Interruption of lymphatic filariasis transmission in Manaus, a former focus of Wuchereria bancrofti in the Western Brazilian Amazon - PAHO IRIS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Original research Pan American Journal
of Public Health
Interruption of lymphatic filariasis transmission in
Manaus, a former focus of Wuchereria bancrofti in the
Western Brazilian Amazon
Marilaine Martins,1 Rebeca Cristina Souza Guimarães,2 and Gilberto Fontes3
Suggested citation Martins M, Guimarães RCS, Fontes G. Interruption of lymphatic filariasis transmission in Manaus, a former focus of Wuchereria
bancrofti in the Western Brazilian Amazon. Rev Panam Salud Publica. 2021;45:e1. https://doi.org/10.26633/RPSP.2021.1
ABSTRACT Objective. To confirm the absence of Wuchereria bancrofti autochthonous cases in Manaus, a former focus of
lymphatic filariasis in the Western Brazilian Amazon.
Methods. A field survey was carried out in 2016 using immunochromatographic rapid tests (ICT card) for the
detection of circulating filarial antigens in blood. The sample included a group of 3 000 schoolchildren aged 6
to 10 years enrolled in schools from different urban areas of Manaus (including the former lymphatic filariasis
focus in the city) and a group of 709 adolescents and adults, between the ages of 11 and 85 years, born and
raised in different areas of Manaus.
Results. All of the individuals tested negative for W. bancrofti antigen.
Conclusions. Although Manaus was once considered endemic, this focus no longer seems to be active for
lymphatic filariasis transmission. The results of this study could support the certification by the World Health
Organization of the lymphatic filariasis transmission elimination exercise in Brazil.
Keywords Wuchereria bancrofti; elephantiasis, filarial; Brazil.
Lymphatic filariasis (LF) is a vector-borne neglected tropical In the Americas, the disease is caused exclusively by W. ban-
disease with serious social and economic impact. It is caused by crofti. It is believed to have been introduced as a result of the
three nematode species, Brugia malayi, B. timori, and Wuchereria slave trade from Africa, the most unfortunate and tragic legacy
bancrofti, the last of which is the main etiological agent, respon- of colonialism (4). Culex quinquefasciatus mosquitoes are consid-
sible for more than 90% of cases (1, 2). ered to be the only competent vector species in this continent
The disease impairs the lymphatic system, leading to (5). The parasite microfilariae found in patients circulate in the
chronic disability such as lymphedema, hydrocele, and ele- peripheral blood mainly at night (nocturnal periodicity) (6),
phantiasis, and is considered a global public health problem and can be detected in thick blood smear samples taken for
by the World Health Organization (WHO) (1, 2). Currently, diagnostic purposes.
LF is found in 49 countries in Asia, Africa, and the Ameri- In 1997, the World Health Assembly (Resolution WHA 50.29)
cas, affecting approximately 100 million people, and putting set the year 2020 as the target for the elimination of LF as a
around 893 million people at risk of acquiring it (1, 2). The global public health problem (7). In 2000, WHO launched the
two most recent countries to receive validation from WHO for Global Programme to Eliminate Lymphatic Filariasis to achieve
the elimination of LF are Yemen and Kiribati, a Pacific island this goal (8). As per WHO recommendations, the main strategy
nation (3). to interrupt LF transmission is mass drug administration. This
1
Fundação de Medicina Tropical Dr. Heitor Vieira Dourado, Manaus, Brazil 2
Instituto Leônidas e Maria Deane/Fiocruz Amazônia, Manaus, Brazil
* Marilaine Martins, marilaine@fmt.am.gov.br 3
Universidade Federal de São João del-Rei, Divinópolis, Brazil
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 IGO License, which permits use, distribution, and reproduction in any medium, provided the
original work is properly cited. No modifications or commercial use of this article are permitted. In any reproduction of this article there should not be any suggestion that PAHO or this article endorse any specific organization
or products. The use of the PAHO logo is not permitted. This notice should be preserved along with the article’s original URL.
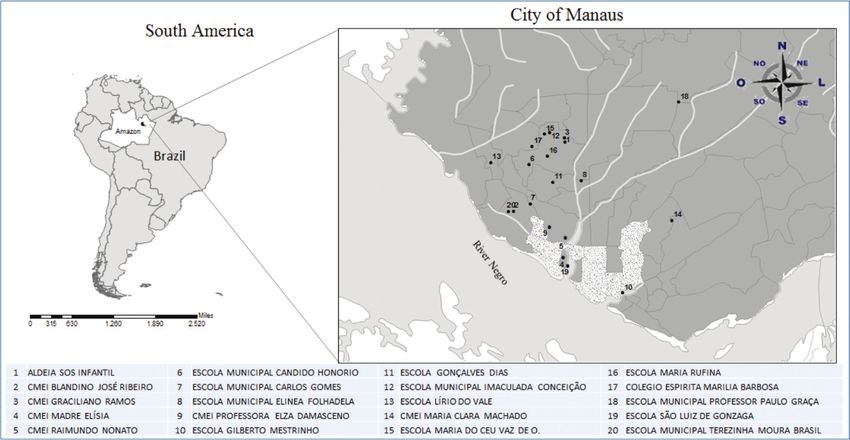
Rev Panam Salud Publica 45, 2021 | www.paho.org/journal | https://doi.org/10.26633/RPSP.2021.1 1Original research Martins et al. • Interruption of lymphatic filariasis in Manaus should be followed by a Transmission Assessment Survey and MATERIALS AND METHODS monitoring (9). LF foci persist in four countries of the Americas: Brazil, the Study area Dominican Republic, Guyana, and Haiti (10, 11). Endemic areas of LF along the northeastern coast of Brazil are limited to Recife, The study was conducted in the urban area of Manaus in Pernambuco State, and three cities within the Recife metro- (03º06'07" S, 60º01'30" W), capital of Amazonas State, located politan region (Olinda, Jaboatão dos Guararapes, and Paulista) in the Western Amazon, Brazil (Figure 1). The city has a total (11, 12). These foci are currently being reassessed through a area of 11 401 092 km², encompassing 63 neighborhoods with Transmission Assessment Survey, in order for the Brazilian LF an estimated population of 2 182 763 inhabitants (population Elimination Program (PEFL) to certify the absence of active density of around 158.1/km²) (16). Manaus is a city with areas W. bancrofti transmission. of poverty, per capita income of 790.27 Brazilian reals, and a The cities of Belém (Pará State) and Manaus (Amazonas Municipal Human Development Index of 0.737 (16), with high State), situated in the north of Brazil, were also known to be population density. endemic, yet they are now considered nonendemic (11). Inter- ruption of transmission in Belém was confirmed in 2001. No Sampling and collection microfilaremic subjects and no infected mosquitoes were found as a result of extremely thorough study (11, 13), attesting to the A cross-sectional randomized survey was conducted from effectiveness of the measures adopted in that city. No study has September 2015 to July 2016. The study samples were com- been conducted to assess interruption of LF transmission in posed of school-age children and general population. Manaus. Results of a study conducted in Manaus in 1949 revealed School-age children. Students aged 6 to 10 years from urban LF positive findings in 2% (48/2 405) of the study popula- area municipal public elementary schools were investigated tion (autochthonous cases) (14). The last LF epidemiological as per guidance of WHO (8) and the Transmission Assessment study in the city was carried out in 1956, the findings of which Survey of the Global Programme to Eliminate Lymphatic Fila- revealed 0.2% positivity (microfilariae positive for W. bancrofti) riasis (9). WHO calls for a sample of 3 000 children to be tested among the 10 889 individuals examined (15). There is no fur- following the rapid survey methodology based on rapid immu- ther information relative to the distribution and prevalence of nochromatographic test (ICT) cards to verify LF transmission in autochthonous cases of W. bancrofti in Manaus since these two a suspected area. earlier studies. Thus, the aim of this study was to reassess the The municipal education department provided an updated occurrence of LF in Manaus to support the country’s dossier in list with the names of the students enrolled in the elementary the certification of interruption of LF transmission. schools, to allow the survey to be carried out. In order to come FIGURE 1. Map of Manaus, Amazonas State, Brazil, showing the geographic location of the 20 schools (1–20) where a sample of schoolchildren was examined for circulating Wuchereria bancrofti antigen, 2016 2 Rev Panam Salud Publica 45, 2021 | www.paho.org/journal | https://doi.org/10.26633/RPSP.2021.1
Martins et al. • Interruption of lymphatic filariasis in Manaus Original research
up with the population to be surveyed among the city’s dif- Diagnostic tool and blood collection
ferent neighborhoods, 20 (34.5%) out of 58 urban municipal
public elementary schools (comprising a total of 18 990 school- Participants were tested using rapid ICT (BinaxNOW Fila-
age children) were randomly selected. The total population of riasis, Alere Scarborough, Orlando, United States of America)
the 20 selected schools was 7 562 children. Five of these schools for the detection of W. bancrofti circulating antigens. Briefly,
were selected among those neighborhoods of Manaus where capillary blood samples were obtained from finger pricks in
microfilariae carriers had been detected in the past (14, 15). The a calibrated microhematocrit tube (100 μL) and transferred
other 15 schools were randomly chosen, representing the over- to the ICT card, according to the manufacturer’s instructions.
all urban area of the city. The results of the tests were read by a trained technician after
To reach the required total sample size of 3 000 children to 10 minutes, and positives recorded.
be tested, the sample size withdrawal was proportional to the
number of students enrolled in each school, in relation to the Ethics approval
total students from the 20 chosen schools (7 562). Schoolchil-
dren were randomly selected from the list of students provided This study was approved by the Research Ethics Commit-
by the schools. The children’s data (name, age, sex, and address) tee of the Fundação de Medicina Tropical Dr. Heitor Vieira
were obtained from the school’s administrative records. Dourado, Manaus (CAAE No. 06959813.0.0000.0005). All data
Lectures about the disease and the survey were given to obtained and herein reported were treated anonymously by the
teachers, parents/legal guardians, and students at each school. investigators.
The inclusion criterion was enrolled students aged 6 to 10 years.
Consent forms were signed by the parents or legally authorized RESULTS
representatives of each child.
A total of 3 000 ICT-based tests were performed in school-
General population. Adolescents (>10 years old) and adults children attending a sample of public elementary schools.
were randomly selected from within the same areas as the sam- Table 1 shows the stratified school-age children sample by age
pled schoolchildren. The authors included this group in order and gender. The average age was 7.9 ± 1.1 years, and the gender
to assess the status of people who were born, raised, and had distribution was 1 757 (58.6%) females and 1 243 (41.4%) males.
lived for many years in one of the former LF-endemic neigh- No test was found positive for the presence of W. bancrofti cir-
borhoods. All participants were informed about the study and culating antigens. All 709 of the adolescents and adults (ages
those ≥18 years old were asked to sign a consent form. Minors 11–85 years) tested had a negative result for circulating filarial
had the form signed by their parents or legal guardians. antigen (Table 2).
TABLE 1. Distribution, by age and sex, of school students examined for Wuchereria bancrofti antigenemia, Manaus, Amazonas
State, 2016
Male Female Total
Age ICT* results
n % n % n %
6 328 41.5 462 58.5 790 26.3 Negative
7 308 41.5 435 58.6 743 24.8 Negative
8 278 41.6 392 58.6 669 22.3 Negative
9 186 41.3 264 58.5 451 15.0 Negative
10 143 41.2 204 58.8 347 11.6 Negative
Total 1 243 41.4 1 757 58.6 3 000 100.0 Negative
* Immunochromatographic Card Test
Source: Prepared by authors from the study data.
TABLE 2. Distribution, by age group and sex, of adolescents and adults examined for Wuchereria bancrofti antigenemia, Manaus,
Amazonas State, 2016
Male Female Total
Age ICT* results
n % n % n %
11–20 47 40.9 68 59.1 115 16.2 Negative
21–30 126 51.2 120 48.8 246 34.7 Negative
31–40 108 61.4 68 38.6 176 24.8 Negative
41–50 50 64.9 27 35.1 77 10.9 Negative
≥51 56 58.9 39 41.1 95 13.4 Negative
Total 387 54.6 322 45.4 709 100.0 Negative
* Immunochromatographic Card Test
Source: Prepared by authors from the study data.
Rev Panam Salud Publica 45, 2021 | www.paho.org/journal | https://doi.org/10.26633/RPSP.2021.1 3Original research Martins et al. • Interruption of lymphatic filariasis in Manaus
DISCUSSION areas where mass drug administration is required and surveil-
lance is to be maintained (8). The test is easy to perform in field
Despite the efforts to control LF around the world, the disease settings and has a high level of sensitivity for the detection of
remains endemic in 49 countries, including Brazil (1), where filarial antigen (25).
the microfilariae of W. bancrofti were described for the first time According to WHO (8, 9), children between 6 and 10 years
by Otto Wucherer in 1866 (17). However, the earliest system- old should be the target of epidemiological surveys, because
atic epidemiological studies on the distribution of Bancroftian it is in this age group where a positive test will indicate a
filariasis in Brazil were conducted decades later (11, 18). In a recent infection. The sample of 3 000 children as defined by
study conducted between 1951 and 1958, a total of 811 361 indi- WHO (8) is not useful to measure LF prevalence, but it is a
viduals were examined (using thick blood film), and 120 399 fast way to determine whether transmission is still occurring
specimens of mosquito vectors were dissected (18). The simul- in the area. The rationale for examining young children is
taneous discovery of microfilaremic individuals and infected therefore to assess recent infections. Negative findings pro-
mosquitoes provided evidence of local LF transmission in vide a good indicator that transmission has ceased in the
11 cities of the country, including Manaus (Amazonas State) area (26). According to WHO, antigenemia levels of >0.1%
(18). In fact, a previous study in Manaus in 1949 had already indicate ongoing transmission. In this situation, a population
demonstrated a prevalence of 2.0% (48/2 405) of W. bancrofti survey to determine LF prevalence and morbidity would be
microfilariae carriers in the neighborhoods of São Raimundo, required.
Santo Antônio, Vila da Prata, Cachoeirinha, São Francisco, A sample of adolescents and adults was used in this study
and Presidente Vargas (14). In 1956, Rachou and Lacerda (15) to assess the status of LF in people born, raised, and living for
examined 10 889 persons in Manaus and identified that 0.2% many years in a former LF-endemic area. This was important,
were microfilariae-positive. Since then, beyond the selective as no LF survey had been carried out in the city since the 1950s.
treatment of infected patients, no specific measures focusing The Brazilian LF Program needs to look at all historical LF foci
on the prevention of filarial infections were implemented, and in order to prepare a dossier for submission to WHO to obtain
no epidemiological surveys to investigate LF had been carried the validation of elimination of LF as a public health problem
out. The Ministry of Health no longer considered Manaus to be in Brazil.
LF endemic (19). This is the first study that relied on the WHO criteria to eval-
The present study revealed that LF had indeed been suc- uate the current LF situation in Manaus. The results presented
cessfully eliminated in Manaus, despite the persistence of risk here are quite promising, indicating that the historical LF focus
factors. The examined individuals live in areas where the envi- in Manaus has indeed been eliminated. The Ministry of Health
ronmental conditions and the lack of urban infrastructure and of Brazil considers that LF transmission has been interrupted
sanitation favor vector proliferation and W. bancrofti transmis- in almost all the foci in the country, including Belém, Maceió
sion. Furthermore, some of the surveyed schools are located in (27, 28), Salvador, Castro Alves, Florianópolis, Ponta Grossa,
the very same neighborhoods where LF had been found to be and Barra de Laguna (11). It has since 2011 been working
endemic. These factors could very well facilitate LF reintroduc- intensively to eliminate the remaining active foci in the Recife
tion, should Manaus eventually receive infected people coming metropolitan region (28).
from LF-endemic areas. Certification of LF elimination as per the WHO standardized
Reintroduction of the infection through migration was procedures and those of the Strategic and Technical Advisory
described in Sri Lanka (20) and in the metropolitan areas of Group for Neglected Tropical Diseases will require careful
Recife in Brazil, where LF had already been eliminated (21). preparation of the dossier (29, 30). This study constitutes an
Surveillance measures must therefore be sustained, focusing important element of the dossier.
specially on immigrants from LF-endemic areas and coun-
tries. A study conducted by Silva et al. in 2014 (22) on a Author contributions. GF and MM conceived the original
population of Haitian refugees in Manaus showed very low idea, planned the experiments, analyzed the data, interpreted
prevalence rates of LF. Only one immigrant among the 244 the results and wrote the manuscript. MM and RCSG collected
evaluated (0.4%) was found to be positive. The possibility and analyzed the data. All authors reviewed and approved the
of reintroduction of LF should not be ruled out, as there is final version.
a large density of the main vector C. quinquefasciatus in the
region, as well as adequate conditions for the transmission of Acknowledgment. To the Pan American Health Organization
the parasite (23). and the Ministry of Health of Brazil for the donation of the ICT
Three other cities (Humaitá, Guajará-Mirim, and Porto cards (BinaxNOW Filariasis®); to Secretária Municipal de Edu-
Velho) in the Western Brazilian Amazon region were studied cação (SEMED) Manaus; and Fundação de Medicina Tropical
by Korte et al. in 2013. There was a history of allochthonous Dr. Heitor Vieira Dourado, Manaus. The authors are grateful to
cases of W. bancrofti infections dating back to the 1950s in all Dra. Eliana M.M. Rocha (Universidade Federal de São João del-
three cities (24). No humans or mosquitoes were found to be Rei) for the critical reading and review of the manuscript, and
infected with the parasite in the 2013 study, indicating that the to Marco Antonio Saboia Moura for the map.
area was no longer positive for LF transmission (24). It appears
that the small number of people infected and the mild nature Conflicts of interest. The authors declare no conflicts of interest.
of the microfilarial infection reported in the past were not suffi-
cient to sustain transmission (24). Disclaimer. Authors hold sole responsibility for the views
ICT card tests are recommended by WHO as the diagnostic expressed in the manuscript, which may not necessarily reflect
tool of choice to be used in LF elimination programs to define the opinion or policy of the RPSP/PAJPH and/or PAHO.
4 Rev Panam Salud Publica 45, 2021 | www.paho.org/journal | https://doi.org/10.26633/RPSP.2021.1Martins et al. • Interruption of lymphatic filariasis in Manaus Original research
REFERENCES
1. World Health Organization [Internet]. Geneva: WHO; 2020 18. Rachou RG. Conceito e programa de profilaxia da filariose
March 2 [cited 2020 May 21]. Lymphatic filariasis, Key facts. bancroftiana no Brasil. Rev Bras Malariol Doenças Trop. 1960;12:
Available from: https://www.who.int/news-room/fact-sheets/ 11–40.
detail/lymphatic-filariasis 19. Ministério da Saúde. Controle das Endemias no Brasil (de 1979 a
2. World Health Organization. Global programme to eliminate 1984). Superintendência de Campanhas de Saúde Pública. Brasília:
lymphatic filariasis: progress report, 2018. Wkly Epidemiol Rec. SUCAM; 1985, 154 p.
2019;94(41):457–72. Available from: https://apps.who.int/iris/bit 20. Ramaiah KD, Das PK, Appavoo NC, Ramu K, Augustin DJ, Vijay
stream/handle/10665/329087/WER9441-eng-fre.pdf Kumar KN, et al. A programme to eliminate lymphatic filariasis in
3. World Health Organization [Internet]. Geneva: WHO; 2019 Tamil Nadu State, India: compliance with annual single-dose DEC
August 15 [cited 2019 December 25]. Neglected tropical diseases. mass treatment and some related operational aspects. Trop Med Int
Despite challenges, Yemen eliminates lymphatic filariasis. Avail Health. 2000;5(12):842–7.
able from: https://www.who.int/neglected_diseases/news/yemen 21. Medeiros Z, Alves A, Brito JA, Borba L, Santos Z, Costa JP, et al. The
-eliminates-lymphatic-filariasis/en/. present situation regarding lymphatic filariasis in Cabo de Santo
4. Orihel TC. Filariae. In: Beaver PC, Jung RC (editors). Animal agents Agostinho, Pernambuco, Northeast Brazil. Rev Inst Med Trop São
and vectors of human disease. 5th ed. Philadelphia: Lea & Febiger, Paulo. 2006;48(5):263–7.
1985;171–91. 22. Silva EF, Lacerda MVG, Fontes G, Mourão MPG, Martins M.
5. World Health Organization. Lymphatic filariasis: a handbook of Wuchereria bancrofti infection in Haitian immigrants and the risk
practical entomology for national lymphatic filariasis elimination of re-emergence of lymphatic filariasis in the Brazilian Amazon.
programmes. Geneva: WHO; 2013. Available from: https://www Rev Soc Bras Med Trop. 2017;50(2):256–9. https://dx.doi.org
.who.int/lymphatic_filariasis/resources/9789241505642/en/. /10.1590/0037-8682-0407-2016
6. Fontes G, Rocha EMM, Brito AC, Fireman FA, Antunes CM. The 23. Barbosa MGV, Fé NF, Marcião AHR, Silva APT, Monteiro WM,
microfilarial periodicity of Wuchereria bancrofti in northeastern Bra- Guerra MVF, et al. Record of epidemiologically important
zil. Ann Trop Med Parasitol. 2000;94:373–9. https://doi.org/10.1080 Culicidae in the rural area of Manaus, Amazonas. Rev Soc Bras Med
/00034983.2000.11813552 Trop. 2008;41(6):658–63. https://doi.org/10.1590/S0037-8682200800
7. World Health Organization. Fiftieth World Health Assembly, 0600019
Geneva 5–14 May 1997. Resolutions and decisions, annexes. 24. Korte RL, Fontes G, Camargo J de S, Rocha EMM, Araújo EA,
Geneva: WHO; 1997 (Document WHA50/1997/REC/1). Oliveira MZ, et al. Survey of Bancroftian filariasis infection in
8. World Health Organization. Preparing and implementing a national humans and Culex mosquitoes in the western Brazilian Amazon
plan to eliminate lymphatic filariasis: a guideline for programme region: implications for transmission and control. Rev Soc Bras Med
managers. Geneva: WHO; 2000. Available from: https://www.who Trop. 2013;46(2):214–20.
.int/lymphatic_filariasis/resources/who_cds_cpe_cee_2000.15/en/. 25. Njenga SM, Wamae CN. Evaluation of ICT filariasis card test using
9. World Health Organization. Monitoring and epidemiological whole capillary blood: comparison with Knott's concentration
assessment of mass drug administration in the global programme and counting chamber methods. J Parasitol. 2001;87(5):1140–3.
to eliminate lymphatic filariasis: a manual for national elimination https://doi.org/10.1645/0022-3395(2001)087[1140:eoifct]2.0
programmes. Geneva: WHO; 2011. Available from: https://apps. .co;2
who.int/iris/handle/10665/44580 26. World Health Organization; Global Programme to Eliminate Lym-
10. World Health Organization. Global programme to eliminate lym- phatic Filariasis. Monitoring and epidemiological assessment of the
phatic filariasis: progress report on mass drug administration, 2010. programme to eliminate lymphatic filariasis at implementation unit
Wkly Epidemiol Rec. 2011;86(35):377–88. Available from: https:// level. Geneva: WHO; 2005. Available from: https://apps.who.int/iris
www.who.int/wer/2011/wer8635.pdf /handle/10665/69172
11. Fontes G, Leite AB, de Lima ARV, Freitas H, Ehrenberg JP, Rocha 27. Fontes G. Consolidação dos inquéritos e estudos sobre a Filariose
EMM. Lymphatic filariasis in Brazil: epidemiological situation and linfática realizados nos estados de Alagoas e Pará, visando à elim-
outlook for elimination. Parasit Vectors. 2012;5:272. https://doi inação da enfermidade no Brasil. Documento Técnico. Brasília: MS
.org/10.1186/1756-3305-5-272 /OPAS; 2015. 75p.
12. Xavier A, Oliveira H, Aguiar-Santos A, Barbosa Junior W, da Silva 28. Ministério da Saúde do Brasil, Secretaria de Vigilância em Saúde.
E, Braga C, et al. Assessment of transmission in areas of uncer- Departamento de Vigilância das Doenças Transmissíveis. Situação
tain endemicity for lymphatic filariasis in Brazil. PLOS Negl epidemiológica da filariose linfática no Brasil. Boletim Epidemi-
Trop Dis. 2019;13(11):e0007836. https://doi.org/10.1371/journal. ológico. 2016;47(9):1–5.
pntd.0007836 29. World Health Organization. Report of the WHO Strategic and Tech-
13. Fontes G, Braun RF, Neto HF, Vieira JBF, Padilha SS, Rocha RC, et al. nical Advisory Group for Neglected Tropical Diseases. Geneva:
Filariose linfática em Belém, Estado do Pará, Norte do Brasil e a per- WHO; 2016. Available from: https://www.who.int/neglected_dis
spectiva de eliminação. Rev Soc Bras Med Trop. 2005;38(2):131–6. eases/NTD_STAG_report_2016.pdf
14. Deane MP. Sôbre a incidência de filárias humanas em Manaus, 30. World Health Organization. Validation of elimination of lymphatic
Estado do Amazonas. Rev Serv Espec Saude Publica. 1949;2:849–58. filariasis as a public health problem. Geneva: WHO; 2017. Available
15. Rachou RG, Lacerda NB. Transmissão da filariose brancrofti- from: https://apps.who.int/iris/bitstream/handle/10665/254377
ana em Manaus (Amazonas). Rev Bras Malariol Doenças Trop. /9789241511957-eng.pdf
1956;8(2):369–71. PMID: 13494855.
16. Instituto Brasileiro de Geografia e Estatística [Internet]. Rio de
Janeiro: IBGE; c2017 [cited 2019 December 9]. Brasil, Amazonas,
Manaus [Data]. Available from: https://cidades.ibge.gov.br/brasil/
am/manaus/panorama
17. Gurgel CBFM, Carneiro F, Coutinho E. A contribuição brasileira
para a descoberta do agente etiológico da filariose linfática. Rev Manuscript received on 27 January 2020. Revised version accepted for publication
Patol Trop. 2010;39(4):251–9. on 10 July 2020.
Rev Panam Salud Publica 45, 2021 | www.paho.org/journal | https://doi.org/10.26633/RPSP.2021.1 5Original research Martins et al. • Interruption of lymphatic filariasis in Manaus
Interrupción de la transmisión de la filariasis linfática en Manaos,
anteriormente un foco de Wuchereria bancrofti en la Amazonia occidental de
Brasil
RESUMEN Objetivo. Confirmar la ausencia de casos autóctonos de Wuchereria bancrofti en Manaos, anteriormente un
foco de filariasis linfática en la Amazonia occidental de Brasil.
Métodos. En el 2016 se llevó a cabo una encuesta en el terreno con pruebas rápidas inmunocromatográfi-
cas (tiras inmunocromatográficas) para detectar antígenos filáricos circulantes en sangre. La muestra constó
de un grupo de 3 000 escolares de 6 a 10 años matriculados en escuelas de diferentes zonas urbanas de
Manaos (incluida la zona que anteriormente era el foco de filariasis linfática en la ciudad) y de un grupo de
709 adolescentes y adultos, de edades comprendidas entre 11 y 85 años, nacidos y criados en diferentes
áreas de Manaos.
Resultados. Todas las personas dieron negativo en la prueba de antígeno de Wuchereria bancrofti.
Conclusiones. Aunque hubo un tiempo en que Manaos se consideraba zona endémica, parece que este
foco de transmisión de la filariasis linfática ya no está activo. Los resultados de este estudio podrían brindar
apoyo a la certificación de la Organización Mundial de la Salud respecto de los esfuerzos realizados en Brasil
para eliminar la transmisión de la filariasis linfática.
Palabras clave Wuchereria bancrofti; filariasis linfática; Brasil.
Interrupção da transmissão da filariose linfática em Manaus, anteriormente
um foco de Wuchereria bancrofti na parte leste da Amazônia brasileira
RESUMO Objetivo. Confirmar a ausência de casos autóctones de Wuchereria bancrofti em Manaus, anteriormente um
foco da filariose linfática na parte leste da Amazônia brasileira.
Métodos. Uma pesquisa de campo foi realizada em 2016 com o uso de teste rápido por imunocromatografia
(cartão ICT) para detecção de antígenos de microfilárias circulantes no sangue. A amostra estudada consistiu
de um grupo de 3 000 crianças escolares entre 6 e 10 anos de idade matriculados em escolas de diferentes
áreas da zona urbana de Manaus (englobando a área anteriormente com o foco de filariose linfática) e um
grupo de 709 adolescentes e adultos entre 11 e 85 anos de idade nascidos e crescidos em diferentes áreas
de Manaus.
Resultados. Todos os indivíduos pesquisados tiveram teste negativo para o antígeno da W. bancrofti.
Conclusões. Apesar de Manaus ter sido anteriormente uma área endêmica, parece que não existe mais foco
ativo de transmissão da filariose linfática na cidade. Os resultados deste estudo podem servir para embasar a
certificação pela Organização Mundial da Saúde da eliminação da transmissão da filariose linfática no Brasil.
Palavras-chave Wuchereria bancrofti; filariose linfática; Brasil.
6 Rev Panam Salud Publica 45, 2021 | www.paho.org/journal | https://doi.org/10.26633/RPSP.2021.1You can also read