Joga Gobburu Division of Pharmacometrics - OCP/OTS/CDER/FDA Need Slides?
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Joga Gobburu
Division of Pharmacometrics Need Slides?
OCP/OTS/CDER/FDA Joga.gobburu@gmail.com
Gobburu 1
R&D Challenge
R&D
Learn & Apply, Cases
L&A Future
Future
Obsessive focus on ‘Confirm’ goal contributed to R&D inefficiency.
R&D goals ought to be about learning, applying.
R&D Challenge
R&D
Learn & Apply, Cases
L&A Future
Future
Obsessive focus on ‘Confirm’ goal contributed to R&D inefficiency.
R&D goals ought to be about learning, applying.

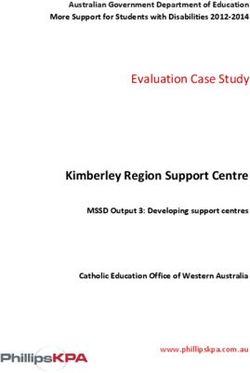
Potential Root Causes
Direct drivers of declining R&D productivity
A. Looming patent cliffs and
high revenue requirements
I Higher attrition
B. High expectations of R&D
C. New R&D paradigms
D. Organizational complexity X Declining R&D
E. Increasing competitive productivity:
intensity II Higher numbers Flat/declining
of programs = output, soaring
F. Technological
R&D spend
innovation/automation
G. More complex X
targets/mechanisms/
molecules III Higher cost per
program
H. Regulatory scrutiny
I. Payor/HTA pressure
Singh N. McKinsey1990 – 2007
Category of root cause Description % of overall failures (n = 106)
Efficacy vs. placebo ▪ Failure to demonstrate significant
difference from placebo in treatment 45
effects
Confirmation of ▪ Safety issues either raised in earlier
early safety trials or seen in similar class of on- 8
Safety vs. concerns market compounds
placebo 27
Unclassifiable ▪ Unable to determine from outside-in
cause of safety failure 19
Efficacy ▪ Given similar safety profile, failure to
Lack of demonstrate superior efficacy vs. 24
differen- active comparator
tiation 28
Safety ▪ Given similar efficacy, failure to
demonstrate superior safety vs. active 4
comparator
Sources: Evaluate; Pharmaprojects; Factiva; literature search; team analysis 6´ Industry, regulators and academia are all in
this together.
´ This talk is not about Pharmacometrics – but it
is about the fundamental R&D goals. Excessive
focus on ‘confirmation’ is curtailing innovation.
I propose an alternative here for your
consideration.
Gobburu 7R&D Challenge
R&D
Learn & Apply, Cases
L&A Future
Future
Obsessive focus on ‘Confirm’ goal contributed to R&D inefficiency.
R&D goals ought to be about Learning, Applying.“Currently, the practical goal of drug
development is (regulatory) approval. This goal
drives the intellectual focus: demonstrating
(confirming) efficacy. Thus, understanding
confirmatory study design (primarily how to
avoid confounding) and devising and evaluating
test statistics are seen as the intellectually
challenging tasks as, indeed, a glance at the
contemporary clinical trial or biostatistics
literature will confirm.”
Learning versus confirming in clinical drug development
LB Sheiner, CPT, 1997
Gobburu 9Kola I, Landis J. Nat.Rev.Drug.Disc. Aug 2004. Gobburu 10
Gobburu 11
Gobburu 12
L ea r n
Apply
Gobburu 13Gobburu 14
´To confirm is important, but should not be the only goal of drug development. ´ Confirmation applies only effectiveness, but safety, dosing, why a trial failed, biomarker- endpoint relationship etc are equally important. Hence drug development decisions will need to take them into account. ´ Here is where Pharmacometrics comes in…
Decisions
• Go/No‐go,
Go/No‐go, trial design
• Approval, Label, Policy
• Personalized medicine
Analysis Information
• Quantitative disease
disease‐‐ • Data collected in trials
drug ‐trial modeling
drug‐trial and studies.
• Simulations • Domain expertise
Pharmacometrics is the science of quantifying disease, drug and trial
characteristics with the goal to influence drug development, regulatory
and therapeutic decisions.1950 1960 1970 1980 1990 2000 2010
Diverse
Expertise
FDA Data Physiology
Disease Drug Trial
Model Model Model
Molecule Trial Design
Dose
Screening Patient Selection Endpoints
Selection Policy
Gobburu, Pharmacometrics 18Remifentanil Cellcept
• One of the early MBDD • One of the early trials
• Approved dosing not designed prospectively by
directly studied in trials. advanced CTS.
Trileptal Firmagon
• Mono‐therapy in • First NDA with EOP2A
pediatrics approved based meeting.
on Pharmacometric‐ • Registration trial dose
bridging. No additional determined at EOP2A
trials needed. meeting.
• Drug currently approved.90
80
Number of Reviews
70
60
50
40
30
20
10
0´ 400 projects in 2008 for 10 companies
´ Senior management expects volume increase
´ Entry-level scientists expected to have some
pharmacometrics skills
PhRMA Survey. JCP 2010.70 Impact on Approval-ER
Approval
60 Labeling analysis provided
supportive or pivotal
Number of Reviews
50 evidence of
effectiveness.
40 Impact on labeling-ER
analysis supported D&A,
30 Warnings,
Intrinsic/Extrinsic
20
factors sections
10
045 45
40 40
35 35
% Reviews
% Reviews
30 30
25 25
20 20
15 15
10 10
5
5
0
0 6mo
6mo
Trial Duration Savings
Trial Duration Savings
70 60
60 50
% Reviews
% Reviews
50 40
40
30
30
20
20
10 10
0 0
6mo 400
Trial Duration Savings Trial Size Savings
Based on 2007-08 reviewsREGULATORY POLICY & OPPORTUNITIES Good Review Management Processes Office of Clinical Pharmacology (OCP) is expected to routinely review: - Does the exposure-response support evidence of effectiveness? - Is the proposed dosing strategy acceptable? Formation of Division of Pharmacometrics DPM was officially formed in 2009 within the OCP Integrated Genomics, Pharmacometrics, Clinical Pharmacology Review (IRP) Manual of Policies and Procedures (MAPP) IRP expects reviewers from the three disciplines and medical to scope the review questions within 45 days of a submission End-of-Phase IIA Meeting Guidance, MAPP Opportunity for industry and FDA to discuss competing development strategies earlier; driven by science.
Case#
1
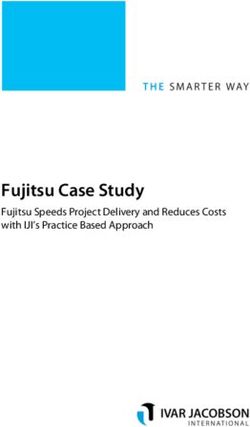
´ Sponsor was developing a drug for a life-
threatening condition.
´ Few approved drugs available in US
´ 3 Registration trials conducted
« ~600 patients, 3 doses
« Mild, severe baseline disease patients
« All 3 trials failed to meet primary endpoint
Gobburu 25Case#
1
Mild Baseline Disease Severe Baseline Disease
80
(Unlikely Responders) (Likely Responders)
80
60
Placebo-Subtracted Change
60
Placebo-Subtracted Change
In Score A at Week 12
In Score A at Week 12
40
40
20
20
0 0
-20 -20
-40 -40
0 5 10 15 20 25 30 0 5 10 15 20 25 30
Dose, mg Dose, mg
Gobburu 26Case#
1
M=Mild
S=Severe
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1
Yr1 Yr2 Yr3 Yr4 Yr5
Gobburu 27Case#
1
Gobburu 28Gobburu 29
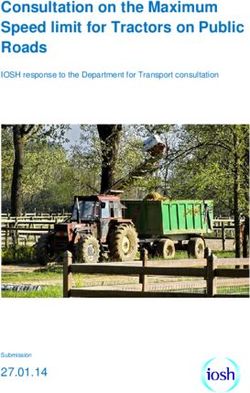
30
Insomnia patients LPS
% change from mean placebo response
-30
Y = 0.31x -32.5
-35
r2 = 0.66
PM approach and impact
-40 ▪ Sponsor developing a drug to treat insomnia
-45 held an end-of-phase 2a meeting (EOP2A)
-50
▪ Key questions discussed were:
– Is the dose range selected for the Phase
-55 2b studies in insomnia patients
-65 -60 -55 -50 -45 -40 -35 -30 -25 -20 -15 -10 -5 0 reasonable?
Healthy volunteers LPS, – What should be the duration of the Phase
% change from mean placebo response 2b studies?
▪ Analysis conducted by 1 person for
Insomnia patients WASO31
NDA submission – Feb 29, 2008; approval – Dec 24, 2008
Activity 2001 02 03 04 05 06 2007 PM approach and impact
CS02/N = ▪ Sponsor needed to determine the
129, 6 mo dosing for a drug 7 years in
development for advanced prostate
CS06/N = cancer patients
82, SD
▪ Key questions were:
CS07/N =
172, SD – Is a loading dose needed to
suppress testosterone, and, if so
CS12/N = how much?
187, 12 mo Registration
trial – Is a maintenance dose and
CS14/N = suppression regimen needed?
127, 12 mo
▪ Sponsor developed a mechanistic data
CS21/N = 610 model to explore dosing strategies via
trial simulations
EOP2A meeting
▪ Identified alternative dosing strategies
CS21 dose/
and clarified regulatory expectations
regimen that led to approval
not finalized
Mar 02 Mar 03 Mar 04 Mar 05 Mar 06 Mar 07
NOTE: Only dose-finding studies shownR&D Challenge
R&D
Learn & Apply, Cases
L&A Future
Future
Obsessive focus on ‘Confirm’ goal contributed to R&D inefficiency.
R&D goals ought to be about learning, applying.2020
Strategy Targets
• Health technology assessment
Share Case Studies
• Novel MOAs Publish, present 250
• Global drug development applications of
• Smarter safety testing Pharmacometrics.
Process Targets People Targets Business Targets
Standardize & automate Train 500 100% protocols designed
data, analysis, reports Pharmacometricians by simulations
for 15 indications´ Egan TD, Muir KT, Hermann DJ, Stanski DR and Shafer SL. The
electroencephalogram (EEG) and clinical measures of opioid potency: defining
the EEG-clinical potency relationship (‘fingerprint’) with application to
remifentanil. Intl J Pharm Med. 2001, 15: 001-002.
´ Reigner BG, Williams PE, Patel IH, Steimer JL, Peck C and van BP. An evaluation
of the integration of pharmacokinetic and pharmacodynamic principles in clinical
drug development. Experience within Hoffmann La Roche Clin Pharmacokinet
33:142-152, 1997.
´ Olson SC et al. Impact of population pharmacokinetic-pharmacodynamic analyses
on the drug development process: experience at Parke-Davis Clin Pharmacokinet
38:449-459, 2000.
´ Zhang L, Sinha V, Forgue ST, et al. Model-based drug development: the road to
quantitative pharmacology. J.PKPD. 33(3):369-393, 2006.
´ Lalonde RL et al. Model-based drug development. Clin Pharmacol Ther 82:21-
32, 2007.
´ Lee H, Yim DS, Zhou H, Peck CC. Evidence of effectiveness: how much can we
extrapolate from existing studies? AAPS J. 2005 Oct 5;7(2):E467-74. Review.
´ Bhattaram VA et al (2005) Impact of pharmacometrics on drug approval and
labeling decisions: a survey of 42 new drug applications. AAPS J 7:E503-E512.
´ Hale, Michael D, et al (1998) The pharmacokinetic-pharmacodynamic
relationship for mycophenoalte mofetil in renal transplant, Clin Pharmaco Ther,
64, pp. 672-683
´ Firmagon’s approval history.
www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseaction=search.
Label_ApprovalHistory (accessed 21 May 2010).You can also read