Il trattamento anticoagulante orale nella prevenzione dell'ictus ischemico nel paziente anziano comorbido con fibrillazione atriale ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Il trattamento anticoagulante orale nella prevenzione dell’ictus ischemico
nel paziente anziano comorbido con fibrillazione atriale
Giovambattista Desideri
UO Geriatria e Lungodegenza
Università degli Studi di L’Aquila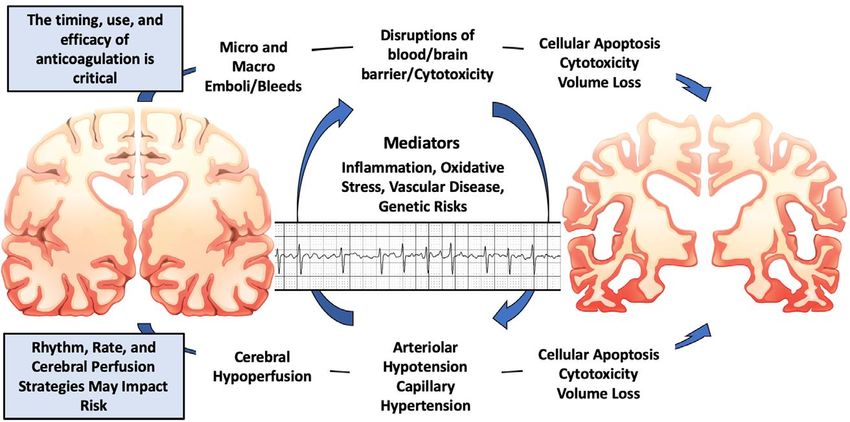
Atrial Fibrillation
Demographics by Age
Comorbidities in
Atrial Fibrillation
ETNA-AF-Europe study
13092 patients
65–74 years - 4456 (34.0%)
>75 years - 6640 (50.7%)
J.R. de Groot et al. Eur Heart J Card Pharm 2020
Heering J, et al. Eur Heart J 2006 Brandes A, et al. Arrhythm Electrophysiol Rev. 2018
Age-Specific Incidence, Outcome, Cost and Projected Future Burden of AF-Related
Embolic Vascular Events: A Population-Based Study
Age- and sex-specific rates per 100,000 population per year for all incident AF-related ischaemic stroke and
systemic embolism: the Oxford Vascular Study (2002-2012; N=92728; 9 general practices - about 100 family
doctors)
Rate per 1000 per year
Yiin GSC et al. Circulation. 2014;130(15): 1236–1244.
Albers Et al. Chest 2004;126(3 suppl): 438S-512S
Age Group
Thom et al. American Heart Association. Circulation 2006;113:385-e151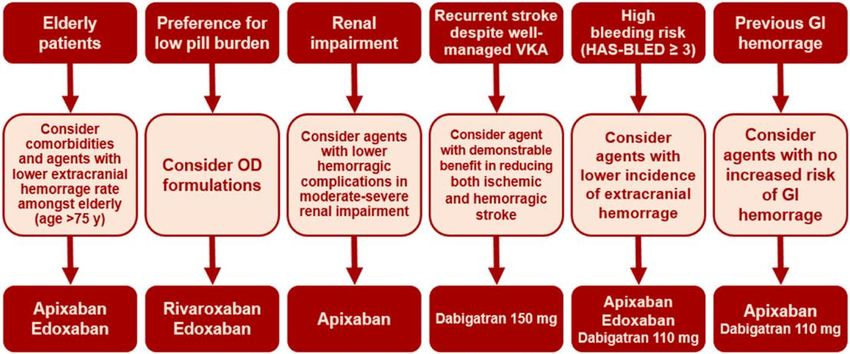
Older patients are at higher risk of all cardiovascular events - observations from
the ARISTOTLE trial
Stroke or systemic embolism All-cause mortality
ISTH major bleeding Intracranial haemorrhage
Halvorsen S et al. European Heart Journal (2014) 35, 1864–1872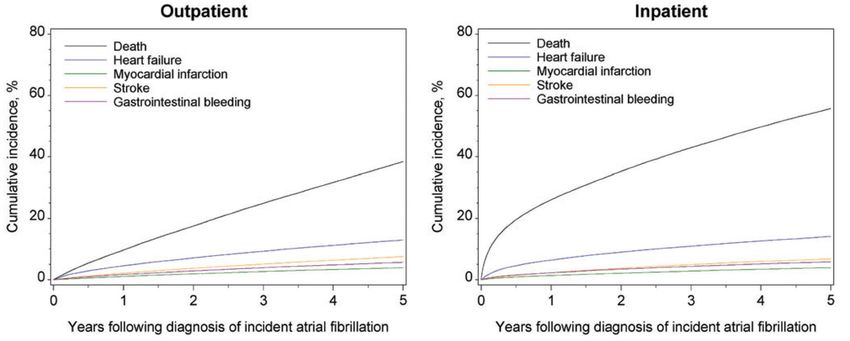
The ischemic and bleeding risks both increase with increasing age regardless of
anticoagulant use
Japanese Rhythm Management Trial for
PREvention oF thromboembolic events – European Atrial Fibrillation
Registry in Atrial Fibrillation (PREFER in AF) (J-RHYTHM ) Registry
Kato et al. Ageing Reasearch Reviews (2019) 49; 115-124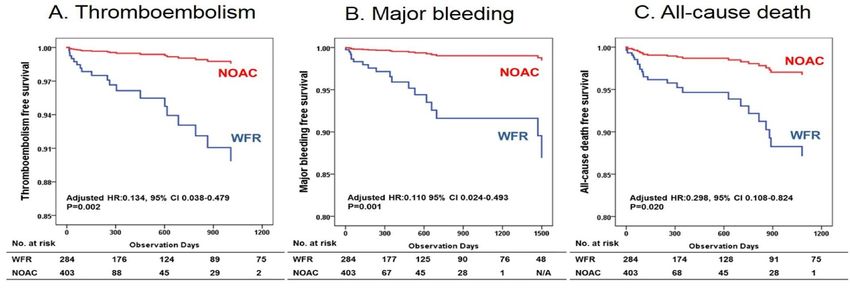
Net clinical benefit, adjusted for the mortality risk, of OAC vs no OAC according to
different age strata: a sub-analysis from the PREFER in AF
Net clinical benefit in the overall population:
-2.19%: 95% CI -4.23%, -0.15%; P=0.036
Patti G et al. J Am Heart Assoc. 2017;6:e005657.
Current presentation and management of 7148 patients with atrial
fibrillaton in cardiology and internal medicine hospital centers: The
ATA AF study
CHADS2 (%)
75,3
>2
53,1
19,5
1
33,1
5,2
0
13,0
0 20 40 60 80 100
Di Pasquale G et al. Int J Cardiol 2013;167:2895–2903
Clinical course of atrial fibrillation in older adults: the importance of
cardiovascular events beyond stroke
Observed cumulative incidence of events in the 5 years after the diagnosis of incident atrial fibrillation by setting
of diagnosis in the primary study cohort.
Piccini JP et al. Eur Heart J 2014;35:250–256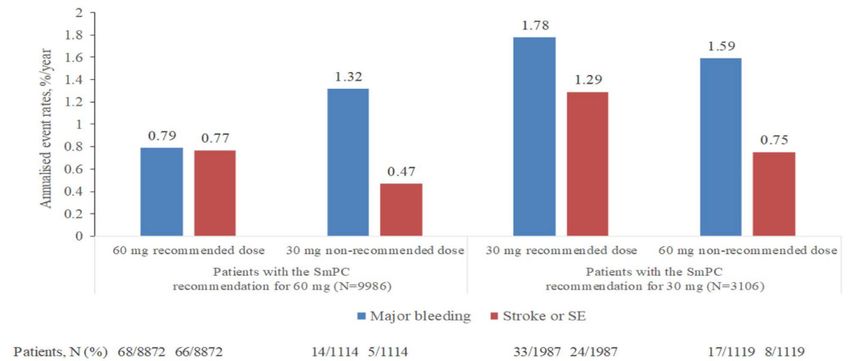
Anticoagulation with
DOAC in elderly patients
with AF according to
frailty status
≈50%
≈20%
≈30%
Eur J Int Med 71 (2020) 32–38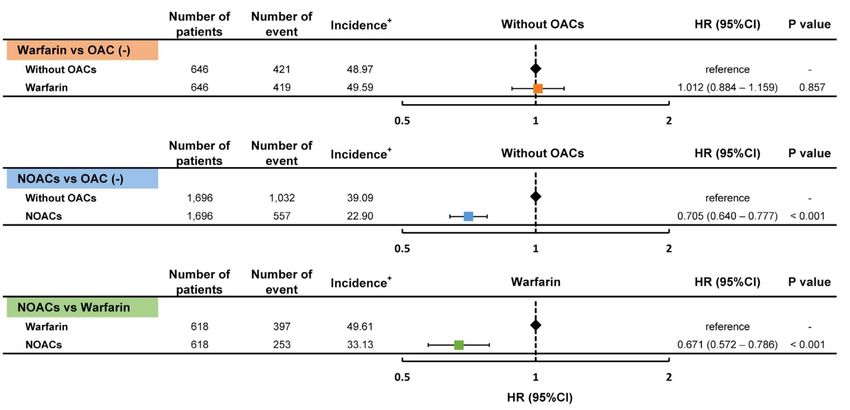
Benefic
i Rischi
(ê ictus e ES) (é emorragie)Benefic
i Rischi
(ê ictus e ES) (é emorragie)Efficacy and safety outcomes in patients ≥ 75 years from sub-
analysis of Phase III RCTs on DOACs
Stroke/ SE Major bleedings
RR (95% CI) RR (95% CI)
Apixaban
0.71 (0.53–0.95) 0.64 (0.52–0.79)
ARISTOTLE
(≈31%>75 ys)
Rivaroxaban
0.80 (0.63–1.02) 1.11 (0.92–1.34)
ROCKET AF
(≈44%>75 ys)
Dabigatran 150
0.67 (0.49–0.90) 1.18 (0.98–1.42)
RE-LY
(≈40%>75 ys)
Dabigatran 110
0.88 (0.66–1.17) 1.01 (0.83–1.23)
RE-LY
(≈40%>75 ys)
Edoxaban
0.83 (0.67–1.04) 0.83 (0.70–0.99)
ENGAGE-AT TIMI 48
(≈40%>75 ys)
Favours NOAC Favours warfarin Favours NOAC Favours warfarin
Derived from Bo M. et al. European Journal of Internal Medicine 41 (2017) 18–27Safety and efficacy of non-vitamin K antagonist oral anticoagulants in elderly
patients with atrial fibrillation: systematic review andmeta-analysis of 22 studies
and 440 281 patients
Silverio A et al. European Heart Journal - Cardiovascular Pharmacotherapy (2021) 7, f20–f29Oral anticoagulants in extremely-high-risk, very elderly (>90 years)
patients with atrial fibrillation
Composite net clinical endpoint of ischemic stroke, ICH,
major bleeding, or mortality. Chao TF et al. Heart Rhythm 2021;18:871–877)Prevention
Choosing a particular oral anticoagulant and dose
for stroke prevention in individual patients with
non-valvular atrial fibrillation: part 2
Age > 75 years High risk of GI bleeding
First choice • Apixaban 5 mg twice daily [2.5 mg if ≥2 • Apixaban 5 mg twice daily
of the following: age ≥80 years, body • Dabigatran 110 mg twice daily
weight ≤60 kg, or creatinine ≥1.5
mg/dL (133 mmol/L)]
Second Choice • Dabigatran 110 mg twice daily • Dabigatran 150 mg twice daily
• Rivaroxaban 20 mg once daily • Edoxaban 60 mg once daily
• Edoxaban 60 mg once daily • Rivaroxaban 20 mg once daily
Diener HC et al. Eur Heart Journal 2016. doi:10.1093/eurheartj/ehw069❖ ESGE recommends restarting anticoagulant therapy following acute GIB in patients with
an indication for long-term anticoagulation (GRADE: strong recommendation, moderate
quality evidence).
❖ In patients at low thrombotic risk, ESGE suggests restarting anticoagulation at the
earliest by day seven after anticoagulation interruption (GRADE: weak
recommendation, low quality evidence).
❖ In those at high-thrombotic risk, an earlier resumption of anticoagulation with heparin
bridging, preferably within 72 hours, is recommended (GRADE: strong recommendation,
low quality evidence).
Veitch AM, et al. Gut 2021;70:1611–1628.Restarting Anticoagulation and Outcomes After Major
Gastrointestinal Bleeding in Atrial Fibrillation
➢ There is a trend toward reduced incidence of thromboemboic events the earlier warfarin is introduced; this trend is
more evident within 15 days
➢ Resuming warfarin within 7 days is associated with a 3-fold increased risk of rebleeding
➢ Decision to restrat warfarin after 7 days of interruption is associated with decreased thromboembolism, improved
survival without increased risk of recurrent GI bleeding
Qureshi V et al. Am J Cardiol 2014;113:662e 668Benefic
i Rischi
(ê ictus e ES) (é emorragie)Insufficienza renale cronica e fibrillazione atriale
Incidenza di ictus o embolia sistemica
in base a valori di CrCl e storia clinica
di pregresso ictus in pazienti con FA in
terapia AO
10
9 Renal impairment
Ictus o embolia sistemica (%)
Storia di ictus
8 PREFER in AF: 10.3%
& eGFRPrimary efficacy, safety, and net clinical outcome end points by prespecified CrCl
subgroups in the ENGAGE AF-TIMI 48 Trial
*HDER of 60 mg daily or 30 mg daily if dose reduced for creatinine
clearance (CrCl) ≤50 mL/min, weight ≤60 kg, or potent
phosphorylated glycoprotein inhibitor use.
Bohula EA et al. Circulation. 2016;134:24-36.Efficacy and safety of apixaban compared with warfarin for stroke prevention in
atrial fibrillation according to age and renal function: observations from the
ARISTOTLE trial
Hohnloser SH et al. European Heart Journal (2014) 35, 1864–1872Efficacy of apixaban when compared with warfarin in relation to renal
function in patients with AF: insights from the ARISTOTLE trial
Hohnloser SH et al. European Heart Journal (2012) 33, 2821–2830Potential mechanisms of cognitive decline and dementia in patients
with atrial fibrillation
Bunch TJ et al.Circulation 2020 Aug 18;142(7):618-620Long-Term Population-Based Cerebral Ischemic Event and
Cognitive Outcomes of DOAC Compared With Warfarin Among Long-term
Anticoagulated Patients for Atrial Fibrillation
5,254 patients. Intermountain Healthcare Clinical Pharmacist Anticoagulation Service (CPAS).
Rivaroxaban 55.3%
Apixaban 22.5%
Dabigatran 22.2%
Jacobs V et al. Am J Cardiol 2016;118:210e 214Anticoagulant Use for Atrial Fibrillation Among Persons With Advanced
Dementia at the End of Life
Among 15.217 nursing home
residents with AF and
advanced dementia (mean
age, 87.5+6.76 years, 68.2%
women), 5033 (33.1%)
received an anticoagulant in
the last 6 months of life.
Ouellet GM et al. JAMA Intern Med. 2021Outcomes of Direct Oral Anticoagulants in Atrial Fibrillation
Patients Across Different Body Mass Index Categories
Barakat AF et al. J Am Coll Cardiol EP 2021;7:649–58)2021 European Heart RhythmAssociation Practical Guide on the Use of Non-
Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation
NOACs in under- and overweight patients.
Barakat AF et al. J Am Coll Cardiol EP 2021;7:649–58)Direct oral anticoagulants versus vitamin K antagonists in
patients with atrial fibrillation and cancer a meta-analysis
Mariani M et al. Journal of Thrombosis and Thrombolysis (2021) 51:419–429Benefic
i Rischi
(ê ictus e ES) (é emorragie)Absolute Risk Reduction of HDER Compared With Warfarin in Patients at Increased
Fall Risk Versus Not at Increased Fall Risk
ENGAGE AF–TIMI 48 Analysis
Absolute Risk Reduction of HD Edoxaban Regimen Compared With Warfarin in Patients at Increased Versus Not
at Increased Fall Risk
Bleed
Events / 10,000 Patient Years
NNT NNT
157 vs. 500 152 vs. 293
NNT
94 vs. 323
NNT
57 vs. 257
Steffel J et al. J Am Coll Cardiol. 2016 Sep 13;68(11):1169-1178.Clinical Outcomes and History of Fall in Patients with AF Treated with Oral
Anticoagulation. Insights from the ARISTOTLE Trial
Rao MP et al. Am J Med Nov 6, 2017Benefic
i Rischi
(ê ictus e ES) (é emorragie)Major bleeding and stroke/SEE in ETNA-AF-Europe patients dosed in line and
not in line with SmPC recommendations.
All-cause mortality, CV mortality, and rates of major
bleeding were higher in patients receiving reduced dose of
edoxaban
Underdosing was associated with higher rates of all-cause
death, CV death, and major bleeding
De Groot JR et al. Eur Heart J Cardiovasc Pharmacother. 2020Reasons for non-recommended lower dosing (30mg) in patients with no
adjustment factors: ETNA AF - JAPAN
The lower dose of 30 mg edoxaban was administered to approximately
70% of patients (11.4% received a nonrecommended lower dose).
Yamashita T et al. Journal of Arrhythmia. 2020;36:395–405.Efficacy and safety of apixaban compared with warfarin for stroke prevention in
atrial fibrillation according to age and renal function: observations from the
ARISTOTLE trial
Hohnlsoer SH et al. European Heart Journal (2014) 35, 1864–1872Off-label use of reduced dose direct oral factor Xa-inhibitors in subjects with atrial
fibrillation: A review of clinical evidence
Guidelines Uncertainties and subjective clinical reasoning Available evidence
NVAF diagnosis Consistent evidence that patient’s
Maybe a reduced dose could
increase clinical benefit in these characteristics rather than ofXaIs dose are
patients? associated with bleeding and
Recommended OAT? embolic events
yes
Consistent evidence from RCTs of a net clinical
Contraindications to benefit with appropriate of XaIs’ doses over
DOACS? warfarin
no
Evidence form real-life studies that
Criteria for reduced dose
underdosing is not associated with a sizeable
DOACS? net clinical benefit
no
Prescription of full dose but… In the vast majority of patients, oFXaIs should
DOAC? be prescribed according to
approved dosing recommendations
Bo M et al. Eur Heart J Cardiovasc Pharmacother. 2020(Very) Low-Dose Edoxaban in Very Elderly Patients with Atrial
Fibrillation ELDERCARE-AF
A low creatinine clearance (15 to 30 ml per minute), a history of bleeding from a critical area or organ or gastrointestinal
bleeding, low body weight (≤45 kg), continuous use of NSAIDs or current use of an antiplatelet drug.
Okumura K et al. N Eng l J Med 2020Benefic
i Rischi
(ê ictus e ES) (é emorragie)
And so what…?Effectiveness and safety of non-vitamin K antagonist oral anticoagulants
in octogenarian patients with non-valvular AF
Lim HM et al. 2019 PLoS ONE 14(3): e0211766. https://doi.org/10.1371/journal. pone.0211766Net Clinical Benefit of Non-Vitamin K Antagonist Versus Vitamin K
Antagonist Anticoagulants in Elderly Patients With Atrial Fibrillation: PREFER in AF
and PREFER in AF PROLONGATION
Patti G et al. Am J Med. 2019 Jan 18. pii: S0002-9343(19)30071-3.Risultati clinici con rivaroxaban, apixaban, edoxaban e dabigatran vs warfarin negli
studi registrativi ed interazione tra dose piena e ridotta
Efficacia Sicurezza
Efficacia ANALOGA Efficacia SUPERIORE Efficacia ANALOGA
Sicurezza ANALOGA Sicurezza SUPERIORE Sicurezza SUPERIORE
Efficacia SUPERIORE
Sicurezza ANALOGA
Efficacia ANALOGA
Sicurezza SUPERIORE
*ulteriormente più sicuro vs
warfarin.
Rubboli A. G Ital Cardio 2017Therapeutic decisional flow-chart for AF patients candidate to OAT,
according to specific characteristics
patient phenotyping
Bo M. et al. European Journal of Internal Medicine 41 (2017) 18–27…An individualized approach matching the
particular NOAC to the participant profile, taking
into consideration the risk of bleeding and other
comorbidities, should be taken rather than a
generalized “one drug fits all” approach in elderly
adults.
Sardar P et al. J Am Geriatr Soc. 2014;62(5):857-864.You can also read