual
Conference on Nutrition.24 Core, an international, multidisciplinary group of 42
2. Driving commitment for nutrition within the UN Decade of Action professionals. All who expressed interest were invited to
on Nutrition.6 participate in a survey, using the same three questions as
3. e-Library of Evidence for Nutrition Actions.25 for interviews. Participants were asked to provide written
4. Global nutrition policy review 2016–2017: Country progress in cre- responses to the questions via email.
ating and enabling policy environments for promoting healthy diets
and nutrition.26
Data analysis
5. Global nutrition monitoring framework: Operational guidance for
tracking progress in meeting targets for 2025.27 Interview and survey data consisted of a combination of
6. 2018 Global Nutrition Report.28 hand-written notes from responses to questions and email
7. Global targets tracking Tool.29 responses. Two researchers were involved in transcribing
8. Implementation guidance: Protecting, promoting and supporting and validating the responses to check the accuracy. Inter-
breastfeeding in facilities providing maternity and new born servic- view and survey responses were analysed using a compara-
es: the revised baby-friendly hospital initiative.9 tive content analysis approach by the primary investigator
9. Taking Action on Childhood Obesity.30 (SR), whereby individual responses from participants
10. Knowledge Action Portal: Nutrition Knowledge Hub.31 were analysed for common themes, which were then
11. UNICEF-WHO-World Bank Group Joint Child Malnutrition Estimates: collapsed into conjoined statements related to recom-
Key findings of the 2018 edition.32
mendations to improve nutrition education and capacity
12. Weekly iron and folic acid supplementation as an anaemia-
of the health workforce.
prevention strategy in women and adolescent girls. Lessons learnt
from implementation of programmes among non-pregnant women Findings from the review of 18 included publications
of reproductive age.33 and data from interviews with 11 individuals from the
13. Thirteenth general programme of work 2019–2023.10 WHO NFS and written responses from 29 members of
14. Healthy Diet—Fact Sheet.34 the NNEdPro Global Centre for Nutrition and Health
15. Advancing equity, equality and non-discrimination in food systems: (n=40) were synthesised using triangulation. Data were
Pathways to reform.35 organised into key themes to highlight gaps and opportu-
16. The Food and Agriculture Organization of the United Nations nities for improved nutrition education and capacity for
Website.36 health professionals. Themes from key outputs, namely
17. United Nations System Standing Committee on Nutrition (UNSCN) presentations, related to global nutrition capacity are also
Website.37
summarised and inform the recommendations and next
18. Global Governance for Nutrition and the role of UNSCN.38
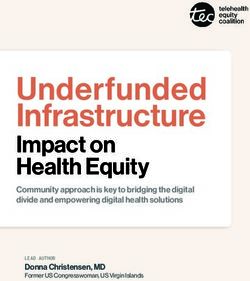
steps. A schematic of methods is provided in figure 1.
Lepre B, et al. bmjnph 2022;0:e000354. doi:10.1136/bmjnph-2021-000354 3 BMJ Nutrition, Prevention & Health
healthcare professional nutrition education and capacity
BMJNPH: first published as 10.1136/bmjnph-2021-000354 on 16 February 2022. Downloaded from http://nutrition.bmj.com/ on June 23, 2022 by guest. Protected by copyright.
and (2) Recommendations to improve nutrition educa-
tion and capacity. Recommendations from the literature
review are grouped into the following subthemes: (A)
Nutrition champions, (B) Government and policy, (C)
Nutrition education and resources, and (D) Governance
of nutrition.
The importance of medical/healthcare nutrition education and
capacity
Sixteen of 18 (89%) documents made some mention
of the importance of nutrition education in capacity
building for the healthcare workforce.6 9 10 24–38
Healthcare professionals and the healthcare system
were identified as central to the promotion of nutrition in
the general population and subsequent improved public
health. Almost all countries in the review (153/159; 96%)
reported nutrition-focussed professionals as part of their
workforce (nutritionists or dietitians as regulated health
professionals).26 However, the density of trained nutrition
professionals, which refers to a policy environment and
capacity indicator related to the number of trained nutri-
tion professionals per 100 000 population, varied greatly
by country, which may reflect the capacity of a country
to design and implement nutrition policy and inter-
ventions.27 Among the 126 countries that reported the
number of nutrition professionals, only 23 (18.3%) had
the recommended density of 10 nutrition professionals
per 100 000 population or higher.26
The healthcare system was identified as the primary
delivery channel for nutrition interventions. The educa-
tion sector was reported to be involved in the imple-
mentation of national nutrition policies in 69 out of 110
countries (63%), and in the implementation of nutrition
programmes in 83 out of 127 countries (65%). Policy
actions to promote healthy diets were more strongly
related to education than to regulatory measures. Nutri-
tion education and counselling on healthy diet were
Figure 1 Schematic of methods used. included in national policies by more countries than any
other action (75%).26
RESULTS
Overall, four key themes were identified based on the liter- Recommendations to improve nutrition education and capacity
ature review, interviews and workshops: (1) The impor- This policy analysis synthesises a number of proposed strat-
tance of medical and healthcare professional nutrition egies to improve nutrition capacity including nutrition
education and capacity, (2) Barriers to the application of advocacy, pledges from governments, supportive policy
nutrition in practice, (3) Barriers to policy formulation including coherence between trade and nutrition poli-
and implementation related to medical and healthcare cies, nutrition education and research and monitoring,
nutrition capacity building and (4) Recommendations to surveillance and evaluation systems related to nutrition
improve medical and healthcare professional nutrition and health. A summary of recommendations synthesised
education and capacity which included (A) Nutrition from the literature review is provided in table 3.
education and resources, (B) Nutrition research, (C)
Nutrition champions, (D) Government and policy and Nutrition champions
(E) Governance of nutrition. Findings are stratified by The Food and Agriculture Organization of the United
method (ie, policy analysis and interviews and workshops). Nations (FAO) recommends the provision of tools, guid-
ance and support for the scaling up of nutrition educa-
Literature review tion and consumer nutrition awareness at a national
A literature review of policy guidance identified two key and local level.39 One of these suggested tools is nutri-
themes as follows: (1) The importance of medical and tion champions, who are able to advocate for nutrition
4 Lepre B, et al. bmjnph 2022;0:e000354. doi:10.1136/bmjnph-2021-000354BMJ Nutrition, Prevention & Health
BMJNPH: first published as 10.1136/bmjnph-2021-000354 on 16 February 2022. Downloaded from http://nutrition.bmj.com/ on June 23, 2022 by guest. Protected by copyright.
Table 3 Key recommendations and examples for improvement in nutrition education and capacity building (from literature
review)
Recommendation Example
(A) Nutrition champions—advocates for nutrition education Advocacy for increased investment in nutrition
(B) Government and policy—key role in interinstitutional Allocation of financial resources for physical infrastructure
cooperation on nutrition education and capacity building and facilities
(C) Nutrition education and research—provides evidence base Design a rigorous evidence-based medical curriculum
and training of personnel to improve nutrition behaviour and
subsequent nutritional status
(D) Governance of nutrition—review and measure ongoing Monitoring progress of nations using objective and
progress validated indicators such as nutrition professionals density
education, based on recognition that a champion cannot building. Recommendations for the delivery of nutrition
work alone and requires capacity and resources.9 The education for the wider community included the use of
Work Programme of the Nutrition Decade suggest nutri- smart technologies to deliver simple and targeted nutri-
tion advocates can empower others to make healthy tion advice to the general population. There are oppor-
lifestyle choices through public nutrition information.5 tunities to strengthen and champion resources to make
For example, at the local level, United Nations System this a key aspect of future policy. Accessible, evidence-
Standing Committee on Nutrition (UNSCN) guidance based public nutrition education is key to empowering
suggests women may have a role as nutrition champions individuals and communities to make healthy dietary
by passing on nutrition knowledge and skills to their choices.
community. Not only does this have the potential to Other recommendations on nutrition education and
improve the nutrition capacity of the wider community, capacity include nutrition education for teachers, as a
but it is also a platform to advance equity, equality and platform for the incorporation of nutrition education in
non-discrimination in food systems. This may be particu- school curricula, and community-based nutrition inter-
larly relevant in rural and remote areas.35 ventions delivered by healthcare workers, particularly in
rural and remote areas. For example, eLENA lists a range
Government and policy
of nutrition interventions such as breastfeeding education
Other recommendations for improvements to existing
for increased breastfeeding duration. Evidence suggests
nutrition education and capacity of the medical and
that educational interventions which target nutrition
healthcare workforce included pledges from local govern-
behaviour such as formal breastfeeding education during
ments to prioritise nutrition education to healthcare
professionals. These pledges were identified as one way to pregnancy may increase the duration of breastfeeding,
support drafting, piloting and delivery of nutrition educa- which has many health benefits for both the mother and
tion to healthcare professionals at scale and provide UHC child.9 25
by 2030, as part of the SDGs.40 Nutrition monitoring, surveillance and evaluation systems related
Nutrition education and research to nutrition and health
The FAO and the WHO recommend continued research A number of documents detail the importance of
on and release of nutrition evidence, data and guide- systems to review and measure on-going progress related
lines related to food composition, nutrition assessment, to established nutrition education and capacity goals.
food-based indicators and human nutrition requirements The majority of countries in this policy analysis reported
across the lifespan.25 The WHO e-library of Evidence for tertiary- educated nutrition professionals as part of
Nutrition Actions (eLENA) recommend expansion and the health workforce. The validated Nutrition Profes-
dissemination of open access nutrition resources and sionals Density measure is recommended as an inter-
evidence and adequate training of relevant WHO staff national indicator for monitoring nutrition capacity.27
in nutrition policy, in order to assist countries to success- The Global Nutrition Monitoring Framework recom-
fully implement and scale up nutrition interventions.25 mends the validity of the indicator is continually reas-
There was recognition within policy guidance of the sessed as national and global nutrition and health data
need to establish a curriculum for nutrition education is accrued.27 Many publications in this analysis state the
across all healthcare sectors, including the development importance of nutrition education for the wider commu-
and expansion of online resources to assist in nutrition nity. Therefore, it is recommended that there are also
capacity building. indicators in place to monitor the effect of nutrition
Many of the publications reiterate the need to upscale education on population health status, dietary choices
community-based programmes which facilitate commu- and the food industry, which ultimately has an impact
nity participation in nutrition education and capacity on the former.
Lepre B, et al. bmjnph 2022;0:e000354. doi:10.1136/bmjnph-2021-000354 5 BMJ Nutrition, Prevention & Health
Interviews and workshops
BMJNPH: first published as 10.1136/bmjnph-2021-000354 on 16 February 2022. Downloaded from http://nutrition.bmj.com/ on June 23, 2022 by guest. Protected by copyright.
Table 4 Key recommendations and examples for
The three key themes identified from interviews, the improvement in nutrition education and capacity building
survey and workshops were as follows: (1) Barriers to the (from interviews, the survey and workshops)
application of nutrition in practice, (2) Barriers to policy
Recommendation Example
formulation and implementation related to medical
and healthcare nutrition capacity building and (3) Nutrition education—to teach Training in nutrition
Recommendations to improve medical and healthcare healthcare professionals the role counselling and
of nutrition and its role in health understanding of referral
professional nutrition education and capacity. Recom-
and disease, and to empower pathways
mendations from interviews are grouped into (A) Nutri-
introduction of evidence-based
tion education and (B) Nutrition research. All illustrative interventions
quotes below are from WHO NFS team members. Nutrition research —to broaden To identify and research
the evidence base of nutrition- problems with nutrition
Barriers to the application of nutrition in practice based interventions and related care
Despite strong agreement among key WHO NFS policies
personnel that nutrition is an important component of
healthcare, participants identified a number of barriers
to the application of nutrition care in practice, which There are multiple actors (including INGOs [inter-
could be addressed by policy. Interview participants national non- governmental organization], NGOs
reported a lack of healthcare professionals with adequate [non- governmental organization]) providing train-
nutrition skills and knowledge as a barrier to nutrition ing on the same topics that are not only less effective
care in practice. but also confusing to the Field Health Workers. Lack
of co-ordination is a serious problem.
Lack of nutrition professionals (e.g., nutritionists, di-
etitians) at each level of health care Furthermore, participants reported that while nutrition
professional density is an important indicator and associ-
A lack of specific knowledge and skills were high- ated with all six global nutrition targets, the definition of
lighted as barriers by participants including a lack of a nutrition professional remains unclear.
focus on motivational interviewing techniques in health
professions nutrition education. Similarly, participants But the question is how a country defines “nutrition
felt current nutrition education was limited by a lack of professionals” and collect the data and report—are
training on practical nutrition recommendations, such as those comparable across countries?
recommendations for infant feeding.
Recommendations for improvements to nutrition education and
Medical professionals are so heavily focused on clin- capacity
ical aspect of healthcare that nutrition almost even A summary of key recommendations from interviews, the
does not exist in their thought. For instance, most survey and workshops is provided in table 4. Illustrative
doctors, even paediatricians in many countries are quotes from NNEdPro personnel are also included from
not trained in infant and young child feeding (breast- this point onwards.
feeding or complementary feeding).
Nutrition education
WHO personnel identified other barriers to the provi- Education was seen as a steppingstone to a wider impact
sion of nutrition care, such as limited time with patients and needs to be connected to capacity building and
and the difficulty of eliciting positive behavioural change, change management to have a more sustained impact.
particularly in the context of the current model of care. Interview participants identified healthcare professionals
Health workers have limited time with each client. at the forefront of public interaction and as a trusted
point of contact between the public and the healthcare
system.
Barriers to policy formulation and implementation related to
Introducing nutrition curricula in academic setting
medical and healthcare nutrition capacity building
(medical/nursing and several relevant courses at uni-
Participants identified barriers to policy formulation
versity level can be a starting point) is important to
and implementation related to medical and healthcare
make a pool of trained nutrition professionals.
capacity building. One of the identified barriers was time,
namely, that long-term efforts are required to develop Furthermore, survey participants (from NNEdPro)
and implement policy related to nutrition education and felt that nutrition education for healthcare profes-
capacity building and that this may have an influence sionals may improve understanding of the established
on action. Participants reported difficulty in collabora- link between diet and the progression and onset of non-
tion between organisations to sustain efforts as another communicable disease. Participants identified this as key
barrier to policy formulation and implementation in this to enhancing the detection, treatment and prevention of
context. non-communicable disease, and the double burden of
6 Lepre B, et al. bmjnph 2022;0:e000354. doi:10.1136/bmjnph-2021-000354BMJ Nutrition, Prevention & Health
malnutrition. However, some participants identified that recommendation for capacity building, as it requires the
BMJNPH: first published as 10.1136/bmjnph-2021-000354 on 16 February 2022. Downloaded from http://nutrition.bmj.com/ on June 23, 2022 by guest. Protected by copyright.
to meet the complex global health challenges we face application of nutrition knowledge and skills in practice.
today, healthcare professionals need education as support
Efforts have been made to provide in-service training
to meet nutrition goals outlined in the Nutrition Decade.
by multiple stakeholders including Ministry of Health
…looking at WHO documents on health work-
force, the fact that a nutrition-trained and nutrition- Nutrition research
knowledgeable health workforce is indispensable for Participants felt that while nutrition education is an
global health improvement is still not ‘evident’… important tool in building the nutrition capacity of the
NNEdPro participants also provided recommendations medical and healthcare workforce, it must be grounded
for core nutrition competencies, such as the basic prin- in theory and research. Participants expressed the need
ciples of a healthy diet, as defined by the WHO and as for nutrition research capacity, as necessary to further
recommended by national food-based dietary guidelines, identify and clarify problems with nutrition care, delivery
in addition to motivational interview techniques, to assist and education so that solutions can be addressed, encour-
in behavioural change. Onward referral was also identi- aging grassroots efforts.
fied as an important nutrition competency, particularly WHO has maintained a rigorous approach to
for doctors, who NNEdPro members acknowledged as evidence-based nutrition in all of its training policies.
well placed to initiate and support nutrition care. Research is regularly undertaken by WHO collaborat-
None or very few of them [doctors] (nurses too) are ing centres.
trained in nutrition counselling. But these are the
techniques that need training to acquire required
Key themes and examples from facilitated discussions on next
skills to practice in day-
to-
day care—both curative
steps related to nutrition capacity building
and preventive.
Five key themes were identified from intermediate outputs,
Furthermore, participants identified a person- centred namely, presentations related to global nutrition capacity:
approach as key to nutrition care in line with FAO recom- (1) Nutrition capacities—A competent and motivated
mendations identified in the document analysis above. Partic- health workforce is key to progress towards ending the
ipants suggested the integration of nutrition competencies double burden of malnutrition, (2) Diet quality and food
related to effective referral and follow-up with patients as an systems—Food systems transformation is key to improve-
important aspect of person-centred care. ments in nutrition outcomes, (3) Indicators to monitor
progress—The density of nutrition professionals is relevant
Client focused and appropriate to the context, in-
to the nutrition capacity and progress within countries, (4)
cluding based on nutritional assessment of the client
Scalable nutrition education interventions for sustainable
as appropriate
change and (5) The role of voluntary nutrition networks.
Lastly, participants suggested nutrition education These themes are discussed in detail below and form part of
include leadership competencies in order to equip the recommendations of this review.
medical and healthcare professionals with the knowl-
edge, skills and confidence to advocate for nutrition in Nutrition capacities: a competent and motivated health workforce
a number of capacities. This may include discussions is key to progress towards ending the double burden of
with their patients, at the local level to advocate for and malnutrition
support peer engagement through education, research At the NNEdPro fifth International Summit on Medical
and practice and at the local and national level to influ- and Public Health Nutrition Education and Research, Dr
ence policy and strategy in the delivery of public health Francesco Branca, Director of the WHO NFS, reiterated
priorities. Participants also identified a need for health- the need for health practitioners to advocate for healthy
care professionals to act as nutrition champions at the diets in a collective effort to reduce malnutrition in all
national level, to influence government policy, engage its forms.41 Ms Lina Mahy, Technical Officer in the WHO
with stakeholders and establish international consensus. NFS, exposed low existing coverage of nutrition actions
This may suggest that healthcare professionals have an through the health system. Nutrition capacity, including a
un-filled role in nutrition advocacy, an important recom- well trained and motivated health workforce is one of the
mendation supported by policy guidance in this analysis. six pillars of an effective health system and is essential to
address all forms of malnutrition.42 43 There remains an
Leadership: Health workers need to liaise with com-
urgent need to scale and improve the nutrition capacity
munity leaders, and to advocate to them to make
of the health workforce, including medical doctors and
their communities nutrition friendly
nurses, who are well placed to provide dietary advice, by
Participants saw programmes of continuing educa- leveraging existing nutrition professionals, such as dieti-
tion in nutrition as a short-term solution, rather than an tians and public health nutritionists.
ongoing method of capacity development. ‘On- the-
job’ ICN2 yielded the Rome Declaration on Nutrition,
sessions were identified as a more suitable education-based encompassing 10 political commitments for effective
Lepre B, et al. bmjnph 2022;0:e000354. doi:10.1136/bmjnph-2021-000354 7 BMJ Nutrition, Prevention & Health
and co-ordinated action to achieve improved nutrition syndrome. These findings led to the establishment of the
BMJNPH: first published as 10.1136/bmjnph-2021-000354 on 16 February 2022. Downloaded from http://nutrition.bmj.com/ on June 23, 2022 by guest. Protected by copyright.
capacity and a framework of recommendations to oper- MTK project, which aims to provide a scalable nutrition
ationalise political commitments.7 Ms Mahy presented intervention to improve the nutrition knowledge and
key ICN2 recommendations to ‘improve nutrition by capacity of the population through demonstration by
strengthening human and institutional capacities to trained nutrition educators for development of a sustain-
address all forms of malnutrition…’.41 The Rome Declara- able model.45 The MTK initiative is based on a ‘See one,
tion highlights the need for improved nutrition capacity do one and teach one’ model, which underscores the
of not only the health workforce, but of other commu- transfer of nutrition knowledge between community
nity members well-placed to provide nutrition education, members, to empower healthy and affordable dietary
such as teachers and social workers.7 choices. Increased investment in some of the most
marginalised in society can have an upward social and
Diet quality and food systems: food systems transformation is key health impact. Overall improvements in clinical status
to improvements in nutrition outcomes and self-perceived nutrition knowledge were seen as a
Diets are shaped by the food environment and food envi- result of the MTK educational intervention—a promising
ronments are shaped by food systems.35 39 Consumer nutri- result.45
tion behaviour has a flow-on effect on health outcomes SR highlighted the need for a strengthened architec-
and the subsequent social, economic and environmental ture of nutrition education for health professionals, in
impacts of such outcomes. Ms Mahy outlined the need line with the Nutrition Decade.41 A recent synthesis of
for political, programme and institutional action at the UK medical education identified a need for enhanced
food supply, food environment and consumer behaviour medical nutrition training, particularly the application of
stages of the food system model.41 nutrition to a clinical context.44 Given continued deficits
in healthcare professional nutrition competency, there is
Indicators to monitor progress: the density of nutrition a need for engaging, scalable training-based solutions to
professionals is relevant to the nutrition capacity and progress increase capacity, such as the MTK initiative and the Nutri-
within countries tion Education Policy in Healthcare Practice (NEPHELP)
Nutrition data and indicators are central to effective project developed by NNEdPro.45 46 See online supple-
nutrition surveillance, policy making and accountability. mental file 1 for an infographic summarising findings
Ms Mahy presented the twenty primary outcomes, inter- from Time for Nutrition in Medical Education.44
mediate, process and policy environment and capacity
indicators encompassed in the WHO Global Nutrition The role of voluntary nutrition networks
Monitoring Framework —Operational Guidance for Given the recommendations previously mentioned,
Tracking Progress in Meeting Targets for 2025.27 41 Nutri- efforts to improve health through action on nutrition
tion professionals are well placed to provide dietary advice require integrative strategies that evaluate the impact of
including evidence-based health and nutrition informa- diets on communities and individuals. The potential of
tion. Therefore, the density of nutrition professionals policy strategies to improve healthy food environments
was highlighted as an important indicator to measure the and human diet is recognised, but since every environ-
political economy and nutrition capacity and importantly, ment is different, a range of approaches is adequate for
progress within a country. Recommendations to improve distinctive realities. Regional or national groups that
capacity development for nutrition include increasing the study and focus on nutrition related problematics should
number of health professionals competent in nutrition. be centres of dissemination of evidence, offers and oppor-
Few countries provide nutrition education as part of tunities, allowing policies and action to focus on specific
higher education. Time dedicated to nutrition in tertiary problem-solving and needs.
curricula is lacking and therefore the quality of nutrition Working on the best interest of regional networks
education may be compromised.44 High-quality nutrition in nutrition means planning a wide- ranging web that
education, such as integrated nutrition training for front- connects different agents in nutrition that transfer knowl-
line health workers, is essential to improve capacity for edge regarding needs, ideas and locally tailored strategies.
nutrition and address all forms of malnutrition.24 The integration of holistic practices in local networks and
systems concerning nutrition allows the development of
Scalable nutrition education interventions for sustainable change action and should start with transdisciplinary evidence-
Dr Luke Buckner, NNEdPro UK- India Scientific Lead based research. After the development and implemen-
and Nutrition Implementation Coalition Co-Convener, tation of action, it is crucial to evaluate outcomes to
provided a global perspective on data- driven insights understand limitations, feasibility and benefits as well as
from outputs related to TIGR2ESS, Cambridge Global measure the impact of these approaches in the multiple
Food Security, Mobile Teaching Kitchens (MTK) and regional and national contexts. As an example, NNEdPro
India.41 Landscaping activities undertaken in Kolkata, convenes regional networks across six continents which
India in 2015 revealed a double burden of malnutrition, provide a primary pathway through which to implement
characterised by undernutrition, wasting and stunting, as the recommendations below in different regions, each
well as pockets of the community living with metabolic with customised and adequate aims and purposes.47
8 Lepre B, et al. bmjnph 2022;0:e000354. doi:10.1136/bmjnph-2021-000354BMJ Nutrition, Prevention & Health
DISCUSSION nutrition competencies identified in the literature
BMJNPH: first published as 10.1136/bmjnph-2021-000354 on 16 February 2022. Downloaded from http://nutrition.bmj.com/ on June 23, 2022 by guest. Protected by copyright.
The six Action Areas of the Work Programme of the Nutri- include awareness of how sociocultural determinants of
tion Decade are interlinked and call for sustainable, resil- health may affect nutrition behaviour and health status,
ient food systems for healthy diets, aligned health systems and the ability to work effectively in a multidisciplinary
to support the universal delivery of essential nutrition team to provide nutrition care.53 Standardised nutrition
actions, increased investment in nutrition and strength- education might address variability in nutrition education
ened governance for nutrition.5 This review reiterates for health professionals and provides incentive for the
the importance of medical and healthcare professional integration of nutrition competencies into curricula. The
nutrition capacity and synthesises key recommendations integration of innovative, skills-based curriculum initia-
to improve nutrition education and capacity based on tives is required to support the development of nutrition
policy guidance from the WHO, FAO and UNSCN, inter- competence. For example, culinary skills training and
views with participants from the WHO NFS and NNEdPro interprofessional education have been shown to promote
Global Centre for Nutrition and Health and key outputs team-based care and lead to significant changes in health
(ie, presentations) related to global nutrition capacity. professionals nutrition knowledge, personal health habits
The need for nutrition capacity building at the indi- and confidence to provide nutrition advice.54 55 The need
vidual, organisational and systemic levels is clear and key to establish global consensus on nutrition competen-
recommendations are discussed below. cies for medical and healthcare professionals has been
The third action area of the Work Programme of the echoed in the literature for decades and further progress
Nutrition Decade, social protection and nutrition educa- is required.17 50
tion, directly relates to nutrition education, based on Nutrition capacity development must be supported by
ICN2 recommendations.5 24 Furthermore, in the Sixth the expansion and dissemination of open access nutri-
Report on the World Nutrition Situation, the UNSCN tion resources and evidence for the medical and health
concludes that ‘for all populations, [nutrition] education workforce. Modern technology (ie, technology- based
and social marketing are crucial components of national, education and resources) can reduce the unavoidable
municipal and community efforts for sustained improve- costs of quality education. For example, the eNutrition
ments in food and nutrition security…’.48 Knowledge and Academy was created in 2014 by a consortium of interna-
education are key to lifestyle and behavioural change and tional organisations and offers free e-learning nutrition
health professionals are well-placed to provide dietary modules for healthcare professionals.56 Similarly, the
advice to support healthy choices.5 Despite this, only 23 of WHO eLENA, an online library of guidelines for nutri-
126 countries (18%) which reported nutrition-focussed tion interventions, aims to assist countries in successfully
professionals as part of their workforce had the recom- implementing and scaling up nutrition interventions by
mended density (10 nutrition professionals per 100 000 providing resources which guide evidence-based policy
population).26 This is of concern given the indicator is development and programme design.25 The World Food
based on recognition that a sufficient workforce with Programme host an open access learning platform called
adequate nutrition capacity will lead to better outcomes nutx, which includes self-paced e-learning courses, inter-
for country-specific nutrition and health outcomes.26 active tests and exercises.57 The continued expansion
Furthermore, nutrition professionals play a central role and dissemination of evidence-based nutrition resources
in training other health professionals to plan and deliver and knowledge hubs is recommended to drive improve-
nutrition interventions. The nutrition competency of ments in the nutrition capacity of the medical and health
the health workforce has been previously established as workforce and country-level efforts to develop supportive
insufficient and variable,49 50 despite international efforts policy and implement and scale nutrition interventions.
to improve nutrition education for health professionals, The above efforts related to nutrition education
such as the Nutrition Academic Award, developed by the and capacity must continue to be grounded in quality
National Heart, Lung and Blood Institute.51 One recom- research supported by government and policy. Innovative
mendation was the establishment of an interdisciplinary nutrition research provides a fundamental evidence base
competency- based nutrition curriculum for health for nutrition education, guidelines and policy develop-
professionals. The use of a competency-based approach ment. The 2020–2030 Strategic Plan for National Insti-
in improving nutrition education for the medical profes- tutes of Health (NIH) Nutrition Research confirms the
sion has been previously established52 and has been role of nutrition research in efforts to improve popula-
shown to increase a clinician’s ability to integrate nutri- tion health and is organised around the vision of preci-
tion into patient care.50 The cross-cutting nature of nutri- sion nutrition.58 There is also current funding provided
tion has the potential to upskill across multiple aspects for research efforts related to the microbiome, digital
of broad health promotion, including both skills and approaches to dietary assessment and the evolution of
capacity building, and therefore, to have continued and artificial intelligence. These efforts underpin the need
wide-ranging impact. Nutrition competencies identified for the health workforce to be competent in nutrition
as core to all health professionals in this paper included given the potential downstream impact of nutrition
the principles of a healthy diet, motivational interviewing, research on healthcare practice. Political entities must
onward referral and leadership. Other cross- cutting commit to a supportive environment for the delivery and
Lepre B, et al. bmjnph 2022;0:e000354. doi:10.1136/bmjnph-2021-000354 9 BMJ Nutrition, Prevention & Health
implementation of nutrition policy and programmes, Global nutrition surveillance and monitoring systems
BMJNPH: first published as 10.1136/bmjnph-2021-000354 on 16 February 2022. Downloaded from http://nutrition.bmj.com/ on June 23, 2022 by guest. Protected by copyright.
such as pledges from local governments to prioritise must be in place to evaluate the impact of changes in
nutrition education for healthcare professionals. Nomi- policy and education. This is a call to action for Govern-
nation of a central coordinator for nutrition education ment to pledge to prioritise nutrition education and
initiatives will reduce difficulty in collaboration between capacity building, as a platform for improved health and
organisations to implement and sustain efforts as iden- well-being. Eliminating malnutrition in all its forms is key
tified as a barrier in this study. This must be matched to progress towards the Sustainable Development Goals.
with increased investment in nutrition, such as funding
for provision of physical infrastructure and innovative
nutrition education curriculum initiatives for healthcare RECOMMENDATIONS
professional nutrition capacity building. 1. Establishment of a national curriculum for nutrition
Finally, improved global data collections mechanisms education across all healthcare sectors, including the
and validated indicators are essential to assess and development and expansion of on-line resources.
measure capacity and progress. FAO states the impor- 2. Individual and government pledge for adopting nutri-
tance of developing ‘countries' capacities to evaluate tion education in community and healthcare as a pri-
and monitor nutrition situations, analyse options, and ority, including establishment of frameworks for best
implement agricultural policies and programmes that practice.
impact positively on nutrition.’36 The Global Nutrition 3. Improved global data collections mechanisms and val-
Monitoring Framework recommends trained nutrition idated indicators to assess and measure capacity and
professional density as a core policy environment and progress, such as the nutrition professionals density
capacity indicator, which can be used to assess country- Indicator.
level capacity to design and implement nutrition policy
and programmes, as mentioned earlier. Validation of the FUTURE VISION
indicator has shown it can predict important maternal, Following a call to action for improved nutrition educa-
infant and young child nutrition outcomes.26 Nutrition tion for health professionals, NNEdPro developed
professional density was one of four indicators deferred NEPHELP, which aims to develop a training programme
for reporting by the WHO until 2018, as Member States for junior doctors, primary care physicians and allied
were unclear how to report these indicators. This review healthcare professionals in nutrition- related problems,
recommends further clarification on the definition of nutrition interventions and scope of practice including
‘nutrition professional’ due to differences in professional appropriate onward referral to a specialist, such as a regis-
education and accreditation internationally. Countries tered dietitian or nutritionist. More broadly, NEPHELP is
are encouraged to implement registration and accredi- a bespoke, interdisciplinary, sustainable nutrition educa-
tation systems for nutrition professional education to tion intervention to improve the capacity of the health
ensure quality training and professional competence. workforce.46
In a joint initiative to support nutrition education and
Strengths and limitations capacity, NNEdPro and LGC developed the International
This paper provides a critical synthesis of capacity- Knowledge Application Network Hub in Nutrition 2025
building efforts with regards to nutrition education (iKANN).59 iKANN is an open access online portal of
for medical and healthcare professionals and provides published evidence in nutrition, encompassing evidence
recommendations to enhance efforts, however, needs to syntheses, raw data and meta data, evidence-based guide-
be considered in the context of its limitations. The role lines and e- learning to support workforce nutrition
of nutrition professionals, namely nutritionist-dietitians, capacity development. The platform was launched on
may vary internationally and particularly between low- 26 September 2020 at the sixth International Summit
income to middle- income countries and high- income on Medical and Public Health Nutrition Education &
countries. This may have implications for the generalis- Research and can be found at www.ikann.global.59 iKANN
ability of the recommendations provided, particularly has been established with over 10 regional network hubs
with regard to nutrition education needs. positioned worldwide for scalability. A key function of
iKANN is to support high quality, scalable nutrition
education and training, to improve knowledge applica-
tion globally.
CONCLUSION
Nutrition data collection, policy, education and imple- Twitter Lauren Ball @laurenball01
mentation of change is likely to improve the nutrition Acknowledgements We would like to thank the WHO Department of Nutrition
behaviour of the wider community, which will in turn and Food Safety, especially, Francesco Branca (Director), Felicetta Catanzaro, Kaia
have population health and economic benefits. None of Engesveen, Fabienne Maertens, Lina Mahy, Thahira Mustafa, Kuntal Saha, Simona
Seravesi & Juan Pablo Pena-Rosas. We would like to acknowledge the support
these benefits are possible without the described actions
of WHO Chief Scientist, Soumya Swaminathan for including feedback in the pre-
to build the nutrition capacity of the medical and health final presentation of this work. We also acknowledge additional WHO colleagues
workforce. including Diana Estevez for helpful comments and Christine Yvonne Tretter from the
10 Lepre B, et al. bmjnph 2022;0:e000354. doi:10.1136/bmjnph-2021-000354You can also read