Inactivity: Symptoms Associated With Gastrocnemius Muscle Disuse During Pregnancy
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
MCN Clinical Issues
Volume 13, Number 2, pp. 248-262
@2002, MCN
Inactivity: Symptoms Associated
With Gastrocnemius Muscle
Disuse During Pregnancy
Judith A. Maloni, PhD, RN, FAAN;
Barbara St. Pierre Schneider, DNSc, RN
II This longitudinal study assessed change gastrocnemius muscle reoxygenation after
in gastrocnemius muscle metabolism exercise significantly increased across
across antepartum bed rest and recovery antepartum bed rest (t = -2.1, P < .05) and
during the first 6 weeks postpartum as significantly decreased during the 6-week
well as symptoms during recovery.The postpartum period (t = 1.83, P < .05).
convenience sample consisted of 65 Women who were on bed rest prior to
pregnant women, hospitalized on bed hospital admission had significantly higher
rest for a mean of 24.8 days (range 5-70 reoxygenation scores upon enrollment (t =
days). A dual wavelength hemoglobin! -8.6, P < .05). Symptoms of postpartum
myoglobin spectrophotometer and muscle soreness, deconditioning, and
ergometer assessed muscle difficulty with mobility were reported.
reoxygenation times after plantar flexion Postpartum assessment and rehabilitation
exercise from hospital admission through are needed to facilitate recovery and
6 weeks postpartum. The Postpartum prevent long-term injury. (KEYWORDS:
Symptom Checklist assessed symptoms pregnancy, bed rest, inactivity, muscle
of muscle deconditioning.The time for disuse, muscle deconditioning)
Each year approximately 700,000 pregnant women who have been on antepartum bed
women are prescribed antepartum bed rest rest are discharged from the hospital without
for prolonged periods despite the lack of ev- an assessment of possible side effects, ad-
idence of its effectiveness.l-4 Bed rest ther- vice about recovery, or a planned program
apy during pregnancy is prescribed from of rehabilitation.3,7 To date, there has been
weeks to several months by 89% to 92% of
obstetricians, and the majority of them are ..........
unaware of the side effects of this From the Frances Payne Bolton School of Nursing,
treatment.' However, the physiologic side ef- Case Western Reserve University, Cleveland, Ohio (Dr
fects of various types of activity restriction in MalonD; and the School of Nursing, University of Wis-
consin, Madison (Dr Schneider).
nonpregnant individuals are widely recog-
nized.6 Many obstetric healthcare providers Reprint requests to Judith A. Maloni, PhD, RN,
FAAN, Case Western Reserve University, Frances
believe that because women are young and Payne Bolton School of Nursing, 10900 Euclid Av-
healthy prior to pregnancy the effects of in- enue, Cleveland, OH 44106-4904 (e-mail: jam44@po.
activity are negligible. Thus, after birth, cwru.edu).
248
Vol. 13, No.2 May 2002 PREGNANCY MUSCLE DISUSE . 249
minimal research examining the side effects induces significant change.9-11Deterioration
of bed rest therapy among pregnant in the musculoskeletal system begins rapidly
women.8 Only one study provides evidence within 6 hours of bed rest.I4-16Absolute loss
that pregnant women demonstrate physio- of muscle mass and protein peaks during 3
logic side effects of bed rest that are similar to 7 days,17The most profound areas of atro-
to those identified in nonpregnant popula- phy are in the postural muscles of the legs
tions.3 Documentation of physiologic side and back. 6.18-20Greater loss occurs with even
effects of bed rest in pregnant women is im- longer periods of inactivity.ll.18.19After 5
portant because bed rest treatment may weeks of bed rest, there is a 27% loss of
place women at risk for both short- and strength in the plantar flexor muscles, in-
long-term disability. Therefore, the purpose cluding the soleus and gastrocnemius.17 In
of this study was to assess change in gastroc- one study, subjects demonstrated a 9% loss
nemius muscle metabolism across antepar- in muscle volume in the lower back group,
tum bed rest and postpartum recovery and 16% to 18% in the quadriceps and hamstring
to describe the prevalence of symptoms as- groups, 20% in the ankle flexors, and 30% in
sociated with recovery from musculoskeletal the ankle extensors after 17 weeks of space
deconditioning after bed rest. flight.19The arms appear to be affected to a
lesser degree but significant atrophy occurs
if bed rest is prolonged.6,21Although there is
o Review of Literature considerable variability in subjects, muscle
volume loss appears to reach a steady state
Inactivity occurs on a continuum ranging or plateau at approximately 4 months of
from reduced activity to complete immobi- space flight.19
lization.6 Bed rest is one type of activity re- Differing models for the study of disuse
striction and has been the focus of extensive atrophy reveal similar changes in muscle
research. Aerospace scientists have used bed mass, protein, and strength. In animals, fiber
rest as a model to study the effects of type and metabolic property changes occur
weightlessness in space.9-11Research across in atrophied muscles.22,23For example, atro-
more than 40 years documents that bed rest phied soleus muscle has fewer slow-twitch
induces changes in every human physiologic fibers.23 Disuse muscle atrophy induces in-
system.9-11The cause of bed rest side effects creased anaerobic capacity in slow-twitch
is unclear but believed to be due to several and fast-twitch oxidative glycolytic fibers of
factors. These factors include the lack of the soleus and gastrocnemius, respectively.23
weight bearing on the skeleton; decreased Data from a space flight study suggest simi-
postural cues to the different organ systems; lar changes in anaerobic capacity in slow-
decreased number and magnitude of muscle twitch fibers of the vastus latera lis muscle.24
contractions, particularly of the postural Therefore, it is possible that bed rest may in-
muscles: and a headward bodily fluid duce alterations in muscle metabolism prop-
shift.9.11The major adverse effect of bed rest erties of pregnant women.
is a general physical deconditioning mani- Much is still unknown about recovery
fested, in part, by alterations in circadian from inactivity because ethical issues limit
rhythms and in cardiopulmonary, immune, the duration of bed rest research and space
hormonal and musculoskeletal systems.9-11 flights are limited to small numbers of sub-
Bed rest also results in insulin resistance in jects.6 However, recovery appears to be pro-
the muscle and liver of women.12,13Of con- longed whether induced by bed rest or
cern is that muscle contraction initiates glu- space flight.8.9.11Like initial deconditioning,
cose uptake. Thus, whole body glucose various organ systems recover at different
homeostasis may be altered by bed rest.12.13 rates.6.9.19Recovery begins with remobiliza-
Being totally confined to bed, or in a Tren- tion and occurs slowly. In a study of 4 crew
delenberg position, increases the severity of members after an 8-day space flight, ham-
side effects.3.6.9 string and lower back muscles were still be-
Organ systems deteriorate at different low baseline at 2 weeks after recovery.I8
rates across the same length of bed rest. During Mir space flights of 115 to 197 days,
However, evena shortdurationof inactivity recovery of muscle volume was completed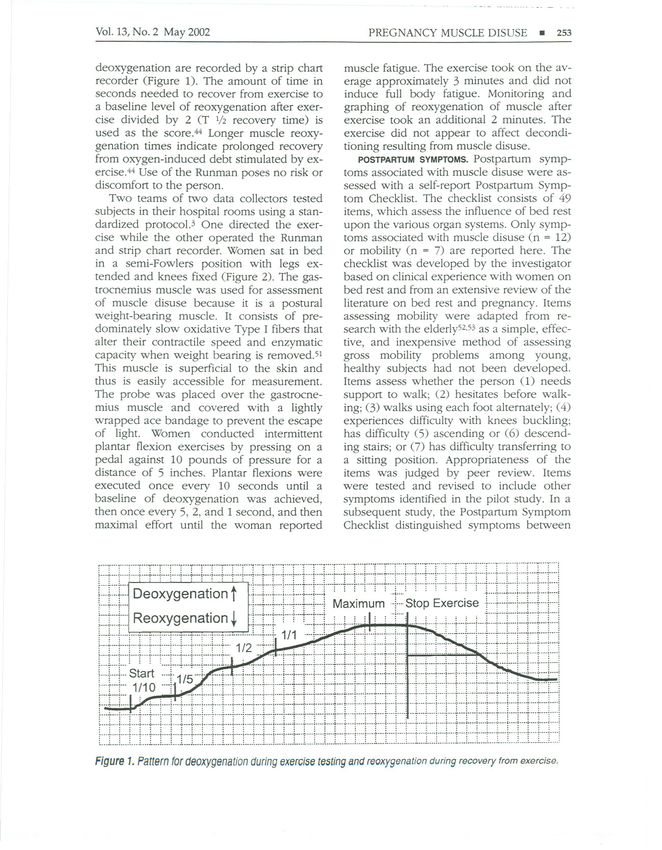
250 . MALONI AND ST PIERRE AACN Clinical Issues
for most individuals by 30 to 60 days after Because the majority of bed rest research
flight.19 However, these results should be in- has been conducted on males and none on
terpreted with caution as many astronauts pregnant women, it was unknown whether
conducted intensive exercise during flight to pregnant women also experience muscu-
offset anticipated losses. loskeletal changes induced during bed rest
In a laboratory study of muscle recovery, and recovery from bed rest. During the last
lower limb suspension was used to study the decade, research has begun to document the
effects of muscle disuse. Six men were side effects of antepartum bed rest; however,
placed on 4 weeks of lower limb suspension this research has primarily focused on the
to mimic the effects of space flight. How- psychosocial side effects.35-38There is only
ever, after 7 weeks of recovery, the ability to one published study documenting the physi-
maintain force output was not fully ologic effects of bed rest during pregnancy.3
restored.25 Although muscle mass had re- Outcomes for 17 women on antepartum bed
turned to normal, endurance remained sub- rest were compared with those for 18
optimal. Of further concern, it is not known healthy pregnant women who were not pre-
whether the changes in musculoskeletal sys- scribed bed rest. Variables included antepar-
tem are totally reversible.ll.19 tum and postpartum muscle reoxygenation
Based primarily on animal studies, recov- time after exercise and postpartum symp-
ery from muscle atrophy, in addition to be- toms of muscle recovery. Results revealed
ing prolonged, appears to involve further that the time needed to reoxygenate the gas-
muscle injury.6.26-30 Muscle damage and in- trocnemius muscle after a short bout of plan-
flammation are evident soon after the re- tar flexion exercise increased as the length
sumption of normal weight bearing.29.30Ex- of bed rest increased and decreased once
ercise has been shown to cause muscle bed rest was terminated. Muscle reoxygena-
damage, especially during the first week of tion times for the control group remained
recovery.26.27It is possible that the damage low and stable across time. During recovery,
occurs because the resumption of normal women who had been on bed rest reported
weight bearing or exercise initially may be symptoms of deep muscle soreness of the
too strenuous for atrophied muscles. Strenu- back, legs, arms, heels, and knees. Two
ous activity, especially that involving muscle women experienced symptoms of a muscle
lengthening, induces an acute muscle injury. tear. All women on bed rest had difficulty
Similar to an exercise-induced muscle injury, walking, especially with ascending and de-
repair and remodeling of the injured atro- scending stairs, while none in the control
phied muscle occur eventually.29.31 group experienced these symptoms.
Several symptoms, including muscle sore- An additional national retrospective study
ness, swelling, and edema, are associated supports these findings (J.A.M., unpublished
with recovery from muscle atrophy. These data, 2002). A randomly selected sample of
symptoms are similar to those experienced 89 women who were prescribed antepartum
by individuals who have undergone strenu- bed rest completed a checklist identifying
ous or unaccustomed exercise. 32 Muscle the symptoms experienced during postpar-
soreness usually develops within 24 to 48 tum recovery. Symptoms experienced by
hours, peaks at 72 hours, then subsides at 5 more than 50% of women included back
to 7 daYS.33Soreness is believed to be associ- muscle soreness; difficulty walking and in
ated with muscle tissue damage. LeBlanc19 negotiating stairs, particularly when ascend-
states that sore leg muscles often are re- ing; dizziness; shortness of breath; and fa-
ported after both short and long space tigue. Symptoms that were reported by more
flights. Muscle cramps, tears, strain, chronic than 25% of women included muscle sore-
pain, and fatigue may be common during re- ness in arms, heels, knees, and upper and
covery.33.34Swelling may be due to several lower leg muscles; knee buckling; swollen
causes including inflammation or pooling of ankles or feet; and difficulty descending
body fluids in the lower limbs. 19Thus, a vari- stairs. Nine percent of women reported post-
ety of symptoms appear to occur during re- partum falls. Thus, current evidence suggests
covery from muscle disuse and the cause(s) that pregnant women who are prescribed
of these symptoms vary. antepartum bed rest experience symptoms
Vol. 13, No.2 May 2002 PREGNANCY MUSCLE DISUSE . 251
associated with muscle deconditioning dur- ing the postpartum, women who have previ-
ing recovery, similar to those experienced in ously been on antepartum hospital bed rest
nonpregnant populations. will demonstrate a decrease in muscle re-
The presence of adverse physiologic ef- oxygenation time after exercise from an-
fects of antepartum bed rest that extend into tepartum discharge through 6 weeks post-
postpartum recovery is of concern for three partum as measured by T 1/2 muscle
reasons. First, antepartum bed rest is pre- reoxygenation time. An additional research
scribed for large numbers of women.2 Sec- question was to describe the symptoms as-
ond, research has failed to document the ef- sociated with muscle deconditioning and re-
fectiveness of bed rest for improving covery across the postpartum period.
fetal/infant or maternal mortality or morbid-
ity.2,7,8,39
Third, current data, which is consis-
tent with that of aerospace research, now o Methods
suggest that antepartum bed rest treatment
has significant side effects. However, an- Women treated with antepartum bed rest
tepartum bed rest therapy continues to be were assessed for symptoms of muscle dys-
prescribed without apparent regard for these function using a repeated measures longitu-
effects. 2,5 dinal design.
Side effects such as muscle atrophy may
place women at increased risk for long- Subjects
term sequelae such as permanent muscle
damage. Women may also be at risk for The convenience sample consisted of 65
fractures and an early osteoporosis as bed women who were studied from enrollment
rest also induces bone 10SS.9,19Whether upon antepartum hospital admission
such bone loss is totally reversible is not through 6 weeks postpartum. The data pre-
known.1l,28 There is some evidence for an- sented here are for a subset of subjects who
tepartum depression3 and for adverse an- participated in a larger study of the physio-
tepartum psychosocial effects on the hus- logic and psychosocial side effects of an-
band and the family.4,40If further evidence tepartum bed rest. Subjects were recruited
about the adverse physiologic and psy- from the antepartum inpatient units of three
chosocial side effects of antepartum bed tertiary care, university affiliated hospitals in
rest is supported, it would suggest that an- two midwestern cities. Pregnant women di-
tepartum bed rest treatment should not be agnosed with a pregnancy complication
prescribed because it is both ineffective who were prescribed bed rest were eligible
and iatrogenic. Therefore, the specific to participate. Criteria for inclusion were
aims of this study were to determine women who were between 21 and 33 weeks
whether women on antepartum bed rest gestation, at least 16 years of age, healthy
demonstrate change in gastrocnemius prior to pregnancy, 'and able to read and
muscle metabolism across time from an- speak English. Subjects were limited to
tepartum hospital admission through 6 women with the diagnosis of preterm labor,
weeks postpartum, and to describe the preterm rupture of membranes, placenta
symptoms indicative of muscle decondition- previa, placental abruption, incompetent
ing and recovery in the postpartum period. cervix, multiple gestation, or a combination
of these conditions. Women were excluded
if they had any acute or chronic metabolic
o Hypotheses disease such as chronic hypertension, preg-
nancy-induced hypertension, asthma, dia-
During the antepartum, pregnant women on betes mellitus, an admission diagnosis of
hospital bed rest will demonstrate an in- gestational diabetes, or any impairment in
crease in muscle reoxygenation time after muscle function or mobility.
exercise from hospital admission through Subjects were primarily white (63.1%),
the end of antepartum hospitalization, as and married (60%), with ages ranging from
measured in TI/z muscle reoxygenation time 16 to 40 (mean 28.0, SD 6.8). Years of mater-
(TI/z = one half of the time in seconds). Dur- nal education ranged from 8 to 21 (mean
252 . MALONI AND ST PIERRE AACN Clinical Issues
13.9, SD 2.9) and 36% of women had globin! myoglobin (Hb/Mb) spectropho-
household incomes at or below $30,000. tometer (Runman) invented by Dr Britton
Most women were multigravidas (80%), al- Chance of the University of Pennsylvania.
though only half of these had a living child. The Runman was used in the investigator's
Women were diagnosed with preterm labor previous study and differentiated muscle re-
(27.7%); preterm labor combined with an- oxygenation after short-term exercise for
other of the above inclusion pregnancy di- women on bed rest and that of the control
agnoses (33.8%); preterm rupture of mem- group of pregnant women not on bed rest.3
branes (18.5%); placenta previa (7.7%); The Runman examines muscle metabo-
placental abruption (3.3%); or a combination lism by measuring oxygenation/deoxygena-
of non-preterm labor diagnoses (9%). Eigh- tion of muscle tissue. The Runman has been
teen percent of the pregnancies were multi- used to assess oxygenation of tissue in adult
ple gestations. The gestational age of the brain after circulatory arrest after pacemaker
pregnancy upon hospital admission ranged removal,41 as well as the oxygenation of the
from 21 to 33 weeks (mean 28.4; SD 3.0), fetal brain,42 and respiratory muscle.43 The
whereas the mean gestational age at birth Runman also has been used to assess reoxy-
was 34.1 weeks (SD 3.3) and ranged from 24 genation of the quadriceps of 22 elite com-
to 40 weeks. Sixty-six percent of women had petitive male and female rowers44 and in
a vaginal delivery, 21.1% had an elective ce- three studies of the gastrocnemius muscle of
sarean section, and 12.3% had an emergency non-pregnant, non-bed rest, subjects.45-47
cesarean section. The length of hospital bed Although the capability of the Runman to
rest ranged from 5 to 70 days (mean 24.77, assess deoxygenation/reoxygenation re-
SD 14.6). Twenty-six women (40%) were on sponses in a variety of populations has been
bed rest at home prior to hospital enrollment validated, norms for various populations
for a mean length of 22.7 days (SD 18.24, have not yet been established.
range 2-89). The Runman pulses near red light waves
(760 and 850 nm) through superficial tissue
Measures to obtain signals from the Hb/Mb content of
the muscle during exercise and exercise re-
A list of variables and instruments used to covery.44The difference in absorption at the
assess them is given in Table 1 two wavelengths approximates desaturation
MUSCLE METABOLISM. Measurement of mus- of Hb/Mb during exercise and resaturation
cle disuse in high-risk pregnant women during recovery.44,48-50A small-rubberized
placed on bed rest presented unique chal- encasement (probe) about the size of a large
lenges as standard methods of muscle as- wristwatch containing silicon diodes and in-
sessment involve rigorous activity and are terference filters is placed over the muscle
contraindicated.3 Anthropometric measure- and secured by a Velcro band. Light waves
ment, muscle biopsy, and magnetic reso- penetrate through superficial tissue to pick
nance imaging were considered but re- up signals of deoxygenation and resatura-
jected because of lack of reliability, tion of the muscle. The Runman is combined
excessive cost or discomfort, or potential with a portable ergometer (pedal) to con-
danger to the fetus. Therefore, muscle me- duct plantar flexion exercise so that patterns
tabolism was assessed using the new exper- of deoxygenation in response to exercise
imental noninvasive dual wavelength hemo- can be observed. Signals of oxygenation and
TABLE1. Study Variablesand Instruments
Variable Instrument
Muscle metabolism Hemoglobin/myoglobin spectrophotometer and
ergometer
Postpartum muscle symptoms Postpartum symptoms checklist
Postpartum mobility Postpartum symptoms checklist
Vol.13, No.2 May 2002 PREGNANCYMUSCLEDISUSE . 253 deoxygenation are recorded by a strip chart muscle fatigue. The exercise took on the av- recorder (Figure 1). The amount of time in erage approximately 3 minutes and did not seconds needed to recover from exercise to induce full body fatigue. Monitoring and a baseline level of reoxygenation after exer- graphing of reoxygenation of muscle after cise divided by 2 (T 1/2 recovery time) is exercise took an additional 2 minutes. The used as the score.44 Longer muscle reoxy- exercise did not appear to affect decondi- genation times indicate prolonged recovery tioning resulting from muscle disuse. from oxygen-induced debt stimulated by ex- POSTPARTUM SYMPTOMS. Postpartum symp- ercise.44 Use of the Runman poses no risk or toms associated with muscle disuse were as- discomfort to the person. sessed with a self-report Postpartum Symp- Two teams of two data collectors tested tom Checklist. The checklist consists of 49 subjects in their hospital rooms using a stan- items, which assess the influence of bed rest dardized protocol.3 One directed the exer- upon the various organ systems. Only symp- cise while the other operated the Runman toms associated with muscle disuse (n = 12) and strip chart recorder. Women sat in bed or mobility (n = 7) are reported here. The in a semi-Fowlers position with legs ex- checklist was developed by the investigator tended and knees fixed (Figure 2). The gas- based on clinical experience with women on trocnemius muscle was used for assessment bed rest and from an extensive review of the of muscle disuse because it is a postural literature on bed rest and pregnancy. Items weight-bearing muscle. It consists of pre- assessing mobility were adapted from re- dominately slow oxidative Type I fibers that search with the elderly5253as a simple, effec- alter their contractile speed and enzymatic tive, and inexpensive method of assessing capacity when weight bearing is removed. 51 gross mobility problems among young, This muscle is superficial to the skin and healthy subjects had not been developed. thus is easily accessible for measurement. Items assess whether the person (1) needs The probe was placed over the gastrocne- support to walk; (2) hesitates before walk- mius muscle and covered with a lightly ing; (3) walks using each foot alternately; (4) wrapped ace bandage to prevent the escape experiences difficulty with knees buckling; of light. Women conducted intermittent has difficulty (5) ascending or (6) descend- plantar flexion exercises by pressing on a ing stairs; or (7) has difficulty transferring to pedal against 10 pounds of pressure for a a sitting position. Appropriateness of the distance of 5 inches. Plantar flexions were items was judged by peer review. Items executed once every 10 seconds until a were tested and revised to include other baseline of deoxygenation was achieved, symptoms identified in the pilot study. In a then once every 5, 2, and 1 second, and then subsequent study, the Postpartum Symptom maximal effort until the woman reported Checklist distinguished symptoms between Figure1. Patternfor deoxygenationduringexercisetestingandreoxygenationduring recovery from exercise.
254 . MALON! AND ST PIERRE AACN Clinical Issues
Hb/Mb Spectrophotometer
!
Strip Figure 2. Setup for spectrophotome-
Recorder ter (Runman) testing.
women on bed rest and pregnant women data collection, with the exception of two
who did not receive bed rest.4 Cronbach al- days after delivery, occurred in the subjects'
pha was established at O. 84. The symptom homes. A baseline measure of muscle me-
checklist was administered by the data col- tabolism was obtained upon hospital admis-
lector and scored as present or absent. The sion, and at the end of the antepartum, and
checklist took approximately 3 to 4 minutes at 6 weeks postpartum. Postpartum symp-
to complete. tom data were collected at 2 days after deliv-
DEMOGRAPHICS. An expanded form of the ery and weekly through 6 weeks. Demo-
Demographic and Medical History Instru- graphic and perinatal data were obtained
ment3 was used to obtain descriptive data upon enrollment and updated using the
from the hospital record and from patient in- medical record as new conditions emerged.
terview. Information about maternal demo- Subjects received a $50 incentive for partici-
graphic and perinatal characteristics includ- pating in the study.
ing sample descriptor variables such as
previous history of home and hospital bed
rest for this and previous pregnancies was o Statistical Analyses
obtained.
PROCEDURE. The medical records of poten- Data were analyzed using the Statistical
tial subjects were screened for their appro- Package for the Social Sciences (SPSS) 10.0
priateness for entry into the study. Informed for windows. Descriptive statistics and Stu-
consent was obtained after study approval dent t tests were computed. Power was cal-
by the Human Subjects Boards. Enrollment culated for the larger study containing multi-
of subjects occurred over a 3.5-year period. ple variables and nine hypotheses. 54For the
Six weeks of data collector training was con- current analysis. hypotheses were directed
ducted prior to enrollment of subjects. After for one group of bed-rested women with
training, data collectors had to successfully three assessments across time. However,
assess gastrocnemius muscle metabolism us- upon analyzing the perinatal data we de-
ing the Runman on 10 different women, at tected a change in the characteristics of the
least 3 of whom had to be on bed rest. Due bed rest treatment across the study. When
to the complexity of the Runman instrument, the study was initiated, pregnant women
procedural reliability was reassessed approx- were admitted directly to the hospital for
imately every 2 months on a random sched- bed rest and remained there until delivery.
ule. Interrater reliability for the Postpartum However, across time home bed rest began
Symptom Checklist was established and re- to be prescribed prior to hospital admission.
assessed quarterly to maintain reliability of As a result the sample consists of both
0.95. women whose bed rest was started upon
hospitalization (n = 39) and women whose
Data Collection bed rest was initiated prior to hospitalization
(n = 26). Because muscle atrophy occurs
Antepartum data collection took place while rapidly,l1 the sample was divided into these
each subject was hospitalized. Postpartum tWo groups for part of the analysis to detect
Vol. 13, No.2 May 2002 PREGNANCY MUSCLE DISUSE . 255
the influence of home bed rest prior to ad- bed rest subjects was not appropriate at this
mission. Thus using a one tailed t test, alpha time, as they may represent values of a pop-
set at 0.05, posthoc power was estimated at ulation to which generalization about effects
0.52 with an effect size of 0.45. need to be made.
Given that the power was low but the ef-
fect size was moderate to high, options were
considered to address the low power. De- o Results
creasing within group variability would in-
crease power. However, the Runman is a During antepartum bed rest, the length of
new experimental assessment tool. The va- time needed for women's gastrocnemius
lidity of the tool for assessing oxygenation! muscle to reoxygenate after exercise signifi-
deoxygenation of tissue has been estab- cantly increased from hospital admission
lished but the range of normal values has through discharge (t = -2.1, P < .05). In
not yet been established. Furthermore, the contrast, the length of time needed for post-
state of. the science in understanding the partum muscle reoxygenation after exercise
physiologic effects of muscle atrophy upon significantly decreased (t = 1.83, P < .05).
pregnant women is limited. In the absence Figure 3 demonstrates the pattern of change
of norms, the variability in muscle reoxy- across the three time periods. Despite signif-
genation scores might represent some factor icant differences in muscle reoxygenation
as yet unknown. Thus, we were hesitant to scores across time, women's scores demon-
eliminate outliers. strated great variability. The type of delivery
Furthermore, although the standard devi- (ie, vaginal versus cesarean section) did not
ations for muscle reoxygenation scores were influence postpartum muscle reoxygenation
large, similar standard deviations were found scores.
in a previous study of 31 healthy pregnant Because 40% of the women were on
women using the Runman (J.A.M., unpub- bed rest prior to hospital admission, sub-
lished data, 2002). Whether or not the range jects were divided into two groups. The
of values contains true outliers is unknown groups consisted of those women who
at this time. However, strip chart recordings were not on bed rest prior to hospital ad-
for eight subjects who appeared to have ex- mission (n = 39) and those who were (n =
treme outliers were reviewed. Three test 26). Muscle reoxygenation scores were sig-
scores were eliminated due to a scoring er- nificantly higher upon enrollment for those
ror. The remaining tests appeared to be valid who had previously been on bed rest (t =
and were included in the data set. Therefore, -8.6, P < .05) but not significantly different
it was decided that elimination of outliers for at the end of the antepartum or postpartum
E 44
E=
= 42
-
.~
~
~
40
~
~
~
38
IX
.E 36
Cj
256 . MALONI AND ST PIERRE AACN Clinical Issues
periods. Figure 4 depicts the patterns for (Table 4). Support to walk was needed
muscle reoxygenation scores for the two across the first week postpartum for a num-
groups. Variability among reoxygenation ber of women and more than 40% needed
scores was greater among women who help to sit. Initially, more than 50% of
were prescribed home bed rest prior to women hesitated before beginning to walk.
hospital admission (Table 2). Most women (77%) began using stairs during
The prevalence of musculoskeletal de- the first week at home. Difficulty negotiating
conditioning symptoms occurring from 2 stairs started at this time. For some women,
days after delivery through 6 weeks postpar- stair-climbing difficulties and knee buckling
tum is listed in Table 3. Soreness in weight- persisted across 6 weeks postpartum.
bearing postural muscles dominated the
symptoms reported by women. Soreness in
back and neck muscles, followed by upper o Discussion
and lower leg soreness, were reported most
frequently and decreased across 6 weeks. A The current study demonstrates that in-
large percentage of women also initially re- creases in the time needed for the gastrocne-
ported arm muscle soreness. At 6 weeks mius muscle to reoxygenate during the an-
postpartum, 45% of women were still experi- tepartum decrease during the first 6 weeks
encing back muscle. soreness and 21% had postpartum. Additionally, the development
persistent neck muscle soreness. Only a few of symptoms of recovery from muscular de-
women reported muscle tears. Fatigue, conditioning and difficulty with mobility
pedal edema, and shortness of breath on ex- during the first 6 weeks postpartum was
ertion were greatest immediately after birth confirmed in the current study. These results
with only high levels of fatigue remaining at support the supposition that muscle atrophy
6 weeks. occurs during antepartum bed rest and re-
Assessment of mobility revealed that dur- covers with remobilization.6.9.1l,28Using a
ing postpartum women experienced diffi- summary of studies, Fortney et al9 created a
culty in all seven areas of walking, which composite description of physiologic re-
rapidly improved across 6 weeks postpartum sponses during bed rest recovery. They re-
44
E
E: 42
=
0
40
=
38 i / "- 1- Bedrest
No Prior
36
"-
34 I
1 / 1- -Prior
Bedrest
-
--
N
Eo- 32
30
First Last Last
Antepartum Antepartum Postpartum
Figure 4. Gastrocnemiusmuscle reoxygenationtime afterexerciseforwomenwho wereprescribedbed rest
prior to hospitalizationand thosewhowerenot.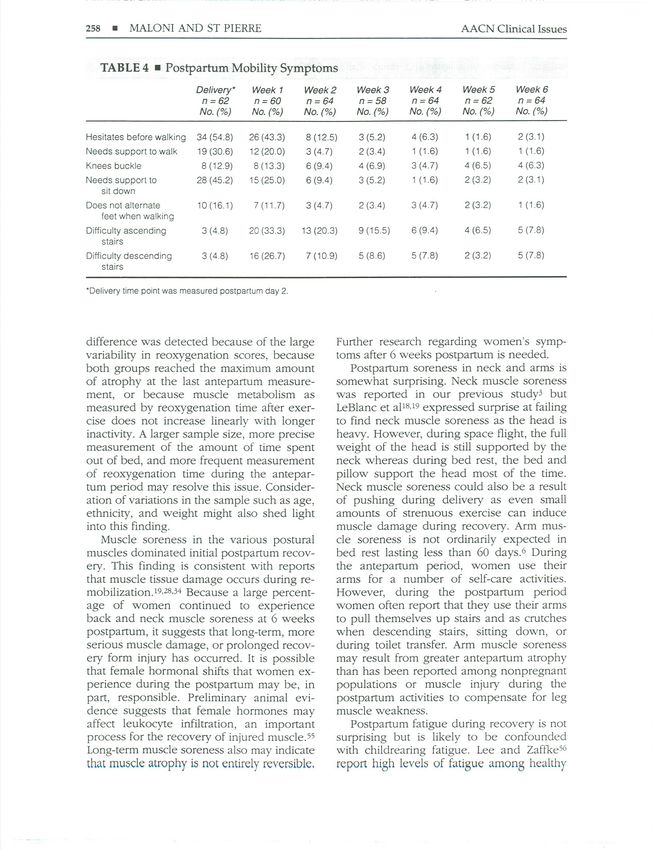
Vol. 13, No.2 May 2002 PREGNANCYMUSCLEDISUSE . 257
TABLE2. Variabilityin MuscleReoxygenation Scores
First Antepartum Last Antepartum Last Postpartum
Mean ~ SO Mean ~ SO Mean ~ SO
No previous bed rest 31.04::t: 15.43 41.72::!: 16.66 34.59 ::!: 16.36
Previous bed rest 39.64 ::!:23.24 39.78:!: 19.88 36.69 ::!:22.56
port that subjects demonstrated generalized on home bed rest were significantly higher
weakness; poor exercise tolerance; distur- at admission but no additional change oc-
bance of coordination, posture, and gait; curred across hospitalization. The lack of
foot pain; difficulty standing without sup- change in the prior bed rest group suggests
port: difficulty walking; and leg pain. The that, at some point, bed rest atrophy reaches
current study results agree with this compos- a plateau similar to astronauts.19 This finding
ite and confirm our previous findings for is also consistent with reports that other or-
pregnant women on bed rest.3.39Study re- gan systems adapt physiologically to this
sults also support findings of atrophy in non- state across time.9,1l
pregnant subjects on bed rest or those par- Longer inactivity is usually accompanied
ticipating in space flight.9.11.18-20
In women by greater atrophy and longer recovery, 11,19
without a prior bed rest history, the steep in- so it was expected that a longer period of in-
crease in muscle reoxygenation times across activity would proportionally affect muscle
the antepartum supports the rapid onset of metabolism as evidenced by a prolonged
muscle deconditioning or atrophy soon after muscle reoxygenation time. Muscle reoxy-
bed rest is started.9.11,18-20 genation scores for women on home bed
Comparisons for the two groups of rest prior to admission remained slightly ele-
women, one of which had been on bed rest vated at six weeks postpartum. However, no
prior to admission, reveal additional under- significant difference in postpartum muscle
standing of the muscle atrophy process. The reoxygenation was detected between the
muscle reoxygenation scores for the women two groups of women. It is possible that no
TABLE 3 . Postpartum Symptoms of Deconditioning
Delivery* Week 1 Week 2 Week 3 Week 4 Week 5 Week 6
n=62 n=60 n=64 n=58 n=64 n=62 n=64
No. (%) No. (%) No. (%) No. (%) No. (%) No. (%) No. (%)
Upper legs sore 24 (38.7) 21 (35.0) 17 (26.6) 8 (13.8) 8 (12.5) 3 (4.8) 4 (6.3)
Lower legs sore 18 (29.0) 24 (40.0) 15 (23.4) 12 (20.7) 8 (12.5) 5 (8.1) 5 (7.8)
Arms sore 17 (27.4) 15 (25.0) 10(15.6) 6 (10.3) 7 (10.9) 5 (8.1) 8 (12.5)
Neck sore 21 (33.9) 20 (33.3) 15 (23.4) 14 (24.1) 17 (26.6) 11 (17.7) 14 (21.9)
Back sore 44 (71.0) 35 (58.3) 27 (42.2) 23 (39.7) 25(39.1) 24 (38.7) 29 (45.3)
Heel sore 13 (21.0) 11 (18.3) 7 (10.9) 5 (8.6) 7 (10.9) 6 (9.7) 5 (7.8)
Knee sore 9 (14.5) 7 (11.7) 7 (10.9) 7 (12.1) 8 (12.5) 9 (14.5) 8 (12.5)
Muscle cramps 28 (45.2) 18 (30.0) 13 (20.3) 5 (8.6) 9 (14.1) 3 (4.8) 9 (14.1)
Muscle tears 0(0) 1 (1.7) 1 (1.6) 0(0) 1 (1.6) 0(0) 1 (1.6)
Shortness of breath 23 (37.1) 19(31.7) 16 (25.0) 8 (13.8) 6 (9.4) 8 (12.9) 6 (9.4)
Fatigue 46 (74.2) 44 (73.3) 40 (62.5) 32 (55.2) 32 (50.0) 27 (43.5) 34(53.1)
Pedal edema 26 (41.9) 24 (40) 11 (17.2) 6 (10.3) 6 (9.4) 6 (9.7) 4 (6.3)
"Delivery time point was measured postpartum day 2,258 . MALONI AND ST PIERRE AACN Clinical Issues
TABLE 4 . Postpartum Mobility Symptoms
Delivery* Week 1 Week 2 Week 3 Week 4 Week 5 Week 6
n=62 n=60 n=64 n=58 n=64 n=62 n=64
No. (%) No. (%) No. (%) No. (%) No. (%) No. (%) No. (%)
Hesitates before walking 34 (54.8) 26 (43.3) 8 (12.5) 3 (5.2) 4 (6.3) 1 (1.6) 2 (3.1)
Needs support to walk 19 (30.6) 12 (20.0) 3 (4.7) 2 (3.4) 1 (1.6) 1 (1.6) 1 (1.6)
Knees buckle 8 (12.9) 8 (13.3) 6 (9.4) 4(6.9) 3 (4.7) 4 (6.5) 4 (6.3)
Needs support to 28 (45.2) 15 (25.0) 6 (9.4) 3 (5.2) 1 (1.6) 2 (3.2) 2 (3.1)
sit down
Does not alternate 10 (16.1) 7 (11.7) 3 (4.7) 2(3.4) 3 (4.7) 2 (3.2) 1 (1.6)
feet when walking
Difficulty ascending 3(4.8) 20 (33.3) 13 (20.3) 9 (15.5) 6 (9.4) 4 (6.5) 5 (7.8)
stairs
Difficulty descending 3 (4.8) 16 (26.7) 7 (10.9) 5 (8.6) 5 (7.8) 2 (3.2) 5 (7.8)
stairs
"Delivery time point was measured postpartum day 2.
difference was detected because of the large Further research regarding women's symp-
variability in reoxygenation scores, because toms after 6 weeks postpartum is needed.
both groups reached the maximum amount Postpartum soreness in neck and arms is
of atrophy at the last antepartum measure- somewhat surprising. Neck muscle soreness
ment, or because muscle metabolism as was reported in our previous study3 but
measured by reoxygenation time after exer- LeBlanc et aP8.19expressed surprise at failing
cise does not increase linearly with longer to find neck muscle soreness as the head is
inactivity. A larger sample size, more precise heavy. However, during space flight, the full
measurement of the amount of time spent weight of the head is still supported by the
out of bed, and more frequent measurement neck whereas during bed rest, the bed and
of reoxygenation time during the antepar- pillow support the head most of the time.
tum period may resolve this issue. Consider- Neck muscle soreness could also be a result
ation of variations in the sample such as age, of pushing during delivery as even small
ethnicity, and weight might also shed light amounts of strenuous exercise can induce
into this finding. muscle damage during recovery. Arm mus-
Muscle soreness in the various postural cle soreness is not ordinarily expected in
muscles dominated initial postpartum recov- bed rest lasting less than 60 days.6 During
ery. This finding is consistent with reports the antepartum period, women use their
that muscle tissue damage occurs during re- arms for a number of self-care activities.
mobilization.19.28.34Because a large percent- However, during the postpartum period
age of women continued to experience women often report that they use their arms
back and neck muscle soreness at 6 weeks to pull themselves up stairs and as crutches
postpartum, it suggests that long-term, more when descending stairs, sitting down, or
serious muscle damage, or prolonged recov- during toilet transfer. Arm muscle soreness
ery form injury has occurred. It is possible may result from greater antepartum atrophy
that female hormonal shifts that women ex- than has been reported among nonpregnant
perience during the postpartum may be, in populations or muscle injury during the
part, responsible. Preliminary animal evi- postpartum activities to compensate for leg
dence suggests that female hormones may muscle weakness.
affect leukocyte infiltration, an important Postpartum fatigue during recovery is not
process for the recovery of injured muscle.55 surprising but is likely to be confounded
Long-term muscle soreness also may indicate with childrearing fatigue. Lee and Zaftke56
that muscle atrophy is not entirely reversible. report high levels of fatigue among healthyVol. 13, No.2 May 2002 PREGNANCY MUSCLEDISUSE . 259
mothers because of fragmented sleep. Fur- o Nursing Implications
ther study may reveal whether the fatigue
experienced by those previously on bed rest The implications of these findings for nurs-
is different in magnitude or quality. ing are numerous. In the absence of elimi-
Postpartum symptoms disappeared rapidly nating pregnancy bed rest treatment, a com-
for most women. Women are highly moti- mon thought is to prevent atrophy by using
vated to resume ambulation to care for the antepartum exercise. Astronauts have at-
infant. Early ambulation may be helpful in tempted to do so but have only been par-
tially successful. 6.28 The type of exercise
restoring function but women may be prone
to falls. This is of grave concern for two rea- needed to offset atrophy is intensive and in-
sons. First, women may be carrying their in- volves heavy resistance training.6 This type
of exercise is not conunonly used by healthy
fants and both could be injured during a
fall. Second, aerospace research shows a women and is currently contraindicated dur-
strong correlation between bed rest induced ing a high-risk pregnancy. However, an-
muscle loss and bone loss, with recovery of tepartum exercise involving increased
bone lagging behind that of muscle.6.9.19 weight bearing might help reduce muscle at-
Thus, during resumption of walking women rophy. In addition, a systematic assessment
of muscle weakness and an accompanying
may also be at risk for fractures, particularly
at the point when muscles have reached program of postpartum rehabilitation may
facilitate recovery and prevent long-term in-
their maximal strength but bone has not.6
Women's muscle reoxygenation scores jury of muscle and bone.
After inactivity, the goal is to enable
exhibited a large degree of variability across
women to return to a normal level of physi-
time, especially for those on previous home
cal activity without injury.34 A number of
bed rest. Several explanations could account measures will facilitate maternal recovery
for this finding. First of all, aerospace re-
and are suggested for nursing practice.
searchers have found variability in muscle
These include assessing for:
atrophy obtained by a variety of assessment
methods.19 Researchers using the Runman in
nonpregnant samples have also found large
. the type of physical activity conducted
prior to bed rest to know what kinds of
variability (personal communication,
Chance, March, 2001). However, the vari-
B.
. activity the woman will resume;
the duration of home and hospital bed rest
ability for our pregnant sample is somewhat
larger than expected. The variability could
be due to measurement error, variations in
. and the severity of activity restriction;
muscle weakness to determine which
muscle groups are most seriously af-
the length of bed rest among the sample
(range 5-70 hospital days), or the influence
of subject activity. All women were allowed
. fected by bed rest;
symptoms of difficulty walking, de-
creased strength, fatigue, and other
out of bed each day to go to the bathroom symptoms associated with muscle recov-
and it is not uncommon for women to walk
to the bathroom 10 to 13 times per day.
While such trips usually last 5 minutes or
. ery and ambulation-induced injury;
symptoms of postpartum depression asso-
ciated with postpartum loss of function
less, some women linger for longer periods. and independence or antepartum stress;
and
Variability could also indicate that preg-
nancy might influence muscle metabolism
in some way that is not yet understood. A
. family problems related to the stress of
having a high-risk pregnancy.
large degree of variability was also demon- Nurses also should advise the woman to:
strated in our study of healthy pregnant
women who were not on bed rest (J.A.M., . begin weight-bearing activity to facilitate
unpublished data, 2002). Additional re-
search is needed to clarify these issues. Fur- . recovery; .
remobilize carefully to avoid overusing
ther research is needed to define the range
of normal values for deoxygenation re-
sponse to exercise among healthy and high-
. muscles and inducing further damage;
exert caution as there is a potential for
falls due to knee buckling and decreased
risk pregnant women. leg strength;260 . MALONI AND ST PIERRE AACN Clinical Issues
· rebuild back and leg muscles through
gradual exercise as these muscle groups
to document women's postpartum com-
plaints about muscle dysfunction, muscle
· are most likely to be weak;
consult with a healthcare professional
who is familiar with both exercise and
soreness, physical limitations that inhibit en-
gagement in activities, and the time at which
women reach full postpartum functional ca-
assessment of muscle function and de- pacity after antepartum bed rest.
· conditioning about postpartum exercise;
exert caution even when muscle groups
reach normal functioning as bone mass is o Summary
still in the process of restoration;
· expect limited strength, fatigue, and Pregnant women who are prescribed bed
muscle soreness as a result of pregnancy rest experience significant changes in mus-
· bed rest treatment;
report symptoms after bed rest to their
healthcare provider;
cle metabolism while hospitalized and a sig-
nificant reversal of these changes in the
postpartum. The postpartum period is also
· use acetaminophen, if possible, instead characterized by symptoms commonly asso-
of nonsteroidal anti-inflammatory drugs ciated with recovery from muscle
(NSAIDS) for symptom relief, as NSAIDS atrophy / deconditioning. Numerous nursing
may interfere with macrophage function actions can facilitate maternal postpartum re-
· and delay recovery from injury;
expect that fatigue might occur during
physical activity and that function, inde-
covery and prevent long-term injury to mus-
cle and bone.
pendence, and mobility eventually will Acknowledgments
be restored;
· increase sufficient protein intake to en- This study is funded by a grant from the Na-
sure muscle repair, especially in later tional Institute of Health, National Institute
part of the muscle recovery period. of Nursing Research ROI-NRO-3323. The au-
thor thanks Sarah Korkowski for her assis-
Patient referrals will be necessary for: tance.
· an in-depth assessment of muscle weak-
ness and development of a planned pro-
gram of rehabilitation, and References
· obtaining instrumental support for assis-
tance with completing household tasks. 1. Enkin M, Keirse M, Renfrew M, Neilson J. A
Guide to Effective Care in Pregnancy and
Childbirth. 2nd ed. New York: Oxford Uni-
In addition, the results have major impli-
cations for research. Further research is versity Press; 1995.
needed in this population to determine 2. Goldenberg RL, Cliver SP, Bronstein J, Cutter
GR, Andrews WW, Mennemeyer ST. Bed rest
whether recovery of muscle mass is accom-
in pregnancy. Obstet Gynecol. 1994;84:131-
panied by a return of endurance. Endurance 136.
among subjects on bed rest has rarely been 3. Maloni J, Chance B, Zhang C, Cohen A, Betts
studied, and anecdotal evidence from our D, Gange S. Physical and psychosocial side
subjects indicates that recovery of muscle effects of antepartum hospital bed rest. NuT'S
function is not accompanied by endurance. Res. 1993;42:197-203.
There has not been any research about the 4. Maloni J, Tomasi J, Johnson L. Antepartum
optimal mode, duration, and intensity of ex- bed rest: effect upon the family. J Obstet Gy-
ercise training that bed rest patients can use necol Neonatal NuT'S.2001;30:165-173.
to minimize musculoskeletal deconditioning. 5. Maloni J, Cohen A, Kane J. Prescription of ac-
tivity restriction to treat high-risk pregnan-
Additional research is needed regarding the cies. J Womens Health. 1998;7:165-173.
recovery of other organ systems. Lastly, 6. Bloomfield SA. Changes in musculoskeletal
complaints about postpartum symptoms af- structure and function with prolonged bed
ter bed rest often are dismissed because of rest. Med Sci Sports Exerc. 1997;29:197-206.
lack of physician awareness of the side ef- 7. Maloni J. Bed rest and high-risk pregnancy:
fects of bed rest. Further research is needed differentiating the effects of diagnosis, settingVol. 13, No.2 May 2002 PREGNANCY MUSCLE DISUSE . 261
and treatment. Nurs Clin North Am. muscle by hind limb unweighting. ] Appl
1996;31:313-325. Physiol. 1990;68:1-12.
8. Maloni J, Kasper CEoPhysical and psychoso- 24. Edgerton YR, Zhou M, Ohira Y, et at. Human
cial effects of antepartum hospital bedrest: a fiber size and enzymatic properties after 5
review of the literature. Image] Nurs Sch. and 11 days of space flight. ] Appl Physiol.
1991;23:187-192. 1995;78:1733-1739.
9. Fortney SM, Schneider VS, Greenleaf JE. The 25. Tesch PA, Berg H, Haggmark T, Ohlsen H,
physiology of bed rest. In: Fregly MJ, Blatteis Dudley GA. Muscle strength and endurance
CM, eds. Handbook of Physiology: Section 4: following lower limb suspension in man.
Environmental Physiology III. New York: Ox- Physiologist. 1991;34:S104-S106.
ford Press; 1996;889-939. 26. Kasper C. Spatial patterns of atrophied mus-
10. Rubin M. The physiology of bed rest. Am] cle fibers during exercised recovery. Bioi Res
Nurs. 1988;88:50-55. Nurs.1999;1:38-47.
11. Sandler H, Vernikos). Inactivity: Physiologi- 27. Kasper C, White T, Maxwell L. Running dur-
cal Effects. Orlando, Fla: Academic Press; ing recovery from hind limb suspension in-
1986. duces muscle injury. ] Appl Physiol. 1990;68:
12. Ryder J, Gilbert M, Zierath). Skeletal muscle 533-539.
and insulin sensitivity: pathophysiological al- 28. Prou E, Marini JF. Muscle research in space:
terations. Front Biosci. 2001;6:D154-D163. increased muscle susceptibility to exercise-
13. Blanc S, Normand S, Pachiaudi C, Fortrat J, induced damage after a prolonged bedrest.
Laville M, Gharib C. Fuel Homeostasis during Int] Sports Med. 1997;18(suppl 4):S317-
physical inactivity inducted by bed rest. ] Clin S320.
Endocrinol Metab. 2000;85:2223-2233. 29. St Pierre BA, Tidball). Differential response
14. Booth F. Time course of muscular atrophy of macrophage subpopulations to soleus
during immobilization of rats. ] Appl Physiol. muscle reloading after rat hind limb suspen-
1977;656-661. sion.] Appl Physiol. 1994;77:290-297.
15. Booth F, Seider). Early change in skeletal 30. Krippendorf B, Riley D. Distinguishing un-
muscle protein synthesis after limb immobi- loading versus reloading-induced changes in
lization of rats. ] Appl Physiol. 1979;47:974- rat soleus muscle. Muscle Neroe. 1993;16:99-
977. 108.
16. Tucker K, Seider M, Booth F. Protein synthe- 31. Kellett). Acute soft tissue injuries: a review of
sis rates in atrophied gastrocnemius muscles the literature. Med Sci Sports Exerc. 1986;
after limb immobilization. ] Appl Physiol. 18:489-500.
1981;51:73-77. 32. Schneider B, Sannes H. Consequences of
17. Gogia P, Schneider V, LeBlanc A, Krebs ], skeletal muscle injury induced by accus-
Schonfeld E, Evans H. Bed rest: effects on ex- tomed exercise. Ortho Nurs. 2001;20:49-56.
tremity muscle torque in healthy men. Arch 33. Armstrong R. Mechanisms of exercise in-
Phys Med Rehabil. 1988;69:1030-1032. duced delayed onset muscular soreness: A
18. LeBlanc A, Rowe R, Schneider V, Evans H, brief review. Med Sci Sports Exerc. 1984;
Hedrick T. Regional muscle loss after short 16:529-538.
duration space flight. Aviat Space Environ 34. St Pierre BA, Flaskerud JH. Clinical nursing
Med.1995;66:1151-1154. implications for the recovery of atrophied
19. LeBlanc A, Lin C, Shackelford L, et al. Muscle skeletal muscle following bed rest. Rehabil
volume, MID relaxation times (T2), and body Nursing. 1995;20:314-317.
composition after space flight. ] Appl Physiol. 35. Heaman M. Stressful life events, social sup-
2000;89:2158-2164. port, and mood disturbance in hospitalized
20. LeBlanc A, Rowe R, Evans H, West S, Shack- and nonhospitalized women with pregnancy
elford L, Schneider V. Muscle atrophy during induced hypertension. Can] Nurs Res. 1992;
long duration bed rest. Int] Sports Med. 24:23-37.
1997;18(suppI4):S283-S285. 36. Heaman M, Gupton A. Perceptions of bed
21. LeBlanc A, Schneider V, Evans H, Peintok C, rest by women with high-risk pregnancies: a
Rowe R, Spector E. Regional changes in mus- comparison betWeen home and hospital.
cle mass following seventeen weeks of bed Birth. 1998;25:252-258.
rest.] Appl Physiol. 1992;173:2172-2178. 37. Schroeder CA. Women's experience of bed
22. Desplanches D. Structural and functional rest in high-risk pregnancy. Image] Nurs 5ch.
adaptations of skeletal muscle to weightless- 1996;28:253-258.
ness. Int] Sports Med. 1997;18(suppl 4):S259- 38. Maloni], Kutil R. Antepartum support group
s264. for women hospitalized on bed rest. Matern
23. Thomason D, Booth F. Atrophy of the soleus Child Nursj. 2000;25:204-210.262 . MALONI AND ST PIERRE AACN Clinical Issues
39. Chalmers I, Enkin M, Keirse M. Effective Care sured by ne-ar red spectroscopy. Presented at:
in Pregnancy and Childbirth. Oxford: Oxford American College of Sports Medicine Annual
University Press; 1991. Meeting; May 30, 1991; Orlando, Fla.
40. Maloni j, Ponder MB. Fathers' experience of 48. Chance B, Maris M, Sorge j, Zhang M. A
their partners' antepartum bed rest. J Obstet phase modulation system for dual wave-
Gynecol Neonatal Nurs. 1997;29:183-188. length difference spectroscopy of hemoglo-
41. Smith D, Levy W, Maris M, Chance B. Reperfu- bin deoxygenation in tissues. Proceedings of
sion hypoxia in the brain after circulatOIYar- SPIE. 1990;1204:481-491.
rest in humans. Anesthesiology. 1990;73:12-19. 49. Chance B, Zhang M, Sorge j, Leight j, jurth D,
42. Benaron DA, Kurth CD, Steven jM, Delivoria- Nioka S. A 100MH dual wavelength phase
Papadopoulos M, Chance B. Transcranial op- modulation spectrophotometer. Biophys J.
tical path length in infants by near-infrared 1990;57:189.
phase-shift spectroscopy. J Clin Monit. 1995; 50. Chance B, Nioka S, Kent j, et al. Time re-
11:109-117. solved spectroscopy of hemoglobin and myo-
43. Mancini D, Ferraro N, Nazzaro D, Chance B, globin in resting and ischemic muscle. Anal
Wilson J. Respiratory muscle deoxygenation Biochem.1988;174:698-707.
during exercise in patients with heart failure 51. Reiser P, Kasper C, Moss R. Myosin subunits
demonstrated with near-infrared spec- and contractile properties of single fibers
troscopy. JAm Coli Cardiol. 1991;18:492-498. from hypokinetic rat muscles. J Appl Physiol.
44. Chance B, Dait M, Zhang C, Hamaoka T, 1987;63:2293-2300.
Hagerman F. Recovery from exercise induced 52. Imms S, Edholm O. The assessment of gait and
desaturation in the quadriceps muscle of elite mobility in the elderly. Proceedings from the
competitive rowers. Am J Physiol. 1992;262: Conference on the Ageing Brain. 1978;7-10.
C766-C775. 53. Tinetti M, Ginter S. Identifying mobility dys-
45. Wilson j, Mancini D, McCully K, Ferrara N, function in elderly patients. JAMA. 1988;259:
Lanoce V, Chance B. Noninvasive detection 1190-1193.
of skeletal muscle under perfusion with near- 54. Cohen j. Statistical Power Analysis for the Be-
infrared spectroscopy. Circulation. 1989;80: havioral Sciences. 2nd ed. Hillsdale, NJ: Erl-
1668-1674. baum; 1988.
46. Mancini D, Chance B, Wilson J. Effect of 55. Schneider B, Correia L, Cannon J. Sex differ-
dobutamine on skeletal muscle oxygenation ences in leukocytes invasion in injured mus-
assessed by near infrared spectroscopy. Heart cle. Res Nurs Health. 1999;22:243-250.
Fail. 1990;65:1121-1126. 56. Lee K, Zaffke M. Longitudinal changes in fa-
47. Hamaoka T, Albani C, McCully K, Chance B. tigue and energy during pregnancy and the
Prolonged recovery of muscle capillary oxy- postpartum period. J Obstet Gynecol Neonatal
genation levels following triathalon as mea- Nurs. 1999;28:183-191.You can also read