Green Cleaning in Healthcare: Current Practices and Questions for Future Research
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
H E A L T H C A R E R E S E A R C H C O L L A B O R A T I V E Green Cleaning in Healthcare: Current Practices and Questions for Future Research SEPTEMBER 2011 AUTHORS: Xiaobo Quan, Ph.D., EDAC Anjali Joseph, Ph.D., EDAC Matthew Jelen The Center for Health Design
Health Care Without Harm has initiated a research collaborative coordinated by faculty of the University of Illinois at Chicago School of Public Health, with support from the Pioneer Portfolio of the Robert Wood Johnson Foundation, aimed at stimulating collaborative research around health and safety improvements in health care. The Research Collaborative is designed to increase the evidence base concerning the impacts of sustainable design, construction, organization, operations, and materials and chemicals choices in the health care sector on patient, worker and environmental safety. This paper is the ninth in a series of papers in which the Collaborative provides research and analysis of factors influencing patient, worker and environmental safety and sustainability in the healthcare sector. The editors of this series are Peter Orris, MD, MPH and Susan Kaplan, JD.
TA B L E O F C O N T E N T S
Executive Summary........................................................................................................................................3
I. Introduction...........................................................................................................................................5
Green Cleaning in Healthcare............................................................................................................................. 5
The HHI Pebble Project....................................................................................................................................... 6
II. Methods.................................................................................................................................................7
Expert Advisory Group......................................................................................................................................... 7
Conceptual Framework/Literature Review........................................................................................................... 7
Case Study............................................................................................................................................................ 7
Questionnaire Survey........................................................................................................................................... 8
Data Analysis........................................................................................................................................................ 8
III. Results...................................................................................................................................................9
The Conceptual Framework................................................................................................................................. 9
Case Studies........................................................................................................................................................ 11
Dartmouth-Hitchcock Medical Center, Lebanon, NH............................................................................ 11
Ridgeview Medical Center, Waconia, MN.............................................................................................. 12
Magee-Womens Hospital of UPMC, Pittsburgh, PA .............................................................................. 14
Boulder Community Hospital, Boulder, CO............................................................................................ 16
Cleveland Clinic, Cleveland, OH............................................................................................................ 17
Case Study Summary.......................................................................................................................................... 18
Common Green Cleaning Practices in Participating Facilities............................................................... 18
Implementation of Green Cleaning......................................................................................................... 19
Evaluation & Results of Green Cleaning................................................................................................. 20
Survey of High Priority Research Topics/Questions.......................................................................................... 20
Respondents.............................................................................................................................................. 20
Key Components of Green Cleaning....................................................................................................... 20
High Priority Research Topics.................................................................................................................. 22
High Priority Research Questions............................................................................................................ 22
Research Questions About Green Cleaning’s Effects on Staff and Patient Health................................. 24
IV. Conclusion...........................................................................................................................................25
Appendix I. Case Study Phone Interview Protocol.........................................................................................27
Appendix II. Green Cleaning Research Priority Survey Questionnaire...........................................................32
Appendix III. Selected Materials From the Facilities......................................................................................36
Appendix IV. Research Questions From Survey Respondents........................................................................46
Appendix V. Expert Advisory Group Members..............................................................................................51Acknowledgements We would like to thank case study interviewees Brian G. Kovaly, John Litchfield, Damian Natal, John J. Welenc, and Todd Wilkening, as well as all individuals who responded to the questionnaire survey. We also thank Janet Brown and Nancy DellaMattera for their help with online survey distribution. Special thanks go to advisory committee members Judene Bartley, Pat Burdullis, Janet Brown, Ridley Kinsey, Jason Marshall, and Hubert Murray for their guidance and support throughout the project. We would also like to thank Susan Kaplan for her guidance and input on various drafts of this report. We are grateful for the support from Health Care Without Harm and the Healthier Hospitals Initiative.
EXECUTIVE SUMMARY
Environmental cleaning plays a key role in prevent- energy consumption), patient and staff satisfaction, and
ing healthcare associated infections (HAIs). But cost-effectiveness.
many current cleaning practices in healthcare may
negatively impact human health and the environ- Eight green cleaning practices were found in the five
ment. Green cleaning is a new, promising approach to case study facilities. These practices generally fall into
environmental cleaning that aims at reducing harm to three main categories: 1) selection of cleaning products
human health and the environment while maintaining (including green cleaners, cleaning tools or equipment
or improving the hygiene of the healthcare environ- that use less water and chemicals, and minimal number
ment. While a growing number of healthcare facilities of chemical types); 2) operational change (including
are adopting green cleaning practices, there are many cleaning for appropriate levels of cleanliness, applica-
essential questions around green cleaning that remain tion and dispensing methods, and use of fluorescent
unanswered due to the lack of research in this area. marker); and 3) building design (including interior
design that reduces the need for cleaning or facilitates
The objective of the Healthier Hospitals Initiative cleaning, and layout that makes housekeeping more
(HHI) Pebble Project is to promote and support efficient). Variations exist in green cleaning practices
development of green cleaning initiatives by better across different facilities. The selection of cleaning
understanding current green cleaning practices and products that contain or use less harsh chemicals is the
identifying future research topics of high priority. most commonly adopted method. Operational changes
Under the guidance of an advisory group consisting commonly implemented include the establishment of
of industry experts, the project team at the Center appropriate cleanliness levels in different areas based
for Health Design (CHD) a) established a conceptual on infection risk estimation and optimal application
framework for green cleaning through literature review, and dispensing of cleaning chemicals (e.g. squeezing or
b) conducted case study interviews with representatives pouring chemicals directly onto cleaning cloth instead
from five major healthcare facilities, and c) conducted of spraying). All case study facilities have made efforts
an online questionnaire survey of high-priority research to select flooring materials that require less cleaning
questions around green cleaning. and maintenance, but research evidence is lacking to
support informed decisionmaking on this issue.
The conceptual framework takes a systemic approach
toward green cleaning. Factors around green clean- The implementation of green cleaning usually
ing generally fall into three groups: The healthcare involves strong leadership from facility administration
hygiene system, external and internal factors impact- and internal multi-disciplinary sustainability teams,
ing the healthcare hygiene system (e.g. regulations, as well as staff acceptance and ownership. Almost all
sustainability movement, staff education and training), case study facilities conducted initial evaluation of
and outcomes influenced by healthcare cleaning and new products and procedures before implementation,
hygiene. The healthcare hygiene system is an integra- but rarely monitored or evaluated the performance of
tion of not only healthcare cleaning (including risk the products and procedures after adoption. Certain
assessment and the selection, application, and disposal healthcare outcome data have been routinely collected
of cleaning agents) but building design (e.g. ventilation for other business purposes (e.g. infection preven-
system, interior finish materials) and operational design tion), but typically were not utilized in the evaluation
(e.g. building maintenance, waste management). These of green cleaning. Anecdotal evidence from the case
components of the healthcare hygiene system interact studies suggests that green cleaning generally results
with each other and other factors to influence multiple in benefits such as reduced use of water and chemicals,
outcomes, including environmental cleanliness, risk of fewer complaints from staff and patients, and lower
HAIs, health effects (e.g. asthma, dermatitis), envi- levels of infection rates.
ronmental impact (e.g. bioaccumulation, waste, and
Green Cleaning in Healthcare: Current Practices and Questions for Future Research 3The 150 respondents to the survey were mostly health- The actual effects of green cleaning are typically not
care staff, including environmental service managers, routinely monitored and evaluated, even though cer-
nurses, sustainability consultants and administrators. tain relevant data may already be collected for other
The majority of the respondents perceived green clean- purposes in various health care departments. For the
ing to be only a practice of selecting and using appro- ongoing development of green cleaning initiatives,
priate cleaning products, while other important aspects it is urgent to conduct research focusing on practical
including operational changes and building design were questions from real settings, for example:
largely ignored. The three most important research
• How do green cleaning products/practices effec-
topics identified in the survey are 1) the effect of green
tively impact environmental cleanliness and HAI
cleaning on facility cleanliness and HAI prevention;
transmission?
2) the effectiveness of green cleaning in protecting
the environment; and 3) the health effects of green • How do green cleaning products/practices effectively
cleaning. Other important research topics identified impact the environment?
include the cost-effectiveness of green cleaning and the
• How do green cleaning products/practices effectively
development of standard methods to evaluate different
impact human health (e.g. asthma, dermatitis)?
green cleaning products and practices.
• What are the standard tools and methods for the
In conclusion, green cleaning is an interdisciplinary, comparative evaluation of various green cleaning
systematic approach involving the selection and use of products/practices?
cleaning products as well as operational changes and
• How cost-effective and feasible are certain products/
building design. A variety of green cleaning products
practices?
and practices have been implemented in healthcare
facilities. However, one big challenge in implement- • What are the advantages and disadvantages of vari-
ing green cleaning is the limited evidence regarding ous flooring materials in regard to cleaning?
the effectiveness of these products and practices.
4 Green Cleaning in Healthcare: Current Practices and Questions for Future ResearchI. INTRODUCTION
Green Cleaning
Concerned about the adverse human and environ-
mental effects of traditional cleaning practices, many
healthcare organizations have been increasingly adopt-
in Healthcare ing green cleaning or sustainable cleaning practices.
However, a commonly accepted definition is lacking,
Maintaining the cleanliness of the healthcare environ- and ‘green cleaning’ has taken on different forms in
ment and minimizing the concentration level of patho- different organizations. Green cleaning, or sustainable
gens is an essential way of preventing healthcare-asso- cleaning, generally refers to a variety of environmental
ciated infections (HAIs), which pose serious threats cleaning approaches (e.g. selection of cleaners, use
to patient safety and contribute to an increase in of alternative cleaning methods, changes in build-
healthcare costs (Sehulster, et al., 2004). In addition, ing design and operations) that aim at reducing the
environmental cleanliness is a critical factor impacting harmful effects of cleaning on human health and the
other healthcare outcomes, such as patient satisfaction environment while maintaining or improving the
(Sofaer, Crofton, Goldstein, Hoy, & Crabb, 2005). cleanliness of the healthcare environment for the pur-
pose of infection prevention. Promising green clean-
Various chemicals have been used in the cleaning pro- ing efforts such as purchasing and using cleaners with
cedure (removing visible soils such as soil particles and more benign chemicals have been reported in multiple
organic matter) and the disinfecting procedure (killing hospitals around the country.
microorganisms) routinely performed in healthcare
settings. A growing body of evidence suggests that However, many knowledge gaps exist around green
the ingredients of many cleaning and disinfecting cleaners and green cleaning programs (Markkanen,
products may have unintended negative impacts on Quinn, Galligan, & Bello, 2009). For example, there
human health and the environment. Patients’ and appears to be a lack of industry agreement as to what
staff’s exposures to cleaning chemicals can cause constitutes a green cleaning program for a healthcare
dermatitis, endocrine and neurologic effects, cancer, facility. Also, what kinds of cleaners should be defined
asthma, and other respiratory disorders (Delclos et al., as ‘green?’ Further, there is no clear evidence indicating
2007; Rosenman et al., 2003; Stingeni, Lapomarda, whether cleaners that are promoted as ‘green clean-
& Lisi, 1995). Cleaning chemicals may contribute to ers’ effectively meet infection prevention needs and
the pollution of outdoor air and water supplies, dam- standards given the current focus on the environmen-
age to ecosystems, bioaccumulation in animals and tal contribution to HAIs (Goodman et al, 2008) or
plants, and ozone depletion (Environmental Protection whether such cleaners have unknown health risks; and
Agency, n.d.). Further, certain cleaning practices are there are no widely available data about the imple-
found to be associated with musculoskeletal disorders mentation and the effectiveness of the green cleaning
in cleaning staff (Kumar, Chaikumarn, & Lundberg, programs in different healthcare facilities (Markkanen,
2005; Unge, Ohlsson, Nordander, Hansson, Skerfving, et al., 2009; Sattar, 2010). There is an urgent need to
& Balogh, 2007). conduct research around cleaning in healthcare to fill
these knowledge gaps.
Green Cleaning in Healthcare: Current Practices and Questions for Future Research 5The HHI Pebble Project
This paper is the ninth paper in the Health Care
Research Collaborative’s monograph series providing
research and analysis of factors influencing patient,
worker and environmental safety and sustainability in
the health care sector. The Research Collaborative was
initiated by Health Care Without Harm (HCWH), an
international nonprofit coalition that promotes envi-
ronmental responsibility in health care, and is coordi-
nated by faculty of the University of Illinois at Chicago
School of Public Health, with support from the Pioneer
Portfolio of the Robert Wood Johnson Foundation.
The Research Collaborative’s mission is to stimulate
the development, coordination and dissemination of
research focused on the impact of the health care built
environment, operations and organization on patient,
worker and environmental safety and sustainability.
The Collaborative also interacts closely with the
Healthier Hospitals Initiative (HHI), a group of health
systems that are leading the way in implementing green
practices in healthcare.
HCWH and HHI engaged with the Center for Health
Design’s (CHD) Pebble Project to promote and support
research on green cleaning. The aims of this proj-
ect were: To conduct a literature review in order to
establish a conceptual framework for green cleaning, to
conduct five best practice case studies in order to gather
information about the current status and effectiveness
of green cleaning practices, and to conduct a question-
naire survey of practitioners and experts in the field to
identify high priority research questions around green
cleaning in healthcare. In a future phase, HHI and
HCWH will support and engage qualified researchers
to investigate top priority research questions identified
during this project. This report describes the methodol-
ogy, procedures, and findings from this study.
6 Green Cleaning in Healthcare: Current Practices and Questions for Future ResearchII. METHODS
Under the guidance of an expert advisory group, the
project team at CHD conducted the study in three
steps. Literature review, phone interview and question-
Case Study
naire survey were the major methods used in the study.
Based on the conceptual framework and HCRC paper,
a phone interview protocol was developed for the best
practice case studies. The protocol was divided into six
Expert Advisory Group sections (see Appendix I):
• General information about the healthcare organiza-
An expert advisory group provided guidance through- tion (e.g. name, address, # of beds, type)
out the project. The group members had expertise in • Green cleaning program (e.g. risk assessment, cleaning
green cleaning but were from diverse backgrounds, products, building design, and operational changes)
including healthcare sustainability, infection preven- • Implementation process (e.g. organization of the
tion and control, healthcare operations, evaluation of green cleaning program, logistics, timeline, chal-
cleaning chemicals and equipment, and building mate- lenges and difficulties)
rials manufacturing. Regular conference calls between • Evaluation methods
advisory group members and the research team were • Benefits and lessons learned
conducted. The advisory group provided feedback on • High priority research questions
the conceptual framework, identified healthcare orga-
• In addition, the protocol asked for additional infor-
nizations and field experts to be included in the case
mation and materials such as cleaning protocol and
studies and the survey questionnaire, helped to refine
personal comments.
the phone interview protocol and the survey question-
naire, and reviewed the final report.
The recruitment of case study facilities was conducted
through emails and phone calls. The advisory committee
members recommended a total of seven healthcare orga-
Conceptual Framework/ nizations, as well as one or two individuals familiar with
the green cleaning program at each organization. The
Literature Review project team contacted individual facilities by email and
followed up with phone calls. However, not all identified
The project team reviewed the 2009 Health Care facilities were responsive to the request for participation
Research Collaborative (HCRC) paper focusing on and one facility decided to withdraw after initially agree-
green cleaning in healthcare and some of the articles ing to participate. Therefore, several additional facili-
and reports about green programs that were specifically ties were added to the list of potential participants. The
mentioned in the HCRC paper (Markkanen, et al., recruitment process continued until five healthcare orga-
2009). Based on the literature review and comments nizations agreed and completed the telephone interview.
from the advisory group, a conceptual framework for
green cleaning was established and refined. Then the A telephone interview was conducted with a represen-
conceptual framework was used to develop a case study tative from each participating facility. Four interview-
interview protocol and a survey questionnaire. ees are the directors or managers of environmental/
housekeeping departments. One is the director of the
facility. The length of interviews averaged about 1 hour
and ranged from about 45 minutes to 1.5 hours. The
project team generally followed the interview protocol
and made adjustments based on specific situations of
Green Cleaning in Healthcare: Current Practices and Questions for Future Research 7different organizations. Detailed notes were taken dur-
ing each interview. Before each interview, the project
team gathered information (e.g. web pages, presenta-
Data Analysis
tions) about the green cleaning programs at the facility.
The data collected from case study interviews were
After each interview, the project team followed up with
sorted and compiled in a matrix, where the data was
the interviewee to request materials used in the green
classified into several categories—green cleaning
cleaning program and detailed results.
features, implementation, green cleaning definition,
evaluation and results, and high priority research ques-
tions. Common themes were extracted from interview
Questionnaire Survey data through content analysis. Additional data pro-
vided by the interviewees were analyzed according to
data type.
An online questionnaire was developed, based on
findings from the 2009 HCRC paper and the case
Questionnaire survey responses were collected using
studies. The primary purpose of the questionnaire was
tools integrated in Survey Monkey and transferred to
to identify high priority research topics around green
Excel format. The data were analyzed using descriptive
cleaning in healthcare. Respondents were also asked to
statistics. Top research topics and questions were tabu-
define components of a green cleaning program, based
lated. Common themes were extracted from responses
on their experience/expert knowledge. The online
to the open-ended questions regarding the key compo-
questionnaire contained a total of 10 questions. In
nents of green cleaning and most important research
addition to selecting high priority topics from a list,
questions.
respondents were also asked to provide examples of
specific high priority research questions. The paper ver-
sion of the questionnaire was reviewed and was revised
based on feedback from the advisory group members.
The online version was pre-tested with a small group of
green cleaning experts.
The online survey was sent out by email to the list-
serv mailing list of Practice Greenhealth and the
Healthcare Career Advancement Program (H-CAP),
as well as a list of experts identified by the advisory
members. A total of about 2,500 email notifications
were sent out in the first round. Reminders were sent
out one week and two weeks later to ask recipients to
complete the survey.
8 Green Cleaning in Healthcare: Current Practices and Questions for Future ResearchIII. R E S U LT S
The Conceptual Framework
• Healthcare hygiene system: Healthcare cleaning is
a key component of the healthcare hygiene system,
which serves the purpose of controlling infections in
hospitals by reducing cross-contamination of envi-
ronmental surfaces (Guh, Carling, & Environmental
Evaluation Workgroup, 2010; Carling et al., 2008).
Other components of the healthcare hygiene system
include building design (e.g. patient rooms, HVAC,
finish material) and operational design (e.g. build-
ing maintenance, waste management). All the
above components interact with each other and are
According to the literature, green cleaning generally integrated into an overall healthcare hygiene system
refers to “cleaning to protect health without harming (Markkanen, et al., 2009). For example, research
the environment,” or the efficacy of infection preven- found that building design may facilitate or hinder
tion and control “toward effective products with the healthcare cleaning (Guenther & Vittori, 2008).
fewest adverse effects on human health and the envi- Research also found that the amount of harmful
ronment,” or “maintaining and improving cleanliness exposure to cleaning chemicals was not only deter-
and supporting infection control while protecting mined by the physical characteristics of cleaners
workers and the environment from the risks posed by (e.g. aerosols vs. liquids), but also impacted by types
cleaning materials and processes” (ABM Industries, of cleaning tasks (e.g. spraying vs. mopping) and the
n.d.; Markkanen et al., 2009; Practice Greenhealth, built environment (e.g. ventilation) (Bello, 2008).
n.d.). Even though there is not a definition of green Evaluation of thoroughness of cleaning was consid-
cleaning that is widely accepted, the 2009 HCRC ered an essential element of a complete system (Guh
paper clearly indicated that green cleaning is a sys- et al., 2010; Carling & Bartley, 2010).
tematic approach including not only the use of clean-
ers identified as ‘green’ due to their chemical composi- • Healthcare outcomes: The healthcare outcomes
tion and attributes, but a comprehensive performance influenced by the healthcare hygiene system are
improvement process that includes any other methods classified into four categories—infection prevention
that may reduce the negative impact of hospital and control, health effects, environmental impact
cleaning on human health and the environment (e.g. and other outcomes. It is well documented that
using micro-fiber mops, improving performance of environmental hygiene is a key factor impacting
cleaning staff, and selecting finish materials that are the prevalence of environmentally-mediated HAIs
easier to clean). among patients and healthcare workers (Sehulster
et al., 2004; Ulrich et al., 2008; Goodman et al.,
Based on the 2009 HCRC paper, a framework of 2008). As discussed previously, the practice of
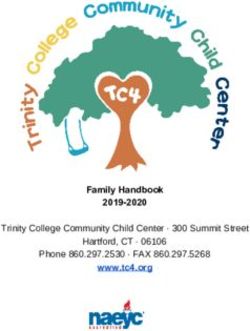
green cleaning was created. The framework (see using strong chemicals to maintain environmental
Figure 1) demonstrates factors around green cleaning hygiene in healthcare may have some unintended
in three columns: effects, such as asthma in patients and healthcare
staff, dermatitis and musculoskeletal disorders of
• External and internal factors impacting healthcare cleaning staff, and bioaccumulation of chemicals in
cleaning: Many factors could impact the implemen- the environment (Delclos et al., 2007; EPA, n.d.;
tation of healthcare cleaning and the purchasing of Unge et al., 2007). In addition, the cleanliness of
cleaning products. For example, the sustainability the healthcare environment greatly impacts patient
movement acts as a driving force towards more satisfaction with the overall healthcare services
attention to human health, including sensitivity that they received (Krueckeberg & Hubbert, 1995).
to chemicals and pollutants in healthcare (Green Cleanliness of the environment is used to measure
Guide for Health Care, 2007). The limited avail- patient satisfaction in the Centers for Medicare
ability and high cost of effective green cleaning & Medicaid Services (CMS) Hospital Consumer
products as well as skepticism from healthcare Assessment of Healthcare Providers and Systems
staff and administrators could impede the imple- (HCAHPS) survey, as well as the Press Ganey
mentation and development of green cleaning patient satisfaction survey.
(Markkanen, et al., 2009).
Green Cleaning in Healthcare: Current Practices and Questions for Future Research 9Figure 1. Conceptual Framework of Green Cleaning in Healthcare
FACTORS IMPACTING
HYGIENE SYSTEM HEALTHCARE HYGIENE SYSTEM OUTCOMES
External factors Cleaning Healthcare infection
•• Regulations, guidelines, Infection Control Risk Assessment prevention & control
certifications (e.g., EPA, •• Measurable surface cleanliness/
•• Levels of cleanliness (critical, non-critical, high-
CMS; CDC guidelines; cleanability
touch surfaces, etc.)
Green Seal, EcoLabel) •• HAI
•• Green-sustainability Cleaning Agents
movement (Detergents, disinfectants, etc.)
•• Availability of products Health effects
•• Chemical characteristics
•• Respiratory (asthma)
•• Physical characteristics (aerosols, liquids)
•• Skin effects (dermatitis)
Intra-hospital influences •• Compatibility with surfaces
•• Musculoskeletal disorders
•• Environmental services Application and disposal •• Cancer
productivity, education, •• Unknown effects
•• Application (spraying, mopping, powered cleaning
training policies/
equipment, dilution control system)
procedures
•• Applicator types (e.g. cloth vs. mops, microfiber Environmental impact
•• Environmental purchasing
system) •• Bioaccumulation (biodegradation
programs
•• Procurement, use, disposal time, bioconcentration value)
•• Infection prevention •• Ecosystems
& control •• Air pollution (smog)
Other hygiene methods •• Ozone depletion
•• Clinical
•• Administration Building design (fixed) •• Waste (product packaging)
•• Single rooms •• Energy consumption
•• Ventilation system
•• Surface finish materials (flooring not requiring Other outcomes
regular stripping/polishing) •• Cost
•• Technology (e.g., motion-sensitive lights, doors, sink •• Job satisfaction
design, automated faucets, HEPA filters, UVGI, etc.) •• C-suite satisfaction
•• Equipment/furniture •• CMS HCAHPS survey
Operational design (movable)
•• Work practices (feedback on cleaning effectiveness,
e.g. targeting methods; exterior facility / entryway
maintenance, e.g. matting system)
•• Technology (e.g. HEPA filtered vacuums)
•• Building maintenance (water leaks / dampness)
•• Waste management / recycling
Green cleaning aims at: 1) reducing hospital cleaning’s harmful effects on human health and the environment;
2) enhancing hospital hygiene and reducing infections. In order to develop green cleaning programs, an under-
standing of basic cleaning programs helps to focus on removal of soil/bioburden in a manner that permits evalua-
tion of cleaning thoroughness. Then the least harmful cleaner can be used in developing a “green” cleaning program.
10 Green Cleaning in Healthcare: Current Practices and Questions for Future ResearchCase Studies
This section takes a close look at each of the individual green cleaning programs at the five participating healthcare
facilities. Then it summarizes the common features of green cleaning programs across different facilities in order to
explore current best practices and identify lessons learned that are applicable to other facilities.
Dartmouth-Hitchcock Medical Center, Lebanon, NH
Dartmouth-Hitchcock Medical Center (DHMC), New • Cleaning tools or equipment that use less water and
Hampshire’s only academic medical center, includes a chemicals: DHMC adopted micro-fiber mops and
396-bed acute care hospital, a medical school, a clinic, cloths for cleaning, since they use less water and
and a physician network. DHMC’s green cleaning chemicals and generate less waste than the tradi-
efforts began about 10 years ago, when green cleaners tional string mops and cloths. To prevent cross-
were introduced into the facility. contamination, each mop head is used in only one
patient room at DHMC. From the perspective of
Green Cleaning Components staff health, micro-fiber mops are lighter and easier
The main green cleaning features at DHMC include to maneuver, thus may reduce staff fatigue and back
green benign cleaners, green floor finishes and strippers, injuries. DHMC is also using a new type of floor-
finish materials requiring less cleaning and finishing, scrubbing machine with specialized floor pads that
reduction of horizontal surfaces, movable furniture, use less floor stripper to remove finish from large floor
floor mat system at entrances, vacuum cleaners, micro- areas more efficiently (less labor and time) (Clarke
fiber mops and cloths, new methods of dispensing and Autoscrubber with BOOST). Another type of floor
applying cleaning chemicals, and green pest control. machine used at DHMC helps to reduce chemical
and water use by using a different application process
• Green cleaners: DHMC uses green cleaners certi- in which self-collapsing foam attracts dirt more
fied by Green Seal, including the carpet cleaner, the effectively (Nobles FAST technology). For cleaning
glass cleaner, the degreaser and citric acid cleaner, surfaces, DHMC has adopted the use of a spray bottle
as well as the all-purpose peroxy cleaner that is used that uses electrically charged water (ActiveIon).
on all other surfaces that do not need disinfection. This technology claims to be effective in cleaning
A disinfectant not categorized as green is used to surfaces without the use of any chemicals.
disinfect surfaces that patients frequently touch.
Sensitivity and allergy concerns drove the shift from • Application and dispensing methods: Metered
old style floor finishes with heavy metals and ammo- chemical dispensers at DHMC reduce spills and
nia to green finishes and stripping methods. waste of chemicals by carefully dispensing chemicals
at the right dilution rate. A new practice of applying
• Interior design that reduces the need for cleaning chemicals is to squeeze chemicals from a bottle with
and finishing or facilitates cleaning: This includes a pour spout onto a cleaning cloth. Compared to the
flooring finish materials that do not need regular old practice of spraying chemicals onto surfaces, this
finishing such as rubber flooring, large ceramic tiles helps to avoid chemical aerosols entering indoor air.
with minimal grout, wall protection, reduction of A new floor finish applicator is also used to contain
horizontal surfaces that collect dust, and movable floor finish in a box during application, thus prevent
furniture at nursing stations and other places that odors and volatile organic compounds (VOCs) from
helps to reduce interference between cleaning and escaping into the air.
other healthcare activities. In addition, DHMC
utilizes a floor mat system at entrances and vacuum
cleaners to reduce the need for chemical cleaning.
The amount of soil and dirt inside buildings was
reduced by using a floor mat system at each entrance
and vacuuming and sweeping entrances.
Green Cleaning in Healthcare: Current Practices and Questions for Future Research 11Implementation ATP (adenosine triphosphate) testing. ATP testing is
The green cleaning program at DHMC has been a new method to efficiently evaluate the effectiveness
evolving over recent years. The facility’s leadership is of products and procedures and the performance of
a strong advocate of sustainability, willing to try new cleaning staff. However, the high cost of ATP test-
products or methods that enhance sustainability, even ing prohibits its wide usage. Currently, DHMC uses
at an extra cost. Over the years, DHMC gradually ATP testing only in operating rooms, other procedure
increased the use of green cleaners and other green rooms, and patient rooms. In addition, staff injury
cleaning methods as they became available. Training data are collected and monitored by the safety depart-
and educating staff has been a key component of the ment. However, this data was not accessible to the
green cleaning program. The environmental service research team for this project.
department at DHMC includes supervisors and a train-
ing and quality assurance manager to oversee cleaning It is estimated that green cleaning can be economically
performance and provide training to new and exist- beneficial, especially when chemical usage is reduced or
ing staff. There were challenges and difficulties in the eliminated. Although detailed data are not available,
implementation of certain green cleaning measures. it is evident that some green cleaning methods (e.g.
For example, cleaning staff sometimes were not willing micro-fiber mops) may result in significant reduction in
to give up conventional practices (e.g. spray bottles, use of chemicals and water. In addition, since the cost
cotton string mops). This problem was successfully of green cleaners has dropped significantly in recent
addressed by explaining to staff the benefits of new years, changing from conventional to green cleaners
products and practices to personal health. However, does not cause a significant cost increase.
some staff members still complain that micro-fiber
mops do not clean as well as conventional mops. Questions for Further Research
DHMC is interested in identifying the pros and cons
Evaluation & Results of different flooring materials (including linoleum
DHMC evaluates new cleaning products or proce- and rubber) in terms of ease of cleaning, installation,
dures through visual inspection, customer survey, and and so on.
Ridgeview Medical Center, Waconia, MN
Ridgeview Medical Center (RMC) is an independent, location of housekeeping closets, and high-concen-
regional healthcare network including a Waconia- tration chemicals.
based 109-bed acute care hospital (about 242,000 • Cleaning for appropriate levels of cleanliness:
SF), various primary and specialty care clinics, emer- Ridgeview follows CDC guidelines to determine
gency services, and specialty programs. It serves the appropriate cleanliness levels in different areas. To
west-metro area of Minneapolis. At Ridgeview, green avoid potential negative impacts of using overly
cleaning is an integrated management process aiming strong cleaning chemicals, only chemicals with
at using products with minimal toxicity to achieve minimal toxicity levels are used at least frequency
hospital hygiene without increasing rates of HAIs. The as determined to be necessary for specific areas.
facility began to implement green cleaning in 2003. Areas that only need general sanitation are not
disinfected. For example, important clinical areas
Green Cleaning Components with high infectious risks such as ORs and ICUs
Major components of green cleaning at Ridgeview may need more potent chemicals than general office
include the practice of using minimal toxicity clean- areas. The facility used to clean floors in critical
ers to achieve appropriate levels of cleanliness in areas using phenolics and quaternary cleaners but
various areas, green benign cleaners, minimal number later realized that it is not necessary to disinfect
of chemical types in one facility, interior design the flooring in critical areas since the flooring was
resulting in less need for cleaning, a floor mat system, always non-sterile anyway. Therefore, only least
12 Green Cleaning in Healthcare: Current Practices and Questions for Future Researchtoxic cleaners are used to clean OR floors. The facil- • Layout that makes housekeeping more efficient.
ity also switched from quaternary cleaners to general Ridgeview has conducted modeling studies to
sanitation in office and back room areas and reduced examine how the location of housekeeping closets
the frequency of chemical cleaning and the amount impacts the footsteps and travel distance of cleaning
of chemicals used in critical areas such as ORs. staff members. Lean construction modeling was used
According to Todd Wilkening, Director of Facilities, to minimize staff walking. Fewer footsteps could be
“Never dust with dynamite!” is a simplistic way of translated into more cleaning time, better cleaning
describing the industry’s norm of “over cleaning.” performance, less need for re-cleaning, and lower
Wilkening adds that “through these process changes, cost to the organization, not to mention less staff
no increase in infection rates is evident.” fatigue, which leads to greater staff satisfaction and
performance.. However, this data is not currently
• Green cleaners. Green Seal certified cleaners are
being collected by the organization.
used at Ridgeview, including the general purpose
cleaner, the glass cleaner, cleaning and degreasing
compounds, floor cleaners, waxes, and the restroom Implementation
cleaner. Complaints from staff and patients regard- Ridgeview’s green cleaning program is driven by its
ing sensitivity to certain chemicals have led to the quadruple bottom line—social, economic, and envi-
adoption of least toxic chemicals. In some areas, ronmental benefits, and passion for the organization
vinegar and water or soap and water are used to and the community. Both facility leadership and staff
reduce the use of toxic chemicals and reduce the ownership are important to the success of the program.
amount of personal protection devices such as eye A value analysis team, including representatives from
shield and gloves that are used. Further, it is noted nursing, material management, finance, environmen-
at Ridgeview that it is important to select clean- tal and facility services, and infection control, plays
ing products that have minimal aerosolization and an important role in the program. The team members
fragrances, in order to improve indoor air quality. review products from different (sometimes conflicting)
This includes the use of fragrance free chemicals. perspectives, reach compromises, and provide recom-
The amount of waste, including used containers of mendations to department managers. The sometimes
cleaning chemicals, is also reduced by using high- conflicting interests lead to making the best well-
concentration chemicals. rounded decisions for an organization. This is truly a
health “dynamic tension.”
• Minimal number of chemical types: Increased risks
of long-term cumulative effects may be associated As a part of the integrated patient care initiative, the
with the existence of many different types of chemi- green cleaning program emphasizes the training of
cals in one healthcare setting. Ridgeview has been staff and the education of patients. New staff members
making efforts to identify versatile cleaners that can usually go through a formal orientation process to learn
clean multiple types of surfaces. However, it has about the appropriate use of various kinds of chemicals.
been challenging to find a one-size-fits-all product. During staff education, evidence about the toxicity of
• Interior design that reduces the need for cleaning and conventional cleaners and the benefits of green clean-
finishing or that facilitates cleaning: A well-designed ers has been an effective tool to facilitate the transition
HVAC system, finish materials that are easy to clean to green cleaners. Through education, staff members
and maintain, and a good matting system are interior understand the personal and professional benefits of
design features adopted at Ridgeview Medical Center green cleaning.
that reduce the chemical cleaning required. When
selecting products, thinking of the “end in mind” The identification and selection of suitable green
operationally is critical. Service departments need products is one challenge encountered in implementing
to be involved during the design process in order to green cleaning. First, it takes time (from several days to
reduce operating expenses and toxicity in the work- months) to evaluate, select, and procure new prod-
place. According to Todd Wilkening, “If you study ucts. Second, sometimes it is difficult to find the right
the model of integrated medicine, it is a no brainer!” product. When the program began in 2003, few green
He adds, “It becomes about living your faith through cleaners were cost-effective. This forced Ridgeview to
your organization’s mission.” look at different manufacturers or go back to conven-
tional cleaners that were more toxic, which was not
Green Cleaning in Healthcare: Current Practices and Questions for Future Research 13desirable. However, when looked at holistically, green staffing (e.g. new staff with hypersensitivity issues).
cleaners are not costly, according to Ridgeview, when For the evaluation of new products, manufactur-
the costs of personal protective equipment (PPE) and ers are asked to provide material safety data sheets
employee risk are added into the equation. Although (MSDSs) and the carbon implications of using the
more green cleaners have become available recently, it products (including the environmental impact of the
is still difficult to find a one-size-fits-all cleaner in order manufacturing process, although this could be a very
to minimize the number of chemical types. Another rough estimate). The facility typically monitors costs of
challenge is the false perception of many people that supplies, cleaning staff hours per square footage, HAI
any sustainability efforts would cost a lot and sacrifice rates, employee illness, and job satisfaction, although
business for the environment. Education, external some of the data are collected for purposes unrelated to
pressures, and guidelines are critical to overcome these the cleaning program. In addition, the facility conducts
challenges. culture tests to assess surface cleanliness, though this is
not a consistent effort and data is difficult to interpret.
Evaluation & Results According to Paul Whittaker, Environmental Services
Ridgeview conducts pilot tests on new products and Manager at Ridgeview Medical Center, “Based on the
periodically re-evaluates cleaning products regarding overall cost data, the cost of green cleaning is at or
their effects on staff health after they are accepted slightly above the historic level, and green cleaning is
into the facility. The re-evaluation and replacement not a financial burden for the facility.”
of cleaners may be justified when there is a change in
Magee-Womens Hospital of UPMC, Pittsburgh, PA
Magee-Womens Hospital of UPMC is a specialty prevention and control perspective. For example,
women and children’s hospital providing a wide range bleach wipes are used in daily cleaning on high touch
of services. It has 350 patient beds, an emergency room, surfaces in patient rooms such as TV remote control,
and ambulatory facilities on four floors. It was a stand- over-bed tables, door knobs, and bedside equipment,
alone hospital before it merged with UPMC in 1999. which tend to get contaminated through contact
Magee-Womens started its sustainability initiative, with staff and patients, but are not used in public
including green cleaning, in 2006. At Magee-Womens, areas. A spray bottle quaternary cleaner is used to
green cleaning is the balancing of sustainability with clean high tough surfaces in those rooms where
effectiveness against HAIs. It goes beyond the selection patients complain about the smell of bleach wipes.
of cleaning chemicals and includes other factors such as
• Green cleaners: The facility currently uses two
equipment, interior finish materials, and the amount of
Green Seal certified products—a neutral floor
packaging for cleaning products.
cleaner and a glass cleaner. However, there is no
green disinfectant available to clean up blood and
Green Cleaning Components body fluids. As a result, the facility uses a chemical
The green cleaning program at Magee-Womens disinfectant for that purpose.
includes several key components: Various levels of
cleaning for areas with different risk levels, use of green • Interior design that reduces the need for cleaning
cleaners, selection of flooring materials that need no and finishing or that facilitates cleaning: The facility
stripping and waxing, using cleaning machines that is switching from conventional VCT flooring that
require minimal chemicals, and use of micro-fiber mops, requires regular stripping and waxing to a type of
wood-looking linoleum sheet vinyl (luxury vinyl
• Cleaning for appropriate levels of cleanliness: The tile) which does not need stripping and waxing.
facility utilizes different methods to clean different
areas of the facility depending on the level of disin- • Cleaning equipment using minimal chemicals: A
fection and cleanliness required from an infection type of floor-cleaning machine (Tennant Eco-H2O)
uses electrically charged water to attract and remove
14 Green Cleaning in Healthcare: Current Practices and Questions for Future Researchdirt so that chemicals are not used. Micro-fiber mops Evaluation & Results
are extensively used in patient areas at Magee- Magee-Womens’ evaluation of a new cleaning prod-
Womens.The implementation of micro-fiber mops uct typically begins with requesting efficacy data and
was initiated from infection prevention concerns. MSDS from the vendor. The staff members from
When using conventional mops, it is required to environmental services and infection control depart-
change mop heads every 3-4 rooms, but this rule ments then evaluate the product’s advantages and
was not always followed by cleaning staff, posing a disadvantages. Sometimes, trials are conducted so that
significant risk of cross-contamination. When using front-line staff members can try out the products and
micro-fiber mops, one mop head is used in only one provide feedback. For example, before introducing the
patient room so that the possibility of transmission Eco-H2O machine, trials were conducted for several
of pathegens through contaminated mops is greatly weeks and the cost analysis provided by the vendor was
reduced. Further, the square shape of micro-fiber evaluated. The purchase was justified by the fact that
mops makes it easier to clean dirt from edges and the savings from using less quantity of chemicals may
corners, although it may take a little more time to offset the incremental cost of purchasing the machine
mop a room or an area. in the long run.
Implementation For Magee-Womens, some of the potential benefits
Magee-Womens’ green cleaning program aims at from the adoption of green cleaning practices include
providing a safe environment for everybody in the hos- the reduction of healthcare associated infections
pital, including patients, visitors and workers. The pro- and reduced complaints from staff and patients. The
gram is led by a hospital-wide green team, with strong Environmental Services manager at Magee-Womens
support from hospital leadership. The team consists of believes that the practice of changing micro-fiber mop
about 30 people from different departments—environ- heads between patient rooms significantly reduces the
mental services, dietary, facility, nursing units, educa- risks of infection. However, they have not conducted
tion, pharmacy, administrator, and office staff. The any research studies to evaluate this hypothesis. The
team’s monthly meetings usually focus on sustainability staff and patients used to complain about the offensive
issues reported from different departments. smell of flooring stripping and waxing. These com-
plaints have become minimal or non-existent after
One of the challenges encountered during the imple- switching to no-wax flooring. The measurements of the
mentation of green cleaning at Magee-Womens was effects of green cleaning could use certain data rou-
convincing staff to change from conventional string tinely collected by the hospital for other purposes, such
mops to the micro-fiber mops. For staff members, this as budgets for chemicals and infection rates. However,
was a significant change in daily practice. Major edu- the data have not been used to critically evaluate green
cational efforts, including meeting with vendors and cleaning efforts.
infection prevention and control personnel, helped to
change the old habits and obtain acceptance from staff. Questions for Further Research
Another challenge during the introduction of micro- Magee-Womens is interested in researching how effec-
fiber mops was justifying the extra costs in order to gain tive green cleaners are in killing germs and how practi-
support from the system-wide purchasing department. cal green cleaners are in the real world (for example,
The hospital does not have an in-house laundry service some cleaners need to sit on surfaces for more than15
to clean soiled mops. It turned out to be quite expen- minutes to effectively remove soils or kill germs, which
sive to have an outside company clean the micro-fiber is not considered to be practical in daily usage).
mops in its own facility and then deliver the clean
mops back to the hospital. A preliminary cost analy-
sis balancing the costs of micro-fiber mops with the
savings from reducing potential infections helped the
decisionmaking process. This was also facilitated by the
support from the administration.
Green Cleaning in Healthcare: Current Practices and Questions for Future Research 15Boulder Community Hospital, Boulder, CO
Boulder Community Hospital (BCH) is a 172-bed capillary action. This method ensures that a correct
general acute care hospital serving Boulder County in amount of cleaning solution is distributed. The satu-
Colorado. Environmental services at BCH is managed rated mop/cloth is used to clean floors and other sur-
by ARAMARK, an international company providing faces. The cleaning cloth can be folded so that there
environmental services as well as food services, facility are eight cleaning surfaces. In this way, fewer cloths
services, and transportation services. ARAMARK is are needed to clean the same amount of space.
responsible for cleaning a total of 593,000 square feet
• Interior design that reduces the need for cleaning
of space. At BCH, the term “sustainable cleaning” is
and finishing or facilitates cleaning. BCH’s inte-
preferred over “green cleaning.” It refers to cleaning in
rior design committee looks at the sustainability of
the most effective way to reduce the usage of environ-
interior design and selects materials that are easier
mental resources and reduce negative impacts on the
to clean (such as vinyl furniture) and flooring that
environment, community, patients, and staff.
needs less frequent or no finishing, stripping, and
waxing.
Green Cleaning Components
The main components of sustainable cleaning at BCH
include: Proper cleaning levels in different areas, green
Implementation
Sustainable cleaning at BCH is a system-wide effort
cleaners, micro-fiber mops and cloths, new methods
(including outside vendors) led by a sustainability
of dispensing and applying cleaning solutions, and
committee consisting of 12 members from facility
interior finish materials that are easy to clean or require
management, nutrition, hospital administration, nurs-
low maintenance.
ing, purchasing, clinical and clerical departments. It
• Cleaning for appropriate levels of cleanliness: is implemented with ARAMARK’s SpaceCare QL
Different cleaning products and procedures are used program, which was developed as a best practice system
according to the risk levels of cross-transmission of of cleaning tools, techniques, and procedures for the
infections in various areas. For example, a light duty improvement of efficiency of environmental cleaning
green cleaner is used on floors, except for operating in healthcare. As a simple example of the SpaceCare
rooms, where a disinfectant is used. The environ- QL approach, stocking most frequently used tools, such
mental services staff regularly cleans windows, blinds as gloves, at a standard spot on top of the housekeeping
and carpets in the office area. However, office occu- carts has been found to improve efficiency.
pants clean their work spaces so that the amount of
work by the cleaning staff can be reduced. Regular training and education has been an impor-
tant factor in implementing sustainable cleaning.
• Green cleaners: BCH uses cleaners designed by
Sustainability coaches at ARAMARK provide coach-
Ecolab for ARAMARK, which has strict require-
ing to facilities. The head of the BCH environmental
ments regarding cleaners. All cleaners except for
services department goes through formal training
disinfectants are green products. A chemical solu-
provided by ARAMARK every three years and then
tion distribution system is used to reuse bottles to
trains his managers, supervisors, and staff. Supervisors
reduce waste.
conduct daily rounding to observe cleaning perfor-
• Cleaning tools or equipment that use less water and mance and provide feedback and coaching to clean-
chemicals. BCH was among the first hospitals to use ing staff. The inspection-training tour is essential for
Eco-H2O machines that use ionized water to clean maintaining the quality of environmental cleaning.
floors. Micro-fiber mops and cloths are used to save During the coaching process, the supervisor typically
on water and chemicals. demonstrates the correct cleaning procedure once, asks
the staff member to perform in the same manner twice,
• Application and dispensing methods. Instead of
and then asks the staff member to teach the procedure
spraying, cleaning solution is contained in a bucket
back to the supervisor.
and directly applied to mops and cloths through
16 Green Cleaning in Healthcare: Current Practices and Questions for Future ResearchYou can also read