Health support planning: Anaphylaxis and severe allergies in education and care
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Procedure
Health support planning:
Anaphylaxis and severe allergies in education
and care
Please note this procedure is mandatory and staff are required to adhere to the content.
Summary
This document is a practical direction for all staff working in education and care to plan and manage for
children and young people with anaphylaxis and severe allergies.
Table 1 - Document details
Publication date August 2018
File number 18/07540
Related legislation Code of Practice First Aid in the Workplace 2012
Work Health and Safety Act 2012
State Records Act 1997
Disability Discrimination Act 1992
Disability Standards for Education 2005
National Disability Insurance Scheme Act 2013
Education and Early Childhood Services (Registration and
Standards) Act 2011
Education Regulations 2012
Education and Care Services National Law 2010
Education and Care Services National Regulations
and within those regulations in particular:
Regulation 12(b)(i)
Regulation 90(1)(a)
Regulation 91
Regulation 92
Regulation 94(1)
Regulation 95
Regulation 96
Regulation 136(1), (2) and (3)
Regulation 153(1)(j)
Regulation 162(c), (d) and (e)
Regulation 168(2)
1 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018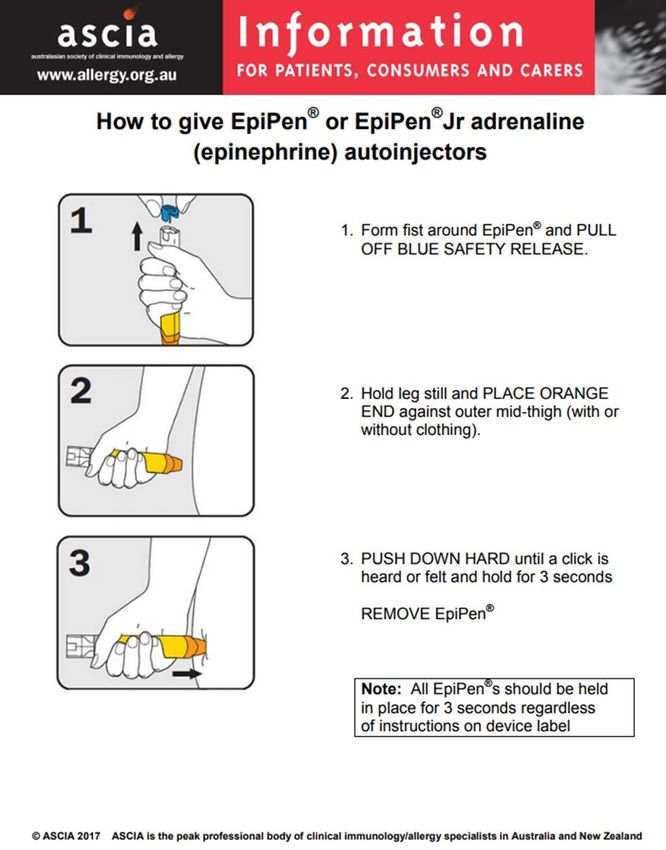
Regulation 173(2)(f)
Regulation 177(1)(c)
Regulation 183(2)(a), (b) and (c)
Related policies, Duty of Care policy
procedures, guidelines,
Work Health and Safety policy
standards, frameworks
First Aid and Infection Control Standard
Direct Health Support of People with Disability (DCSI Policy)
Medication management in education and care procedure
Version 1.0
Replaces Anaphylaxis in education and children's services, revised edition
2012
Anaphylaxis management in education and care (2014 FAQs)
Policy officer (position) Health Support Planning Policy Officer
Policy officer (phone) 8226 1769
Policy sponsor (position) Director, Disability Policy and Programs
Executive director Executive Director, Early Years and Child Development
responsible
Applies to All education and care staff
Key words adrenaline, allergy, anaphylaxis, duty of care, epipen, first aid,
guidelines, health support, medication, procedure, training, HSP120,
HSP151, HSP154, HSP321, HSP322, HSP323
Status Approved
Approved by Senior Executive Group
Approval date 10 August 2018
Review date 10 August 2019
2 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018
Table 2 - Revision record
Date Version Revision description
Pending 1.0 New procedure developed incorporating information from
the former ‘Guidelines for anaphylaxis in education and
children’s services’ revised edition 2012 and
‘anaphylaxis management in education and care’ 2014
FAQs.
The national law is clearly articulated.
This procedure clearly explains the management of
children and young people diagnosed with severe
allergies and the emergency response for any person
that may experience an episode of anaphylaxis while in
an education and care setting.
This procedure includes guidelines for the provision and
management of general use adrenaline autoinjectors at
all education and care services.
3 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018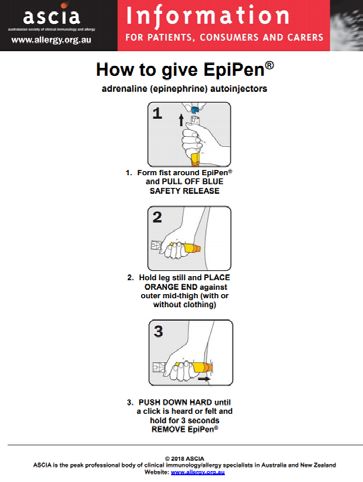
Table of Contents
1. Title..............................................................................................................................................................5
2. Purpose .......................................................................................................................................................5
3. Scope ..........................................................................................................................................................5
4. Procedure detail ...........................................................................................................................................5
4.1 Legislative requirements .........................................................................................................................5
4.2 Aboriginal cultural context statement.......................................................................................................6
4.3 Cultural diversity .....................................................................................................................................7
4.4 Allergic reactions and anaphylaxis background .......................................................................................7
4.5 Signs and symptoms of allergic reaction including anaphylaxis ...............................................................8
4.6 Treatment for anaphylaxis ......................................................................................................................8
4.7 Mental health and anaphylaxis..............................................................................................................10
4.8 ASCIA Action Plans, Health Care Plans and Health Support Agreement ..............................................10
4.9 Adrenaline autoinjector (Epipen®) ........................................................................................................14
4.10 Planning and post-incident management.............................................................................................19
4.11 Training and education .......................................................................................................................21
4.12 Risk management...............................................................................................................................22
5. Roles and responsibilities ...........................................................................................................................26
6. Monitoring, evaluation and review...............................................................................................................28
7. Consultation ...............................................................................................................................................28
8. Definitions and abbreviations......................................................................................................................29
9. Supporting documents................................................................................................................................31
10. References.................................................................................................................................................32
Appendix ...............................................................................................................................................................33
4 | Health support planning: Anaphylaxis and severe allergies in education and care | August 20181. Title
Health support planning: Anaphylaxis and severe allergies in education and care.
2. Purpose
This procedure describes:
• the roles and responsibilities of education and care staff for managing the health support needs
both proactively and reactively for children and young people who suffer from anaphylaxis and
severe allergies
• signs and symptoms of mild to moderate allergic reactions and of anaphylaxis
• the emergency response for any person experiencing an episode of anaphylaxis while in an
education or care setting
• the requirement for all government preschools and schools to maintain at least one general use
adrenaline autoinjector on site
• education and training for anaphylaxis and severe allergies
• risk minimisation strategies for children and young people suffering from severe allergies and/or
anaphylaxis
3. Scope
This procedure applies to educators, early childhood development specialists, Principals, Directors and
education support staff working in education and care.
In addition to this procedure, some children and young people may require support from the Access
Assistant Program (AAP) or Registered Nurse (RN) Delegation of Care Program where they have
invasive or complex healthcare needs, uncertain or changing health. The Access Assistant Program
Flowchart or RN Delegation of Care Service Provider Toolkit support education and care staff to
determine when additional supports are required.
This procedure applies from the time a child or young person is enrolled until they leave the education or
care service.
4. Procedure detail
4.1 Legislative requirements
Education and care staff have a duty of care and safe work obligations (see Duty of Care Policy).
The education and care service and its staff have a duty of care to take reasonable steps to be
informed as to whether a child or young person has a health condition and to take reasonable
precautions during the period of care. The specific steps taken to minimise risk depend on the
health condition, age and stage of development of the child or young person, triggers and the
circumstances of the environment.
Pursuant to Regulation 136(1) and (2) of the Education and Care Services National Regulations
2014 education and care settings are required to have at least one staff member who is in
attendance at a site and is immediately available in an emergency who holds a current approved
first aid qualification, together with at least one staff member who is in attendance at a site and is
immediately available in an emergency who has completed a current approved anaphylaxis
management training course. It is sufficient to satisfy requirements where the same person holds
both qualifications.
The Department for Education has an expectation that all staff have up to date first aid training.
5 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018In accordance with the Department for Education School Transport Policy there is no requirement
for drivers of departmentally owned and operated buses to be trained in first aid procedures and
would therefore not be required to administer emergency response medications. Drivers of
departmental owned buses must use discretion in an emergency situation, but on no account leave
children unsupervised in such a situation.
All staff working with a child or young person who is known to be at risk of anaphylaxis should
complete the approved anaphylaxis management training course in conjunction with practical
training using an adrenaline autoinjector training device.
The Australasian Society of Clinical Immunology and Allergy (ASCIA) offer a free e-training course
on anaphylaxis management in education and care services. Education and care staff should
complete this course every three years and have regular practical training using an adrenaline
autoinjector training device.
The Director or Principal must ensure appropriate support to enable all children and young people
to participate in and benefit from their educational experience, as per requirements of the Disability
Discrimination Act 1992 (DDA) and Disability Standards for Education 2005 (DSE). This includes
the allocation of staff who are appropriately trained and able to provide the required level of
support and supervision. For example, a child or young person cannot be excluded from an
education or care service because they require health support assistance and staff are
uncomfortable or unqualified to provide assistance.
4.2 Aboriginal cultural context statement
The Department for Education acknowledge and give thanks to the members of the Women’s and
Children’s Health Network Aboriginal Focus Group for their time and commitment to developing
this generic Aboriginal cultural context statement for the health support planning procedures.
Note: The term ‘Aboriginal’ is used to refer to people who identify as Aboriginal, Torres Strait
Islanders, or both Aboriginal and Torres Strait Islander. This is done because the people
indigenous to South Australia are Aboriginal and we respect that many Aboriginal people prefer the
term ‘Aboriginal’. We also acknowledge and respect that many Aboriginal South Australians prefer
to be known by their specific language group(s).
Australian Aboriginal culture is the oldest living culture in the world, yet Aboriginal people currently
experience the poorest health and education outcomes when compared to non-Aboriginal
Australians. [The National Aboriginal and Torres Strait Islander Social Survey 2014-2015 shows
poor education and literacy are linked to poor health status.]
The cumulative effects of forced removal of Aboriginal children, poverty, exposure to violence,
historical and transgenerational trauma, the ongoing effects of past and present systemic racism,
culturally unsafe and discriminatory services are all major contributors to the disparities in
Aboriginal education outcomes.
To achieve the best Aboriginal education outcomes, education and care services have a
responsibility to provide a culturally safe environment allowing Aboriginal children and families to
draw strength in their identity, community and culture.
Aboriginal children are born into strong kinship structures where roles and responsibilities are
integral and woven into the social fabric of Aboriginal societies. The primary caregiver for
Aboriginal children is not always the parent. Education and care staff should consider engaging
members of the extended family in the absence of parents and legal guardians where appropriate.
Education and care staff can secure positive long term education and wellbeing outcomes for our
Aboriginal children and young people by making well informed decisions in consultation with
families, based on cultural considerations.
6 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018Health support agreements must be developed in partnership with parents. The opportunity to
identify cultural needs is paramount. Education and care staff should be aware that parents may
request the input of Aboriginal Community Education Officers (ACEOs) or Aboriginal Health
Workers (AHW) in the development of their child’s Health Support Agreements. The use of an
Aboriginal languages interpreter or translator should also be considered.
4.3 Cultural diversity
Cultural diversity refers to the differences between human communities based on differences in
their ideologies, values, beliefs, norms, customs, meanings and ways of life. These differences are
expressed and exemplified in social practices, attitudes and values, family interactions and
expectations, values concerning education, ways of defining and treating health (physical and
mental), business and management behaviours and practices, political practices and interpersonal
relations.
Education and care services have a responsibility to provide a culturally safe environment through
fostering awareness of cultural diversity and implementing culturally inclusive practices.
To support the development of culturally valid health support planning in education and care
settings, consideration must be given to the political, cultural, spiritual, emotional, environmental,
structural, economic and biological factors impacting on the wellbeing of all children and young
people. The development of health support agreements must be completed in consultation with
parents and legal guardians; with an assurance that parents and legal guardians understand the
content and the underlying values of the Australian context as well as have the opportunity to
discuss their cultural perspective and needs.
The Department for Education English as an Additional Language or Dialect (EALD) program
supports children and young people, and their families, from culturally and linguistically diverse
backgrounds, and provides access to interpreter services and Community Liaison Officers (CLOs).
Family members and friends should not be used as interpreters.
The Preschool Bilingual program may be able to assist preschools to access interpreter services to
support children and their families from culturally and linguistically diverse backgrounds.
4.4 Allergic reactions and anaphylaxis background
An allergic reaction occurs when the immune system reacts to substances in the environment
that are harmless to most people; known as ‘allergens’ and found in foods, insects, pollen, mould,
dust mites and some medications. Most allergic reactions are mild and do not involve the airways
or circulation.
Anaphylaxis is a potentially life threatening, severe allergic reaction and should always be treated
as a medical emergency. Not all people with allergies are at risk of anaphylaxis. Anaphylaxis
involves the obstruction of oxygen (air) to the airway and lungs and/or the heart, brain and blood
vessels.
Research shows an increase of 10% per year in hospital admissions for food-induced
anaphylaxis between 1997 and 2013 1, with the majority of food-induced anaphylaxis admissions
occurring in children aged less than 5, and fatalities as a result occurring between 8 and 35 years
of age. Sting-induced anaphylaxis hospital admissions peak between 5 and 9 years of age, with
no fatalities within this age group.2
1
http://allergenbureau.net/food-related-anaphylaxis-fatalities-rise-australia/
2
https://www.ncbi.nlm.nih.gov/pubmed/19117599
7 | Health support planning: Anaphylaxis and severe allergies in education and care | August 20184.5 Signs and symptoms of allergic reaction including anaphylaxis
The first symptoms of an allergic reaction are often skin rash or facial swelling, however this is not
always the case. Early symptoms to food-based reactions may also include abdominal pain and/or
vomiting.
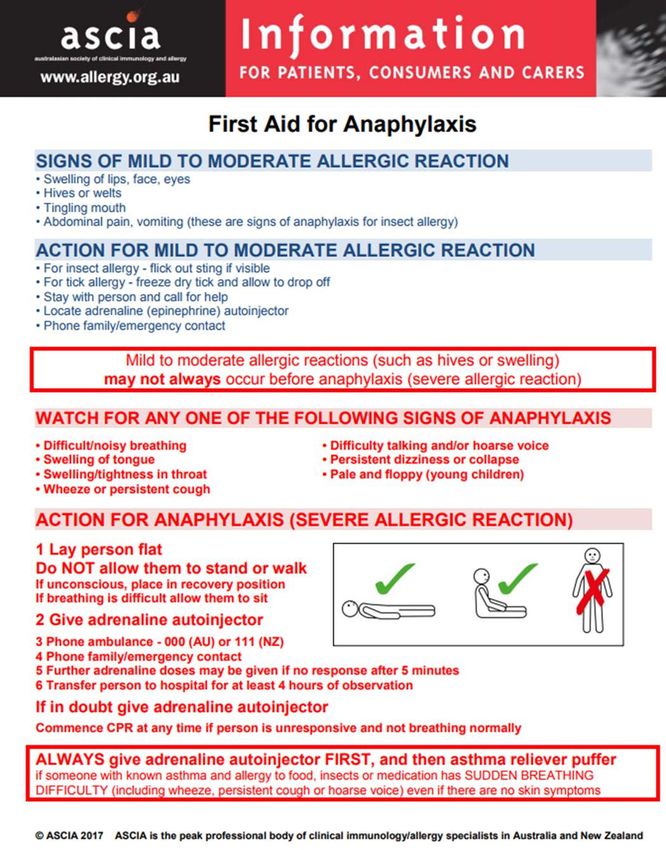
Mild to moderate allergic reactions (hives/swelling) may not always occur before anaphylaxis
(severe allergic reaction).
Anaphylaxis may present with symptoms of breathing difficulty, cough or wheeze. If the same child
or young person has asthma then it can be difficult to determine if this is anaphylaxis or asthma.
SIGNS OF A MILD TO MODERATE ALLERGIC REACTION AND ANAPHYLAXIS
Mild to moderate allergic reaction Anaphylaxis (Severe allergic reaction)
• Tingling mouth • Difficult/noisy breathing
• Swelling of lips, face, eyes • Swelling of tongue
• Hives or welts • Swelling/tightness in throat.
• Abdominal pain, vomiting (these are • Difficulty talking and/or hoarse voice
signs of anaphylaxis when the trigger
• Wheeze or persistent cough
is insect venom)
• Persistent dizziness or collapse
• Pale and floppy appearance (young children)
If in doubt give adrenaline autoinjector
Always give adrenaline autoinjector FIRST and then asthma reliever puffer if someone with
known asthma and allergy to food, insects or medication has SUDDEN BREATHING
DIFFICULTY even if there are no skin symptoms.
4.6 Treatment for anaphylaxis
All education and care staff are required to provide first aid measures following any relevant ASCIA
action plan or health support agreement and contacting emergency services.
4.6.1 First aid treatment for an allergic reaction including anaphylaxis
• Lay person flat. Do not allow them to stand or walk.
If breathing is more difficult lying down allow them
to sit. If unconscious place in recovery position
• Ensure the child or young person is no longer
exposed to the allergen or trigger
• Administer adrenaline autoinjector into the muscle
of the outer thigh (when using an EpiPen® hold in
place for 3 seconds after the injection)
• Phone ambulance 000
• Phone family/emergency contact
• Further adrenaline doses may be given if no
response after 5 minutes, if another adrenaline
autoinjector is available
• Commence cardiopulmonary resuscitation (CPR)
at any time if person is unresponsive and not
breathing normally
8 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018• In all cases of anaphylaxis the care for the child or young person must be transferred
to the ambulance officer for admitting to hospital for at least 4 hours of observation
• The used adrenaline autoinjector should be handed to the ambulance officer, and they
should be advised of the time of administration
4.6.2 Who can provide first aid for anaphylaxis by administration of an adrenaline
autoinjector?
Adrenaline autoinjectors have been designed for use by anyone in an emergency,
including people who are not medically trained, such as a friend, teacher, childcare
worker, parent, passer-by, or the individual with anaphylaxis themselves (if they are
capable and old enough). Instructions are shown on the label of each device and on the
ASCIA action plan for anaphylaxis.
4.6.3 Using an adrenaline autoinjector (eg EpiPen®, EpiPen®Jr)
• Give the injection in to the child or young person’s
outer mid-thigh (intra-muscular). You can do this
through clothing taking care to avoid seams and
pockets.
• There is no need to swab the skin
• When using an EpiPen® hold the autoinjector in
place for 3 seconds after the injection
• Do not rub or massage the injection site
• An Epipen® has an orange needle shield; after use
the needle is retracted back into the device, no
needle is exposed
4.6.4 Self-administration of an adrenaline autoinjector
If a child or young person self-administers their own
adrenaline autoinjector:
• A staff member must supervise and monitor the child or young person at all times
• Follow instruction in section 4.6.1 ‘First aid treatment for an allergic reaction
including anaphylaxis’
The decision as to whether a child or young person can carry their own and/or self-
administer an adrenaline autoinjector in an education or care service can be made by
using the carrying and/or self-administration of medication decision making tool, in
consultation with the child or young person and parent or legal guardian.
The Principal or Director (or nominated delegate) will determine if a child or young person
is capable of assuming the responsibilities of carrying, self-administered and/or disposal
of nominated medication(s); and will determine if notification, supervision and
documentation of the medication administration is required.
Some children and young people may choose to self-administer as they recognise the
early stages of an anaphylaxis reaction but will most likely require assistance if their
condition deteriorates.
Staff cannot expect children and young people experiencing anaphylaxis to self-
administer adrenaline via an adrenaline autoinjector. Individuals experiencing anaphylaxis
can become confused and the risk of error in administration is high. In these
circumstances education and care staff need to be prepared to administer the adrenaline
autoinjector.
9 | Health support planning: Anaphylaxis and severe allergies in education and care | August 20184.6.5 Potential for a delayed response to an emergency
Anaphylaxis management can be more difficult in remote and rural sites where ambulance
bases are many kilometres away, or are operated by volunteer services.
Under these circumstances parents or legal guardians may choose to provide a second
adrenaline autoinjector that travels between home and the site, in addition to the
adrenaline autoinjector that remains at the education or care service.
4.7 Mental health and anaphylaxis
Children and young people who have anaphylaxis, and their parents and legal guardians, may be
anxious about their allergies3.
In a small number of cases anxiety may become debilitating, preventing the child or young person
from engaging in daily activities at home, school, or socially (ie a child or young person with an
insect sting allergy might completely avoid the outdoors; or where there is a severe food allergy
might follow an overly restrictive diet or avoid friends’ homes for fear of encountering an allergen; a
young child with anaphylaxis might refuse to stay at school without a parent for fear of having a
reaction there).
Where there are recurrent episodes of anxiety related to anaphylaxis or severe allergies a health
support agreement should be developed (or updated) to reflect strategies to reduce and manage
the anxiety. It is important to return the child or young person quickly to class activities to distract
the focus from remaining symptoms and prevent reinforcement of avoidant behaviours that may
exacerbate anxiety. Calling parents or legal guardians to remove the child or young person from
the education or care service may promote school avoidance.
High levels of anxiety may often be seen in parents and legal guardians of children and young
people with severe allergies, particularly those with nut allergies 4 . Prescribing adrenaline
autoinjectors has been associated with a reduction in anxiety for parents and legal guardians.
Stress and anxiety for children and young people with severe allergies, and their parents or legal
guardians, can significantly increase when there is a change in lifestyle such as starting (or
changing) education or care service.
There are four main causes of stress and anxiety relating to anaphylaxis for parents and legal
guardians5:
• the potential seriousness of anaphylaxis (life-threatening)
• the inconvenience and changes in lifestyle (difficulty with shopping, reading labels,
constantly having to explain the allergy)
• feeling isolated and that others don’t understand
• letting go (trusting the child or young person and others to deal with the allergy)
Regular and ongoing communication with parents and legal guardians is important to reassure
them of the strategies in place to manage the child or young person’s allergies, with an emphasis
on the ability of the education or care service to ensure a safe environment.
4.8 ASCIA Action Plans, Health Care Plans and Health Support
Agreement
The Australasian Society of Clinical Immunology and Allergy (ASCIA) have developed Action Plans
to provide instructions for first aid treatment of anaphylaxis to be delivered by people without any
3
https://www.hindawi.com/journals/ja/2012/316296/
4
http://onlinelibrary.wiley.com/doi/10.1034/j.1399-3038.2003.00072.x/abstract;jsessionid=685123D861FB4C0826013399132E77A4.f02t02
5
http://www.aaia.ca/en/living_with_anaphylaxis_handling_the_stress.htm
10 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018special medical training. ASCIA action plans must be completed by the treating health
professional.
There are two types of Action Plans for Anaphylaxis and a third Action Plan for Allergic Reactions.
• ASCIA general action plan for anaphylaxis (‘orange plan’)
o Does not contain any personal information; for management of an anaphylaxis
incident using the general use EpiPen®
• ASCIA personal action plan for anaphylaxis (‘red plan’)
o Contains personal information and a photo for individuals that have been
prescribed a personal use EpiPen®
• ASCIA action plan for allergic reactions (‘green plan’)
o Contains personal information and a photo for individuals with medically confirmed
allergies but have not been prescribed and EpiPen®
There may also be circumstances where a non-specific health care plan is developed in
consultation with the child or young person, parent or legal guardian and treating health
professional that may include management for anaphylaxis where an ASCIA action plan is not in
place. This may include where a child or young person has multiple diagnoses that are
incorporated into a single health care plan.
A health support agreement with a safety and risk management plan may be developed in
consultation with the parent or legal guardian to identify and document risk minimisation strategies,
management and treatment for the child or young person in the event of an allergic reaction or
anaphylaxis in the context of the education or care setting.
4.8.1 ASCIA General Action Plan for Anaphylaxis (‘orange plan’)
The general version (orange plan) does not contain personal information and must be
stored in the education or care service with the general use adrenaline autoinjector and
used as an instruction guide.
4.8.2 ASCIA Personal Action Plan for Anaphylaxis (‘red plan’)
The personal anaphylaxis version (red plan) is for a person who has been prescribed an
adrenaline (epinephrine) autoinjector. This plan includes personal information, an area for
a photo and a review date.
The red plan may include a description, including the name, dose and administration
instruction, of other medication (if prescribed) under the ‘action for mild to moderate
allergic reaction’ section. This must be completed by the treating health professional and
can be used as a medication agreement provided all relevant information is included and
legible (ie dose, strength, form, route).
4.8.3 ASCIA Action Plan for Allergic Reactions (‘green plan’)
The allergic reaction version (green plan) is for a person with medically confirmed
allergies where an adrenaline autoinjector has not been prescribed. This green plan
includes personal information, an area for a photo and a review date.
The green plan is developed for a person with a confirmed food, insect or medication
allergy who is thought to be at risk of anaphylaxis. However, as it is not possible to be
certain that the person will not have a severe reaction; the green plan provides guidance
on how to manage anaphylaxis if it occurs.
The green plan may include a description, including the name, dose and administration
instruction, of other medication (if prescribed) under the ‘action for mild to moderate
allergic reaction’ section. This must be completed by the treating health professional and
11 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018may be used as a medication agreement provided all relevant information is included and
legible (ie dose, strength, form, route).
4.8.4 Non-specific Health Care Plan
In some circumstances a non-specific health care plan may be developed by the treating
health professional or specialised nurse practitioner in consultation with parents or legal
guardians, where a child or young person has a severe allergic reaction but has
alternative management strategies for an anaphylaxis incident or has comorbidities. This
may include where a child or young person has multiple diagnoses that are incorporated
in a single care plan.
In these circumstances this must be clearly and regularly communicated to education and
care staff to ensure appropriate management of the child or young person in the event of
a severe allergic reaction.
Where a child or young person has invasive or complex healthcare needs, uncertain
health or changing health they may be eligible for and supported by the Access Assistant
Program (AAP). The Access Assistant Program Flowchart supports education and care
staff to determine when to contact the AAP to talk to a Referral Coordinator.
4.8.5 Individual first aid plan
In some circumstances an individual first aid plan may be developed by the treating health
professional in consultation with the parents or legal guardian where a child or young
person requires a first aid response that is not the standard first aid response for their
health condition.
Where the first aid response for the child or young person is the standard first aid
response for management of anaphylaxis and severe allergies an individual first aid plan
is not required.
4.8.6 Medication management
Administration of medication in an education and care setting must be done following the
medication management in education and care procedure. Administration of any
medication requires a medication agreement with the exception of emergency medication
(adrenaline autoinjector and asthma reliever inhaler).
Where the ASCIA action plan includes the prescription of other medication under the
‘action for mild to moderate allergic reaction’ section a separate medication agreement is
not required provided all relevant information is included and legible (ie dose, strength,
form, route).
It is the responsibility of the parent or legal guardian to provide the education or care
service with prescribed medication. This must be in-date, in the original pharmacy
dispensed package, and include name, date of birth and dose information.
4.8.7 Health Support Agreement
Where a child or young person has been identified to be at risk of allergic reaction and/or
anaphylaxis (this could be with or without a medical diagnosis; and with or without an
ASCIA action plan or a non-specific health care plan) the education or care service may
complete a health support agreement in consultation with the parent or legal guardian.,
including the completion of the safety and risk management plan to ensure the
identification and documentation of site specific risk minimisation strategies, and
individualised management and treatment for the child or young person in the event of an
allergic reaction or anaphylaxis.
The health support agreement should clearly identify cultural, spiritual and language
needs and where a child or young person’s anaphylaxis is severe.
12 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018A health support agreement should be completed where a child or young person has not
been previously diagnosed, but is assumed to have had anaphylaxis and has been
administered the general use adrenaline autoinjector. This should be completed as soon
as practicable after the event and preferably before the child or young person returns to
the education or care service.
A health support agreement should be reviewed in consultation with the parent or legal
guardian in each of the following circumstances:
• annually (at the start of each year)
• when the ASCIA action plan or non-specific health care plan has been reviewed
and updated
• as soon as practicable after an episode of anaphylaxis at the education or care
service to ensure all risk minimisation strategies have been identified and
documented
• prior to the child or young person participating in an offsite activity ie camps or
excursion, or at onsite special events ie class parties, cultural days, fetes, sports
or swimming events, incursions (where the safety and risk management plan has
not addressed risk minimisation strategies for offsite activities an offsite safety
and risk management plan should be developed).
4.8.8 One Plan
This section only applies where a child or young person has a One Child One Plan
(referred to as One Plan).
Where a child or young person has health support needs this must be referenced in the
child or young person’s One Plan. Health needs are recorded under the Notes/Agreed
Actions screen. Under the Type field select Medical from the drop down box.
Health support needs may be recorded in the Support screen to document specific
support requirements, the focus for support, frequency and intensity of the support. This
will enable education and care staff to monitor and provide health support needs for the
child or young person through the One Plan.
4.8.9 Where severe allergies are identified but there is no ASCIA Action Plan or Health
Care Plan
In some circumstances parents or legal guardians may indicate a child or young person
has severe allergies, however there is no ASCIA action plan or non-specific health care
plan in place. In this instance the education or care service should:
• encourage the parent or legal guardian to seek advice from a health professional
to obtain an ASCIA action plan for the management and treatment of the allergies
and anaphylaxis
• develop a health support agreement and safety and risk management plan in
consultation with the parent or legal guardian
• advise the parent or legal guardian of the standard first aid response for
managing allergic reactions and/or anaphylaxis in an education or care service
4.8.10 Who can complete the ASCIA Action Plan, Non-specific Health Care Plan and
Health Support Agreement
ASCIA action plans and non-specific health care plans can only be completed by a
treating health professional or specialised Nurse Practitioner. ASCIA action plans and
health care plans cannot be completed by a parent or legal guardian or by education and
care staff.
Health support agreements are completed by the education or care service in consultation
with the parent or legal guardian, and child or young person (where appropriate).
13 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018Where the health support agreement is being completed for an Aboriginal child or young
person this should be developed in consultation with the primary caregiver, who is not
always the parent. Extended family members and Aboriginal Community Education
Officers (ACEOs) or Aboriginal Health Workers (AHW) may also assist in the development
of the health support agreement to ensure they are developed in a culturally appropriate
and meaningful way.
The development of health support agreements must be completed with an assurance
that the content is understood and culturally valid. Children and families from culturally
and linguistically diverse backgrounds may require additional support persons and access
to interpreter services and Community Liaison Officers (CLOs).
4.8.11 Copies and locations of care plans and support agreements
Original copies of the ASCIA action plans can be photocopied or scanned, preferably in
colour as they are colour coded.
Copies of the child or young person’s personal (red) action plan must be located with
their adrenaline autoinjector and easily accessible.
Additional copies of the personal (red) and allergic reaction (green) action plans should
be kept in various locations around the education or care service so they are easily
accessible by education and care staff in an emergency situation. Locations may include
the child or young person’s classroom, canteen, sick bay, school office and yard duty bag.
A general (orange) action plan must be stored with the general use adrenaline
autoinjector.
The number and location of care plan and support agreement copies will be determined
by the Principal or Director of the education or care service based on a risk assessment
with consideration of timeliness of access in an emergency situation.
A document control for care plans and support agreements form may be completed to
identify the number and location of all copies of the care and support plans. When a care
plan or support agreement is reviewed and updated all forms in all locations must be
replaced.
4.8.12 Review of ASCIA Action Plans and Health Care Plans
The personal (red) and allergic reaction (green) action plans include the date of next
review. Action Plans do not need to be updated each year. If there are no changes in the
diagnosis or management, the medical information on the Action Plan or non-specific
health care plan may not require updating, however the photo should be updated each
time so the child or young person can be easily identified.
Action Plans are often updated and replaced when the child or young person is
reassessed by their treating health professional and/or when their condition changes.
Where a review date has expired the action plan remains valid until an updated form is
received. A review date is NOT an expiry or end date.
4.9 Adrenaline autoinjector (Epipen®)
Adrenaline autoinjectors are automatic injectors that contain a single pre-measured dose of
adrenaline which cannot be reused. They are designed to be used by anyone in an emergency,
including people who are not medically trained. Instructions are shown on the label of each
autoinjector and on the ASCIA action plan for anaphylaxis.
Adrenaline works within minutes to reduce throat swelling, open up the airways and maintain blood
pressure in people experiencing a severe allergic reaction. Withholding or delaying adrenaline
may result in deterioration and potentially death of someone experiencing anaphylaxis.
14 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018In all cases when an adrenaline autoinjector is administered an ambulance must be called and
care for the child, young person or adult must be transferred to the ambulance officer for admission
to hospital for observation and monitoring.
If in doubt give adrenaline autoinjector
It is better to use the adrenaline autoinjector even if in hindsight the reaction is not anaphylaxis.
The potential risks of NOT giving adrenaline far outweigh the potential risks of giving adrenaline.
ASCIA advises that no serious harm is likely to occur from mistakenly administering adrenaline to
a child or young person who is not experiencing anaphylaxis.
4.9.1 Provision of general use adrenaline autoinjector(s) for education and care services
One clearly labelled, ‘general use’ adrenaline autoinjector that has not been prescribed
to a particular child or young pers006Fn must be available at each preschool and school.
• Preschools must have one general use 0.15mg adrenaline autoinjector (eg
EpiPen®Jr)
• Schools must have one general use 0.3mg adrenaline autoinjector (eg EpiPen®)
Where a school has campuses across multiple physical locations and staff are unable to
access the general use adrenaline autoinjector across campuses the Principal or Director
may purchase additional devices.
Adrenaline autoinjectors for general use are available for purchase at any pharmacy
without a prescription. When purchasing an adrenaline autoinjector it is important to
ensure the date on the device has at least 12 months before expiry.
Adrenaline autoinjectors are funded by the education or care service.
Adrenaline autoinjectors must be replaced as soon as practicable after use, when the
integrity of the medication is compromised, or prior to expiry.
The anaphylaxis risk assessment can be completed by education and care services to
assist in planning and measuring the implementation and use of general use adrenaline
autoinjectors.
4.9.2 Prescribing an adrenaline autoinjector to children and young people with a known
risk of anaphylaxis
The child or young person’s treating health professional will prescribe the adrenaline
autoinjector within the context of a comprehensive anaphylaxis management plan. The
decision to prescribe an adrenaline autoinjector for any child or young person is a medical
decision which occurs during a consultation between the treating health professional,
parent or legal guardian and child or young person.
Two adrenaline autoinjectors are usually prescribed to a child or young person where they
have a high risk of anaphylaxis and these are subsidised under the Pharmaceutical
Benefits Scheme (PBS). At least one adrenaline autoinjector should be kept within close
proximity of the child or young person.
Not all children or young people with a diagnosed allergy will be prescribed an adrenaline
autoinjector.
Additional adrenaline autoinjectors can be purchased without prescription from a
pharmacy at full cost.
4.9.3 Adrenaline autoinjector dose recommendations
Adrenaline autoinjectors currently available in Australia include the EpiPen® and
EpiPen®Jr.
15 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018EpiPen®Jr
• Green label device
• Contains 0.15mg of adrenaline
• Usually prescribed/administered for children
aged 1 to 5 years of age (10kg-20kg)
• However, if only a yellow label EpiPen® is available this should be used in
preference to not using one at all.
EpiPen®
• Yellow label device
• Contains 0.3mg of adrenaline
• Usually prescribed/administered for children
over 5 years of age, young people and adults (20kg+)
• However, if only a green label EpiPen®Jr is available this should be used in
preference to not using one at all.
4.9.4 Storing adrenaline autoinjectors
All adrenaline autoinjectors must be kept out of reach of small children but quickly
accessible and not locked in a cupboard or classroom (during recess or lunch). In some
cases exposure to an allergen can lead to anaphylaxis within 5 minutes. An ASCIA action
plan for anaphylaxis must be kept with the adrenaline autoinjector.
Adrenaline autoinjectors are light and heat sensitive and must be stored in a cool dark
place at room temperature (between 15 and 25 degrees Celsius). Where there is a
fluctuation outside of these temperatures the adrenaline autoinjector may be stored in an
insulated wallet with an ice brick; however not in contact with the ice brick as this may
damage the autoinjector mechanism.
Adrenaline autoinjectors must not be stored in a refrigerator or freezer as this may affect
the autoinjector mechanism.
Education and care services need to conduct emergency response training exercises to
time how long it takes to obtain an adrenaline autoinjector (from raising the alarm to
administration) across various locations; this should include consideration of access and
availability of adrenaline autoinjectors on excursions and camps. All emergency response
training should include a review of all aspects of the response; including review of current
action plans, care plans and/or support agreements for effectiveness and review of
storage location of adrenaline autoinjectors to ensure timely access. Areas requiring
further planning or improvements should be identified and actioned.
Points for consideration about adrenaline autoinjector storage:
Front office/first aid area: In the classroom:
Is this the place staff will most likely Is the adrenaline autoinjector stored in a
go to or contact in an emergency? classroom or locker that is not accessible
during breaks? (It should not be stored in a
Are staff always available in this
locked location)
area?
Will the staff on duty (who may be temporary)
Strategy for consideration: teachers
know the location of the adrenaline
to carry a mobile phone and contact
autoinjector?
the front office in the event of an
anaphylaxis emergency so the Will staff know where the adrenaline auto-
adrenaline autoinjector can injector is stored in the room?
immediately be taken to the location
Are adrenaline autoinjectors available on
of the emergency
excursions and school camps?
16 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018In some circumstances, the adrenaline autoinjector may be carried by the child or young
person (refer section 4.6.4 ‘Self-administration of an adrenaline autoinjector by a child or
young person’). For young children (child care or early primary) it is not appropriate for
them to carry an adrenaline autoinjector.
Labelling:
• Where a child or young person has a personal adrenaline autoinjector these must
have a pharmacy label and be stored in the original container that is clearly
labelled with the child or young person’s name.
• The education or care service’s general use adrenaline autoinjector must be
stored within the original labelled container and clearly labelled as ‘general use’.
Training devices:
• Adrenaline autoinjector training devices must never be stored in the same
location as personal use or general use adrenaline autoinjectors to avoid the risk
of confusion.
• All adrenaline autoinjector training devices must be clearly labelled ‘training
device only’.
4.9.5 Disposal of adrenaline autoinjectors (used, expired or damaged)
An EpiPen® is designed for the needle to automatically retract back into the device when
administered, preventing the risk of needle stick injury.
The used adrenaline autoinjector should be handed to the ambulance officer.
Expired or damaged adrenaline autoinjectors should be returned to the pharmacy when
replacing the device.
4.9.6 Expired or damaged adrenaline autoinjectors
The shelf life of an adrenaline autoinjector is around 1-2 years from the date of
manufacture. Devices must be replaced prior to the expiry date. It is important to check
the expiry date on the device, rather than the box.
Education and care services are encouraged to register with the EpiClub® reminder
program when an EpiPen® is purchased. This free service sends a reminder via SMS,
email or post, when the EpiPen® is nearing expiry.
Where the adrenaline autoinjector is for a child or young person’s personal use, and it is
noted by the education and care staff that the expiry date is nearing, the parent or legal
guardian should be notified as soon as practicable. It is the responsibility of the parent or
legal guardian to ensure that at all times medications are in date, and in the original
container with a pharmacy label that includes name, dose and administration instructions.
The ASCIA website notes that a recently expired adrenaline autoinjector should be used
in preference to not using one at all; however the education or care service must ensure
that a regular review is undertaken and general use adrenaline autoinjectors close to
expiry date are replaced.
The EpiPen® contains a clear window near the tip where the
adrenaline can be checked. This should be checked regularly.
Adrenaline is a clear liquid (refer Image A). Where the adrenaline
is cloudy or discoloured (refer Image B) or there is evidence of
sediment the general use device should be replaced or the
parent or legal guardian notified for personal use devices.
Image A Image B
17 | Health support planning: Anaphylaxis and severe allergies in education and care | August 20184.9.7 Regular review of adrenaline autoinjectors
Education and care services should have a nominated staff member to undertake a
regular review of all adrenaline autoinjectors. This includes all general use devices, and
personal use devices that are held by the education or care service.
The review requires a visual inspection of each adrenaline autoinjector to check the expiry
date and the integrity of the adrenaline. This should be completed on the review of
adrenaline autoinjectors checklist.
4.9.8 Using a child or young person’s personal use adrenaline autoinjector for another
person
If the education or care service has a general use adrenaline autoinjector this should
always be used in the first instance.
If the general use adrenaline autoinjector is not available and it is an emergency, the
priority and overarching duty of care is to assist the person having the reaction as it may
be life-threatening. In this instance another child or young person’s personal use
adrenaline autoinjector may be used.
In the event of this education and care staff must ensure the child or young person whose
adrenaline autoinjector has been used is not exposed to any risks until a replacement
device is available. This may include supervision inside if the allergen is environmental or
insect related; or if food related, restrict food options to ensure exposure is minimised.
If a child or young person’s personal use adrenaline autoinjector has been used on
another person the education or care service must, as soon as practicable, purchase a
replacement adrenaline autoinjector from a pharmacy at the education or care service
expense; and the parent or legal guardian notified.
4.9.9 Medication management and legislation for adrenaline autoinjectors
In all cases education and care services must ensure that medication is not administered
to a child or young person unless the administration is authorised and the medication is
administered in accordance with Regulation 95 and 96 of the Education and Care
Services National Regulations 2014 and the Department for Education medication
management in education and care procedure.
The requirement for an authorisation does not apply in cases where the emergency
relates to anaphylaxis or asthma (see Regulation 94(1)). Where an adrenaline autoinjector
is administered in an emergency without an authorisation, the education or care staff must
notify the parent or legal guardian, call the ambulance and transfer duty of care of the
child or young person to the ambulance officer.
Where an ASCIA action plan includes a description of other medication under the ‘action
for mild to moderate allergic reaction’ section, completed by the treating health
professional, this can be used as a medication agreement.
4.9.10 If a parent or legal guardian has not provided an adrenaline autoinjector
Enrolment or attendance cannot be refused because an adrenaline autoinjector is not
provided where a child or young person has a known risk of anaphylaxis.
Parents or legal guardians are ultimately responsible for their child or young person’s
wellbeing and have a duty of care to provide information to the education or care service
about their child or young person’s health care needs together with the appropriate
documentation, equipment and medication. The parent or legal guardian should be
encouraged to provide a personal adrenaline autoinjector for their child or young person.
18 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018If a parent or legal guardian does not provide the education or care service with an
adrenaline autoinjector when this has been prescribed for their child or young person, the
following action should be taken:
• the education or care service will use their general use adrenaline autoinjector if
the child or young person experiences anaphylaxis
• reduce the child or young person’s involvement in high risk activities eg:
o food allergy: only eating food provided from home (need to be very careful at
class parties and during cooking classes)
o insect allergy: kept inside if a bee swarm is present or away from grassed
areas on high-risk occasions as sports days on ovals and during recess and
lunch breaks
o refer to section 4.12 ‘Risk management’ for further risk minimisation activities
• advise the parent or legal guardian of the standard first aid response for
managing anaphylaxis in an education or care service
4.10 Planning and post-incident management
4.10.1 Emergency management
The education or care service has a responsibility to plan for a medical emergency
incident.
A local emergency plan in response to a medical emergency must be developed,
documented and communicated to staff. This should include:
• coordination and responsibilities of education or care staff members
• location of first aid kits and emergency medications
• what will happen during situations such as swimming, excursions, camps, out of
school hours care and on other special occasions
• who will follow up incident management requirements
• appropriate training and regular updates for education and care staff; including
emergency response training exercises
The Department for Education recommends all education and care services undertake
emergency response training periodically to measure the timely response to a medical
emergency or incident across various locations and scenarios. Emergency response
training should:
• include scenarios such as during an excursion, special event or school camp
• include scenarios specific to a child or young person’s action plan, care plan and/or
support agreement (where possible)
• include as many education and care staff as practicable, including out of school
hours care, temporary staff, canteen and kitchen staff, sports staff and volunteers
• measure the time taken to obtain and administer first aid kit and/or emergency
medication (this should include across various location and include the location on
the premises that is the furthest from emergency medication)
• measure time taken for emergency services to arrive on location (this should include
discussion with local emergency services providers to determine best and worst
case scenarios for arrival)
19 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018• prompt improvements and updates to individual Health Support Agreements and the
local emergency plan for the response to a medical emergency where delays are
identified
The Department for Education recommends all education and care services undertake a
post-incident review of all aspects of the local emergency plan for the response to a
medical emergency. The review should be conducted in partnership with clinicians with
relevant expertise and updates to the local emergency plan completed where required.
4.10.2 Child or young person with a known risk of severe allergic reaction or anaphylaxis
Advance planning is the best way to minimise the risk of an incident for children and
young people with a known risk of severe allergies or anaphylaxis.
The following are requirements for education and care services that have an enrolled child
or young person with a known risk of allergic reactions or anaphylaxis:
• an ASCIA personal action plan for anaphylaxis (‘red’ plan), or an ASCIA action plan
for allergic reactions (‘green plan’), or a non-specific health care plan, that has been
completed by the treating health professional
• when planning an off-site activity (ie camps, excursions) or on-site special event (ie
class parties, fetes, cultural days, incursions) where a child or young person with a
known risk will be participating; a review of the action or care plan should be
completed in consultation with the parent or legal guardian (an offsite safety and risk
management plan may be developed)
• a staff member trained in anaphylaxis management including practical training in the
administration of an adrenaline autoinjector available at all times
• an adrenaline autoinjector that is easily accessible in an emergency
• additional medication as authorised in the action plan, health care plan or
medication agreement as an emergency response medicine
• regular communication with parent or legal guardian and other education and care
staff to ensure appropriate and up-to-date information for risk minimisation
strategies, and the management and treatment for the child or young person in an
emergency incident
4.10.3 Post-incident and near miss management
An emergency incident or a near miss incident involving a child or young person
experiencing a medical emergency can be a traumatic experience for the child or young
person involved, staff, parents, peers and other people that have witnessed the incident.
A post-incident debrief should be offered to all people involved, including any witnesses to
the incident, with post-incident counselling available on an individual basis.
Department for Education staff can access the Employee Assistance Program for
confidential face-to-face or phone counselling sessions at any time.
The first aid kit and any emergency medications must be replenished (where required) as
soon as possible.
o If a personal adrenaline autoinjector is used the parent or legal guardian must
be notified; replacement of personal devices are the responsibility of the parent or
legal guardian even when they are used in the education or care service
environment.
o If this is a general use adrenaline autoinjector the education or care service
must replace this as soon as practicable.
An interim management plan should be identified should another episode of anaphylaxis
occur prior to the replacement of the adrenaline autoinjector:
o If this is a personal device the education or care service general device can be
used in the interim
20 | Health support planning: Anaphylaxis and severe allergies in education and care | August 2018You can also read

















































