Journal of the Italian Society of Anatomic Pathology and Diagnostic Cytopathology, Italian Division of the International Academy of Pathology ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Cited in Index Medicus/MEDLINE, BIOSIS Previews, SCOPUS
Journal of the Italian Society of Anatomic Pathology and Diagnostic Cytopathology,
Italian Division of the International Academy of Pathology
Periodico trimestrale - Aut. Trib. di Genova n. 75 del 22/06/1949 - ISSN: 0031-2983 (Print) – ISSN: 1591-951X (Online)
In this issue:
Review
Glomus coccygeum: a review
Original article
Detection and genotyping of hpv-dna through different types of diagnostic
platforms in liquid-based cervical-cytology samples Vol. 110 December 2018
Case reports
Pathologica storica
Pathologica ai tempi della Spagnola
Proceedings
IV Meeting Nazionale Gruppo Italiano Paleopatologia
Società Italiana di Anatomia Patologica e Citopatologia Diagnostica,
Divisione Italiana della International Academy of Pathology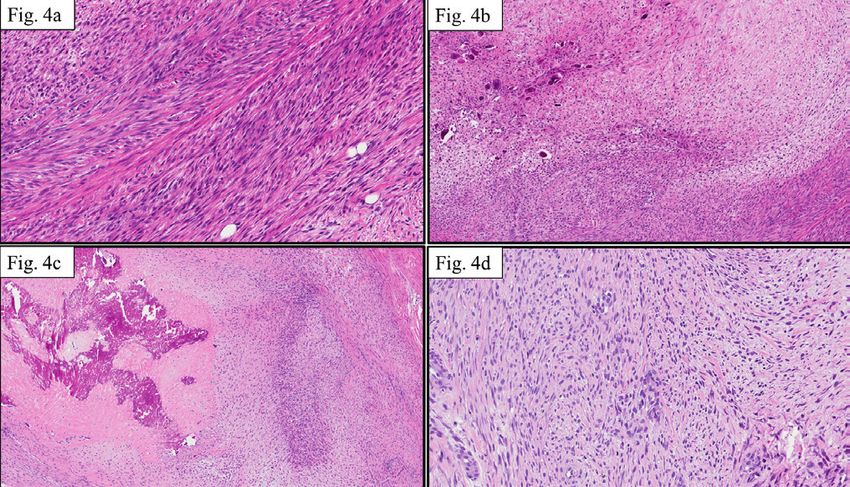
Cited in Index Medicus/MEDLINE, BIOSIS Previews, SCOPUS
Journal of the Italian Society of Anatomic Pathology
and Diagnostic Cytopathology,
Italian Division of the International Academy of Pathology
Editor-in-Chief L. Resta, Bari Copyright
M. Barbareschi, Trento G. Rindi, Roma Società Italiana di Anatomia
A.G. Rizzo, Palermo Patologica e Citopatologia
Associate Editor G. Rossi, Modena Diagnostica, Divisione Vol. 110 December 2018
M. Chilosi, Verona G. Santeusanio, Roma Italiana della International
A. Sapino, Torino Academy of Pathology
Managing Editor L. Saragoni, Forlì
P. Nozza, Genova G.L. Taddei, Firenze Publisher
G. Tallini, Bologna Pacini Editore S.r.l.
Scientific Board L. Ventura, L’Aquila Via Gherardesca, 1
R. Alaggio, Padova G. Zamboni, Verona 56121 Pisa, Italy
G. Angeli, Bologna Tel. +39 050 313011
V. Barresi, Messina Editorial Secretariat Fax +39 050 3130300
A. Bondi, Bologna M. Brunelli, Verona info@pacinieditore.it
G. Bulfamante, Milano G. Martignoni, Verona www.pacinimedicina.it
G. Cenacchi, Bologna F. Pedica, Milano
C. Clemente, Milano
M. Colecchia, Milano Governing Board
P. Cossu-Rocca, Olbia SIAPEC-IAP
G. d’Amati, Roma President:
E. d’Amore, Vicenza
M. Truini, Milano
A. D’Errico, Bologna
C. Doglioni, Milano President Elect:
F. Facchetti, Brescia A. Sapino,Torino
G. Fornaciari, Pisa
M.P. Foschini, Bologna General Secretary:
G. Fraternali Orcioni, Genova E. Bonoldi, Lecco
E. Fulcheri, Genova Past President:
W. Grigioni, Bologna
G. De Rosa, Napoli
M. Guido, Padova
L. Leoncini, Siena Members:
M. Lestani, Vicenza M. Basciu, Bolzano
G. Magro, Catania E. Bonoldi, Lecco
E. Maiorano, Bari G.Fadda, Roma
A. Marchetti, Chieti A. Maria Florena, Palermo
G. Marucci, Bologna E. Fulcheri, Genova
B. Murer, Venezia E. Maiorano, Bari
O. Nappi, Napoli A. Marchetti, Chieti
G. Negri, Bolzano D. Massi, Firenze
A. Orlandi, Roma G. Mazzoleni, Bolzano
M. Papotti, Torino G. Negri, Bolzano
M. Paulli, Pavia F. Pietribiasi, Torino
G. Pelosi, Milano
F. Pierconti, Roma Associate Members
S. Pileri, Bologna Representative:
P. Querzoli, Ferrara T. Zanin, Genova
Società Italiana di Anatomia Patologica e Citopatologia Diagnostica,
Divisione Italiana della International Academy of Pathology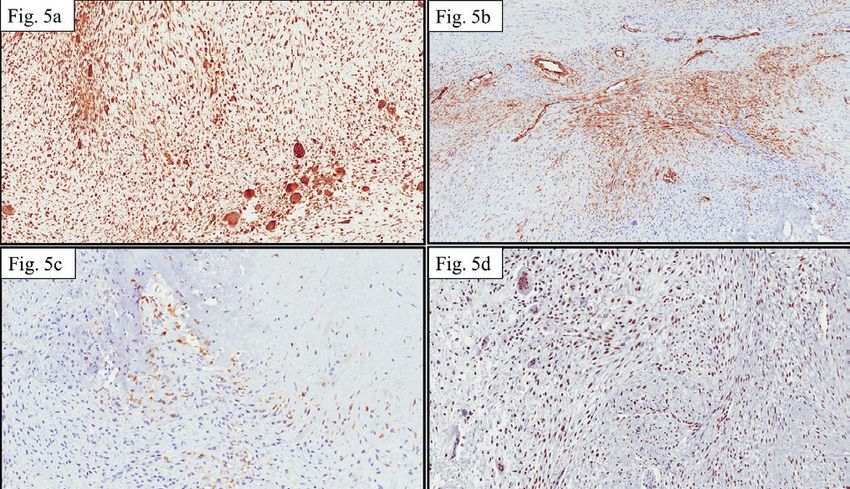
Updated information for Authors
including editorial standards
for the preparation of manuscripts
Pathologica is intended to provide a medium for the communication of A concise title; a set of key words (no more than 5); the names of the
results and ideas in the field of morphological research on human diseases authors and the institution or organisation to which each author is
in general and on human pathology in particular. affiliated; the category under which the authors intend the work to be
The journal welcomes contributions concerned with experimental published (although the final decision here rests with the Editor-in- Chief);
morphology, ultrastructural research, immunocytochemical analysis, and the name, mailing address, and telephone and fax numbers of the
and molecular biology. Reports of work in other fields relevant to the author to whom correspondence and the galley proofs should be sent.
understanding of human pathology may be submitted as well all papers on The second page should contain the abstract. At the end of the text
the application of new methods and techniques in pathology. The official should appear the bibliography, the legends to the tables and figures, and
language of the journal is Italian. Articles from foreign authors will be specification (where applicable) of the congress at which all or part of the
published in English. data in the paper may have already been presented.
Authors are invited to submit manuscripts according to the Tables
instructions outlined below: Must be limited in number (the same data should not be presented twice, in both
by mail addressed to: the text and tables), typewritten one to a page, and numbered consecutively
Pathologica – pathologica@pacinieditore.it with Roman numbers. In the text and legend of the tables, Authors must use,
The manuscript must have the following enclosures: in the exact order, the following symbols: *, †, ‡, ¶, **, ††, ‡‡ …
1) The manuscript must be submitted by e-mail to the address: Figures
pathologica@pacinieditore.it Send pictures in separate files from text and tables.
The files containing the article, illustrations and tables must be sent in - Software and format: preferably send images in .TIFF or .JPEG format,
attachment and the statements of the Authors indicated at the previous resolution at least 300 dpi (100 x 150 mm). Will not be accepted for
points 2 and 3 must also be enclosed or sent by air mail. publication manuscript with images of bad quality.
2) A separate covering letter, signed by every Author, must state that the The references must be limited to the most essential and relevant
material submitted has not been previously published, and is not under citations, identified in the text by Arabic numbers and listed at the end
consideration (in whole or in part) elsewhere, and that it is conform with of the manuscript in the order in which they are cited. The format of the
the regulations currently in force regarding research ethics. The Authors references in the bibliography section should conform with the examples
are solely responsible for the statements made in their paper, and must provided in N Engl J Med 1997;336:309-15. The first six Authors must
state that they have obtained the informed consent of patients for their be indicated, followed by et al. Journals should be cited according to the
participation in the experiments and for the reproduction of photographs. abbreviations reported on Index Medicus.
For studies performed on laboratory animals, the authors must state that Examples of the correct format for bibliographic citations:
the relevant national laws or institutional guidelines have been adhered to. Journal articles: Jones SJ, Boyede A. Some morphological observations
Only papers that have been prepared in strict conformity with the editorial on osteoclasts. Cell Tissue Res 1977;185:387-97.
norms outlined herein will be considered for publication. Their eventual Books: Taussig MJ. Processes in pathology and microbiology. Oxford:
acceptance is conditional upon a critical assessment by experts in the field, Blackwell 1984.
the implementation of any changes requested, and the final decision of the Chapters from books: Vaughan MK. Pineal peptides: an overview. In
Editor-in-Chief. Reiter RJ (ed.). The pineal gland. New York: Raven 1984:39-81.
3) Conflict of Interests. in the letter accompanying the article, Authors Acknowledgements and information on grants or any other forms of
must declare if they got funds, or other forms of personal or institutional financial support must be cited at the end of the references.
financing – or even if they are under contract – from Companies whose Notes to the text, indicated by an asterisk or similar symbol, should be
products are mentioned in the article. This declaration will be treated by shown at the bottom of the page.
the Editor-in-Chief as confidential, and will not be sent to the referees. Mathematical terms, formulae, abbreviations, units and measures
Accepted works will be published accompanied by a suitable declaration, should conform to the standards set out in Science 1954;120:1078.
stating the source and nature of the financing. Drugs should be referred to by their chemical name; the commercial name
Editorial standards for the preparation of manuscripts: should be used only when absolutely unavoidable (capitalizing the first
Pathologica will accept for publication only manuscript in English. letter of the product name and giving the name of the pharmaceutical firm
The article, in English, should be written in Microsoft Word™ preferably, manufacturing the drug, town and country).
saving files in .RTF, .DOC or .DOCX format. Any other programme can The editorial office accepts only papers that have been prepared in strict
be used, including open source programmes: please always save files in conformity with the general and specific editorial norms for each survey.
.RTF, .DOC or .DOCX format. The acceptance of the papers is subject to a critical revision by experts in
Do not use, under any circumstances, graphical layout programmes such the field, to the implementation of any changes requested, and to the final
as Publisher™, Pacemaker™, Quark X-press™, Adobe Indesign™. Do decision of the Editor in Chief.
not format the text in any way (avoid styles, borders, shading …); use only The Authors are required to correct and return (within 3 days of their
character styles such as italics, bold, underlined. mailing) only the first set of galley proofs of their paper.
Do not send the text in PDF. Authors may order reprints, at the moment they return the corrected proofs
Text and individual tables must be stored in separate files. by filling in the reprint order form enclosed with the proofs.
The article must include:
(1) a title (in English); The Publisher remains at the complete disposal of those with rights whom
(2) an abstract (in English); it was impossible to contact, and for any omissions.
(3) a set of key words (in English);
(4) titles and legends for all of the tables and figures. Journal registered at “Registro pubblico degli Operatori della
The Authors are required to correct and return (within 48 hours of their Comunicazione” (Pacini Editore srl registration n. 6269 - 29/8/2001).
being sent) the first set of galley proofs of their paper.
On the first page of the manuscript should appear: Published by Pacini Editore, Pisa, Italy - December 2018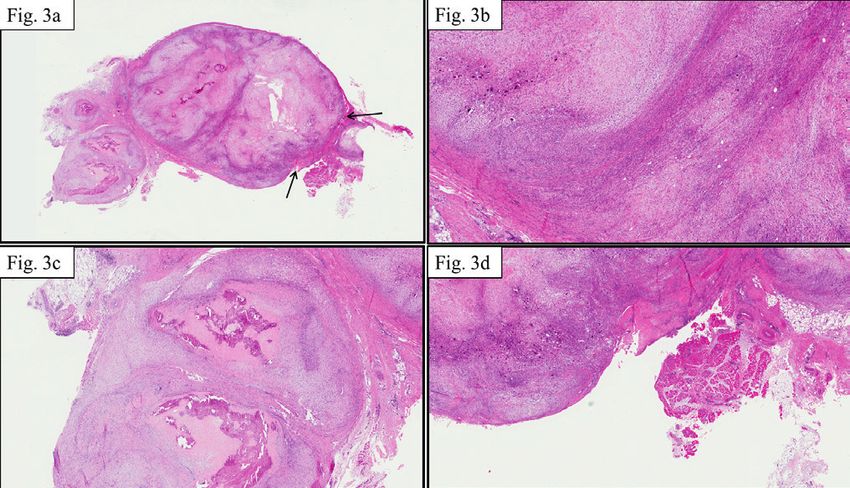
CONTENTS
Review
Glomus coccygeum: a review
M. Bisceglia, S. Bisceglia, C. Ciampi, G. Panniello, C. Galliani......................................................................................................... 287
Original article
Detection and genotyping of hpv-dna through different types of diagnostic platforms in
liquid-based cervical-cytology samples
B. Cassani, G. Soldano, D. Finocchiaro, S. Conti, A. Bulfamante, G. Lemorini, G. Bulfamante..................................................... 294
Case reports
Unclassified sex cord/gonadal stromal testis tumor with a “pure” spindle cell component: a
case report
C. Spairani, S. Squillaci, A. Pitino, F. Montefiore, W. Fusco.............................................................................................................. 302
Calcifying aponeurotic fibroma: a core biopsy-based diagnosis
F. Motta, S. Scavo, G.M. Vecchio, G. Fuccio-Sanzà, F. Nicolosi, G. Magro....................................................................................... 307
Lymphnode metastasis of thyroid cancer misinterpreted as lateral aberrant thyroid 40 years
before identification of primary tumor. Case report and review of the literature
G. Riva, M. Villanova, G. Francia, G. Valotto, L. Mezzetto, M. Toaiari, A. Eccher, L. Novelli........................................................ 313
Pathologica storica
Pathologica ai tempi della Spagnola
C. Patriarca, C.A. Clerici........................................................................................................................................................................ 316
Proceedings
IV Meeting Nazionale Gruppo Italiano Paleopatologia................................................................................ 321
Front cover: Core biopsy specimen. (A) Low magnification of the fragments. (B) Area composed of plump spindle- to
focally stellate-shaped cells. Mitoses and necrosis were absent. (C) Hypocellular tumor area with a dense fibrous stroma.
(D) Multinucleated osteoclastic-like giant cells are intermingling with the spindle cells; microcalcifications (arrows) were
scattered throughout the fibrous stroma (page 309).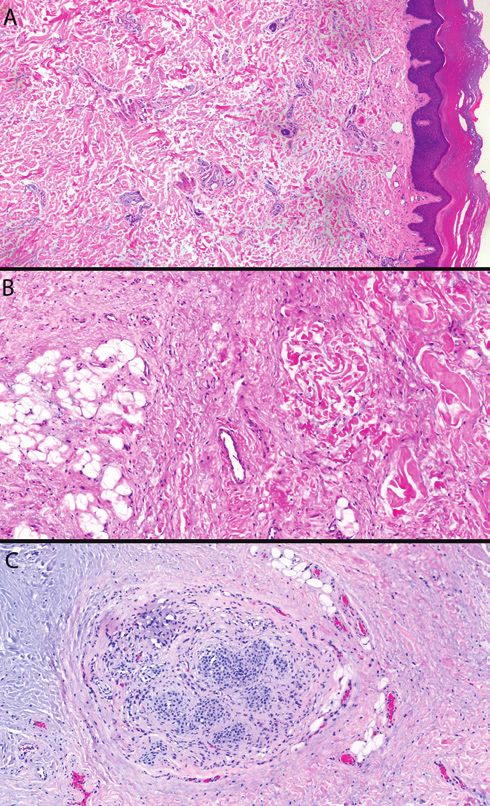
PATHOLOGICA 2018;110:287-293
Review
Glomus coccygeum: a review
M. BISCEGLIA1, S. BISCEGLIA2, C. CIAMPI2, G. PANNIELLO3, C. GALLIANI4
Anatomic Pathology, School of Biomedical Sciences, Etromapmacs Pole, Lesina (FG), Italy;
1
2
Polyclinic of Modena, Modena, Italy; 3 Unit of Clinical Dermatology, Polyclinic “Ospedali Riuniti” di Foggia, Italy;4 Department of
Pathology, Children’s Minnesota, Minneapolis & St. Paul, MN, USA
Key words
Glomus coccygeum • Sucquet-Hoyer canals • Arterio-venous anastomosis • Glomus tumor • Coccygodinia
Summary
With limited information about the coccygeal glomus found in pilonidal disease specimens. Familiarization with its microana-
classic textbooks, we deemed it necessary to review the subject. tomical features may help to avoid inappropriate interpretation of
The illustrations presented in this article derive from four coc- this enigmatic structure.
cygeal glomera incidentally encountered during examination of
Introduction hood. In the elderly, the glomera regress, sclerose, and
diminish in number, thus explaining the increase suscep-
A glomus body is a spheroidal to ovoid dermal micro- tibility to thermoregulatory disturbances affecting the
anatomical structure that constitutes an arteriovenular extremes of life 1.
glomeriformis anastomosis. Each glomus consists of Glomera are frequently encountered in the hands and
one or more arterial segments that branch into a num- feet, chiefly in the deep dermis of the digital pads and
ber of glomic arterioles surrounded by rows of round, nail beds, but they also occur in the ears, nasal and ali-
uniform, epithelioid contractile cells, that drain into a mentary mucosa (where the function is related to ab-
collecting venous plexus 1. These sphincteric anastomo- sorption), thyroid, erectile tissue, and many other sites
ses, the essential parts of the glomus, are eponymously including the coccygeal region 1.
known as the Sucquet-Hoyer canals after J.P. Sucquet In 1860, Hubert von Luschka (1820-1875), a German
(1840-1870), a French anatomist, and H. Hoyer (1864- surgeon and anatomist, first identified the glomus coc-
1947), a Polish anatomist, who first described them. cygeum at the ventral tip of the coccyx in his dissection
Endowed with a high-sympathetic tone, the glomus body studies of the pelvis, naming it “glandula coccygea” 4.
is involved in skin thermoregulation acting as a sphincter Luschka compared glomus coccygeum with the carotid
to control the flow of blood by locally mediated axon body (“glomus caroticum”), a chemoreceptor, thinking
reflex responses, to bypass or enable the capillary bed, that both were glands. In 1865, the Swiss-born Julius Ar-
and prevent loss or dissipate heat. nold (1835-1915) described the “glandulae coccygeae”
Knowledge of the function of cutaneous arteriovenous even on the ventral surface of sacrum, recognizing their
anastomoses in man dates back to the early 1930s when vascular origin along the median sacral artery, and nam-
the work 2 of the British physiologists and cardiologists ing them “glomeruli arteriosi coccigei” 5. He considered
Thomas Lewis (1881-1945) and George W. Pickering both glomus coccygeum and “glomus” caroticum as
(1904-1980) as well as the work 3 of the British cardiolo- true glomeruli 6. In 1902, these microanatomical struc-
gist Ronald T. Grant (1892-1989) and the American car- tures were included in the paraganglion system 7 by the
diologist Edward F. Bland (1901-1992) were published. Austrian histologist Alfred Kohn (1867-1959). In 1907,
These arteriovenous anastomoses are scarce in the new- the non-paraganglionic (non-chromaffin) nature of the
born, but develop rapidly during infancy and early child- glomus coccygeum was demonstrated histochemically 8
Correspondence
Michele Bisceglia, via Santa Chiara 9, 71043 Manfredonia (FG),
Italy - Tel. +39 0884 587546 - E-mail: bismich@alice.it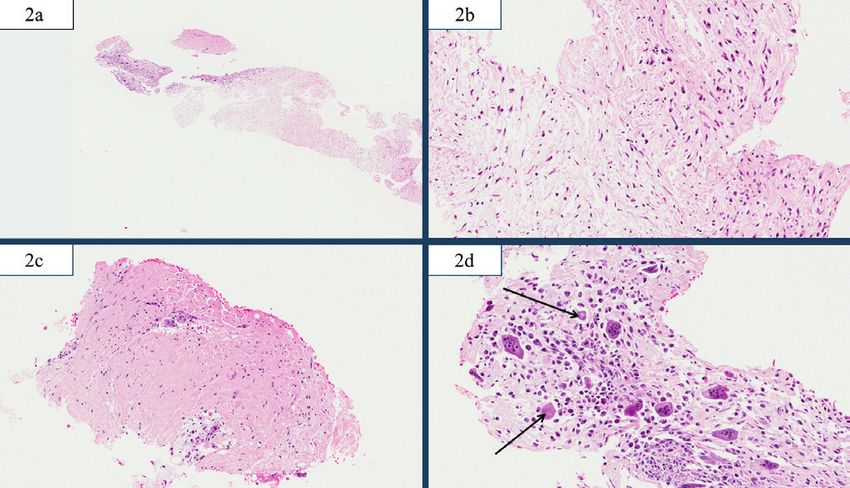
288 M. BISCEGLIA ET AL.
by another Austrian Mediziner, the anatomic patholo- Fig. 1. Scanning view of skin and subcutaneous tissue from
gist Oskar Stoerk (1870-1926). However, credit is due to the sacroccygeal region of a surgical specimen in a 25-year-old
William H. Hollinshead (1906-1986), an American anat- woman with pilonidal cyst. Top and center: Natal cleft and cu-
omist, who in 1942 categorically established anatomi- taneous sinus tract, typical of mostly inactive pilonidal disease,
and a 1 mm glomus coccygeum (arrow) with associated vein lying
cal and physiological distinctions between the “glomus” just under the apex of the sinus. Inset: the glomus coccygeum at
coccygeum and “glomus” caroticum (carotid body) 9. higher magnification.
Several terms have been used in the past, referring to
the same glomus coccygeum, such as coccygeal body,
glomus coccygicum, pericoccygeal glomus, Luschka’s
body, gland of Luschka, coccygeal gland, and “glandula
coccygea”.
Glomus coccygeum is homologous to the “caudal glom-
eruli” (also called “glomerula caudalia”), which are
non-nutrient arteriovenous anastomoses present in vari-
able number (up to 15) – according to species – in tailed
mammals, from rodents to monkeys 9-16. However, while
there is evidence that caudal arteriovenous anastomoses
in animals play an important role in thermoregulation 15-
17
, glomus coccygeum in humans (and in other tailless
primates as well) represents a phylogenetic vestigial
rest, that is an atavic organ loosing the normal thermo-
regulatory function as the dermal glomera of other sites.
In fact, the subcutaneous panniculus, where the glomus
coccygeum resides, serves as an insulator, not as a dis-
sipator or absorber of heat.
However, the precise function of this structure in humans
remains speculative 18. A presumptive hematopoietic
function via an immunomodulatory activity of the sym-
pathetic nervous system has been recently proposed 19.
There is limited data, if any, regarding glomus coccyge-
um in classic textbooks of anatomy and physiology, and The prevalence of glomus coccygeum is uncertain. Its
therefore in this article we review the world literature on presence was nearly constantly documented in three
the subject. anatomic autopsy studies as it was found by different
investigators in 5 out of 5 28, in 29 of 32 26, and in 17
of 20 24 coccygectomy specimens either from adults 28,
Anatomic and clinical findings elderly 26, or individuals of pediatric and adult ages 24.
Instead, in anatomic studies of specimens submitted for
There is no recorded evidence of this type of arteriove-
surgical pathology, glomus coccygeum was identified in
nous shunt in fetuses between 10-18 weeks-gestation,
when a presumptive anlage for the coccygeal body may 13 of 40 (32.5%) coccygectomy specimens resected in
be an arterial plexus derived from a tortuos median sacral individuals with coccygodinia 25 and in 18 of 37 (48.6%)
artery admixed with nerve fibers and sympathetic gan- coccygeal bones removed during rectal resection for
glion cells 20. However, well-formed coccygeal glom- advanced rectal and uterine carcinomas and for various
era have been observed for decades in previable fetuses other reasons 27.
(145-170 mm crown rump length) 21. As a normal structure, the coccygeal body is inapparent.
Postnatally, the glomus coccygeum lies deeply buried in In five cases of coccygodynia which had been ascribed
the adipose tissue immediately below or just ventral to to pericoccygeal glomus tumors 29-32, which were most
the tip of the coccyx, near the center of the natal cleft, likely normal coccygeal glomera, the symptomatology
in the vicinity of the anococcygeal ligament, between subsided after coccygectomy, but in 3 cases there were
the branches of the median sacral artery and vein, inner- radiographic abnormalities of the coccyx or intraopera-
vated by the pelvic sympathetic plexus 18-20 22-26 (Fig. 1). tively proven fractures. And there are large series of pa-
Glomus coccygeum, which is endowed of up to 4 arte- tients treated with coccygectomy for both traumatic and
rial segments may be either single 22, binodal, or mul- idiopathic coccygodynia in which no remarkable features
tiple 24 27, or present as a network of glomus bodies in the involving glomus coccygeum were encountered in most
coccygeal region 12 24, with a few of them occasionally of the cases, except for histological degenerate changes in
located even in coccygeal vertebrae 24 25. the sacrococcygeal or intercoccygeal discs in some 25 32 34.
It is one of the largest glomera in humans 18 25, measuring In clinical practice glomus coccygeum is usually an
between 1 and 5 mm (mean diameter: 3.5 mm in a large incidental finding in excised specimens from sacrococ-
study) 22 25. cygeal areas for diverse causes, such as pilonidal dis-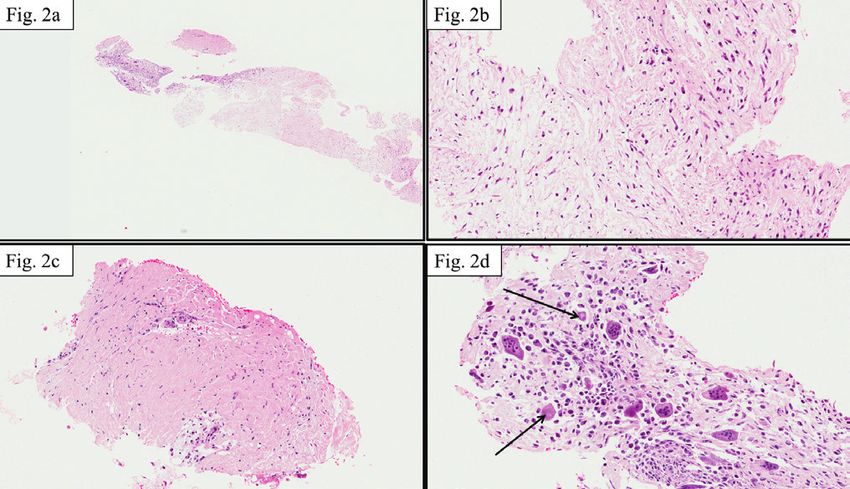
GLOMUS COCCYGEUM: A REVIEW 289
ease 35-39, coccygeal dimple 40, coccygeal pad 41 42, myxo- body in general are immunoreactive for vimentin, col-
papillary ependymoma 43, tailgut cyst 44, sacrococcygeal lagen type IV (external basal lamina), muscle specific
teratoma 45, as well as in surgical specimens from coccy- actin, and alpha-smooth muscle actin (Fig. 2B), and
gectomies for idiopathic or secondary coccygodinia 27 29- negative for epithelial markers, EMA, endothelial mark-
32
, and in perirectal resections including coccyx for rectal ers (CD31 and FVIII-RA), and neuroendocrine mark-
or advanced uterine cancers 27. Two cases were observed ers, such as chromogranin and synaptophysin, with low
in infants, in surgical resection specimens performed for proliferative activity 25-27 36 38 39. Conflicting findings have
pilonidal sinus 37 in a case, including the apex of coccyx, been reported for neuron specific enolase (mostly posi-
and for coccygeal dimple 40 in the other one, respectively. tive), desmin, and S-100 protein (mostly negative) 25.
Of interest, in a study based on archival pathology ma- CD34 was expressed in 3 cases, focally in 2 38, and dif-
terial, glomus coccygeum was found in only 2 cases fusely in one 32.
among 382 pilonidal sinus excision specimens 38. Ultrastructurally, pericellular external lamina, subplas-
We incidentally observed several cases of glomus coc- malemmal vesicles, bundles of actin microfilaments,
cygeum during examinations of surgical specimens ex- groups of membrane bound organelles including mito-
cised for pilonidal disease as well as for other causes chondria and endoplasmic reticulum can be seen in glo-
(see illustrations), and the pictures herein presented are mus cells, but no membrane bound endocrine granules
from 5 such coccygeal bodies found in 4 young and one have ever been observed 27 31 46.
elderly individuals.
Histological differential diagnosis
Histological features
In a compilation of tumoral and pseudotumoral entities
Glomus coccygeum may exhibit a well-circumscribed of the soft tissues that surfaced over the preceding quar-
or multinodular appearance, mainly comprised of small ter of a century published in 2006, two of the authors
arterioles surrounded by a mantle of epithelioid myoid (MB; CAG) made reference to the potential pitfall for
cells, rich of unmyelinated nerve fibres and embedded the “glomus coccygeum of Luschka” 47.
in loose to dense fibrous connective tissue. In fact, because of its considerable size and multiple anas-
Due to the variable proportion of the constitutive ele- tomotic channels, coccygeal glomus mimics glomus tu-
ments of the glomus body, some authors distinguish the mor, that is a tumor mostly occuring in distal extremities
following variants: the glomus cell nodule-dominant which was firstly described in 1924 48 by the French-born,
type, an intermediate mixed morphology with a mixture Canadian, histopathologist Pierre Masson (1880-1959).
of nodules and vessels, and the vascular-dominant type As a matter of facts, P. Masson applied it the name “glo-
with scattered individual glomic cells 26 (Figs. 2-6). mus” (“neuromyoarterial glomus tumor”, also called “ar-
terial angioneuromyoma”) 48 to depict its similarity to the
glomus coccygeum of Luschka, hence the term glomus
Immunohistochemistry and electron tumor has occasionally been used synonymymously (but
microscopy erroneously) to refer to a normal glomus coccygeum 37.
Parenthetically, glomus tumor was also alternatively
Immunohistochemically, the glomic cells of the glomus named “glomangioma” in 1935 by the American pa-
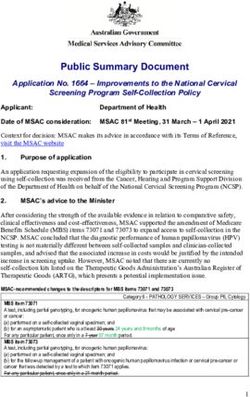
Fig. 2. Glomus coccygeum of the so-called “glomus cell nodule-dominant type” (same case as Fig.1). (A) A well circumscribed, unencapsu-
lated glomus body with densely packed clusters of glomic cells, embedded in fibrous connective tissue. While some cell aggregates exhibit
slit-like lumina lined by flattened endothelial cells, others are seemingly devoid of vascular lumina. (B) Immunoperoxidase for smooth
muscle actin highlighting the glomus cells that surround vessels of the Sucquet-Hoyer canals.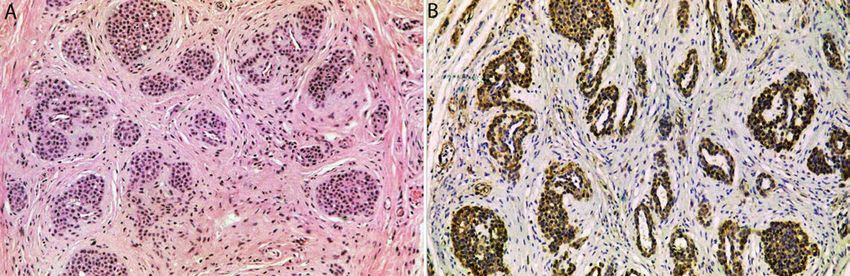
290 M. BISCEGLIA ET AL.
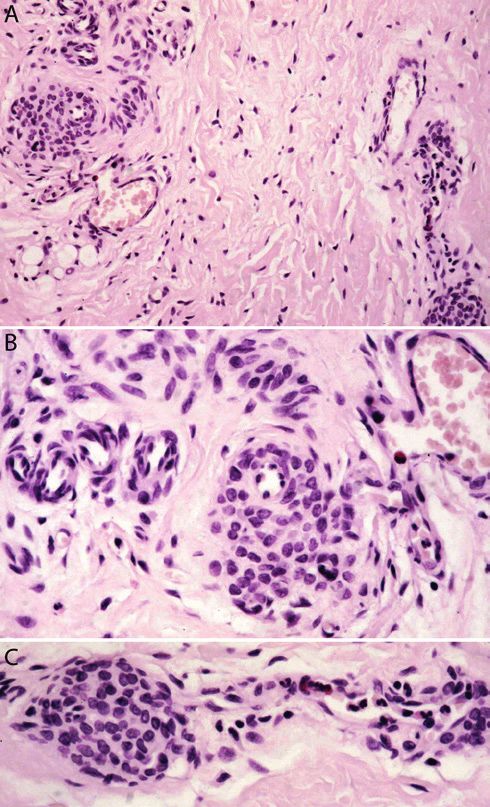
Fig. 3. Glomus coccygeum of the so-called “vascular-dominant type with scattered individual glomic cells”, in a 28-year-old man with pilo-
nidal cyst. (A) The glomus coccygeum is seen at the level of its arterial pole with branches of the Sucquet-Hoyer canals. The media of the
arterioles show in this case a poorly development of the epithelioid cell component. (B) Higher magnification. Several unmyelinated nerve
fibres are in the immediate vicinity of arterioles and glomic cells.
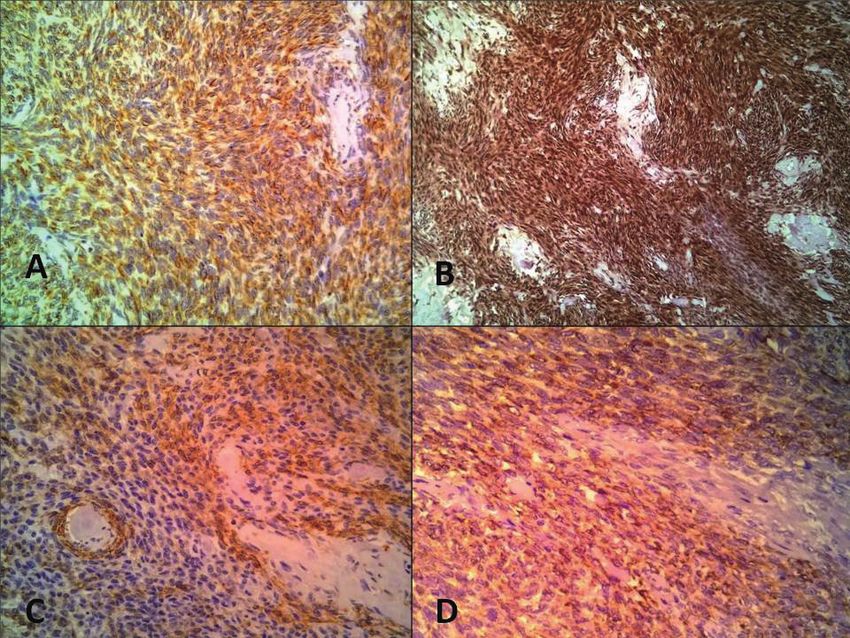
Fig. 4. Glomus coccygeum of the so-called “intermediate mixed type (nodular and vascular)”, in a 15-year-old girl with pilonidal cyst. (A) Low
power view of a binodal variant of glomus coccygeum with central draining veins. (B) Higher magnification of the lower left-sided part of
the glomus.
thologist Orville T. Bailey (1909-1998), who believed it coccygeal benign glomus tumors have been reportd so
represented a subgroup of (hem)angiomas 49. far in the literature: 2 of the 3 cases by Nutz and Stel-
Importantly, glomus coccygeum may be easily misin- zner 51, and the cases by Llombart et al. 53 and Kim et
terpreted as a coccygeal glomus tumor by the unwary al. 54. These tumors, which were clinically a “palpable
histopathologist, and in fact a series of glomus coccy- lesion”, and of 1 to 2 cm in size, exhibited the same
geal tumors, presumed to be normal coccygeal glomera, morphologic features of glomus tumors occurring in the
have been reported by several authors 29 30 31 50 51 [1 of the 3 usual extracoccygeal sites. Benign glomus tumors are
cases reported in the last reference of the ones quoted herein]
. Bell and collabo- expansile lesions, which cause the classic triad of pain,
rators first exposed the potential for confusion 28, and tenderness, and cold sensitivity, sometimes eroding the
Albrecht and Zbieranowski emphasized the risk of this adjacent bone surface.
misinterpretation 35. No additional coccygeal glomus tu- There is no record of inherited glomus vascular malfor-
mors have been published since, and subsequent publi- mations, malignant glomus tumor, or glomus tumors of
cations all warned against misdiagnosis and overdiagno- uncertain biologic behaviour involving the glomus coc-
sis of this normal microanatomical structure 27 36 38 39 43 52. cygeum.
Therefore, it seems that the glomus body in this specific Extracoccygeal glomus vascular malformation or glo-
location is not particularly susceptible to neoplastic muvenous malformation (multiple “familial glomangio-
transformation. mas”) are either localized (glomangiomatosis) or wide-
However, although any coccygeal glomus tumor should spread, with an autosomal dominant pattern of inheri-
be viewed with scepticism, 4 cases of solitary “true” tance 55 56.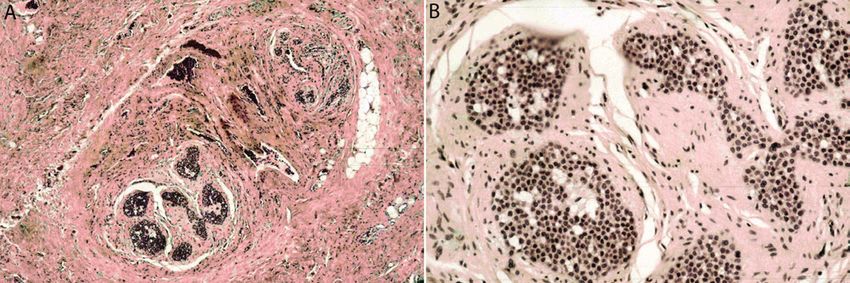
GLOMUS COCCYGEUM: A REVIEW 291 Fig. 5. Glomus coccygeum of the “intermediate mixed type”, Fig. 6. Glomus coccygeum in a 19-year-old male with trisomy 21, buried within dense fibrous connective tissue. This is an inciden- who presented with a longstanding, gradually enlarging “mass” tal finding from a carcinoma of the lower rectum specimen of in the intergluteal (natal) cleft region, clinically felt to be quies- a 74-year-old man. (A) Sucquet-Hoyer canals with collarettes of cent pilonidal disease, but histologically diagnosed as coccygeal glomic cells, emptying in thin-walled venous channels. (B) Mag- pad (juvenile coccygeal fibrosis). (A) Skin showing orthokeratotic nification of the left section in “A” detailing a glomus arteriole epidermis and massively expanded dermis with haphazardly ori- and its relevant capaceous thin-walled venule. (C) Magnification ented, variably thick collagen bundles. (B) Deep dermis with in- of the right section in “A” featuring a longitudinally oriented Suc- creased dermal mucin, and fibrotic subcutaneous tissue. (C) Bur- quet-Hoyer canal, connecting a spheroid of epithelioid contrac- ied in a collagenous matrix is a glomus coccygeum of the “glo- tile cells in the media of an arteriole of the glomus body with its mus cell nodule-dominant type”, incidentally found very close to relevant venule (visible in “A”). the deep margin of resection. Generally, malignant glomus tumors 55 are deeply seated, Intradermal melanocytic nevus is less organoid and im- measure 2 cm, exhibit atypical mitotic figures, moderate munohistochemically is strongly positive for S-100 pro- to high nuclear grade, and at least 5 mitotic figures/50 tein and negative for alpha-smooth-muscle actin. high power fields. Glomus tumors of uncertain biologic Paraganglioma (paraganglioma of the filum terminale behaviour 57 exhibit high-mitotic activity and are super- might be in point) is a tumor arising from the paragan- ficially located, or of large size only, or deep seated only. glion system. If carefully examined, it looks morpho- No histological variants of glomus tumors, either with logically different, is positive for argyrophilic stains and oncocytic features 58 or symplastic high grade nuclei 57, immunoreactive for neuroendocrine markers, and shows have been reported in the coccygeal region. typical neuroendocrine granules when ultrastructurally Other entities which may possibly enter the differential examined. Although the glomus coccygeum is not related diagnosis with normal glomus coccygeum are the fol- to the paraganglia, with which it may be confused, we lowing: intradermal melanocytic nevus, paraganglion would like to alert the reader about the incorrect use, in and paraganglioma, neuroendocrine tumor, adnexal skin the older literature 59 as well as among clinicians of some tumor, and metastatic carcinoma. discipline even today, of the name “glomus” for other dif-
292 M. BISCEGLIA ET AL.
ferent microanatomical chemoreceptorial structures of the 12
Staubesand J. Der Feinbau des Glomus coccygeum und der Glo-
paraganglion system (glomus caroticum, glomus jugu- merula caudalia. Acta Anat 1953;19:105-31, 209-32, 309-344.
lare, glomus tympanicum, …), which erroneously glomus 13
Kondo H. An electron microscopic study on the caudal glomerulus
coccygeum one and a half century ago was ascribed to. of the rat. J Anat 1972;113:341-58.
Adnexal skin tumors (mainly eccrine acrospiroma), neu- 14
Wright PG. Observations on the anatomy of the tail in the vervet
roendocrine tumors, and metastatic carcinomas have dif- monkey, Cercopithecus, which bear on thermoregulatory function in
the organ (Primata: Cercopithecidae). Zool Afr 1977;12:475-83.
ferent morphologies and can be easily excluded with the 15
Wright PG. A counter-current heat exchange system in the tail of
support of immunohistochemistry, mainly evidencing the vervet monkey, Cercopithecus pygerythrus (Primata: Cercopi-
their consistent cytokeratin immunoreactivity. thecidae). Zool Afr 1977;12:485-95.
16
Vanhoutte G, Verhoye M, Raman E, et al. In-vivo non-invasive
study of the thermoregulatory function of the blood vessels in the
Conclusions rat tail using magnetic resonance angiography. NMR Biomed
2002;15:263-9.
17
Owens NC, Ootsuka Y, Kanosue K, et al. Thermoregulatory
Take-home-messages: control of sympathetic fibres supplying the rat’s tail. J Physiol
-- It is surprising how little attention is devoted to glo- 2002;543:849-58.
mus coccygeum in standard textbooks of human
18
Woon JT, Stringer MD. Clinical anatomy of the coccyx: a system-
atic review. Clin Anat 2012;25:158-67.
anatomy and histology.
-- It is a normal, likely phylogenetic vestigial anatomi-
19
Conti A, Maestroni GJ, Cosentino M, et al. Evidence for a neu-
roimmunomodulatory and a hematopoietic role of the Luschka’s
cal structure with similar cytoarchitectural constitu- coccygeal body. Neuro Endocrinol Lett 2000;21:391-403.
ents as the dermal Sucquet-Hoyer canals. 20
Jin ZW, Cho KH, Jang HS, et al. Median sacral artery, sympathetic
-- Its functional significance is uncertain, even enig- nerves, and the coccygeal body: a study using serial sections of hu-
matic, given its ectopic location in the hypodermis. man embryos and fetuses. Anat Rec (Hoboken) 2016;299:819-27.
-- Its constituents seem to be disinclined to pathologi- 21
Krompecher, S. Histologische und entwicklungsgeschichtliche
cal alterations such as hyperplastic and neoplastic Untersuchungen uber das Glomus coccygeum des Menschen. Ver-
proliferation. handl D Anat Gesellsch 1932;41:176-85.
-- In summary, familiarization with this seldom ob- 22
Di Marino V, Bonnoit J, Bonneau HP, et al. Anatomical studies of
served microanatomical structure of the coccygeal Luschka’s gland. Bull Assoc Anat 1975;59:391-7.
region is necessary to avoid overinterpretation as a 23
Lack EE. Glomus coccygeum. In: Sternberg SS, ed. Diagnostic
pathological one. surgical pathology. New York, NY: Raven Press 1994, p. 617.
24
Albrecht S, Hicks MJ, Antalffy B. Intracoccygeal and pericoccy-
geal glomus bodies and their relationship to coccygodynia. Sur-
References gery 1994;115:1-6.
25
Maggiani F, Kashima T, Ostlere SJ, et al. Immunophenotypic anal-
1
Standring S. Gray’s Anatomy - The anatomical basis of clinical ysis of glomus coccygeum associated with coccygodynia. Skeletal
practice. 40th ed. London (UK): Churchill Livingstone Elsevier Radiol 2011;40:1455-9.
(Ch.6) 2008, pp. 134-135. 26
Jin ZW, Cho KH, Jang HS, et al. Coccygeal body revisited: an
2
Lewis T, Pickering GW. Vasodilatation in the limbs in response immunohistochemical study using donated elderly cadavers. Anat
to warming the body, with evidence for sympathetic vasodilator Rec (Hoboken) 2017;300:1826-37.
nerves in man. Heart 1931;16:33-51. 27
Gatalica Z, Wang L, Lucio ET, et al. Glomus coccygeum in sur-
3
Grant RT, Bland EF. Observations on arteriovenous anastomoses gical pathology specimens: small troublemaker. Arch Pathol Lab
in human skin and in the bird’s foot with special reference to the Med 1999;123:905-8.
reaction to cold. Heart 1931;15:385-407. 28
Bell RS, Goodman SB, Fornasier VL. Coccygeal glomus tumors: a
4
Luschka H. Die Steissdruse des Menschen. Virchow Archiv case of mistaken identity? J Bone Joint Surg Am 1982;64:595-7.
1860;18:106-18. 29
Ho KL, Pak MSY. Glomus tumor of coccygeal region. Case report.
5
Arnold J. Ein Beitrag zu der Structur der sogenannten Steiss- J Bone Joint Surg 1980:62A:141-2.
drüsse. Virch Arch Pathol Anat 1865;32:293-331. 30
Pambakian H, Smith MA. Glomus tumor of the coccygeal body as-
6
Arnold J. Ueber die Struktur des Ganglion intercaroticum. Virch sociated with coccydynia. A preliminary report. J Bone Joint Surg
Arch Path Anat 1865;33:190-209. Br1981;63-B:424-6.
7
Kohn A. Das chromaffine Gewebe. Ergebn Anat Entw 1902;12:253- 31
Duncan L, Halverson J, De Schriver-Kecskemeti K. Glomus tumor
348. of the coccyx. A curable cause of coccygodynia. Arch Pathol Med
8
Stoerk O. Über die Chromreaktion der Glandula coccygea und die 1991;115:78-80.
Beziehungen dieser Driise zum Nervus sympathicus. Arch F Mikr 32
Urban Ramón A, Amela AD, Sanmartin Cabrera X, et al. Present-
Anat 1907;69:322-39. ación de un caso de glomus coccígeo: consideración y valoración
9
Hollinshead WH. A comparative study of the glomus coccygeum histológica. Rev Esp Patol 2011;44:216-9.
and the carotid body. Anat Rec 1942;84:1-16. 33
Pennekamp PH, Kraft CN, Stutz A, et al. Coccygectomy for coc-
10
Arnold J. Über die Glomeruli caudales der Säugethiere. Virchows cygodynia: does pathogenesis matter? J Trauma 2005;59:1414-9.
Arch 1867;36:497-520. 34
Balain B, Eisenstein SM, Alo GO, et al. Coccygectomy for coccy-
11
von Schumacher S. Über das Glomus coccygeum des Menschen dinia: case series and review of literature. Spine (Phila Pa 1976)
und die Glomeruli caudales der Säugetiere. Arch Mikr Anat 2006;31:E414-20.
1908;71:58-115. 35
Albrecht S, Zbieranowski I. Incidental glomus coccygeum.GLOMUS COCCYGEUM: A REVIEW 293
When a normal structure looks like a tumor. Am J Surg Pathol sue: new entities and new variants of old entities recorded during
1990;14:922-4. the last 25 years. Part XII: appendix. Pathologica 2006;98:239-98.
36
Bisceglia M, Zaffarano L, Clemente C. Glomo coccigeo inciden- 48
Masson P. Le glomus neuromyo-artérial des régions tactiles et ses
tale: una normale struttura che simula un tumore. G Ital Dermatol tumeurs. Lyon Chir 1924;21:257-80.
Venereol 1999;134(Suppl 2):148-9.
49
Bailey OT. The cutaneous glomus and its tumors - glomangiomas.
37
Méndez-Gallart R, Gómez Tellado M, Somoza Argibay I, et al. Tu-
Am J Pathol 1935;11:915-35.
mor glómico en la región coccígea (glomus coccygeum) en edad
pediátrica. Cirugía Española 2001;70:251-2. 50
Weiss SW, Goldblum JR. Enzinger and Weiss’s soft tissue tumors.
38
Santos LD, Chow C, Kennerson AR. Glomus coccygeum may mim- 4th ed. St. Louis: Mosby 2001, p. 985.
ic glomus tumour. Pathology 2002;34:339-43. 51
Nutz V, Stelzner F. Glomus tumor as a cause of coccygodynia.
39
Rahemtullah A, Szyfelbein K, Zembowicz A. Glomus Chirurg 1985;56:243-6.
coccygeum:report of a case and review of the literature. Am J Der- 52
John I, Rao UNM. An unusual normal finding in coccygectomy
matopathol 2005;27:497-9.
specimens. Int J Surg Pathol 2017;25:700-1.
40
Park CK, Hong EK, Kim NH. Incidental glomus coccygeum as-
sociated with coccygeal dimple. Korean J Pathol 1993;27:198-9.
53
Llombart A, Lopez-Fernandez A, Peydro A. Glomangiome neu-
ropérycitarie de localisation coccygienne. Ann Anat Pathol
41
Hashimoto I, Shono Y, Ishida S, et al. Developmental mechanism
1969;14:327-34.
of juvenile coccygeal fibrosis (so-called coccygeal pad). J Derma-
tol 2013;40:832-6. 54
Kim HS, Yang SH, Park HJ, et al. Glomus tumor as a cause of coc-
42
Song HS, Kang HY. Sacrococcygeal nodule in a young male pa- cydynia. Skeletal Radiol 2013;42:1471-3.
tient. Ann Dermatol 2014;26:771-3. 55
Boon LM, Brouillard P, Irrthum A, et al. A gene for inherited cuta-
43
Marc’hadour FL, Pasquier B. Subcutaneous sacrococcygeal ep- neous venous anomalies (“glomangiomas”) localizes to chromo-
endymoma with incidental glomus coccygeum. Histopathology some 1p21-22. Am J Hum Genet 1999;65:125-33.
1991;18:570-2. 56
Boon LM, Mulliken JB, Enjolras O, et al. Glomuvenous malfor-
44
Kim MJ, Lee SN, Kim SS, et al. Tailgut cyst with glomus coccyg- mation (glomangioma) and venous malformation: distinct clinico-
eum: report of a case. Korean J Pathol 1996;30:643-5. pathologic and genetic entities. Arch Dermatol 2004;140:971-6.
45
Palumbo LT, Cross KR, and Paul RE. Sacrococcygeal teratoma: 57
Folpe AL, Fanburg-Smith JC, Miettinen M, et al. Atypical and ma-
review of the literature: report of case in an adult containing a
lignant glomus tumors: analysis of 52 cases, with a proposal for the
glomus. Ann Surg 1951;133:421-7.
reclassification of glomus tumors. Am J Surg Pathol 2001;25:1-12.
46
Sargon MF, Hamdi Celik H, et al. Fine structure of the human
coccygeal body: a light and electron microscopic study. Ann Anat
58
Slater DN, Cotton DWK, Azzopardi JD. Oncocytic glomus tumor:
1998;180:11-4. a new variant. Histopathology 1987;11:523-31.
47
Bisceglia M, Spagnolo D, Galliani C, et al. Tumoral, quasitumoral 59
Lagacé R, Delage C, Gagné F. Paraganglioma of the filum termi-
and pseudotumoral lesions of the superficial and somatic soft tis- nale. Can J Neurol Sci 1978;5:257-60.PATHOLOGICA 2018;110:294-301
Original article
Detection and genotyping of HPV-DNA through
different types of diagnostic platforms in liquid-based
cervical-cytology samples
B. CASSANI, G. SOLDANO, D. FINOCCHIARO, S. CONTI, A. BULFAMANTE, G. LEMORINI, G. BULFAMANTE
U.O.C. di Anatomia Patologica, Citogenetica e Patologia Molecolare, P.O. San Paolo, ASST dei Santi Paolo e Carlo, Milano, Italia;
Dipartimento di Scienze della Salute, Università degli Studi di Milano, Italia; Servizio di medicina di laboratorio per il programma di
screening lombardo del tumore della cervice uterina (D.D.G. n. 12386 del 28 novembre 2016)
Key words
Cervical cancer • HPV test • Screening
Summary
Background. At present cervical cancer represents the second GeneXpert® Infinity Systems platform (Cepheid). Every platform
most common cancer in women worldwide and it reaches a global researched high-risk HPV genotypes panels (hr-HPV). Part of the
mortality rate of 52%. Only the early detection and the adequate clinical records has also been analyzed through PCR and genes
treatment of pre-neoplastic lesions and early-stage cervical cancer L1 and E6/E7 complete sequencing, in order to further typing the
decrease the mortality rate for this type of cancer. Cervical carci- viral population.
noma screening, as a method of second prevention, is currently Results. We have examined 1284 samples of women aged 16
feasible through molecular research of high-risk HPV genotypes to 73 years: 1125 have been tested using HC2 procedure, 272
and in lots of organized screening programs the Pap-test is per- samples with Onclarity method, 159 with Xpert® method and
formed only in women with positive HPV-test. Currently, there 55 samples have been analyzed using PCR and sequencing of
are various diagnostic platforms detecting and molecular geno- gene L1 and gene E6/E7. HPV-DNA was detected with Onclar-
typing HPV, which are based on different procedures, determin- ity method in 15,07%, with Xpert® method in 13,83% and using
ing uneven viral genotypes panels and using diverse type of vials HC2 procedure in 12,27% of samples. The comparison between
to collect and store the samples. Previous studies have pointed the three molecular methods revealed diagnostic discrepancies in
out that DNA-HPV test can be negative in pre-neoplastic lesions, 3,14% of our records between Onclarity test and Xpert® method
even of high grade, or in presence of cervical cancer. Therefore, and in 2,20% (6/272) between HC2 test and Onclarity test. Glob-
it’s important to assess the risk of false negative diagnoses using ally, in 431 tests, compared using different diagnostic platforms,
DNA-HPV molecular test, because in this circumstance women discrepant diagnoses, referring to hr-HPV presence or to detected
do not undergo immediately Pap-test, but they are submitted to genotype, have been observed 11 times (2,55%). Genotype 16
second round screening with DNA-HPV test after 5 years: this appeared the most expressed in the positive samples (20,99%),
protocol could increase the incidence of “interval cancers”. The whereas genotype 18 resulted the less expressed in the examined
present study aims at comparing the results of HPV detection and population (4,94%).
genotyping on liquid based cervical cytology, using some of the Discussion. The present study highlights the following: 1) Positive
most relevant diagnostic platforms in commerce. results’ percentage for high-risk HPV-DNA genotypes, deriving
Methods. The study is based on a group of patients which went from the three diagnostic platforms used and with the same vial to
to their private gynecologist in a contest of opportunistic screen- collect and store samples, does not significantly vary on the basis
ing. The vial used in the examined population has been EASY- of the type of equipment and it is congruent with the Italian per-
PREP® preservative solution (YD Diagnostics CORP-Republic of centage already detected during organized screening programs. 2)
Korea); liquid-based cervical cytology sampling has been done Even the molecular diagnostic approach could give false negative
using a single device (plastic brush), allowing to collect simul- results, preventing the detection in the screened population of cer-
taneously cytological material from exocervix and endocervix vical HPV-related lesions and theoretically endangering women to
(Rovers® Cervex-Brush®). The diagnostic platforms employed develop “interval cancer”. 3) In the population examined, geno-
have been the following: A) Digene HC2 HPV DNA Test, on RCS type 16 has been the most expressed, whereas genotype 18 was
System (QIAGEN); B) BD Onclarity™ HPV test, on automate among the less frequently detected. Other genotypes often noticed
platform BD Viper™ LT (Becton Dickinson); C) Xpert® HPV, on have been: 56-59-66 (Onclarity P3 group), 31, 51 and 35-39-68
Correspondence
Gaetano Bulfamante, Head Unit of Human Pathology, Cytogenetics
and Molecular Pathology, St. Paolo Hospital, ASST Saints Paul
and Charles, Milan, Italy - Tel. +39 02 503 23167 - 23180 - Fax
+39 02 503 23168 - E-mail: gaetano.bulfamante@unimi.itDETECTION AND GENOTYPING OF HPV-DNA THROUGH DIFFERENT TYPES OF DIAGNOSTIC PLATFORMS IN LIQUID BASED CERVICAL-CYTOLOGY SAMPLES 295
(Onclarity P2 group). This remark emphasizes the importance of ated with type-specific interactions between genotypes in multiple
HPV infection and genotypes distribution’s continuous monitoring, infections and, in addition, other genotypes, not targeted by quad-
considering that HPV-vaccines planned in Italy in the “National rivalent HPV-vaccine, can increase the risk of cervical carcinoma.
vaccination prevention program 2017-2019” are not specific for 5) As there’s a different combination of HPV-genotypes in diagnos-
the majority of these genotypes. 4) The necessity to improve the tic categories used by the HPV screening platforms, it’s important
screening program to identify cervical carcinomas and pre-neoplas- that anyone who is in charge of this diagnostic analysis promotes
tic cervical lesions is remarked by the detection during HPV-test among clinicians the adequate rendition of the laboratory’s data
of possible coinfection (present at least in 8,76% of our records). in the patient records, reporting both the diagnostic result and the
In fact, the risk of development of cervical cancer might be associ- method through which it has been obtained.
Introduction compares the results of HPV detection and genotyping
on liquid based cervical cytology, using some of the
At present cervical cancer represents the second most most relevant diagnostic platforms in commerce. This
common cancer in women worldwide 1. More than 85% comparison has two main goals: a) to verify the diagnos-
of cervical cancers develops in low-income or resource tic homogeneity among the various platforms, especially
limited countries 2, whereas in 2010, the invasive cervi- as in the Lombardy cervical cancer screening program,
cal cancer rate in the US was 7.5 per 100.000 women 3. women having a negative HPV molecular test do not un-
This type of cancer reaches a global mortality rate of dergo a Pap-test; b) to verify the most common high-risk
52 2. Around 90% of these deaths affects low or medium HPV genotypes in this examined population, particular-
income countries 4 and it is expected that by 2030 98% ly referring to available cervical cancer vaccines.
of cervical cancer deaths will occur in these same coun-
tries 5. The early detection and the adequate treatment
of pre-neoplastic lesions and early-stage cervical cancer Methods
decrease significantly the mortality rate for this type of
cancer 6. Indeed, still nowadays the healing chance is The present study is not based on a population recruited
low when cervical cancer is diagnosed at a later stage through an organized screening program: all patients,
of disease. In 2010 the 5-year survival rate in the US during spontaneous access to their private gynecologist,
was 91% when the diagnosis of invasive cervical can- underwent “liquid based cervical cytology” on which it
cer was made at an early stage of disease, however the has been performed the co-test Pap/Hpv or just the Pap
same survival rate decreased to 16% in late-stage can- test.
cer 7. The conventional Pap-test (Papanicolaou smear) Our clinical records have been collected during the sec-
has historically been the mainstay of pre-neoplastic le- ond half of 2016 and the first half of 2017.
sions detection and cervical cancer screening; recently it The vial used in the examined population has been EAS-
has been introduced a new method, called “liquid-based YPREP® preservative solution (YD Diagnostics CORP-
cervical cytology” (LBCC) 8. The LBCC has one main Republic of Korea); liquid-based cervical cytology
convenience: it’s possible to perform on a single sample sampling has been done using a single device (plastic
both the Thin-Layer Cervical Cytology and the molecu- brush), allowing to collect simultaneously cytological
lar HPV research. Many previous studies 9-16 have sup- material from exocervix and endocervix (Rovers® Cer-
ported the usefulness of molecular research of specific vex-Brush®). Within three months, in the patients who
DNA-HPV genotypes as a primary screening method, underwent Pap-test only it has been performed high-
saving the LBCC just for women with positive HPV test. risk HPV-test, using the sample’ stock. Likewise, within
In this particular occurrence, it’s convenient that the two three months, part of the samples was analyzed through
tests (HPV-test and Pap-test) are realized from the same a second type of DNA-test, using a different diagnos-
liquid-based cytological sample (co-testing), in order to tic platform. The diagnostic platforms employed in the
reduce the number of false negatives of HPV-test or of present study have been the following:
Pap-test 17-22. Lately, the Government of Lombardy has • BD Onclarity™ HPV test, on automate platform BD
approved 23 a regional screening plan which establishes Viper™ LT (Becton Dickinson);
to perform the molecular HPV research in women aged • Xpert® HPV, on GeneXpert® Infinity Systems plat-
between 34 and 64 years. The 12 high-risk HPV geno- form (Cepheid);
types screened are the following: 16, 18, 31, 33, 35, 39, • Digene HC2 HPV DNA Test, on RCS System plat-
45, 51, 52, 56, 58, 59, along with the possibility to in- form (QIAGEN).
clude genotypes 66 and 68. Only women with positive Table I compares high-risk genotypes panels detected
molecular HPV test will undergo liquid based cervical by the various diagnostic platforms with the standard
cytology. Currently there are several types of diagnos- required from Lombardy for its screening program. The
tic platforms detecting and molecular genotyping HPV, molecular and cytological diagnoses have been con-
which are based on different procedures, determining ducted independently by operators in a blind trial; when
uneven viral genotypes panels and using diverse type of the same sample was tested with different platforms in
vials to collect and store the samples. The present study order to identify HPV, operators were working ignoring296 B. CASSANI ET AL.
Tab. I. HPV genotypes determined with different diagnostic plat-
forms. Fig. 1. Characteristics of the examined population. All samples
have been collected with single device (plastic brush) “Rovers®
HPV genotypes Cervex-Brush®” and placed in the vial “EASYPREP® preservative
BD Digene
considered Xpert® solution” (YD Diagnostics CORP-Republic of Korea).
Onclarity™ HC2 HPV
in Lumbardy HPV A. Examined population: 1284 women; 1152 have been examined
HPV test DNA Test in the first place with Digene HC2 HPV DNA Test (blue column),
screening program
and other 159 in the first place with Xpert® HPV test (red column).
16 X X X
B. 272 of 1125 women analyzed using HC2 HPV DNA test have
18 X X X been reassessed with BD Onclarity™ HPV test (green column).
31 X X X C. All 159 women firstly examined with Xpert® HPV test (red col-
umn) have been re-analyzed with BD Onclarity™ HPV test (green
33 X X X
column).
35 X X X
39 X X X
45 X X X
51 X X X
52 X X X
56 X X X
58 X X X
59 X X X
66 (optional) X X
68 (optional) X X X
first analysis result. Pap-test diagnoses are not evaluated
in the present study, because it is focused on HPV-test
diagnostic concordance rate using different platforms:
in fact, organized screening programs, which establish
molecular test as the primary test to perform, do not
prescribe Pap-test execution if molecular test is nega-
tive. Part of the clinical records has also been analyzed
through PCR and direct sequencing of L1 and E6/E7
viral genes region, in order to further typing the viral in 15,07% of samples, with Xpert® method in 13,83% of
population. Our Human Pathology Unit cooperates with samples and using HC2 procedure in 12,27% of samples.
external quality control for HPV screening (VEQ HPV These rates are not significantly different according to a
Screening), organized by Lombardy Government. Re- statistical data analysis (HC2 versus Onclarity: p = 1,54;
sults’ statistical significance has been evaluated accord- Onclarity versus Xpert: p = 0.12; HC2 versus Xpert:
ing to Chi-Squared test (one tailed). A p-value of ≤ 0.05 p = 0.31). The comparison between the three molecular
was considered as statistically significant. methods revealed diagnostic discrepancies in 3,14% of
our records (5/159) between Onclarity and Xpert (re-
spectively 3 positive samples using Onclarity and nega-
tive using Xpert; and 2 positive samples using Xpert and
Results negative using Onclarity) and it revealed discrepancies
We have examined 1284 samples of women aged 16 to in 2,20% of our records (6/272) between HC2 test and
Onclarity test (respectively 6 negative samples using
73 years. Table II displays the age distribution. Among
HC2 and positive using Onclarity). The PCR analysis
these, 1125 have been tested using HC2 procedure, 272
and L1, E6/7 viral genes sequencing revealed 1 positive
samples have been analyzed with Onclarity method, 159 sample for HPV-16 and 2 positive samples for HPV-18:
with Xpert® method (Fig. 1) and 55 samples have been this samples were negative according to HC2 method; in
analyzed using PCR and sequencing of gene L1 and genes these three samples, all belonging to women older than
E6/E7. HPV-DNA was detected with Onclarity method 34 years, the Pap-test has always been positive for HPV-
related lesions. Globally, referring to 431 tests evaluated
with different methods, discrepant diagnoses of hr-HPV
Tab. II. Age distribution in the examined population.
have been recorded 11 times (2,25%): HC2 High-Risk
Number of HPV DNA Test has diagnosed as “negative for hr-HPV
Age %
patients
infection” 6 of 272 samples (2,20%) co-tested with other
< 25 122 09,5%
platforms (Onclarity), Onclarity method has diagnosed
25-33 327 25,5% as “negative for hr-HPV infection” 2 of 159 samples
34-64 794 61,8% (1,26%) co-tested with Xpert and Xpert has diagnosed
> 64 41 3,2% as “negative for hr-HPV infection” 3 of 159 samples
Total 1284 100 (1,88%) co-tested with Onclarity. Among 81 HPV-testDETECTION AND GENOTYPING OF HPV-DNA THROUGH DIFFERENT TYPES OF DIAGNOSTIC PLATFORMS IN LIQUID BASED CERVICAL-CYTOLOGY SAMPLES 297
Tab. III. Specific genotypes detected in 81 HPV-test positive samples. Discussion
Prevalence
HPV Genotypes N° of cases %
ranking The risk of invasive cervical cancer considerably de-
16 17 20,99 1° creases in women who periodically undergo Pap-test
18 04 4,94 7° and/or DNA-HPV test 24 25. The conventional Pap-
31 12 14,81 3° smear has been proven to represent a critical tool to
45 03 3,70 8° diagnose cervical pre-neoplastic lesions and cervical
51 10 12,34 4° early stage cancer 26; its effectiveness has been fur-
52 08 9,88 6° ther enhanced after the introduction in current clinical
P1 04 4,94 7° practice of LBCC 27 28. The Pap-test remains, however,
P2 09 11,11 5° an exam whose diagnostic results are profoundly in-
P3 14 17,28 2° fluenced by human subjectivity (high inter and intra
Keys: P1 = genotypes 35,58. P2 = genotypes 35, 39,68. P3 = genotypes operator variability referring to diagnostic criteria) 29 30
56, 59, 66. and by the level of expertise/tiredness of screeners 31-
33
. Currently, molecular identification of high-risk
HPV genotypes (hr-HPV test) is used as primary test
in several cervical cancer screening programs, because
positive samples, it has been possible to identify the in- its ability to identify high grade intra-epithelial cervi-
fecting genotype (Tab. III). The most detected genotype cal lesions is considered statistically superior than the
has been number 16 (20,99%), followed by P3 Onclar- cytological one 34 35. However, the application of mo-
ity group (including genotypes 56,59,66) (17,28%) and lecular HPV-test as primary cervical carcinoma screen-
by genotype 31 (14,81%). Genotype 18 was observed ing tool unfolds several uncertainties. To date, several
to a lesser extent in our population (4,94%). Using the large available cervical cancer series have documented
three HPV-screening methods, in 8,76% of the popula- that HPV- test is negative in 10 to 19% of women with
tion co-infection with more hr-HPV genotypes has been biopsy-confirmed cancer 36-40. The test power to detect
cervical adenocarcinoma varies from approximately
detected. It was not possible to specifically characterize
32 to 100%, depending on the geographic region and
the genotypes determining these co-infections, because tumor subtype 41-46. Human papillomavirus DNA is
both Onclarity and Xpert join different genotypes in detected in 80 to 100% of the 3 most common histo-
groups, which are not homogeneous and therefore not logical subtypes of cervical adenocarcinoma (endocer-
further analyzable. Onclarity individually reveals geno- vical, endometrioid and intestinal subtypes), whereas
types 16, 18, 31, 45, 51 and 52 positivity; in “P1” group it’s rarely detected in non-mucinous subtypes, such as
it gathers genotypes 33 and 58; in “P2” group genotypes clear cell, serous and mesonephric adenocarcinoma. In
35, 39, 68 and in “P3” group genotypes 56, 59 and 66. addition, the gastric type, which includes minimal-de-
On the other hand, Xpert identifies as “P1” genotype 16, viation adenocarcinoma, was shown to be unrelated to
as “P2” genotypes 18 and 45, as “P3” genotypes 31, 33, HPV infection 47. Cervical adenocarcinomas constitute
35, 52 and 58, as “P4” genotypes 51 and 59 and as “P5” about 5 to 27% of all cervical carcinomas: their number
genotypes 39, 68, 56 and 66. The PCR analysis and L1, varies between different countries 48-52 and it is globally
increasing 53 54. Eventually it has been observed that
E6/7 viral genes sequencing revealed that co-infection
Pap-test cervical carcinoma screening can occasionally
can be determined by high-risk HPV genotypes only, but detect endometrial carcinomas or endometrial atypical
also by concomitant presence of high-risk genotypes and glandular cell (AGC) 55: these pathological entities are
intermediate or low risk ones (Tab. IV). negative using HPV-test 56; therefore, primary HPV-test
screening, instead of Pap-test, may result in losing the
possible benefits of early diagnosis of endometrial can-
Tab. IV. HPV co-infection detected through PCR and genes L1 and cer 57. According to several strategies of cervical cancer
E6/E7 complete sequencing.
screening, the algorithm connecting cervical cytology
HPV Intermediate and hr-HPV test is still debated and it’s influenced by
High risk Low risk
Genotype risk
both economic available resources and patient char-
Case
acteristics (such as age; organized screening program
1 16 + 31
versus spontaneous patient request of exam or occa-
2 16 61
sional medical indication during gynecological visit –
3 16 66
the so called “opportunist screening” (OS)).
4 18 66
Starting from a single liquid based cervical cytology
5 18 66 sample, several diagnostic algorithms are possible:
6 53 + 67 a) the two tests can be always and simultaneously per-
7 31 6 formed (co-testing) 40 58-60;
8 6 + 72 b) it’s possible to initially search the virus presence
9 67 81 (definition of “presence of infection”) and then it canYou can also read