IGA News Summer 2018 - Patron: Dame Maggie Smith - International Glaucoma Association
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
IGA News
Summer 2018
Patron: Dame Maggie Smith
Contents GDPR Page 1 Letter from the editor Page 2 Chief executive news Page 5 Letters, emails and comments Page 9 News Page 4 Talking glaucoma Page 23 Research recruitment Page 40 Sightline Page 46 Experience Page 53 Awareness Page 57 Fundraising Page 61 A day in the life... Page 62 Support groups Page 65 INTERNATIONAL GLAUCOMA ASSOCIATION Woodcote House,15 Highpoint Business Village Henwood, Ashford, Kent TN24 8DH Sightline: 01233 64 81 70 Administration: 01233 64 81 64 Email: info@iga.org.uk Website: www.glaucoma-association.com Editor: Karen Brewer Sub-editor: Tracey Fabre Design/artwork: Yes Design Printed by: Fuller Davies Ltd Charity registered in England & Wales No. 274681, in Scotland No. SC041550 Cover image: Highlighting the IGA’s new Online Book

GDPR
Data protection at the IGA
Following the recent introduction of the General Data Protection Regulation, or
GDPR, we wanted to give our members a quick overview of how we use your data.
We use the information provided by you in a number of ways, for example
• To provide you with information or advice that you’ve asked for,
or to manage a booking for an event like our Annual Lectures
• To carry out a contract between us, or to ensure we know how you
prefer to be contacted
• To process donations and legacies, or to tell you about services and
activities, campaigning, fundraising and appeals for donations
• To seek your views so that we can improve our services or represent
your views to external bodies like NICE
Our legal basis for processing your information
• Where you have provided information to us for the purposes of
requesting information or a service, we proceed on the basis that you
have given consent to us using the information for that purpose.
• We need to hold and use your information so that we can carry out
our obligations under a contract entered into with you
• It is necessary to comply with our legal obligations, for example
processing records relating to Gift Aid or VAT.
• We may also rely on the fact that it is necessary for your legitimate
interests that we provide the information or service requested.
Full details of how we record and use your personal data can be found in our
new Privacy Policy, and if you would like more details please don’t hesitate to
get in touch. You can change the way we contact you at any time, by calling us on
01233 64 81 64 or by emailing info@iga.org.uk
News Summer 2018 1
Letter from the editor
hear directly from you about how
delays and cancellations have affected
you and your vision. So, please take
the time to read more about this on
page 12 and find out how you can
make your voice count.
The All Party Parliamentary Group
for Eye Health and Visual Impairment
also published its recommendations
on 6 June. IGA representative
Chris Wall was heavily involved in
influencing the recommendations
contained in this document. A list
of the recommendations is included
on page 14 and more information
Welcome to your summer magazine. is on the IGA website.
There is so much to report since the Breakthrough research brings us
last issue and there is good reason closer to identifying the genetic
why we have brought this issue characteristics of people with
forward one week. glaucoma. This could play a key role
in channelling resources to those
At the time of writing we were most at risk. At the time of writing
awaiting further news about the the NHS was soon due to publish a
deadline for an important NHS report about ophthalmology
consultation into the pricing for services, with recommendations
ophthalmology appointments (and that leaders could take to minimise
other conditions). The consultation the risk for those at significant
was due to be published in the first harm of sight loss.
week of June, lasting for 28 days. We
need to change the pricing structure A number of you were able to
which financially disincentives follow- make it to our AGM and annual
up appointments. We know from our lecture this year. For those who
Members’ survey 2017 that this is an weren’t able to attend, I have
issue that many of you have struggled included a report given by Karen,
with. NHS Improvement is keen to our Chief Executive and a report
2 News Summer 2018
Letter from the editor
from our guest speaker and dry eye syndrome. This issue
Professor Keith Martin. carries a report from Sightline about
the condition, and our awareness
The involvement of our members week focused on what people
in research is second to none. should be aware of if they have
I have had repeated thanks from both conditions.
researchers who have been surprised
and pleased by the uptake to I am delighted that a number of
requests carried in this magazine. you have got in touch to share
You will see that this issue includes a your news and stories. The help
request for members to help with that you provide each other is
understanding how glaucoma impacts invaluable. To further support
on functional vision page 40. this we have launched an online
book on our website which
The DVLA are also keen to have allows you, or family members
your views and are asking for you to to share experiences.
provide feedback on the letter that
you will receive following We seek to inform, support and
your licence renewal page 44. raise awareness through many
channels including social media
I hope that some of you will have and have active Facebook and
seen our campaign around Ramadan. Twitter sites which pick up on
We have known that there was an interesting news and provides
issue with people not taking eye comment where necessary.
drops during Ramadan, believing that
this breaks the fast. We were We are delighted that we have new
pleased to work with the Muslim trustees who are helping with the
Council of Britain to provide an governance of the IGA and new
educational message about how staff who are committed to
and when eye drops can be taken. supporting people with glaucoma.
This campaign was picked up by More information is included on
the BBC, The Times, online media pages 19-22.
and carried further through our
corporate partners. Finally, but by no means least, we
have been hugely busy in contacting
We are also seeking to support people about what they want to
more people with both glaucoma receive from the IGA and recording
News Summer 2018 3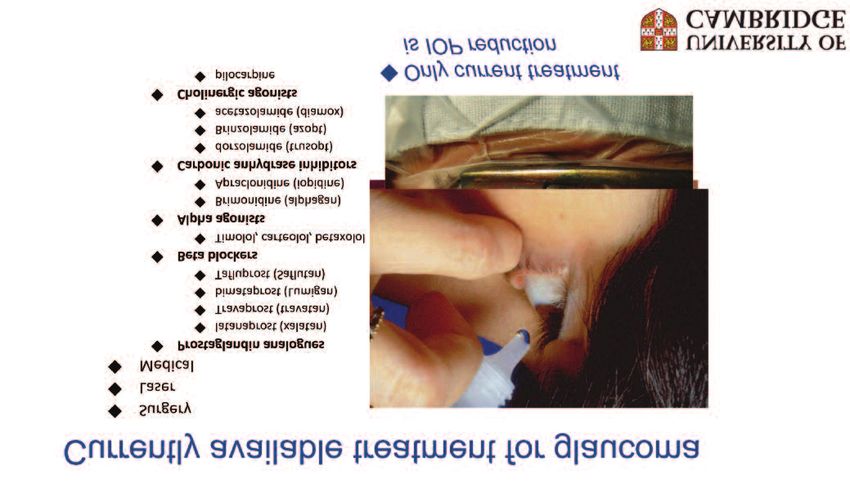
Letter from the editor this, so that we are not in breach of the Government’s General Data Protection Regulation (GDPR) rules. Please do take the time to read and respond to any correspondence that we send you. Thank you for your involvement in the magazine. I do try and reflect what has been raised during the last few months. I know that more information is needed to help you understand the differences between treatments, including risks and complications and plan to do more around this. As always, do keep in touch. Karen Brewer Editor 4 News Summer 2018

Chief executive news
#2 - Eye drops
As you know, dry eye syndrome was
the main focus for National
Glaucoma Awareness Week, and we
hope to make ocular surface disease
more central to some of our patient
support group meetings too.
Compliance remains a problem, but
people very rarely call the helpline
because they’ve got compliance
problems, rather it’s because they’re
experiencing side effects, or there
are issues with availability, which has
been a problem with some products
Dear all over the last year.
At our recent AGM I ran through But we know compliance is an
some of the things that are on our issue so we’ll continue our
radar for the year ahead, and I awareness raising and education
thought it might be useful to share work, and encourage consultants,
them more widely here. I started nurses, optometrists and
by talking about the top five reasons pharmacists that they all have
that people call our helpline, so a part to play.
here goes:
#1 - Surgery and laser queries #3 - Lifestyle queries
Questions and worries about A wide and varied range of
treatment has been top of the list for questions about lifestyles, hobbies,
some years now, but we are seeing a diet and more. There is a real
growth in complex enquiries, leading appetite among members to take
to longer call times, and half an hour active steps to improve their eye
or even hour-long calls aren’t unusual health, and people are looking for
now. Our Buddy service really helps lifestyle and diet changes that may
with these treatment worries and help. Sadly there is no magic bullet,
we’d love to expand this support in but we’ll try and bring you news and
the year ahead. advice as and when we can…
News Summer 2018 5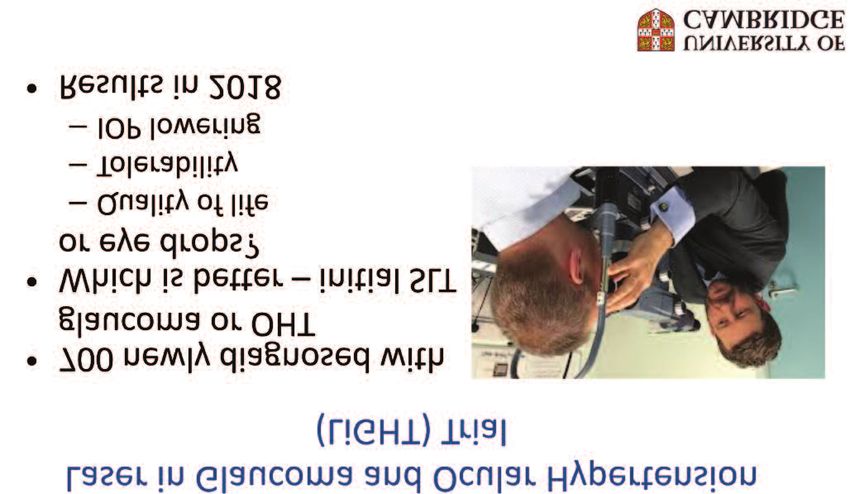
Chief executive news
#4 - Driving continues to the case for the majority of
be a concern glaucoma patients. We made the
We continue to raise your issues point that patients called for
with the DVLA and hope that this follow-up are statistically more likely
benefited you at a time when you to have sight threatening pathology
needed help. We meet every six than new patients: they need to be
months with the DVLA so please seen at regular intervals appropriate
keep on sending us your views. to the severity of their condition and
their lifetime risk of visual loss as
determined by clinicians.
#5 - Delayed appointments
This wouldn’t have been in top five We also made the point that the
even 18 months ago but it is fast significant reduction in payment
becoming a major concern for for follow-up visits has a
members. We produced a new detrimental impact on services,
advice leaflet in response and we’ve because patients with conditions
had good feedback about it, but like glaucoma, may be discharged
we’re starting now to hear from back to general practitioners with
people who’ve tried all the avenues a recommendation that they be
we can think of and are getting referred back in six months because
nowhere, so obviously more help is the proposed tariff will not cover
needed and we’re thinking what we the full cost of follow-up visits.
can do in response. Realistically this will lead to patients
with potentially blinding conditions
being lost to follow-up, as well as
NHS Tariffs simply moving the burden of care
Linked to appointments, we recently around the health system.
wrote to NHS England to express
concern about how outpatient tariffs An IGA patient representative
affect glaucoma patients. The was invited to meet with NHS
National Outpatient Tariffs for England in late May.
2017-19 introduced the concept of
dis-incentivising follow ups, and we
told NHS England that this Editor’s note:
discriminates against patients who More information about NHS
need long term or lifelong follow-up Tariffs and how you can make
to prevent avoidable sight loss, as is your voice heard is on page 12
6 News Summer 2018
Chief executive news
What else will the IGA be To date more than 2,600 staff have
facing in the next year or two? done the training and are proudly
One thing seems fairly certain – wearing IGA lapel badges to show
more people will be getting they passed.
glaucoma and there will be more
people out there who need our help. I was talking to a Specsavers
optometrist recently, and she
So, awareness raising and went to lengths to comment on
profile raising will be key in the the difference it has made to the
coming years, as will effective knowledge and confidence of the
impact measurement and staff in her practices, which is
economic efficiency. very heartening.
With that in mind we’re really We also worked with Vision Express
pleased with the outcomes of our and our staff have attended a
relationships with corporate number of events to raise awareness
partners too. I think it’s fair to say of glaucoma, to accompany their new
that there was – quite rightly - some Vision Van when it visited community
hesitation in developing new venues offering free eye tests.
partnerships with large commercial
organisations when we were looking This Vision Van work led to the
at these some 12 or 16 months ago, partnership being shortlisted for
but we’re delighted with the impact the Business Charity Awards 2018,
this has had. which resulted in some great
publicity for us, even though we
To give you a couple of examples, weren’t the winner.
I hope some of you saw the IGA
branding on Specsavers adverts
during World Glaucoma Week
(WGW) which took place in March.
In the run up to WGW we worked
with Specsavers to develop an online
glaucoma training programme for
their front of house staff –
non-clinicians.
News Summer 2018 7
Chief executive news We’ll also be looking at technology in the next couple of years and thinking about how we use technology to support people. We know there’s widespread digital exclusion among older people and those with sight loss, but this is changing fast, and in a few years I expect that a significant number of people will want to access support and information in different ways, so we need to start looking at things like live chat on our website as well as (not instead of) a telephone helpline, and at virtual support groups as well as traditional face to face groups. I hope that has given you a better understanding of some of the work and challenges ahead. I will be in touch with other news in future copies of the magazine. Karen Chief Executive 8 News Summer 2018
Letters, emails and comments
A member wrote to us asking for clarification around reporting to the
DVLA. This member has glaucoma in both eyes, but with no visual field
defect in the right eye.
As our leaflet states, you only need to report to the DVLA if there is
visual field defects in both eyes. It is worth all members asking their
ophthalmologist about the visual field loss that they have, as this has a
bearing on whether the DVLA require further investigation.
If in any doubt though, do report to the DVLA. It is easy to do this online
by visiting: www.gov.uk/report-driving-medical-condition or for a
short link: bit.ly/2GZPXWe
The IGA sought confirmation about this from the DVLA. Here is an
extract taken from the minutes of the Drivers’ medical group in
March, 2014:
“Panel discussed the diagnosis of glaucoma and noted that this condition
is now sometimes diagnosed in the absence of visual field loss because of
improved diagnostic techniques. Group 1 drivers with glaucoma should
notify DVLA if, in the clinical judgement of a clinician, the driver has a
glaucomatous visual field defect in both eyes. Group 2 drivers should notify
DVLA if they have a diagnosis of glaucoma in one or both eyes.”
Please go ahead with promoting my story if it seems helpful to others. I'm
more than happy for my story to be out there to help people become more
aware of the need to think about eye health and get tested. Only today I was
talking to a young lady whose parents hadn't had an eye test for years. I was
encouraging her to get them to have tests. Dawn Carrington.
(Editor’s note: Dawn’s story is included in the magazine).
News Summer 2018 9Letters, emails and comments
Dear Patricia
I am writing to thank you so much for all the help and advice you gave me
over the phone on Monday afternoon.
It was lovely to speak with someone who was so sympathetic and so
understanding. I had only been diagnosed with glaucoma since the end
of February and I was anxious and yes, a little frightened.
At the hospital there was no one to speak with and they were so matter
of fact. I know that they are very busy but just one kind word would have
been appreciated.
I took your advice and rang the secretary of the consultant that I was
supposed to see in July, as you said that was too long to wait. I told her that
I had spoken to your Association and at first she said I don’t think we can put
you in anywhere, then suddenly she said wait a minute, yes, I can put you in on
Wednesday 30th May. I could hardly believe it. She was then very pleasant
and said what a really nice consultant he was and I would be fine seeing him.
Patricia, this was a great weight off my mind as the appointment is six weeks
earlier than the other appointment in July. I really appreciate how you
helped me and today is the first day that I have enjoyed myself and felt more
like my old self. Many many thanks and I will let you know how things go
after my appointment.
With my very best wishes
Olive
10 News Summer 2018Letters, emails and comments
Dear Karen
I am writing to thank you all your help with my research study. Today I have
received the IGA news and I would like to let you know that I am having
many volunteers thanks to your association.
I will share with you the results obtained as soon as possible.
Dr Nery Garcia Porta, OD, MSc, PhD
Marie-Sklodowska Curie Individual Fellow
Vision and Eye Research Unit
Anglia Ruskin University
Please feel free to write to me:
K.brewer@iga.org.uk or call on 01233 64 81 64
I will consider all thoughts and comments, and come back to you
News Summer 2018 11News Editor’s introduction: At the time of writing, we were expecting the NHS to announce a consultation into NHS Tariffs in England (see pages 2 and 6). This is such an important issue for our members’ to respond to that we took the unusual step of fast-tracking your Summer IGA News, and bringing it out early so that you have at least two weeks to respond. The consultation is about the pricing for appointments for ophthalmology (and other conditions). It was due to be published in the first week of June and last for 28 days. The article below explains more. The IGA will be submitting a response on behalf of members’ but we want YOU to act. NHS Improvement is keen to hear directly from patients about how delayed and cancelled appointments have affected you and your vision. It appears that when the last Tariff consultation took place, the views of eye care professionals and patients was largely absent. Let’s change that. Your help is needed NHS Tariffs for review patients by Christine Wall In April 2018, Professor Bloom and the IGA Trustees wrote a letter to the Secretary of State for Health, the Chief Executive of National Health Service England (NHSE) and others. In it, they expressed their grave concerns about the NHS tariffs which dis-incentivises follow-up appointments and how this severely disadvantages glaucoma patients. The Trustees added that the burden of glaucoma rises as our population ages and the number of people adversely affected by the current tariff system is a cause for real concern. The IGA urged NHSE to consider this evidence when reviewing outpatient tariffs and to act to address the inequity and inefficiency in the current system. The current tariffs are now being reviewed and Christine Wall [IGA patient representative] made contact with NHSE and National Health Service Improvement (NHSI) to express her concerns. A meeting was organised between her, another patient, Rea Mattocks, and Helen Laing, Director of Operations and Clinical & Sector Relations NHSI and Rob Unsworth, Head of Pricing Strategy NHSE. This meeting took place on 25 May 2018. Chris opened the meeting by describing the dismay of eye patients at the very disadvantageous 2017 Tariff settlement, which impacted on the frequency of patients’ review/return visits. This, in turn, has led to needless loss of vision. Chris and Rea emphasised the seriousness of failing vision, including the impact on patients’ day to day lives, associated mental health issues, the impact on general health and wellbeing and on a 12 News Summer 2018
News
patient’s‘ ability to continue contributing to society. Patients are finding it difficult to be
seen by the right doctor, at the right time, in order to prevent further sight loss.
Chris and Rea went on to explain the challenges
facing eye patients with a lack of capacity in the
Its purpose is to seek eye sector, the disincentives of the NHS tariffs
feedback from the sector for follow-up patients and the cuts of £7.5m to
via an on-line pro-forma. the research budget, leaving eye patients feeling
that ‘no-one cares’ about them. The whole eye
The feedback exercise
sector (patients, charities, NHS staff,
will last for only 28 days optometrists) is concerned about the inequity
in funding for eye health.
Chris referred to the recent APPG report “See the light - improving capacity in NHS eye
care in England”, (see the IGA website) which recommends “urgently reviewing the
National Tariff for Ophthalmology” because of its serious impact on patients, particularly
those with glaucoma, wet AMD and diabetic retinopathy who require follow-up as they
are at early risk of avoidable sight loss.
Helen Laing and Rob Unsworth outlined the programme for the “Tariff Engagement
Document” (TED) for 2019 which is due to be published in the first week of June 2018.
It will contain initial ideas around the next set of tariffs and the associated payments.
Its purpose is to seek feedback from the sector via an on-line pro-forma. The feedback
exercise will last for only 28 days.
However, Helen and Rob emphasised that they would most like to hear from patients
about their journeys and the direct impact of the tariff changes on them; from patient
organisations about their experience of the payments and how these have affected their
members and from professionals about both the payments and wider issues. The
pro-formas can be completed, but patients and patient organisations in particular may
want to write or email their concerns. Direct evidence is encouraged such as a letter
from a patient who can say “I absolutely need to be seen as a review patient because…”
or “this is what happened to me because I could not get a follow-up appointment …”
Helen and Rob emphasised that this evidence from patients would be taken fully into
account, and would count for a great deal.
Following the meeting, Chris and Rea felt that significant progress had been made in
putting the needs of eye departments and patients firmly back on the map. There really
is absolutely everything to “play for” regarding 2019 Tariffs. It is hoped very much that
patients will respond to the TED by describing exactly how much they need regular
review by sharing their experiences and fears.
News Summer 2018 13News The All Party Parliamentary Group on Eye Health and Visual Impairment launch report and recommendations The IGA supported the recommendations included in this report. More information is available on our website. The recommendations to the Secretary of State for Health and Social care: 1. To include eye health specifically within the NHS England mandate to ensure it is accorded a higher priority. For NHS England: 2. To review and report publicly on how eye care capacity issues are addressed in sustainability and transformation partnership plans (STP’s) and how these relate to current and predicted need. 3. To bring ophthalmology fully within the NHS transformation programme whilst adequately funding service redesign. 4. To appropriately resource and support Local Eye Health Networks within STPs and Integrated Care Systems to drive improvement. 5. With NHS Digital, to implement routine data collection in ophthalmology departments on waiting times for follow-up appointments, delays to follow-up outside clinically recommended timescales, patients lost to follow-up and consequences. 6. To urgently review the National Tariff for ophthalmology which currently seriously disadvantages some patients with glaucoma, wet age-related macular degeneration (AMD) and diabetic retinopathy who require follow-up appointments and are particularly at risk of avoidable sight loss. 7. To establish a national target to ensure patient requiring follow-up appointments are seen within clinically appropriate times to prevent dlayed and cancelled appointments resulting in patients lost to follow-up. 8. With NHS Digital, to urgently implement IT-connectivity between community optometry and the wider NHS to improve patient care and efficiency. 14 News Summer 2018
News
For the Department of Health and Social Care with the Medicines
and Healthcare products Regulatory Agency
9. To review regulations to ensure that necessary amounts of drugs are dispensed,
stored and available in theatre and outpatient treatment rooms in advance of the
day’s list for treatment.
For Local Authority and Clinical Commissioning Groups
10. To review the eye health needs sections of their Joint Strategic Needs Assessments
to ensure consistency, to assess current and future eye health needs.
For Clinical Commissioning Groups
11. To establish separate ophthalmology contracts with NHS providers from April 2019
to ensure there is a public transparency about funding invested in eye care and how
this correlates to assessed need in Joint Strategic Needs Assessments.
For NHS providers
12. To ensure the eye care pathway is clear for those responsible for managing patient
care and effectively communicated to patients.
13. To review booking procedures to ensure patients who need further appointments
can book their next appointment, within clinically appropriate timescales, before
leaving the clinic. This will benefit patients and aid capacity planning.
For Health Education England
14. To urgently increase the number of trainee ophthalmologists.
15. To review the curricula of medical training institutions to ensure a minimum
standard of eye health education is included, in agreement with the Royal College
of Ophthalmologists.
16. To build on strong support from all relevant professional bodies for consistent
learning outcomes from curriculum and training systems for ophthalmic
professionals such as optometrists, opticians, nurses and orthoptists.
News Summer 2018 15News NHS England Elective Care Ophthalmology High Impact Intervention programme At the time of going to print the NHS England was due to publish its Elective Care Ophthalmology High Impact Intervention programme. This programme will focus on prioritising ophthalmology services and will describe the actions that leaders should take to minimise the risk of significant harm to those patients most at risk of sight loss, due to chronic eye conditions and delays to follow up. It will be published on the NHS website. www.england.nhs.uk/elective-care-transformation or for a short link: bit.ly/2k6dQ4k Researchers identify genetic variants that may predict glaucoma risk A study led by scientists from King’s College London, University College London, Massachusetts Eye and Ear and Harvard Medical School has identified 133 genetic variants that could pave the way for a genetic-based screening program to help identify the world’s leading cause of incurable blindness. The breakthrough represents a major advance in the fight to tackle the degenerative condition, which has virtually no symptoms in the early stages and affects 480,000 people in England and millions worldwide. To better understand the development of glaucoma, scientists studied 140,000 people drawn from the UK Biobank and EPIC-Norfolk. Eye pressure readings were taken which were compared with a DNA analysis of each patient to assess how likely it was that they would develop the condition. Elevated pressure in the eye is the most important risk factor for glaucoma and is created by the continual renewal of fluids within the eye. By comparing the pressure test results with a genetic analysis of the many common, small variations in DNA that contribute a tiny amount to overall eye pressure, the team was able to identify 133 genetic variants in the DNA of those who had high pressure readings, 16 News Summer 2018
News and so were at highest risk of developing the condition. The genetic variations were able to predict whether someone might develop glaucoma with 75 per cent accuracy. Lead author, Dr Pirro Hysi from King’s College London, said: “Knowing someone’s genetic risk profile might allow us to predict what risk of glaucoma he or she carries so that in the future we can focus scarce health care resources on those most at risk.” By understanding how glaucoma develops we can, in time, get ahead of the curve of the condition and support both those living with the disease and those who may develop it. Co-author Dr Anthony Khawaja from the NIHR Biomedical Research Centre at Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology, said: “With this new knowledge, we are now more able to predict the risk of an individual developing glaucoma. The predictive genetic markers could be measured as early as birth, even though glaucoma develops later in adulthood. “These results help us to better understand the previously unknown mechanisms that cause this damaging disease. By understanding how glaucoma develops we can, in time, get ahead of the curve of the condition and support both those living with the disease and those who may develop it.” Dr. Janey Wiggs, co-author from Massachusetts Eye and Ear and Harvard Medical School said, “This study demonstrates the enormous power of large datasets allowing detection of these important genetic risk factors. “Glaucoma remains the leading cause of incurable blindness in the world, but the hope is that this important piece of research could help millions by leading to faster and more accurate diagnoses in the future.” News Summer 2018 17
News The GOC has published some high level findings from its Education Strategic Review concepts and principles consultation. The summary shows 97 per cent of respondents agreed with the development of new education standards for optometrists and dispensing opticians. 82 per cent agreed with embedding clinical experience progressively from the start of education programmes. Stakeholders also showed support for the GOC further informing its education requirements with its Standards for Practice for Optometrists and Dispensing Opticians, with 84 per cent in favour of embedding professionalism into education and training programmes. GOC Chief Executive and Registrar, Vicky McDermott said: “We are delighted to have received many supportive responses to the consultation that will enable us to work at pace to develop our detailed proposals to equip future professionals with the skills, knowledge and behaviours needed to practise safely and competently in a changing sector. “We will make concerted progress in the coming months to transform these concepts into workable approaches for the future.” The GOC’s Education Strategic Review concepts and principles consultation ran from December 2017 to March 2018, comprised 21 questions and sought feedback on 11 concepts and principles. A total of 36 responses were received to the consultation, 26 from organisations and 10 from individuals. The GOC has also commissioned a full independent analysis of the consultation feedback and will publish this separately. To read the high level findings summary please visit: bit.ly/2k2I6go 18 News Summer 2018
News Two new trustees join the Council of the International Glaucoma Association The International Glaucoma Association (IGA) announces that two new trustees, David Sanders and Susan Blakeney, have joined the IGA Board, which is chaired by Philip Bloom, Consultant Ophthalmologist at the Western Eye Hospital. David Sanders is a chartered accountant with more than 30 years of experience in various senior managerial positions, including acquisitions, corporate governance, financial control, IT, logistics, HR and audit, working for companies such as Price Waterhouse Coopers, Litton Industries and Omron Corporation a Japanese multinational company. For the last four years, David has held honorary positions for Access Stichting, a Dutch organisation supporting expats and campelle Euf, an organisation supporting foreign students at the Flensburg University. News Summer 2018 19
News
Susan Blakeney is a practising optometrist.
As well as her optometry degree and
professional certificates in glaucoma and
medical retina, she also has an MA in medical
ethics and law, a bachelors and a masters
degree in law and a PhD. Susan is Clinical
Adviser to the College of Optometrists,
Optometric Adviser to NHS England (South
(South East)) and a case examiner for the
General Optical Council.
She was awarded the Fellowship of the College
of Optometrists for her contribution to the
profession in 2008. She has published several
papers and her book chapter on ‘Legal aspects
of optometry in the United Kingdom’ was
published in 2009.
Picture by www.edwardmoss.co.uk
All rights reserved. College of Optometrists conference,York 2014.
Commenting on the new trustees, Chair of the IGA Board, Philip Bloom, says,
“We are delighted that two such high calibre individuals have joined our
Council, bringing such useful experience and skills. David’s business
background will ensure that our future strategy is robust, while Susan’s
optometry and legal background will also be invaluable in guiding our
existing and future services, including dealing with the wider optometry
industry and stakeholders.”
20 News Summer 2018News
Hannah Morrow joins the IGA as Development
Manager for the North East of England
Hannah Morrow will join the IGA, replacing
David Harris, who retired last year. Hannah
joins Subhash who covers London and the
South East, John who covers Scotland and Eryl
who covers Wales and the South West.
Hannah’s role will consist of direct support
work with people living with glaucoma, raising
awareness and understanding of the condition
among the general population of the North
East. She will help to establish patient support
groups, ensuring advice and support reaches
those most in need.
She will also liaise with a wide range of
healthcare professionals, glaucoma consultants,
nurses, pharmacists, optometrists and
colleagues from across the voluntary and
statutory sight loss sector, promoting
excellence in glaucoma care.
Prior to joining the IGA, Hannah was a Development Manager for Reviving the West End
Ltd (RHWE), a role she held since 2011. She has held several other public facing roles,
including being a Local Involvement Network Development Officer for North Tyneside
VODA, enabling people to influence NHS services. She was also a Health Development
worker for Gateshead Council, encouraging older people to lead healthier lifestyles.
Karen Osborn, Chief Executive comments: ‘‘We’re delighted to welcome Hannah to the
team as our new Development Manager for the North East of England. She brings a
wealth of experience in health and community development and in her most recent roles
she has led on project delivery, participant recruitment, volunteer involvement and
monitoring and evaluation, so I’m sure she’ll get off to a speedy and successful start.
Hannah will be based in Newcastle, providing support across Northumberland, County
Durham and Tyne and Wear.”
News Summer 2018 21News
Hannah Morrow says: “I am delighted to be joining the IGA team as Development
Manager for the North East. I have worked in the region for 15 years and have a
strong background in community engagement and partnership work. I will use my
experience to support people living with glaucoma and their families and carers,
enabling them to work closely with service providers to improve quality and access to
services across the region.”
Carolyn Lewis joins as
IGA joint membership
administrator
We are delighted that Carolyn has joined our
small team at the IGA. She shares her role with
Natalie Smith providing full time cover for our
member and supporter enquiries.
Carolyn previously worked for Valence
School as a Business Support Officer
for the Visual Impairment Team and says
of her appointment:
“My background with the visual impairment
team has given me a deep understanding of the
challenges faced by individuals facing visual impairment and poor eye health. I’m certain
that I can use this empathy and understanding to assist with supporting the work of IGA
and that of its supporters. My aim is to provide a first class administration service to
ensure the smooth efficient running of the organisation.”
Karen Osborn comments “Carolyn’s calm and efficient approach to handling caller
enquiries make her the ideal choice for the IGA. We are delighted to have her on board.”
22 News Summer 2018Talking glaucoma Editor’s introduction: This year’s Annual Lecture was provided by Professor Keith Martin who provided a fascinating overview of the future of glaucoma treatment. Jacqueline Mitton has written this report. Professor Keith Martin, University of Cambridge Glaucoma: What’s on the horizon? For the IGA’s 2018 Annual Lecture, Professor Keith Martin of Cambridge University looked into the future and talked about new ways of treating and managing glaucoma – some likely to be available soon, others still in early stages of research and development. Keith Martin is the first Professor of Ophthalmology appointed at the University of Cambridge and is recognized internationally as a leader in glaucoma research and treatment. His research is mainly concerned with new approaches to treating glaucoma using stem cells, gene therapy and other techniques, and he described some of these exciting developments at the end of his lecture. But he began by talking about the familiar, standard treatments most patients receive at present, the problems with them, and why new ways of treating glaucoma are needed. News Summer 2018 23
Talking glaucoma Daily eye drops from a bottle, some form of laser treatment, or perhaps a more invasive surgical procedure: patients with glaucoma can be offered one or more of these treatment options. All of them are aimed at reducing the pressure inside the eye. They work well enough to prevent many patients having a serious issue with vision loss during their lifetime but none is perfect. Each has its own set of problems. And there are a few patients whose vision continues to deteriorate despite treatment. Their unmet need is a big focus of Professor Martin’s own research. The trouble with drops Any patient who has been prescribed eye drops for glaucoma will recognise the problems Professor Martin identified, starting with the increasing confusion caused by a general move away from branded drops to generic versions. These substitutes may not be exactly the same and seem to come in a different kind of bottle with every prescription. Giving an example, Professor Martin said that people who started off on Xalatan® will mostly now be on a mixture of different types of latanoprost, which changes very frequently, even month to month. Some medications, such as Azarga, have had supply problems. 24 News Summer 2018
Talking glaucoma
Eye drop medication
Professor Martin also mentioned more use being made of preservative-free drops.
Eyes may tolerate them better, but getting the tops off the small individual vials and using
them to dispense the drops can be difficult. “It’s hard enough taking eye drops regularly
without all of these extra problems on top,” he said.
Difficulties like these are one reason why some people give up on
their eye drops. Another is that they simply forget. As glaucoma
doesn’t have any obvious symptoms, it is easy to get out of the
habit of taking drops. Research with large samples of patients in
America found that only about 50 per cent of them were actually
picking up their prescriptions a year on from their diagnosis.
Many people do not use their drops as they should even when they
try, either because they forget how to do it or because they just find
it too difficult. The more drops someone is on, the more complicated
it gets and the less likely they are to get everything right.
And is if that were not enough, some people have problems with
side effects. Then, after a long period of use, drops can make
surgical operations more challenging because unwanted healing
and scarring become more likely.
News Summer 2018 25Talking glaucoma
Selective Laser Trabeculoplasty (SLT)
Research with large samples
of patients in America found SLT is an alternative way of reducing pressure in
that only about 50 per cent the eye. It can be a very useful form of treatment
for some patients with open angle glaucoma,
of them were actually picking
especially those who struggle with eye drops.
up their prescriptions a year Professor Martin explained, “People imagine it’s
on from their diagnosis like punching little holes in the drainage channels
of the eyes but that’s not what happens.
Rather, it stimulates cells in that area to ‘clean up’ and ‘unblock the drains’.” Some older
laser treatments were a lot more destructive, which meant they couldn’t be repeated many
times. By contrast, SLT is unlikely to do major harm and can be repeated – which is why
ophthalmologists like it.
However, SLT does not work for everyone. About 70 per cent of people who have it
achieve a useful lowering of eye pressure but how a particular individual will respond is
unpredictable, as is the length of time the reduction in eye pressure will last. There’s also
a possibility that a person’s ethnic background might impact on SLT’s effectiveness. It all
raises the question of exactly how cost-effective SLT is.
In the face of these uncertainties with SLT, Professor Martin was looking forward to the
results from a major clinical trial taking place under the title LiGHT – standing for “Laser in
Glaucoma and Ocular Hypertension.” Its aim is to answer the question, “Which is better
as the starting point for treatment, SLT or eye drops?” The trial is being led by Consultant
Ophthalmologist Gus Gazzard, who is based at Moorfields Hospital. Over 700 patients
newly diagnosed with glaucoma or high eye pressure have taken part.
A notable feature of the LiGHT trial is the emphasis it puts on how well different
treatments are tolerated and their impact on quality of life, not just their effectiveness at
lowering eye pressure. The results are due to be published later in 2018 and could make
a difference to how many newly diagnosed patients will be treated in future.
No ideal operation
Ophthalmologists and many patients would be quite happy if there were a low-cost
operation without any side effects that always works, guarantees an eye pressure of 10,
removes the need for any medications and completely stabilizes glaucoma. Unfortunately,
26 News Summer 2018Talking glaucoma there is currently no such ideal operation. The operation with the highest chance of achieving low pressures remains trabeculectomy, first developed many years ago. In this procedure, the surgeon makes a small hole in the wall of the eye so fluid can drain out from the inside and creates a small reservoir called a “bleb” underneath the lining that covers the surface of the white of the eye. Fluid accumulates here before it’s absorbed. Although often effective, trabeculectomy is not without its risks and potential problems – and it’s time consuming. “So,” said Professor Martin, “the technology is changing and there is a variety of different little devices coming along that basically take fluid from one part of the eye to another.” This kind of treatment goes under the name MIGS: minimally (or micro) invasive glaucoma surgery. Some devices help fluid drain by the route it would normally take, through the trabecular network in the front angle of the eye. These tiny tubes bypass the place where there’s a blockage. However, they do not often reduce eye pressure by a great deal so they are most useful for people with relatively mild glaucoma. Other kinds of tubes can be used instead, to drain fluid to different spaces within the eye. Then there are tubes that work more like a traditional trabeculectomy operation and News Summer 2018 27
Talking glaucoma
New research
some of them form a bleb. That makes them powerful in terms of lowering pressure but,
as with a trabeculectomy, patients need careful management after the operation and have
to make several visits to the clinic. Even so, “We like them in some ways because they are
quicker and easier to do,” said Professor Martin.
As an example, he explained how one of the devices is inserted, using an “introducer”
to put a 6-mm soft tube into place. The tube connects the inside of the eye with the
area under the conjunctiva (that is, the outer membrane covering the white of the eye),
and forms a bleb. The job’s done in a much shorter time than it takes to perform
a trabeculectomy.
Which patients are most likely to benefit from MIGS and where does it fit in the range
of available treatments? That, said Professor Martin, is the subject of debate among
ophthalmologists at the moment.
“Obviously you the patients would like to have fewer drops,” he said, “and fewer side
effects, a better quality of life and the reassurance that what’s been done is working and
isn’t going to fail. We as ophthalmologists want something that works reliably, is low risk
(ideally lower risk than the operations we have at the moment), and is a cost effective
28 News Summer 2018Talking glaucoma
Minimally Invasive Glaucoma Surgery (MIGS)
treatment that saves time and money. That’s what we’re wrestling with clinically at
the moment.” Many of the MIGS procedures do have a place in the treatment of
particular individuals. One thing Professor Martin could say for certain: none of the
devices is a miracle cure for glaucoma but patients will be hearing more about them in
the coming years as these treatments develop.
For high-risk patients whose glaucoma is advanced or progressing rapidly, a trabeculectomy
or one of the more long-standing forms of tube surgery may still be more suitable than
MIGS. Professor Martin’s view is that “there’s
nothing to beat a well done trabeculectomy
For high-risk patients operation in terms of achieving very low
whose glaucoma is pressures.” At the other end of the spectrum,
advanced or progressing when people are happy with their current
rapidly, a trabeculectomy treatment, their glaucoma is well-controlled
and they are at low risk, “there’s absolutely
or one of the more
no reason to think about changing their
long-standing forms of treatment in that situation.”
tube surgery may still be
more suitable than MIGS So the debate at the moment is focused on
the “people in the middle” – those who may
not be tolerating drops quite as well as they
did, or who are finding it harder to put them in, or have other issues that mean drops are
not ideal. Said Professor Martin, “what we are trying to do with the variety of different
devices available at the moment is to work out which are right, if any, for different patients,
or whether we would be better to look at different ways of delivering drugs to patients by
means of slow release, which doesn’t require you to put in eye drops every day.”
News Summer 2018 29Talking glaucoma New ways with drops Although no really new classes of drops have been introduced in recent years, there are some that have now reached the end of development and will be coming through into clinical practice soon. In particular, Professor Martin mentioned modifications to the type of drops known as prostaglandin analogues (e.g. latanaprost , travaprost, bimataprost, tafluprost) to make them more powerful, and also a completely new class of medications, Rho kinase inhibitors, which may have some role if not as a first line of treatment. Meanwhile, many more combinations have been introduced, so two types of medication can be put in the eye at the same time with a single drop. What is novel is research into devices that can deliver medications to the eye without patients having to put in eye drops every day. Professor Martin’s team at Cambridge is involved in an international clinical trial of a technique in which a dot of one of the prostaglandin analogues is inserted into the eye to release the drug slowly over a number of months. A dot seems to last for at least four months – and up to eight months or more in some patients. The trials are looking not only at whether the system works effectively to reduce eye pressure but also at how well patients tolerate it and the side effects of the drug, which hopefully could be less than when drops go onto the surface of the eye. The disadvantage of this type of treatment is that it is invasive and does require a procedure, albeit a quick one, to place the dot inside the eye. A variety of other slow release systems are under development too. In some, the drug is placed not inside the eye but underneath the conjunctiva, in the space between the white of the eye and the overlying tissue. Although this seems more attractive than something going into the eyeball, because it is less invasive, it presents a different problem: there is considerable variation between patients in the way the drug is released. A totally different approach to slow release is to put the drug inside a little ring, which is worn in the eye rather like a contact lens with a large hole in the middle so it consists only of a rim. The ring slips under the eyelids and stays in place. These are in the clinical trial stage at the moment and work is going on to develop materials that are both comfortable to wear and capable of gradually releasing the eye drops that people are normally using every day. Some of the trials seem to be showing that these devices can be tolerated quite well. 30 News Summer 2018
Talking glaucoma
Keeping track of the pressure
The future for managing glaucoma is not just about new approaches to treatment:
monitoring the effectiveness of treatment, especially eye pressure, is important too.
Patients might go for months between clinic visits without having their eye pressures
checked. How representative are those snap-shot measurements? What is happening in
between them? Clinicians would love to know, so devices are being invented that can
measure eye pressure, either directly or indirectly, around the clock.
One of these comes in the form of a contact lens with a built-in sensor to detect the
stretch of the eye, which correlates with eye pressure. The sensor transmits to a little
pack that the patient carries around on them. That then sends on the data to be analysed
by an ophthalmologist. A patient could wear the lens to record a pressure profile through
the course of 24 hours. Monitoring pressure continuously in that way might help
clinicians identify which patients are likely to do well in the future and who might need
more aggressive treatment. “If it gives us additional information over and above
measurements in the clinic then I think it may be useful”, concluded Professor Martin.
Going a stage further, Professor Martin foresaw how useful it could be for someone to
have a pressure sensor built in to their eye. “If you look at how much micro-electronics
has changed medicine and some of the things that are now being done, this is not beyond
us. It’s already been done in animals and is moving forward to clinical trials now.”
The opportunity arises when a patient has a cataract operation and has a new lens put in
their eye. The new lens can be made to contain a tiny pressure-sensitive device, which
activates a sensor built into a special pair of glasses. You put on the glasses and they
produce a continuous pressure read-out.
“It’s a scary thought for ophthalmologists”
The future for managing confessed Professor Martin, “getting a phone
call every time there’s a spike in someone’s
glaucoma is not just
eye pressure if they have all this information
about new approaches but this is the sort of technology I think we
to treatment: monitoring will have available.” He predicted that
the effectiveness of working out how to manage all the patient
treatment, especially eye data will be harder than developing the d
pressure, is important too evices themselves and that it will take time to
work out how to interpret the information
and put it to good use.
News Summer 2018 31Talking glaucoma Protecting the optic nerve Keeping down the pressure inside the eye is overwhelmingly the most important line of treatment for glaucoma but is there any other way to slow down or prevent the damage to nerve cells that happens in glaucoma and causes loss of vision? Possibly there is. Devices to release potentially protective substances into the eye have reached the clinical trials stage and Professor Martin talked about one example. The device has in it a capsule containing specially prepared human cells from the outer part of the retina. These cells have been “engineered” so they can keep replicating and producing the protective factor. The cells themselves are trapped in the capsule but the protective factor can permeate through. And as long as the cells are in there they keep up the production. The clinical trial is looking at whether the protective substance has any effect on the way the visual field patients whose glaucoma is getting worse changes over time. 32 News Summer 2018
Talking glaucoma
Better diagnosis with artificial intelligence?
Earlier, more accurate diagnosis of degenerative eye conditions means that the right
treatment can start as soon as possible. Recently, Moorfields Hospital has partnered
with a sister company of Google, called DeepMind, which specializes in machine learning,
or “artificial intelligence” (AI).
The project involves studying over a million
photographs of patients’ retinas to see
whether machines can learn how to recognize
The machines are now
early signs of eye conditions, including
glaucoma, and other useful medical information. better than a general
The anonymised data have been sourced from ophthalmologist at
the records of past patients, the UK Biobank diagnosing diabetic
and elsewhere. retinopathy and I don’t
think it will be long before
“The results really are quite stunning,” these sorts of systems
Professor Martin said. “Would you have
overtake experts looking
believed that from a single retinal photograph
the computer could tell with confidence at photographs
whether you are male or female? As
ophthalmologists, we cannot do that.”
After being shown many thousands of photographs and told which are from males
and which from females, the machine learns how to tell the difference. Then, when it’s
shown a photograph it’s never seen before it can identify whether it came from a male
or female patient.
Perhaps that particular ability is not very useful in itself but it illustrates the power of
what AI can do. “If from a single retinal photograph it can accurately tell what someone’s
blood pressure is, you would think that’s impressive,” says Professor Martin. “This is really
about being able to tell a whole range of different things about a patient, such as their risk
of cardiovascular disease, and potentially diagnosing specific eye conditions.
The machines are now better than a general ophthalmologist at diagnosing diabetic
retinopathy and I don’t think it will be long before these sorts of systems overtake
experts looking at photographs.”
News Summer 2018 33Talking glaucoma Stem cell therapy Professor Martin is often asked whether stem cells can be used to restore vision to people with advanced glaucoma. There’s been publicity this year for some exciting results from Moorfields. Two patients with age-related macular degeneration regained useful sight after little patches of cells were put underneath their retinas. But Professor Martin sounded a note of caution. “I stress that this is early days for this sort of technology,” he said. “The patients in this trial were very carefully selected. Often with macular degeneration quite a lot of the light sensitive cells within the eye (the photoreceptors) are lost. If they are gone, this sort of treatment is not going to have very much effect. These patients still had photoreceptors. Nevertheless, the results really are quite exciting.” The details of how the therapy works are obviously quite technical but Professor Martin explained the basics as simply as he could. The cells put into the patients’ eyes came originally from stem cells taken from human embryos. Stem cells can be changed into different kinds of specialized cells. In this case, the stem cells were changed into a type of cell found in the retina called retinal pigment epithelial cells. 34 News Summer 2018
Talking glaucoma News Summer 2018 35
Talking glaucoma
Their job is to support the light-sensitive cells. They clean up waste products from the
light-sensitive cells and are very important for keeping the whole system working.
If you lose them, you are at risk of problems with your central vision. Using stem cells
is potentially a way of replacing them.
So would something similar work in the case of glaucoma? It’s what Professor Martin
and his team are working on, but he warned that replacing the cells lost in glaucoma –
called ganglion cells – is much more difficult. These are nerve cells and there are
more than 20 different types in the eye, all doing different things, and with complicated
connections to the brain.
“Replacing those cells and expecting them to function is a very tall order,” he said. “We
have some progress with changing stem cells into something that looks like a retinal
ganglion cell but less progress with how we connect them within the retina and to the
brain. Using stem cells to replace lost retinal ganglion cells is still a long way off.”
However, there are more promising ways of using stem cells. For example, they could
help the trabecular network where fluid drains out of the eye to function better or even
to repair the optic nerve head where nerve fibres leave the eye and connect to the brain.
This is the place most likely to suffer damage in glaucoma.
Professor Martin’s particularly interest, though, is in using stem cells to give the surviving
ganglion cells a better chance of staying alive for longer and making them more resistant
to injury. This is something already achieved
in rats. Researchers in Professor Martin’s
I spend a lot of time laboratory identified the substance stem
trying to prevent cells make that has protective properties.
exploitation of vulnerable With financial help from an IGA research
patients with grant, they went on to see if it would work
unproven treatments with human tissue.
The answer was “Yes.” Human stem cells
turned out to be very good at protecting human retinal ganglion cells against damage.
At first the outcome was quite encouraging. But there was a problem. In some eyes it
works very well but in others the retina gets damaged by a scarring response. So now
work is under way to try to eliminate the scarring while keeping the protective effect.
Professor Martin had a special warning for patients tempted to go to clinics overseas to
have injections of their own stem cells into their eye. If asked, he always advises against
for many reasons. It’s often very expensive and there are real risks. In most of the
36 News Summer 2018You can also read

















































