LINEAR IGA BULLOUS DERMATOSIS IN PATIENTS WITH INFLAMMATORY BOWEL DISEASE SHOULD NOT BE MISTAKEN FOR DRUG ALLERGY
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Journal of Allergy and Infectious Diseases Williams et al., J Allergy Infect Dis 2020;
1(1):15-17.
Case report
Linear IgA bullous dermatosis in patients with
inflammatory bowel disease should not be
mistaken for drug allergy
Kathy N. Williams1, Angelica Nocerino1, Silvija P. Gottesman2, Shelly Rivas2, Arun Swaminath1*
Division of Gastroenterology,
1
A 36-year-old Hispanic male, with a history of ulcerative colitis (UC) presented to the
Department of Medicine, Lenox Hill inflammatory bowel disease (IBD) clinic for initial evaluation. Over the past six years, the patient
Hospital, Northwell Health, New York,
New York, USA had been treated for his UC with various therapies including prednisone, multiple mesalamine
formulations, and budesonide but always discontinued therapy due to what he perceived were adverse
2
Department of Dermatology, Lenox drug reactions. He described onset of pruritic blisters, affecting his chest, abdomen, back, and arms.
Hill Hospital, Northwell Health, New
York, New York, USA rus He complained of multiple bloody bowel movements each day, associated with rectal burning,
pain with defecation and an unintentional 12-pound weight loss over the past 2 months. After his most
recent colonoscopy revealed pancolitis with biopsies significant for chronic inflammation throughout
the colon without dysplasia with skin tags and anal fissure with rectal sparing, his diagnosis was
*Author for correspondence:
Email: Aswaminath@northwell.edu revised to Crohn’s ileo-colitis. Although symptomatic, he was very hesitant to start medical therapy
given his previous experience. He has never been in clinical remission.
Received date: April 30, 2020
Accepted date: May 25, 2020
Copyright: © 2020 Williams KN, et
al. This is an open-access article
distributed under the terms of the
Creative Commons Attribution License,
which permits unrestricted use,
distribution, and reproduction in any
medium, provided the original author
and source are credited.
Citation: Williams KN, Nocerino A,
Gottesman SP, Rivas S, Swaminath
A. Linear IgA bullous dermatosis in
patients with inflammatory bowel Figure 1: A) Vesicles (arrows) and eroded papules are seen on the posterior neck of the patient. B)
disease should not be mistaken for Hyperpigmented macules are appreciated on the chest, some with depressed appearance. C) Hyperpigmented
drug allergy. J Allergy Infect Dis 2020; macules coalescing in patches due to a resolved bullous dermatitis are seen on the patient’s back and upper
1(1):15-17. arms at a follow up visit.
This article is originally published by ProBiologist LLC., and is freely available at probiologists.com
J Allergy Infect Dis 2020; 1(1):15-17. 15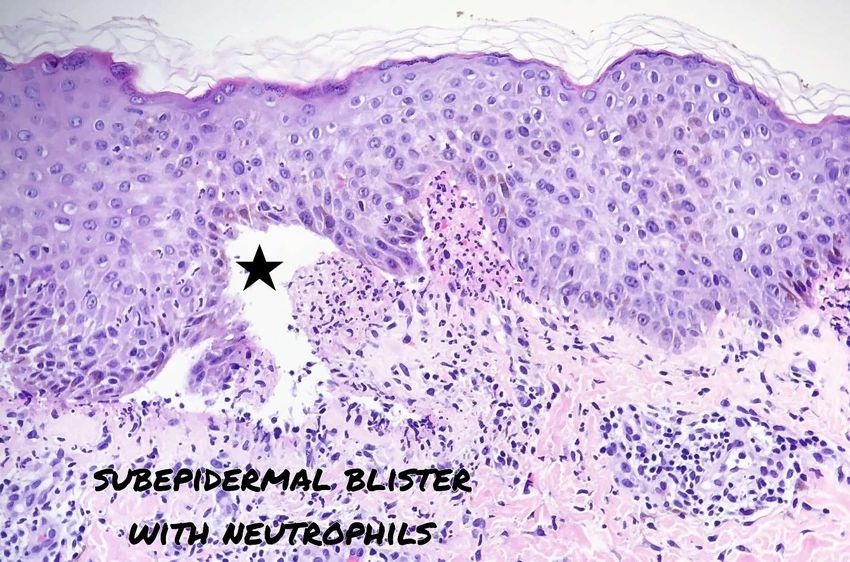
Citation: Williams KN, Nocerino A, Gottesman SP, Rivas S, Swaminath A. Linear IgA bullous dermatosis in patients with inflammatory bowel disease
should not be mistaken for drug allergy. J Allergy Infect Dis 2020; 1(1):15-17.
The patient was referred to a dermatologist for further evaluation Given the neutrophilic nature of this bullous disease, he was
of his skin lesions, as it was unclear whether the etiology of the prescribed dapsone 100 mg daily every other day which resulted
dermatitis was a true adverse drug reaction. On physical exam, small in resolution of the rash. The patient was reassured that these skin
rare intact bullae were noted on the posterior neck, along with eroded reactions were extra-intestinal manifestations of his underlying
papules at the upper back (Figure 1A). Hyperpigmented macules inflammatory bowel disease and not a drug reaction to the medications
coalescing into hyperpigmented patches were noted on his chest he had previously taken for ulcerative colitis. He was subsequently
and back and some appeared to have a slightly depressed appearance treated with infliximab and achieved a deep remission with control
(Figure 1B/C). Skin biopsies were taken, for hematoxylin and eosin of skin rash with dapsone. He did have a brief interruption of
(H&E) and direct immunofluorescence. H&E sectioning revealed therapy with dapsone which resulted in recurrence of the rash. This
subepidermal bulla with brisk neutrophilic inflammation (Figure 2) subsequently resolved with reintroduction of therapy. Workup of
and linear deposition of IgA on direct immunofluorescence (Figure a persistently elevated alkaline phosphatase with an MRI revealed
3). These findings were consistent with linear IgA disease. intrahepatic duct dilation. Liver biopsy confirmed comorbid PSC.
Figure 2: Subepidermal bulla with brisk neutrophilic inflammation is seen on hematoxylin and eosin sections (x200 magnification).
Figure 3: Linear deposition of IgA observed on direct immunofluorescence. These findings were consistent with linear IgA disease.
J Allergy Infect Dis 2020; 1(1):15-17. 16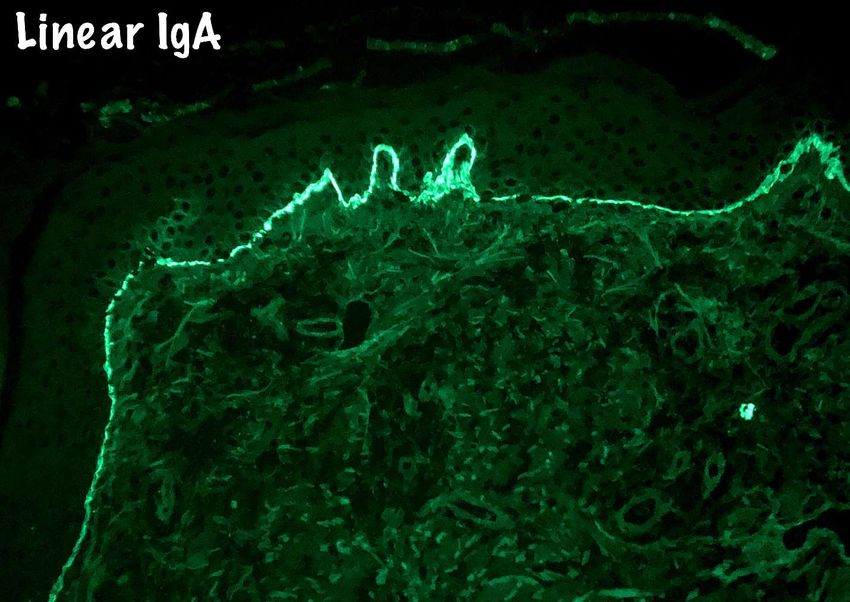
Citation: Williams KN, Nocerino A, Gottesman SP, Rivas S, Swaminath A. Linear IgA bullous dermatosis in patients with inflammatory bowel disease
should not be mistaken for drug allergy. J Allergy Infect Dis 2020; 1(1):15-17.
Discussion This case adds to the literature supporting the idea that LABD
Linear IgA bullous dermatosis (LABD) is suspected to be may be a dermatologic manifestation of IBD. In addition, this case
a rare extraintestinal manifestation of IBD. This autoimmune uniquely illustrates that Linear IgA dermopathy does not track
subepidermal disease presents with bullae, erosions and vesicles. IBD disease activity as the patient continues to require dapsone to
LABD is characterized by the immunopathologic finding of manage his skin manifestations despite achieving deep remission
linear IgA deposits in the basement membrane along the dermo- on infliximab therapy. This is one of few cases confirming the
epidermal junction. This skin disorder was first identified by direct association between Linear IgA bullous disease and Crohn’s disease
immunofluorescence by Chorzelski et al. [2]. Theories about in a patient with comorbid PSC.
pathogenesis include abnormalities in mucosal B cells and mucosal
IgA production as well as abnormal mucosal permeability leading to
References
atypical IgA production. [3,4]. The exact etiology of this rare disease 1. Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J.
Bleeding and Thrombotic Disorders. In:Harrison’s Manual of Medicine.
is still unknown, but both drug induced and spontaneous forms of
19e. 2016, McGraw-Hill Education: New York, NY.
LABD have been observed. There are rare reports of an association
between LABD and Crohn’s disease [5,6]. 2. Guide SV, Marinkovich MP. Linear IgA bullous dermatosis. Clinics in
Dermatology. 2001 Nov 1;19(6):719-27.
While the presence of vesicles makes LABD clinically similar to
bullous pemphigoid and dermatitis herpetiformis, the presence of 3. Selby WS, Janossy G, Bofill M, Jewell DP. Intestinal lymphocyte
linear IgA deposits in the basement membrane defines Linear IgA subpopulations in inflammatory bowel disease: an analysis by
immunohistological and cell isolation techniques. Gut. 1984 Jan
bullous dermatosis as a distinct disease. LABD can be defined by
1;25(1):32-40.
three distinct criteria: presence of vesicles or bullae on skin, presence
of subepidermal vesicles with a neutrophil predominance seen on 4. MacDermott RP, Nash GS, Bertovich MJ, Mohrman RF, Kodner IJ,
histological examination and most definitively, the linear pattern of Delacroix DL, Vaerman JP. Altered patterns of secretion of monomeric
IgA basement membrane zone-specific deposits in the absence of IgA and IgA subclass 1 by intestinal mononuclear cells in inflammatory
bowel disease. Gastroenterology. 1986 Aug 1;91(2):379-85.
other immunoglobulins [7]. The bullae associated with LABD often
appear on the abdomen and limbs but bullae may also present on 5. Torres T, Sanches M, Selores M. Linear IgA bullous disease in a patient
the hand, feet and perineum of affected patients. The form of LABD with Crohn’s disease. Acta Dermatovenerol Alp Pannonica Adriat.
which presents in childhood (childhood onset LABD: chronic 2010;19(1):29-31.
bullous disease of childhood (CBDC) has a peak age of incidence at 6. De Simone C, Guerriero C, PELLICANO R. Linear IgA disease and
4-5 years of age. Adult onset LABD has a peak age of incidence at ulcerative colitis. European Journal of Dermatology. 1998 Jan 30;8(1):48-
60-65 years old. The clinical presentation of CBDC is distinct from 50.
LABD in that CBDC localizes to the lower abdomen and perineum 7. Egan CA, Zone JJ. Linear IgA bullous dermatosis. International Journal
[7]. of Dermatology, 1999 Nov;38(11):818-27..
Drug induced LABD has been associated with treatment with 8. Plunkett RW, Chiarello SE, Beutner EH. Linear IgA bullous dermatosis
vancomycin, amiodarone and other antibiotics, such as penicillin in one of two piroxicam-induced eruptions: a distinct direct
and ceftriaxone; it is not associated with any of the medications immunofluorescence trend revealed by the literature. Journal of the
this patient was on. The drug induced form of LABD has also been American Academy of Dermatology. 2001 Nov 1;45(5):691-6.
associated with non-steroidal anti-inflammatory drugs (NSAIDs) 9. Chanal J, Ingen‐Housz‐Oro S, Ortonne N, Duong TA, Thomas M,
such as piroxicam, naproxen [8,9], as well as amiodarone. The time Valeyrie‐Allanore L, et al. Linear IgA bullous dermatosis: comparison
of onset for drug induced LABD ranges from 2 days to up to 4 between the drug‐induced and spontaneous forms. British Journal of
weeks. The gold standard therapy for LABD is oral dapsone. Dermatology. 2013 Nov;169(5):1041-8.
J Allergy Infect Dis 2020; 1(1):15-17. 17You can also read