Joint Pennine Equality and Inclusion Strategy 2017- 2021 Blackburn with Darwen Clinical Commissioning Group and East Lancashire Clinical ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
NHS Blackburn with Darwen Clinical Commissioning Group
NHS East Lancashire Clinical Commissioning Group
Joint Pennine Equality and Inclusion Strategy
2017– 2021
Blackburn with Darwen Clinical Commissioning Group
and
East Lancashire Clinical Commissioning Group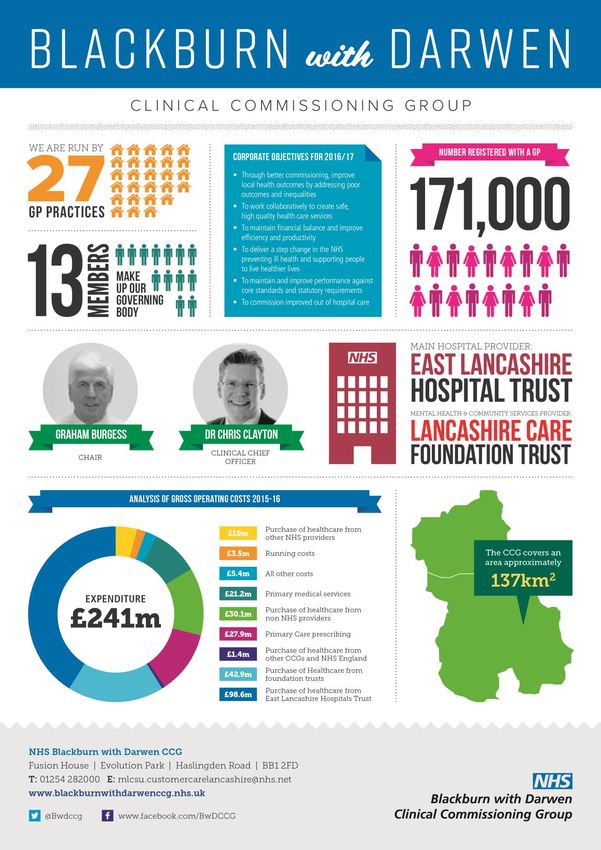
Contents
Document Status .............................................................................................................................................3
Executive Summary ..........................................................................................................................................3
Vision …………………………………………………………………………………………………………………………………………………………3
Our Priorities ....................................................................................................................................................4
Our Populations ................................................................................................................................................6
Local Demographics – Blackburn with Darwen ............................................................................................6
Local Demographics – East Lancashire .........................................................................................................7
Our Legal Duties ............................................................................................................................................ 10
The General Equality Duty ......................................................................................................................... 10
The Specific Public Sector Equality Duty ................................................................................................... 11
The Brown Principles ................................................................................................................................. 11
The Human Rights Act 1998 ...................................................................................................................... 12
Additional Standards ..................................................................................................................................... 12
Equality Delivery System (EDS).................................................................................................................. 12
Workforce Race Equality Standard............................................................................................................ 12
Accessible Information Standard .............................................................................................................. 12
The Equality Protected Groups ..................................................................................................................... 13
Our Equality Objectives for 2017 – 2021....................................................................................................... 15
What this means for the CCG’s ................................................................................................................. 17
Equality Impact and Risk Assessments .......................................................................................................... 17
Patient Involvement and Engagement .......................................................................................................... 18
Citizens Panel – NHS Blackburn with Darwen CCG ................................................................................... 18
Patient Partners Board – NHS East Lancashire CCG .................................................................................. 19
Customer Care ............................................................................................................................................... 20
Leadership and Governance .......................................................................................................................... 20
Our Staff ........................................................................................................................................................ 21
Commissioning and Procurement ................................................................................................................. 21
Service Redesign and Contract or Quality Reviews ................................................................................... 21
Policy Development and Review ................................................................................................................... 22
Quality and Performance Management ........................................................................................................ 22
How the Equality and Inclusion Strategy link to our Vision, Strategic Planning and Commissioning
Intentions ...................................................................................................................................................... 22
2|Page
Document Status
Both NHS Blackburn with Darwen Clinical Commissioning Group (CCG) and NHS East Lancashire
CCG have agreed to joint working on common areas of work. As such this document details the
combined strategy across both organisations. Unless clearly documented the term ‘CCG,’ ‘CCGs’
or ‘our’ within this strategy should be taken to refer to both NHS Blackburn with Darwen and NHS
East Lancashire CCGs.
Executive Summary
NHS Blackburn with Darwen and NHS East Lancashire CCGs are clinically-led membership
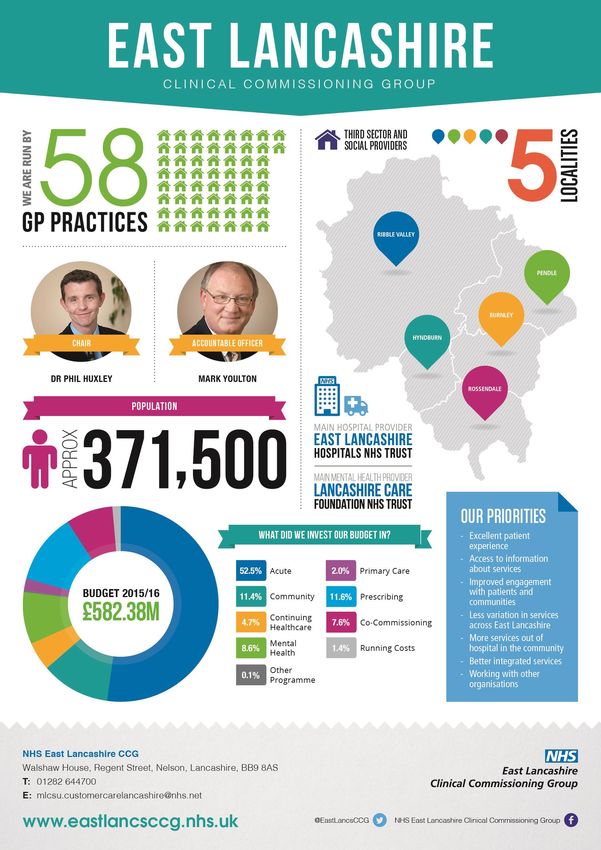
organisations, made up of the 27 General Practices (GPs) in Blackburn with Darwen and 58
General Practices in East Lancashire. The CCG’s role is to commission (buy) healthcare services
for local people and we are committed to improving the health of our community.
Our joint Equality and Inclusion Strategy sets out our commitment to taking equality and
inclusion into account in everything we do. We recognise the importance of embedding equality
principles and practices within the organisation and how equality can support us as Clinical
Commissioning Groups to commission the right services for our local population.
This strategy will be a flexible framework for our equality and inclusion activity which is an
integral part of the way we do business. Within Blackburn with Darwen specifically it will support
the delivery of our 2030 Vision for Health Care in Blackburn with Darwen.
In summary this strategy aims to harness how we achieve better health outcomes, improve
patient access and experience, have a represented and supported workforce and have inclusive
leadership.
This strategy will be reviewed annually, information will be provided to the CCGs Governing
Bodies on an annual basis through the Equality and Inclusion Annual Report to ensure that the
aims and objectives within this strategy are being progressed.
Graham Burgess, Phil Huxley,
Blackburn with Darwen East Lancashire CCG Chair
CCG Chair and Equality Lead
3|Page
Our Visions
NHS Blackburn with Darwen CCG
‘To deliver effective, efficient, high quality, safe, integrated care. This will improve the health and
wellbeing of the population of Blackburn with Darwen and help people live better for longer,
reducing health inequalities and improving outcomes in the borough’.
NHS East Lancashire CCG
‘To use clinical expertise, available evidence and patient experience to ensure that the right
services are commissioned for patients to be seen at the right time, in the right place, by the right
professionals’.
Our Priorities
We aim to uphold the pledges in the NHS Constitution and secure better outcomes for patients
as defined by the five domains of the NHS Outcomes Framework. They are:
1 Preventing people from dying prematurely
2 Enhancing the quality of life for people with long term conditions (LTC)
3 Helping people to recover form episodes of ill health following injury
4 Ensuring people have a positive experience of care
5 Treating and caring for people in a safe environment and protecting them from
avoidable harm
NHS Blackburn with Darwen CCG Corporate NHS East Lancashire CCG Strategic Priority
Objectives for 2016/17 Areas for 2016/17
Through better commissioning, improve Access to urgent care
local health outcomes by addressing poor
outcomes and inequalities
To work collaboratively to create safe, high Developing primary care services
quality health care services
To maintain financial balance and improve Developing services to avoid unplanned
efficiency and productivity admission to hospital
To deliver a step change in Redesigning pathways of care in areas for
the NHS preventing ill health and services such as stroke, diabetes
supporting people to live healthier lives
To maintain and improve performance Work to improve access to mental health
against core standards and statutory services
requirements
To commission improved out of hospital Work to develop dementia care services
care
4|Page5|Page
Our Populations
The social and economic profiles of Blackburn with Darwen and East Lancashire present a broad
range of challenges in developing local health services. National indicators show local health is
generally significantly worse than the England average.
Local Demographics – Blackburn with Darwen
Covering an area of 13,700 hectares, Blackburn with Darwen comprises the two towns of
Blackburn and Darwen and the surrounding countryside. The 2011 Census revealed that the
Borough had approximately 57,453 households and 147,489 residents, which was an increase on
previous estimates. The most recent mid-2014 population estimate, however, shows a slight dip
for the second year running, to stand at 146,743.
Life expectancy in Blackburn with Darwen has risen over recent years and is currently settled at
76.7 years for males and 81.1 years for females in 2012-14. For both males and females, the
biggest impact on life expectancy would come from closing the gap in coronary heart disease
deaths. Male life expectancy in the most deprived tenth of the Borough was 13.5 years lower
than in the least deprived tenth. This is partly a reflection of the wide range of deprivation levels
found within the borough. However, the deprivation gradient for female life expectancy is much
less steep.
People
The Borough’s population is diverse, with the proportion of non-white residents amongst the
highest in the region, mostly from Indian or Pakistani backgrounds (each estimated at 9% before
the Census). Changes in the population structure over the coming 20 years will create significant
additional demand for health and social care services in the Borough.
Existing projections already suggested that the population would reach 159,000 by 2035, with
the proportion of people aged 65+ increasing from 13% to 17%, and the number of very elderly
residents (85+) almost doubling. These may now be expected to be revised upwards following
the Census results. The most significant underlying population factor that will impact on current
and future health and on health inequalities is:
Community
The Borough experiences high levels of material deprivation, being the 17th most deprived
Borough based on the 2010 Index of Multiple Deprivation, with eight small neighbourhoods
amongst the most deprived 1% nationally. Through comparison between 2007 and 2010 Indices
of Multiple Deprivation, some of our most deprived neighbourhoods appear to be becoming
relatively more deprived.
The combination of embedded disadvantage and a fast-changing demography results in concerns
around social cohesion. Over a range of health indicators, such as alcohol-related hospital
admissions, smoking-related mortality, early deaths from cancers and circulatory disease and
6|Pageinfant mortality, Blackburn with Darwen’s rates are significantly worse than both England and the
North West.
Looking ahead
Changes in the population structure over the coming 20 years will create significant additional
demand for health and social care services in the Borough. Existing projections already
suggested that the population would reach 159,000 by 2035, with the proportion of people aged
65+ increasing from 13% to 17%, and the number of very elderly residents (85+) almost doubling.
Ref: Blackburn with Darwen Joint Health & Wellbeing Strategy 2012 - 2015
Our Challenges
Health in summary
The health of people in Blackburn with Darwen is generally worse than the England average.
Blackburn with Darwen is one of the 20% most deprived districts/unitary authorities in
England and about 22% (7,800) of children live in low income families. Life expectancy for both
men and women is lower than the England average.
Health inequalities
Life expectancy is 11.9 years lower for men and 8.3 years lower for women in the most deprived
areas of Blackburn with Darwen than in the least deprived areas.
Child health
In Year 6, 18.6% (356) of children are classified as obese. The rate of alcohol-specific hospital
stays among those under 18 was 62.4*, worse than the average for England.
This represents 24 stays per year. Levels of smoking at time of delivery are worse than the
England average.
Adult health
The rate of alcohol-related harm hospital stays is 797*, worse than the average for England. This
represents 1,072 stays per year. The rate of self-harm hospital stays is 316.7*, worse than the
average for England. This represents 477 stays per year. The rate of smoking related deaths is
360*, worse than the average for England. This represents 229 deaths per year. Estimated levels
of adult smoking and physical activity are worse than the England average. Rates of people killed
and seriously injured on roads and TB are worse than average. The rate of sexually transmitted
infections is better than average.
Local priorities
Priorities in Blackburn with Darwen include tackling the social determinants of health and
reducing inequalities across the life course, including mental health and wellbeing, social isolation
and long term conditions.
7|PageLocal Demographics – East Lancashire
8|PagePopulation Profile
East Lancashire CCG serves a population of approximately 371,500 people, with urban areas such
as Burnley, Rossendale, Nelson and Accrington alongside market towns such as Clitheroe, villages
and rural areas we have 58 GP Member Practices.
We have an aging population, with the number of people over 75 years old increasing. Older
people often have complex and long-term health problems, such as chronic illnesses and more
than one condition, which we call co-morbidities. In East Lancashire, we also have a higher than
England average number of children and young people, meaning we also need to take their
needs into account when commissioning services.
Most of the residents of East Lancashire are White British, though there are a significant number
of people of South Asian origin, making up 11 per cent of the registered population.
It is estimated that the 65+ population will increase 16% over the next 10 years.
Community
Burnley, Hyndburn and Pendle all have significantly higher levels of deprivation than the England
average. Burnley and Hyndburn both have a significantly higher proportion of children. Burnley,
Hyndburn and Pendle all have significantly fewer pupils achieving 5 GCSEs at grades A*-C than
the England average.
Burnley and Hyndburn both have a significantly higher violent crime rates than the England
average and long term unemployment: Burnley has a significantly higher rate of long term
unemployed than the England average.
Our Challenges
Addressing lifestyle challenges in both primary care and through health improvement services:
Smoking prevention and cessation, plus prevention and management of obesity and
excess alcohol intake.
The commissioning of maternity and children’s services, reflecting the special needs of
deprived and ethnic minority communities.
The changing health needs of a population with an increasing number of elderly people,
such as multiple long term conditions and dementia.
The need for better ascertainment of patients with chronic disease, to enable
programmes of self-care and integrated health and social care to be better targeted.
Further detailed scrutiny of areas where there is relatively high premature mortality, such
as cancer.
Careful consideration of emergency presentations to hospitals and elective referral rates,
seeking to reduce variations between practices with similar characteristics (in the same
cluster).
9|PageChild Health
Over 30% of Year sic children in Burnley, Hyndburn and Pendle are estimated to be obese. In
Burnley and Hyndburn alcohol-specific hospital stays among the under 18 are significantly higher
than the England average and Burnley Hyndburn districts have significantly higher under 18
conception rates than the England average.
Adult health
Smoking prevalence: Burnley has a higher smoking prevalence than the England average.
Significantly fewer adults in the Burnley and Pendle districts are believed to be physically active
compared to the England average. Over 20% of adults in each of the East Lancashire districts are
believed to be obese. The districts of Burnley, Hyndburn and Pendle have higher recorded
diabetes prevalence than the England average.
Source: East Lancashire CCG Mini Summary Profile 2015/16
Our Legal Duties
The Equality Act 2010 imposes general and specific duties on all public bodies.
The General Equality Duty
The general duty applies to ‘public authorities’. Further advice about who this includes is
provided in the next section.
In summary, those subject to the general equality duty must, in the exercise of their functions,
have ‘due regard’ to the need to:
Eliminate unlawful discrimination, harassment and victimisation and other conduct
prohibited by the Act.
Advance equality of opportunity between people who share a protected characteristic
and those who do not.
Foster good relations between people who share a protected characteristic and those
who do not.
These are often referred to as the three aims of the general equality duty.
The Equality Act explains that the second aim (advancing equality of opportunity) involves, in
particular, having due regard to the need to:
Remove or minimise disadvantages suffered by people due to their protected
characteristics.
Take steps to meet the needs of people with certain protected characteristics where
these are different from the needs of other people.
Encourage people with certain protected characteristics to participate in public life or in
other activities where their participation is disproportionately low.
10 | P a g eThe Act states that meeting different needs includes (among other things) taking steps to take
account of disabled people’s disabilities. It describes fostering good relations as tackling
prejudice and promoting understanding between people from different groups.
The Specific Public Sector Equality Duty
As well as complying with the general duty, we must also comply with the following specific
duties:
Publish information to demonstrate compliance with the public sector Equality Duty at
least annually.
Prepare and publish equality objectives at least every four years.
This information can be found on the CCG’s equality and inclusion website page
http://www.blackburnwithdarwenccg.nhs.uk/
http://eastlancsccg.nhs.uk/
The Brown Principles
These principles have been taken from the Equality and Human Rights Commission’s paper on
making fair financial decisions (Equality and Human Rights Commission, 2012).
Case law sets out broad principles about what public authorities needs to do to have ‘due regard’
to the aims set out in the general equality duties. These are sometimes referred to as the ‘Brown
Principles’ and set out how courts interpret the duties. They are not additional legal
requirements, but form part of the Public Sector Equality Duty as contained in section 149 of the
Equality Act 2010.
Decision makers must be aware of their duty to have ‘due regard’ and to the aims of the
duty.
‘Due regard’ is fulfilled before and at the time a particular policy that will or might affect
people with protected characteristics is under consideration, as well as at the time a
decision is made.
‘Due regard’ involves a conscious approach and state of mind. A body subject to the duty
cannot satisfy the duty by justifying a decision after the decision has been taken.
The duty must be exercised in substance, with rigour and with an open mind in such a
way that it influences the final decision.
The duty has to be integrated with the discharge of the public functions of the body
subject to the duty. It is not a question of ‘ticking boxes’.
The duty cannot be delegated and will always remain on the body subject to it.
It is good practice for those exercising public functions to keep an accurate record
showing that they had actually considered the general equality duty. If records are not
kept it may make it more difficult, evidently, for a public authority to persuade a court
that it has fulfilled its duty imposed to the equality general duty.
11 | P a g eThe Human Rights Act 1998
The Human Rights Act 1998 refers to the rights and freedoms that belong to all individuals
regardless of their nationality or citizenship. These rights cover matters of life and death but also
everyday rights such as what a person can say or do, their beliefs, right to a fair trial and other
basic entitlements including freedom from discrimination.
Blackburn with Darwen CCG and East Lancashire CCG are committed to upholding the human
rights of staff, patients, carers and communities by taking into account the FREDA model
identified within ‘Human Rights in Healthcare: A framework for Action’: All policies and actions
take into consideration all of these elements.
Additional Standards
Equality Delivery System (EDS)
The EDS is a national tool which has been mandated by NHS England to all NHS organisations
since April 2015. It is used to support the CCG to deliver better equality outcomes for patients
and communities and better working environments for staff, which are personal, fair and diverse.
The EDS provides a robust framework against which we can assess and grade its performance
against a range of nationally determined indicators grouped under the four goals:
• Better health outcomes
• Improved patient access and experience
• A representative and supported workforce
• Inclusive leadership
Workforce Race Equality Standard
NHS Workforce Race Equality Standard (WRES) mandated in 2015 is a useful tool to identify and
reduce any disparities in experience and outcomes for NHS employees and job applicants of
different ethnicities. The Standard will help to support organisations to track progress to identify
and help eliminate discrimination in the treatment of Black and Minority Ethnic (BME)
employees.
Accessible Information Standard
The aim of the Accessible Information Standard mandated in 2016 is to make sure that people
who have a disability, impairment or sensory loss receive information that they can access and
understand and any communication support that they need.
12 | P a g eThe Accessible Information Standard informs organisations how they should make sure that
patients and service users, and their carers and parents, can access and understand the
information they are given. This includes making sure that people get information in different
formats if they need it, for example in large print, braille, easy read or via email.
The Accessible Information Standard also informs organisations how they should make sure that
people get any support with communication that they need, for example support from a British
Sign Language (BSL) interpreter, deafblind manual interpreter or an advocate.
Commissioners must ensure that their commissioning and procurement processes, including
contracts, frameworks and performance management arrangements, with providers of health
and/or adult social care reflect, enable and support implementation and compliance with this
standard.
Commissioners must seek assurance from provider organisations of their compliance with this
standard, including evidence of identifying, recording, flagging, sharing and meeting of needs.
The Equality Protected Groups
The Equality Act 2010 replaced previous anti-discrimination laws and places key duties on
statutory organisations that provide public services. It protects people from unfavourable
treatment and this refers particularly to people from the following categories known as the
Equality Protected Group or protected characteristics:
Protected Equality Definition
Group
Age Age is defined by being of a particular age (for example being 35 years old)
or by being in a range of ages (for example being between 60 and 75 years
old).
Disability A person is classed as having a disability if they have a physical or mental
health condition and this condition has a ‘substantial and long-term adverse
effect on his or her ability to carry out normal day to day activities.’ These
words have the following meanings:
Substantial means more than minor or trivial.
Long term means that this condition has lasted or is likely to last for
more than twelve months. There are progressive conditions that are
considered to be a disability.
These include:
People who have had a disability in the past that meets this
13 | P a g edisability.
There are additional provisions relating to people with progressive
conditions.
People with HIV, cancer, multiple sclerosis are covered by the Act
from diagnosis.
People with some visual or hearing conditions are automatically
deemed to have a disability.
Gender Gender reassignment protects people who have changed their gender from
Reassignment what they were identified as at birth. The Equality Act covers people at any
stage of this process.
Sexual Orientation Sexual orientation means a person’s sexual preference towards people of
the same sex, opposite sex or both.
Sex Sex (gender) is included to protect the individual man or woman from being
discriminated against.
Race Race refers to a group of people defined by their race, colour and
nationality (including citizenship) ethnic or national origins.
Religion or Belief Religion has the meaning usually given to it but belief includes religious
convictions and beliefs including philosophical belief and lack of belief.
Generally, a belief should affect your life choices or the way you live, for it
to be included in the definition.
Pregnancy and Pregnancy is the condition of being pregnant or expecting a baby.
Maternity Maternity refers to the period after the birth, and is linked to maternity
leave in the employment context. Protection against maternity
discrimination is for 26 weeks after giving birth.
Marriage and Civil The definition of marriage varies according to different cultures, but it is
Partnership principally an institution in which interpersonal relationships are
acknowledged and can be between different sex and same sex partners.
Same-sex couples can have their relationships legally recognised as ‘civil
partnerships’. In England and Wales marriage is no longer restricted to a
union between a man and a woman but now includes a marriage between a
same sex couple.
14 | P a g eOur Equality Objectives for 2017 – 2021
The Equality Strategy links to a number of key drivers but is based on the requirements of the
NHS Equality Delivery System (EDS) which aims to embed equality into all policies and practices
whilst driving up performance and going beyond the legislation.
The EDS provides a robust framework against which we can access and grade our performance
against a range of outcomes grouped under the four EDS goals. The CCGs will focus on one EDS
Goal annually over a 4 year cycle to ensure that it is covering every aspect of the mandated EDS.
Overarching Equality To deliver effective, efficient, high quality, safe, integrated care.
Objective
This will improve the health and wellbeing of the population of
Blackburn with Darwen and East Lancashire and help people live
better for longer, reducing health inequalities and improving
outcomes in the borough.
Equality Objective 1 EDS Goal 1: Better health outcomes
1.1 Services are commissioned, procured, designed and delivered to
meet the health needs of local communities
1.2 Individual people’s health needs are assessed and met in
appropriate and effective ways
1.3 Transitions from one service to another, for people on care
pathways, are made smoothly with everyone well-informed
1.4 When people use the NHS services their safety is prioritised and
they are free from mistakes, mistreatment and abuse
1.5 Screening, vaccination and other health promotion services reach
and benefit all local communities
15 | P a g eEquality Objective 2 EDS Goal 2: Improved patient access and experience
2.1 People, carers and communities can readily access hospital,
community health or primary care services and should not be denied
access on unreasonable groups
2.2 People are informed and supported to be as involved as they wish
to be in decisions about their care
2.3 People report positive experiences of the NHS
2.4 People’s complaints about services are handled respectfully and
efficiently
Equality Objective 3 EDS Goal 3: A representative and supported workforce
3.1 Fair NHS recruitment and selection processes lead to a more
representative workforce at all levels
3.2 The NHS is committed to equal pay for work of equal value and
expects employers to use equal pay audits to help fulfil their legal
obligations
3.3 Training and development opportunities are taken up and
positively evaluated by all staff
3.4 When at work, staff are free from abuse, harassment, bullying and
violence from any source
3.5 Flexible working options are available to all staff consistent with
the needs of the service and the way people lead their lives
3.6 Staff report positive experiences of their membership of the
workforce
Equality Objective 4 EDS Goal 4: Inclusive Leadership
4.1 Boards and senior leaders routinely demonstrate their
commitment to promoting equality within and beyond their
organisations
4.2 Papers that come before the Board and other major Committees
identify, equality-related impacts including risks, and say how these
risks are managed
16 | P a g e4.3 Middle managers and other line managers support their staff to
work in culturally competent ways within a work environment free
from discrimination
What this means for the CCG’s
Our progress in meeting these objectives will be assessed and graded in discussion with our local
population and our staff at our EDS Grading assessments. The result of the EDS Grading
assessment will be published on the CCG website, the EDS grading will also be reported on within
the CCG’s E&I annual report.
Equality Impact and Risk Assessments
The Clinical Commissioning Groups have adopted the Equality Impact and Risk Assessment (EIRA)
Tool designed by NHS Midlands and Lancashire Commissioning Support Unit. The EIRA provides a
framework for undertaking equality impact assessments. This combines three toolkits into one
consisting of equality impact, human rights screening and privacy impact. This enables the CCG
to show ‘due regard’ to the three aims of the general equality duty by ensuring that all
requirements around equality, human rights and privacy are given advanced consideration prior
to any policy decisions that the CCG’s Governing Body or senior managers make that may be
affected by these issues. CCG commissioners continue to ensure that the Equality Impact and
Risk Assessment are integral to the decision making processes.
The CCG has embedded the Equality Impact and Risk Assessment into their commissioning cycle.
All Equality Impact and Risk Assessments are quality checked by the CSU Equality and Inclusion
Team to ensure that CCG Commissioners and staff working on behalf of the CCG have considered
all the equality information and engaged and involved local people from Equality Protected
Groups in the decision making process.
Any commissioner wanting to redesign a service and re- write a service specification carries out
an initial EIRA assessment as part of the redesign process. The same process applies to policies
being drawn up that have an impact on our public and patients as well as staff.
17 | P a g eAll service redesigns, service specification and business cases need the support of the relevant
commissioning group (Governing Body Sub-Committee). The chair of these groups will not
accept a paper where an initial Stage 1 EIRA has not been conducted and the assurance that the
EIRA has been reviewed by the E&I team.
Patient Involvement and Engagement
We are committed to involving all sections of the community in development of our objectives
and action plans. We will continue to strive to give every opportunity to our key stakeholders to
comment on health services in Blackburn with Darwen and East Lancashire.
Citizens Panel – NHS Blackburn with Darwen CCG
The CCG has created a public membership scheme called the Citizens Panel. Members of the
public will be recruited to a database and a random selection will be invited to take part in
engagement quarterly. As part of the recruitment process, members of the public will be asked
how they prefer to engage with the CCG – face to face, public events, reach out to
specialist/interest groups, focus groups, surveys both written and electronic, digital forums etc.
and we will commit to engaging with them using the channel of their choice. This would enable
patients and public to get involved and to influence commission decisions.
To strengthen this mechanism for engagement, it is also proposed to look at the feasibility of
linking the membership scheme with the existing PPG network. PPGs provide an invaluable
opportunity to gain information from patients who represent all of our constituent practices and
to also feed issues back into the individual practice patient groups they represent. However, the
current groups have small memberships, meet on an ad hoc basis and are in need of support to
strengthen them in terms of numbers and activity. In addition, it is recognised that the CCG’s
reach will be so much wider and more effective if we are able to harness our partners’ channels
and networks.
A Partner Engagement Group has been created including Healthwatch, Carers, the local
authority, public health, voluntary sector etc. By working with partners who have expertise in
communicating with ‘seldom heard’ groups, this will also help the CCG to communicate and
engage with groups which often have the greatest health and healthcare challenges, but who can
struggle to have a voice. It is also important that the CCG utilises this capacity and capability in
18 | P a g ethe gathering, interpretation and use of service experience, in partnership with such
organisations as HealthWatch to avoid duplication.
Patient Partners Board – NHS East Lancashire CCG
In 2015, our Governing Body learned from a patient story that while patient participation groups
(PPGS) are established, they don’t necessarily feel joined up, nor connected to the CCG. As a
consequence of this, our Lay Member for Patient and Public Involvement, Michelle Pilling
established the Patient Partnership Board.
The Board consists of PPG network Chairs, and local PPG representatives, as well as Carers Link,
and HealthWatch. The Patient Partners Board provides advice and oversight of patient and
public involvement to the Governing Body. The Board has proved to be a useful forum and has
contributed to a more joined up PPG network whose members are actively contributing to the
CCG and health service improvements.
The CCG has attracted a number of patients and public representatives who wish to participate in
and contribute to the commissioning of health services. We established Patient Partners as an
involvement network to enable patients to get involved in the work of the CCG, and more
importantly to contribute to improvements.
The PPG network has a core of interested patients and patient representatives, mainly recruited
via individual practice patient participation groups (PPGs) and via comprehensive engagement
activity in relation to primary care access and work on scheduled care. Anyone registered with
the GP practice is entitled to become a member of their PPG. Members of the PPGs have the
opportunity to work with doctors and practice managers to Influence decisions about services
and facilities, help practices make the best use of resources and ensure patient views are
properly represented at GP practice level.
Both CCGs are committed to ensuring that they have effective communications and engagement
channels in place with a range of stakeholders in order to ensure that the CCGs can receive and
use intelligence to inform commissioning decisions. This will help the CCGs make sure that health
19 | P a g eservices in Blackburn with Darwen and East Lancashire are shaped to meet patient and service
user needs, both now and in the future.
The CCGs have in place an Engagement and Involvement Working Group and the role of this
group’s is to ensure and seek assurance that this principle is central to the CCGs service redesign,
transformation and planning work. It will do this by:
Ensuring the CCG Governing Body receives, hear and consider the patients and public’s
view
Monitor and evaluate the success of the CCG’s Patient and Public engagement work and
communication work
Review and consider how patient and public feedback should be used and employed by
the CCG to inform its plans.
Customer Care
The CCGs place a high priority on the handling of concerns and complaints and recognises they
are a valuable aid to improving services. Midlands and Lancashire Commissioning Support Unit
(CSU) manage complaints on behalf of the CCG and also offer a Patient Liaison Service (PALS).
We are committed to working with the CSU to provide the best service for patients, their families
and carers.
The CCGs are committed to equal opportunity. No patient, or any other person involved in the
investigation and resolution of a complaint, will receive unfair treatment on the grounds of age,
race, ethnic or national origins, religious or their beliefs, gender, marital status, sexual orientation
or disability. The CSU monitors each complaint and records whether the complaint is an Equality
issue. All complaints are made in confidence and will not affect the provision of treatment.
Leadership and Governance
A fundamental role of the CCGs Governing Body Members is to promote, challenge
discrimination and foster good relationships as set out in the Equality Act 2010. Within both CCGs
there is an Equality and Inclusion champion at Governing Body level who are supported by a
small operational team.
20 | P a g eThe CCGs combined leadership approach ensures that there is fairness in our commissioning
decisions and that business is planned and conducted to meet our equality duties. Our Pennine
Lancashire Quality Committee monitors performance against the equality objectives.
The CCG have allocated specific resources for our Equality and Inclusion Strategy that include
staff from both CCGs and additional external resources such as support from the Equality and
Inclusion Team, Midlands and Lancashire Commissioning Support Unit.
Our Staff
We are committed to recruiting, retaining and developing a diverse and skilled workforce. We
are not required by law to collect equality data on our staff, however we have chosen to improve
on this data with the WRES and EDS.
Equality and Inclusion training is routinely provided and mandatory for all staff. The Governing
Body Members of both CCGs have an annual Equality and Inclusion development session which
explains the Governing Body role in meeting the organisations equality duties.
Commissioning and Procurement
Each year, the CCG enters into contracts for buying clinical services. Procured and commissioned
work provides core services to many of our local population and sustains and generates
thousands of jobs, the CCG has a statutory duty to ensure that public money is spent in a way
that ensures Best Value and provides equality of access and outcome for all residents. Staff
responsible for commissioning or procurement should ensure we are meeting our equality and
inclusion duties and meeting the needs of our diverse community.
Service Redesign and Contract or Quality Reviews
Service redesign is the way the CCGs reflect on existing or past commissioning services provision
and plans for the future, establishing key objectives and targets for the coming year. Staff
responsible for service redesign should take this opportunity to assess whether the service is
meeting its equality and inclusion duties and ensure due regard for access to services and
outcomes of satisfaction with the service they deliver are not different or worse for some
patients or communities. Contract or quality reviews are a more fundamental assessment of
commissioned services not just covering how, when and where services are delivered but
21 | P a g ewhether they are delivered at all, staff responsible for carrying out service contract or quality
reviews need to evaluate how service currently meet their equality and inclusion legal duties and
take due regard in considering whether any review will have a detrimental effect protected
characteristics or whether any changes will impact differently or work for some people/patients.
Policy Development and Review
The CCGs produce a range of both clinical and corporate policies to ensure that staff provide, and
patients receive high quality care and treatment. ‘The Equality Impact and Risk Assessment’ of
our policies is attached at the end of the Policies’.
Staff responsible for policy development needs to ensure the policy they are developing and
implementing meets our legal duties in relation to equality and inclusion and takes on board the
views of the local population and our staff.
Quality and Performance Management
The CCG’s Quality and Performance Framework covers a range of activity from how we plan our
finances and services, how we set objectives and targets, how we monitor and measure
performance of our providers and our staff through personal development plans and appraisals
and our corporate objectives.
The CCGs have performance indicators for measuring progress and performance; many are linked
to equality of access and outcomes of service delivery, we will continue to work on defining our
approach to measuring our health and progress relating to equality.
How the Equality and Inclusion Strategy link to our Vision, Strategic Planning and
Commissioning Intentions
The approach to Equality and Inclusion set out in this strategy is to ensure it is integrated in all
mainstream activity. The strategy needs to be integral to how we identify and achieve the right
outcomes in relation to the CCG’s strategic approach to the Integrated Strategic Needs
Assessment and, specific to NHS Blackburn with Darwen CCG, the Blackburn with Darwen Health
and Wellbeing Strategy.
22 | P a g eGovernance and Reporting
The Governance route at both CCG’s for Equality and Inclusion reporting is through the Pennine
Lancashire Quality Committee and the Governing Body.
Pennine Lancashire
Governing Body
Quality Committee
Annual Report and Strategy Review
During each year the CCGs will gather, store and publish evidence such as Equality Impact and
Risk Assessments, Consultation, Engagement and Involvement exercises for the purpose of
demonstrating our legal compliance and also any Freedom of Information requests.
The Pennine Lancashire Quality Committee will monitor activity in relation to our organisational
priorities for Equality and Inclusion. The Equality and Inclusion Team, MLCSU will produce an
annual report, which will provide progress and action on our equality objectives each year and at
least every four years will lead on a review of our Equality strategy objective.
Equality and Inclusion Strategy produced by the Equality and Inclusion Team,
Midlands and Lancashire Commissioning Support Unit
April 2017
23 | P a g eYou can also read