HOW CAN GOOD RESULTS BE EVEN BETTER? - (Part 1) - RCPCH
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
THE SAHLGRENSKA ACADEMY HOW CAN GOOD RESULTS BE EVEN BETTER? (Part 1) NATIONAL PAEDIATRIC DIABETES AUDIT ANNUAL CONFERENCE 2020, JANUARY 17 HOLIDAY INN, REGENTS PARK GUN FORSANDER, ASSOCIATE PROF THE QUEEN SILVIA CHILDRENS HOSPITAL SAHLGRENSKA UNIVERSITY HOSPITAL GOTHENBURG SWEDEN
THE SAHLGRENSKA ACADEMY DISCLOSURE I HAVE RECEIVED LECTURE HONORARIES FROM LILLY, NOVO NORDISK, SANOFI, RUBIN-MEDICAL
THE SAHLGRENSKA ACADEMY
Examples of ongoing work to improve quality of
pediatric diabetes care …
• Internationally; Sweet Study, ISPAD
• Nationally; Swediabkids, IQ-project
• Locally; Policy paper, the Angered
project
Picture: Edvard Munch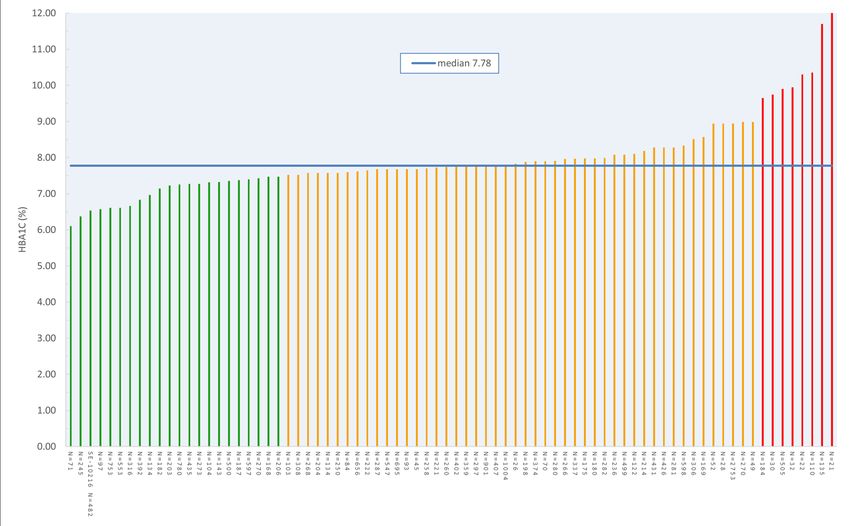
THE SAHLGRENSKA ACADEMY Common treatment targets for a child with diabetes • A high quality of life - both now and for the future • Normal mental and physical growth • No DKA and severe hypoglycaemia • No long-term complications
THE SAHLGRENSKA ACADEMY Were all the problems solved one hundred years ago when the access to insulin treatment appeared? • A lack of insulin is still globally the most common reason behind death in children with diabetes • Insulin is no cure, only a life-supporting treatment • During the decades after introducing insulin treatment 1922, the complications of the disease were shown • The question araised: does the way how the insulin treatment is implemented influence the risk for cardiovascular complications?
THE SAHLGRENSKA ACADEMY
Complications must be avoided-
also of monitary reasons:
• Diabetes complications causes at least 80 % of the diabetes
related costs in society
… must more than insulin, CGM, insulin pumps etc…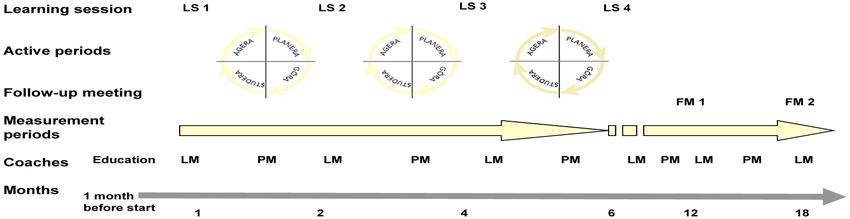
THE SAHLGRENSKA ACADEMY
)
Summary of consensus definitions
Diabetes Care 2017 Dec; 40(12): 16221630. https://doi.org/10.2337/dc17-1624
Outcome Definition
Level 1: glucose 250 mg/dL
(13.9 mmol/L)
Percentage of readings in the range of 70–180 mg/dL
Time in range
(3.9–10.0 mmol/L) per unit of time
Time in target 3.9-7.8 mmol/l (70-140 mg/dl)
Elevated serum or urine ketones (greater than the upper
DKA limit of the normal range) and serum bicarbonate
THE SAHLGRENSKA ACADEMY
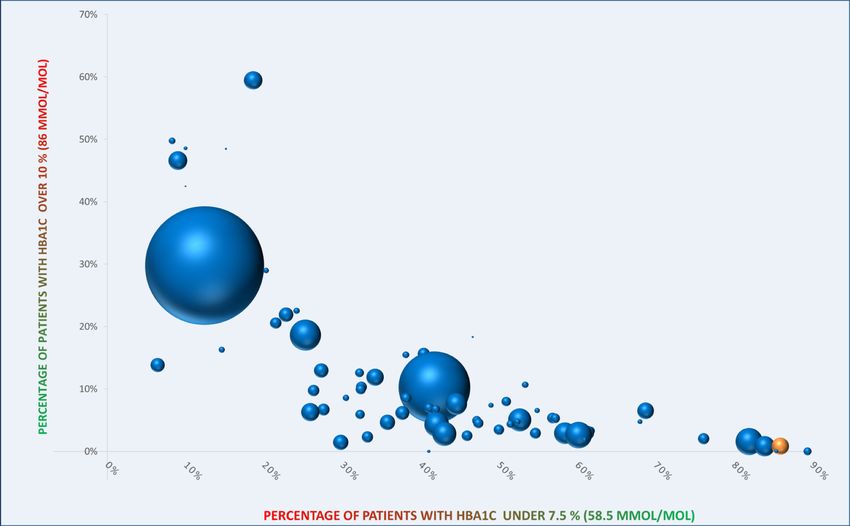
Well and insufficiently controlled patients
all centres, 01/01/2018 - 31/12/2018
- the width of the bubble represents the size of the centre
- yellow bubble: your center
- minimum requirement: 50 patients
8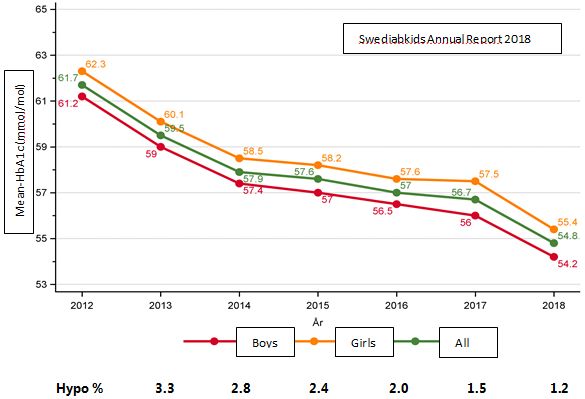
THE SAHLGRENSKA ACADEMY
HbA1c: standard, median of patients’ medians
T1DM, 0-18y, 01/01/2018 - 31/12/2018
STANDARDIZED:
mathematical correction of the HbA1c-values: HbA1cSTANDARDIZED = (HbA1c-RAW / mean HbA1c of your lab-
method) x 5
Median of patients’ medians: first calculate the median per patient per period, then the median of these medians
Number of patients must be at least 20 for being displayed.
9
THE SAHLGRENSKA ACADEMY
BMI-SDS: T1DM, patients 0-18y, WHO 2007reference
01/01/2018 - 31/07/2018
10
N = number of patients with a calculated BMI standard deviation score(SDS)
Based on the mean of the patient’s medians (every patient with a calculated SDSvalues contributes with onemedian.THE SAHLGRENSKA ACADEMY Some national Swedish diabetes quality initiatives and results Painting by E Munch
Swedish National Pediatric Diabetes Registry • Incidence of type 1 diabetes is 45/100 000 in children below 18 years of age • Second highest incidence in the world • Almost everyone diagnosed with diabetes is included in the registry • All 42 pediatric clinics that treat children with diabetes report data
THE SAHLGRENSKA ACADEMY https://swediabkids.ndr.nu
THE SAHLGRENSKA ACADEMY
The Button A push of a button for improvement
work NDR.nu
”Knappen”
The Button
with results from
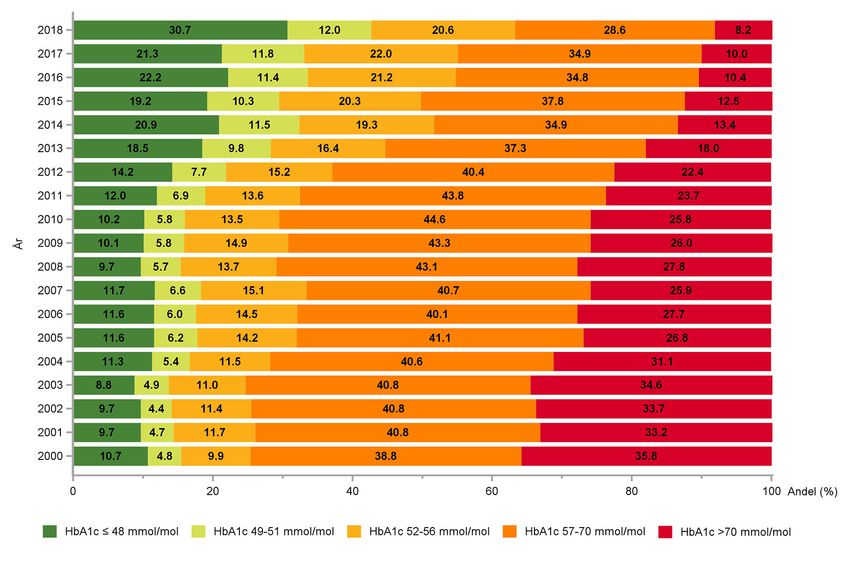
all of SwedenHbA1c ≤ 6.5% HbA1c ≤ 6.6-6.8% HbA1c ≤ 6.9-7.3% HbA1c ≤ 7.4-8.6% HbA1c > 8.6%
ISPAD 2019 KarinISPAD 2019 Karin Åkesson
% Proportion CGM users, %
AgeProportion pump users, %
%
AgeTHE SAHLGRENSKA ACADEMY
Effective team work
Study of Swedish pediatric diabetes clinics via
• Higher compliance with guidelines
• SWEDIABKIDS
Clear message of lower HbA1c-goal
• Well functioning teams
Five centers were selected:
• Lower proportion of diabetes specialist educated team members …
• lowest/
Shorter highest/largest
professional working time … decrease center regarding mean value
• of HbA1c
Engaged team members with a positive attitude
• Higher mean insulin dose
Team members were asked to fill out questionnaires:
• Larger diabetes center
Structure, Process and Policy
• “Team members’ policy and approaches affect glycaemic control in children and adolescents.
Team members need to be aware of their approach and of the importance of using resources
within the team”.
L Hanberger, Diabetes Res Clin Pract, 2012THE SAHLGRENSKA ACADEMY
Insulin dose
Compliance to guidelines at HbA1c levels Process
above target value
Centre size
Team size
Structure
Years of diabetes experience
Specific diabetes education
HbA1c target value Policy
The national Swedish HbA1c target at the time of the study wasTHE SAHLGRENSKA ACADEMY Effective team work with lower HbA1c values were characterized by: • Higher compliance with guidelines • Clear message of lower HbA1c-goal • Well functioning teams • Shorter professional working time (!) • Engaged team members with a positive attitude ISPAD 2019 Karin Åkesson L Hanberger, Diabetes Res Clin Pract, 2012
THE SAHLGRENSKA ACADEMY
As a consequence of this study, a new national project was
launched …
… The IQ-project!THE SAHLGRENSKA ACADEMY
Improving the quality of Swedish pediatric diabetes care
• Initiative taken by the steering group of SWEDIABKIDS
• Improvement would be reached by changes in work processes and not by an increased
work load
Peterson A, PLoS One 2014;9:e97875.THE SAHLGRENSKA ACADEMY
Improving the quality of Swedish pediatric diabetes care
• Initiative taken by the steering group of SWEDIABKIDS
• Improvement would be reached by changes in work processes and not by an increased
work load
• Learning sessions included lectures on improvement methods, teamwork and learning,
and sharing data and ideas
• In the intervals between the learning sessions, the team identified problems and
improvement areas at their centres, created action plans, tested effect of changes, and
followed up on the results
Peterson A, PLoS One 2014;9:e97875.THE SAHLGRENSKA ACADEMY
Improving the quality of Swedish pediatric diabetes care
• Initiative taken by the steering group of SWEDIABKIDS
• Improvement would be reached by changes in work processes and not by an increased
work load
• Learning sessions included lectures on improvement methods, teamwork and learning,
and sharing data and ideas
• In the intervals between the learning sessions, the team identified problems and
improvement areas at their centres, created action plans, tested effect of changes, and
followed up on the results
• Outcome variables were clinical, and included HbA1c, severe hypoglycemia
(unconsciousness, seizures) and DKA
• The process measures were documentation of smoking habits and the degree of physical
activity
Peterson A, PLoS One 2014;9:e97875.THE SAHLGRENSKA ACADEMY
IQ project
LM = Lunch Meeting, PM = Phone Meeting
ISPAD 2019 KARIN ÅKESSON Peterson A et al, PLOS, 2014THE SAHLGRENSKA ACADEMY
Tools
• Problem inventory
• 5P (Purpose, Patients, People, Process, Patterns)
• Clinical value compass Changes that
lead to
• Flow charts improvements
• Activity plans
• PDSA-wheel
(Plan, Do, Study, Act)
• 12-14 diabetes teams at
each course
Ideas, theoriesTHE SAHLGRENSKA ACADEMY
Fishbone diagram used in the IQ project
External collaboration
Staff
Structure of team meetings Day care / School
Attitudes to the team work Social service
Large turnover of dieticians Child Psychiatry
Vague guidelines from the team Pharmacy
Update of local policies and guidelines
Insufficient education of the staff Decrease
HbA1c
Different ability to cope The patients
with the disease lack tools 100 /500-rule
Unmotivated to meet Education about Clarify the leadership of
with dietitian late complications the team
Forgets insulin More pumps Revise the care plan?
doses Clarify the care plan for the patient
Talk about blood glucose, Adherence to
Too few blood
not HbA1c! the care plan?
glucose tests
Age Group meeetings
Patient Self-care Care plan
Patient educationTHE SAHLGRENSKA ACADEMY
What were the project ideas of the individual teams
about?
Examples:
• Frequent visits if high HbA1c
• Carbohydrate counting from onset
• Increased use of CGM and pumps
• Increase the proportion of patients with
HbA1c < 57 mmol/mol
• Reduce proportion HbA1c > 70 mmol/mol
• Lowering target HbA1c to < 52 mmol/mol
• No increase in severe hypoglycemia
Peterson A, PLoS One 2014;9:e97875.
Samuelsson U. Pediatric Diabetes 2016You can also read