Forgotten but Not Gone: Learning From the Hepatitis A Outbreak and Public Health Response in San Diego - IAS-USA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Hepatitis A in San Diego Volume 26 Issue 4 January 2019
Perspective
Forgotten but Not Gone: Learning From the Hepatitis A
Outbreak and Public Health Response in San Diego
ABSTRACT: The recent hepatitis A virus (HAV) outbreak in San Diego was previously found, and an increase in
driven by homelessness, associated sanitation conditions, and illicit drug use. international normalized ratio (INR).
As with an outbreak in Michigan, fueled by similar factors, morbidity and Additional laboratory work showed
mortality were higher than what has been observed with post-vaccine era that the patient had a high HAV RNA
foodborne HAV outbreaks. Control of the outbreak in San Diego was accom- level during this relapsing phase of the
plished with vaccine, sanitation, and education initiatives that targeted illness. HAV IgG remained negative. Of
those at highest risk. Mass vaccination events and mobile foot teams and note, the patient had been found to be
vans brought education and vaccine to high-risk individuals in affected areas. IgG negative a year earlier, and despite
The homelessness crisis in San Diego and in many locales throughout the documentation of lack of immunity to
United States poses risk of increasing numbers of outbreaks of HAV and other HAV, had not received HAV vaccination.
infectious illnesses. This article summarizes an IAS-USA continuing education Liver ultrasound showed hepatomeg-
webinar given by Darcy A. Wooten, MD, on July 19, 2018. aly with diffuse fatty liver and possible
nodularity, trace ascites, normal spleen,
Keywords: hepatitis A, hepatitis A virus, San Diego, epidemic, vaccination, normal common bile duct, and nor-
homeless, public health efforts mal portal vein. Liver biopsy showed
severely active hepatitis, a fibrosis
Consider the case of a patient during total bilirubin of 3.1 mg/dL, AST above stage of 1 out of 6, portal inflam-
the recent outbreak of hepatitis A virus 1,000 U/L, ALT of 792 U/L, and alkaline mation primarily with lymphocytes
(HAV) infections in San Diego County. phosphatase of 276 U/L. Since the HAV and macrophages, bile duct injury, no
He was a 63-year-old man with a his- outbreak was at its peak, house officers steatosis, and spotty necrosis. The
tory of hepatitis C virus (HCV) infection ordered a HAV IgM test, which came patient became increasingly encepha-
and alcoholic liver disease who pre- back positive, confirming a diagnosis lopathic and developed progressive
sented with a left hip fracture suffered of acute HAV infection. The patient was liver failure; he became comatose, was
during a fall while intoxicated. He sub- placed into contact isolation. transitioned to comfort care, and died
sequently underwent surgical repair of Further past medical history revealed approximately a month and a half after
the fracture. Labs drawn on admission that the patient had been diagnosed admission to the hospital.
showed a total bilirubin of 0.32 mg/ with HCV infection in 2011, with risk This patient’s case highlights 3 im-
dL, aspartate aminotransferase (AST) factors that included prior cocaine use portant points. First, he died from a
of 178 U/L, alanine aminotransferase and a history of blood transfusions. completely preventable condition and
(ALT) of 69 U/L, and alkaline phospha- He suffered from severe alcoholism, his story speaks to the need for im-
tase of 90 U/L; results were similar to having 20 to 40 drinks per week for proved public health measures such as
those a month earlier when the patient most of his life. He had numerous vaccination among our most vuluner-
presented to the emergency depart- prior ED visits for falls, fractures, and able populations. Second, he had a rare
ment (ED) for an unrelated issue. intoxication. No formal staging of his complication of acute HAV infection
His hospital stay was prolonged liver disease had been performed, but in the form of a relapsing course. And
because he was homeless. One week he had no known history of cirrhosis finally, he had many of the risk factors
after surgery, he developed fever and or symptoms consistent with decom- for both acquiring HAV and having a
diarrhea and was started on vanco- pensated liver disease. He had a 40- poor outcome from the infection that
mycin and piperacillin/tazobactam for year history of tobacco use, 1 pack per were consistently observed during the
possible hospital-acquired pneumo- day. He had been homeless for 5 years, outbreak in San Diego.
nia, despite the absence of respiratory living primarily in shelters and eating
symptoms and a clear chest x-ray. The in soup kitchens; however, he had no Characteristics of HAV Infection
patient also lacked signs or symptoms known recent sick contacts and re-
of alcohol withdrawal to explain the ported no recent history of eating raw HAV transmission occurs primarily per-
fever. The fever persisted for a week. or undercooked foods. son-to-person by the fecal-oral route.
Cultures were negative, but repeat A week after diagnosis of HAV infec- Stool is infectious 2 to 3 weeks before
liver function tests (LFTs) showed a tion, the patient’s LFTs trended back and 1 week after the onset of symp-
toward normal. However, 2 weeks toms. The peak of infectivity precedes
Dr Wooten is an Assistant Clinical Professor later, daily fevers returned, along with the onset of symptoms. Routes of
at the University of California San Diego in increased abdominal pain, nausea, transmission include food (eg, cooking
San Diego, California. increases in LFTs to higher levels than temperature is not high enough, food is
117IAS–USA Topics in Antiviral Medicine
40,000 typically resolves spontaneously and is
Reported Number of Cases
35,000 treated with supportive care. Cholestyr-
30,000 amine can be given for pruritus.
Acute liver failure is a rare but dev-
25,000
astating complication characterized by
20,000
elevated LFTs (especially bilirubin), co-
15,000 agulopathy, and hepatic encephalopa-
10,000 thy in a patient with previously stable
5,000 liver function. It is estimated that less
0 than 0.1% of HAV cases result in acute
8 0 82 84 86 88 90 92 94 96 98 00 002 004 006 008 010 012 liver failure. Risk factors include older
19 19 19 19 19 19 19 19 19 19 20 2 2 2 2 2 2
age (>50 years), coinfection with hep-
atitis B virus (HBV) or HCV, and under-
Figure 1. Incidence of hepatitis A virus infections in the United States, 1980-2012. Adapted lying liver disease.
from Boston University School of Public Health.1
Treatment and Prevention
prepared by someone who is shedding infection. After the incubation period,
virus), blood transfusion, illicit drug use, viremia occurs followed by shedding Treatment for HAV infection is support-
and sex via oral-anal or digital-anal con- of virus in the feces. With the devel- ive care, including hydration, nutrition,
tact. Humans are the primary natural opment of symptoms, increases in and avoidance of hepatotoxins. The
host with genotypes 1, 2, and 3 caus- transaminases are observed. Next, the vast majority of affected individuals
ing the majority of infections. Although host immune response begins, with completely recover by 6 months fol-
not tested routinely in clinical practice, increases in IgM and a subsequent lowing initial infection, usually much
genotype 1 is the most common in the switch to IgG antibody. Anti-HAV IgG sooner.
United States. Genotypes 1b and 3a antibody is thought to provide lifelong Vaccination is a highly effective
have been associated with fulminant protection against future infection. mode of prevention, with 2 inactivated
hepatitis during prior outbreaks in the Uncommon complications associated whole-virus vaccines given in 2 doses
United States and Korea, respectively. with HAV infection include relapsing 6 months apart. A combined HAV and
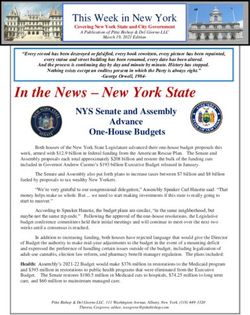
Figure 1 shows the incidence of HAV hepatitis, as was experienced by the HBV vaccine is also available. Approx-
infection in the United States reported patient described, cholestatic hepatitis, imately 95% of adults exhibit serocon-
by the Centers of Disease Control and autoimmune hepatitis, and acute liver version to IgG antibody after the first
Prevention (CDC) between 1980 and failure. Relapsing hepatitis occurs in dose of the 2-dose vaccine, with approx-
2012. The decline starting in 1996 approximately 10% of patients (range, imately 100% seroconverting after the
marks the development and imple- 3%-20%) however the underlying eti- second dose. Seroconversion rates are
mentation of an effective anti-HAV ology and associated risk factors are lower in patients with underlying liver
vaccine. Universal vaccination of chil- unclear. The clinical course is that of disease and in those with advanced im-
dren began in 2006. According to CDC improvement in symptoms after initial munosuppression. For example, among
data, approximate numbers of cases presentation, followed by an increase people with HIV infection, seroconver-
and death rates in recent years have in LFTs (with or without symptoms). sion rates are reported to range from
been fairly stable: 2700 and 2.5% in Relapse is typically milder than the 50% to 90%. Risk factors associated
2011, 3000 and 2.2% in 2012, 3500 initial presentation. HAV RNA
and 2.3% in 2013, and 2500 and 3.0% levels are markedly elevated, ALT
in 2014. similar to levels during initial Total anti-HAV
IgM anti-HAV
The asymptomatic incubation period infection. Relapse occurs 1 to
Concentration
of HAV infection is approximately 1 12 weeks after the initial pre-
month (range, 15-50 days). Symptoms sentation and can persist for 3
include fever, fatigue, nausea, anorexia, weeks to 12 months, with no
abdominal pain, jaundice (in up to well-defined sequelae.
70% of cases), vomiting, diarrhea, dark Cholestatic hepatitis occurs
urine, and light-colored stools. Dura- in approximately 5% of pa-
tion of symptoms is generally less than tients and is marked by pro- 0 1 2 3 4 5 6 12
2 months, with 10% to 15% of cases longed (>3 months) elevation Months After Exposure
having a prolonged or relapsing course. of bilirubin and alkaline phos-
Approximately 20% to 40% of patients phatase levels. The clinical Figure 2. Course of clinical, virologic, and sero-
require hospitalization. Figure 2 shows course is marked by prolong- logic events in hepatitis A virus (HAV) infection. ALT
the clinical, virologic, and serologic ed jaundice, pruritus, fever, indicates alanine aminotransferase. Adapted from
events that occur during the course of weight loss, and diarrhea. It Bennett, Dolin, and Blaser.2
118Hepatitis A in San Diego Volume 26 Issue 4 January 2019
A
Vaccine Routine vaccination for Routine vaccination for
700 children in high-incidence all US children
states (including California)
600
Number of Cases
500
400
300
200
100
0
94 95 96 97 98 99 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18
19 19 19 19 19 19 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20
Year
B
30
Number of Confirmed
or Probable Cases
20
10
0
10-30-2016
11-06-2016
11-13-2016
11-20-2016
11-27-2016
12-04-2016
12-11-2016
12-18-2016
12-25-2016
01-01-2017
01-08-2017
01-15-2017
01-22-2017
01-29-2017
02-05-2017
02-12-2017
02-19-2017
02-26-2017
03-05-2017
03-12-2017
03-19-2017
03-26-2017
04-02-2017
04-09-2017
04-16-2017
04-23-2017
04-30-2017
05-07-2017
05-11-2017
05-21-2017
05-28-2017
06-04-2017
06-11-2017
06-18-2017
06-25-2017
07-02-2017
07-09-2017
07-16-2017
07-23-2017
07-30-2017
08-06-2017
08-13-2017
08-20-2017
08-27-2017
09-03-2017
09-10-2017
09-17-2017
09-24-2017
10-01-2017
10-08-2017
10-15-2017
10-22-2017
10-29-2017
11-05-2017
11-12-2017
11-19-2017
11-26-2017
12-03-2017
12-10-2017
12-17-2017
12-24-2017
12-31-2017
01-07-2018
01-14-2018
01-21-2018
01-28-2018
02-04-2018
02-11-2018
02-18-2018
02-25-2018
03-04-2018
03-11-2018
03-18-2018
03-25-2018
04-01-2018
04-08-2018
04-15-2018
04-22-2018
04-29-2018
05-06-2018
05-13-2018
05-20-2018
05-27-2018
06-03-2018
06-10-2018
06-17-2018
Weeks of Onset
Figure 3. A: Hepatitis A virus infection cases in San Diego, California, 1994 to 2018. B: Number of cases per week in 2017 outbreak. Courtesy
of the County of San Diego, Health and Human Services Agency, Public Health Services, Epidemiology & Immunization Services.
with lack of seroconversion include low transmitting HAV during outbreaks— reflecting the lower prevalence of HAV
CD4+ cell count, high HIV RNA level, eg, healthcare workers, food service in plasma donors in recent years.
HCV coinfection, and tobacco use. For workers, and people who work with
immunocompetent hosts, modeling children, such as in daycare settings.
San Diego Outbreak
studies indicate that greater than 90% Pre-vaccination serologic testing is
of persons maintain protective anti- not recommended in persons with Figure 3A shows the number of cases
bodies 40 years after vaccination. Dura- an indication for vaccination. Post- of HAV infection in San Diego between
bility of immunity in immunocompro- vaccination testing for response is not 1994 and 2018, highlighting the 2017
mised host thought to be lower but is indicated in immunocompetent hosts; outbreak; Figure 3B shows the onset of
less well characterized. its role in imunocompromised persons outbreak cases by week. There were
The current indications for vaccina- is unclear. 590 confirmed outbreak cases between
tion include all children at 1 year of age, Postexposure prophylaxis, consis- November 22, 2016, and June 21, 2018,
travel to endemic countries, chronic ting of the HAV vaccine series and im- all involving HAV genotype 1b. Among
liver disease (eg, HBV or HCV infection, mune globulin in most cases, should the cases, 402 (68%) were boys or men,
cirrhosis), clotting factor disorders, men be given to non-immune individuals as with 14 being MSM. Among all patients,
who have sex with men (MSM), illicit soon as possible and within 2 weeks 405 (69%) were hospitalized and 20
substance users, and persons work- after exposure to a confirmed case of (3.4%) died. This mortality rate was sub-
ing with non-human primates. Other HAV infection. The recommended dose stantially higher than in prior years as
groups, often considered for vaccina-˜ of immune globulin is now 5 times outlined above. The median age of the
tion indications, but in whom vaccina- higher than that previously recom- cases was 43 years (most age 40 to 60
tion currently is not required outside mended, because more recent prepa- years; range, 5-87 years). Risk factors
of the setting of outbreaks, include rations were found to have lower con- for infection included homelessness
those at higher risk of acquiring and centrations of HAV antibodies, likely and illicit drug use in 194 cases (34%),
119IAS–USA Topics in Antiviral Medicine
140
40,000 Centers), implemented outreach to
35,000 those at highest risk (eg, homeless
120
Vaccinations
Probable Cases
30,000
Confirmed or
100 persons and others who lacked health
25,000
80 20,000
insurance or regular contact with the
60 15,000 health system), and implemented a
40 10,000 program for vaccination in EDs. The
20 5,000 routine indications for vaccination
0 0 were expanded to include: all food
16 16 17 17 17 17 17 17 17 17 17 17 17 17 18 18 18 18 18
v 20 c 20 n 20 b 20 r 20 r 20 y 20 n 20 l 20 g 20 p 20 t 20 v 20 c 20 n 20 b 20 r 20 r 20 y 20 service workers; healthcare work-
a p a u c o e Ja Fe Ma Ap a
No De Ja Fe M A M Ju J Au Se O N D M ers, sanitation workers, and public
Pre-response Vaccinations Response Vaccinations safety workers who work with at-risk
populations; homeless service provid-
Figure 4. Effect of vaccination campaign in controlling San Diego hepatitis A virus outbreak. ers and volunteers; and any person
Courtesy of the County of San Diego, Health and Human Services Agency, Public Health Ser- who desired immunity.
vices, Epidemiology & Immunization Services. The public health strategy was
devoted to the effort of going to the
homelessness alone in 91 (15%), and including male predominance, high streets to meet vulnerable persons
illicit drug use alone in 77 (13%), with morbidity and mortality, association and individuals at higher risk to pro-
167 (28%) being associated with neither with illicit substance use and homeless- vide education about the outbreak and
of these risk factors. The risk factors in ness, and cases with HCV coinfection. to offer and provide vaccination. As
56 (10%) were unknown. Geograph- Thus far, there have been 850 cases, noted, the initiatives included holding
ically, the outbreak was centered in with a median age of 40 years and 65% staffed vaccination events at homeless
areas with high rates of homelessness. being male individuals. Hospitalization shelters. Mobile vans traveled from
Approximately 17% of patients had has been required in 80% of cases and place to place, focusing on downtown
HCV coinfection and approximately 3.2% have died. More than 50% of San Diego and El Cajon, where most of
5% had HBV coinfection. In prior years, cases were associated with illicit sub- the cases were occurring, with person-
most cases of HAV infection in San stance use and 13% with homeless- nel providing education and vaccina-
Diego were associated with interna- ness; 27% of cases had coinfection tions to people who were willing to
tional travel. with HCV. Understanding the changing receive them. Mobile foot teams would
The outbreak spread beyond San epimediology of hepatitis A transmis- go from tent to tent and person to per-
Diego, with cases genetically and epi- sion and outbreaks will be important son on the street in areas with high
demiologically linked to the San Diego with regard to prevention efforts going concentrations of homeless individu-
strain including 76 in Santa Cruz, 12 in forward. als, again providing education about
Los Angeles, 12 in Monterey, and 17 in the outbreak and offering and provid-
other areas in California. Linked cases ing vaccination. Figure 4 shows the
San Diego Public Health
were also identified in Arizona, Colo- outcome of these efforts, with the num-
Response
rado, Kentucky, Indiana, Rhode Island, ber of new infections dropping once
West Virginia, and Utah. In response to identification of the HAV the vaccination effort reached its peak.
The outbreak in San Diego and an outbreak, a local health emergency was The sanitation campaign included
ongoing outbreak in Michigan under- declared on September 1, 2017. This the establishment of handwashing sta-
score a change in the nature of HAV was followed by a declaration of a state tions (not employing alcohol-based
outbreaks from mostly food-borne to of emergency by the governor of Cali- sanitizers, which are not effective),
centered on homelessness, sanitation, fornia on October 13, 2017. A public portable toilets and increased access
and illicit drug use. For example, one of health strategy of vaccination, sanita- to public restrooms, and hygiene kits,
the largest post-vaccine era outbreaks tion, and education was instituted by particularly in the downtown areas.
occurred in 2003 in association with the local health department. Food inspections were also conducted,
green onions at a restaurant chain in The vaccination effort included particularly during the early part of
Pennsylvania and Ohio; a total of 660 administration of more than 160,000 the outbreak when food-borne trans-
cases were identified, with 3 deaths. vaccinations, with 85% administered mission was more highly suspected.
A more-recent food-borne outbreak in to high-risk individuals. More than As part of the sanitation campaign,
2016 in Hawaii, associated with raw 30,000 vaccinations were given in the the city employed power spraying of
scallops from a sushi restaurant, in- field through mass vaccination events, sidewalks to remove fecal matter that
volved 292 cases, 74 hospitalizations, mobile foot teams, and mobile vans. accumulated in the setting of home-
and no deaths. The public health department part- lessness and inadequate access to bath-
In contrast, the southeast Michigan nered with local health systems (eg, room facilities. The city also built 3
outbreak, ongoing since 2016, shares University of California San Diego, large industrial tents that could house
features with the San Diego outbreak, Scripps, Sharp, Kaiser, Family Health 700 people as a temporary housing
120Hepatitis A in San Diego Volume 26 Issue 4 January 2019
option for people living on the street, Homelessness and its association need to address the problem of home-
an initiative that cost $6.5 million. with poor sanitation constituted a root lessness and other social determinants
The tents were staffed with 24-hour cause of the outbreak. Homelessness of health.
security, contained bathrooms and was also associated with many chal- Presented by Darcy A. Wooten, MD, in July
showers, and were staffed by person- lenges in trying to stop the outbreak 2018. First draft prepared from transcripts
nel to provide services during the day that differ markedly from those en- by Matthew Stenger. Reviewed and edited by
that included mental health and sub- countered in food-borne outbreaks. Al- Dr Wooten in November 2018..
stance abuse services, job training and though measures to address homeless-
case management, and bridging to per- ness were employed in combating Financial affiliations in the past 12 months:
Dr Wooten has no relevant financial affilia-
manent housing. the outbreak (eg, the temporary hous-
tions to disclose.
As part of the education campaign, ing with industrial tents), it is clear
the department of public health pro- that much more needs to be done in
vided community presentations and addressing the homelessness crisis in References
community outreach and staffed a 24- San Diego and in many areas through-
1. Boston University School of Public
hour hotline to dispense information out the United States. Homelessness Health. Background on Hepatitis A. http://
about vaccination events. Broad media and associated poor sanitation threaten sphweb.bumc.bu.edu/otlt/MPH-Modules/
PH/Sparta/Sparta3.html. Accessed on No-
coverage of the outbreak was provided to make outbreaks of HAV and other vember 26, 2018.
to augment public awareness. Local infectious illnesses more common in 2. Bennett JE, Dolin R, Blaser MJ. Mandell,
and state political will to battle the out- the future. Attention to this threat and Douglas, and Bennett's Principles and
Practice of Infectious Diseases. 8th ed.
break was mobilized and played a large the political will to address the crisis Amsterdam, Netherlands: Saunders (El-
part in securing the resources needed need to be heightened if we are to sevier), 2015.
for the public health efforts to succeed. make any substantial progress in pre-
venting such outbreaks. Additional Suggested Reading
In summary, the San Diego HAV out- Matheny SC, Kingery JE. Hepatitis A. Am
Summary Fam Physician. 2012;86(11):1027-1034.
break is one of the largest outbreaks
The vaccination, education, and sani- reported in the United States to date. Kushel M. Hepatitis A Outbreak in California
tation campaigns in the San Diego It was associated with a high degree of - Addressing the Root Cause. N Engl J Med.
2018;378(3):211-213.
outbreak were very robust. The strat- morbidity and mortality. Homelessness
egies employed were innovative and and substance use were important risk
highly individualized in an attempt to factors identified early on and guided Top Antivir Med. 2019;26(4):117-121.
ensure vaccination of those at highest the public health response. Vaccination ©2019, IAS–USA. All rights reserved
risk. The question remains, however: is was the most important strategy to
this enough? stop the outbreak. There is a continuing
121You can also read