Maintaining Skin Integrity and Preventing Pressure Ulcers - Information for Residential Care Homes - NHS Sutton CCG
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Maintaining Skin Integrity
and
Preventing Pressure Ulcers
Information for Residential Care Homes
Version 1.0 – 25 January 2018 (Review date 2020)
Introduction to using this resource folder
This folder contains comprehensive information about the assessment, monitoring and
maintenance of skin integrity for care home residents. The focus is on prevention of skin
damage but also includes what to consider if the skin is broken. Where available it includes
National evidence-based guidelines.
This folder contains information for carers including ‘top tips’ to ensure your residents are
protected from skin breakdown. All care home staff should have training on how to prevent
pressure ulcers and this guide contains information that can support staff training.
This resource folder has been developed by the Sutton Homes of Care Vanguard. The
contents of this folder represent best practice in this area of care; however, the safe and
effective management of residents’ needs remains the legal responsibility of the care
home.
Contents Page
1.0 The Skin
Why is the skin important? 3
What happens to the skin as we get older? 3
What causes damage to the skin? 4
2.0 Pressure ulcers
What is a pressure ulcer? 4
How do I know if my resident is at risk of pressure ulcers? 5
What to do next 6
3.0 Minimising risk using SSKIN prevention guidance
3.1 Surface: Support surfaces including mattresses and cushions 7
3.2 Skin: How to keep the skin healthy, how to inspect the skin and what to look for 8
3.3 Keep moving: Supporting your residents to change position 10
3.4 Incontinence: Supporting your residents with incontinence 11
3.5 Nutrition: Supporting your residents to eat and drink well 12
3.6 How to write a care plan for residents at risk/with pressure ulcers 12
4.0 Other types of skin damage
4.1 Moisture lesions 13
4.2 Trauma (Skin tears) 14
4.3 Skin changes at end of life 15
5.0 Safeguarding your residents 16
6.0 Residents transferring between care settings 17
7.0 References, acknowledgements and further information 17
Appendices Page
A Stages of pressure ulcers (3 pages) 19
B Waterlow risk assessment tool 22
C Guidance on checking mattresses 23
D Example repositioning/turning chart (double-sided) 24
E Resident and family information leaflet 26
F Example body map 27
G Pictures of moisture lesions 28
2
1.0 The Skin
Why is the skin important?
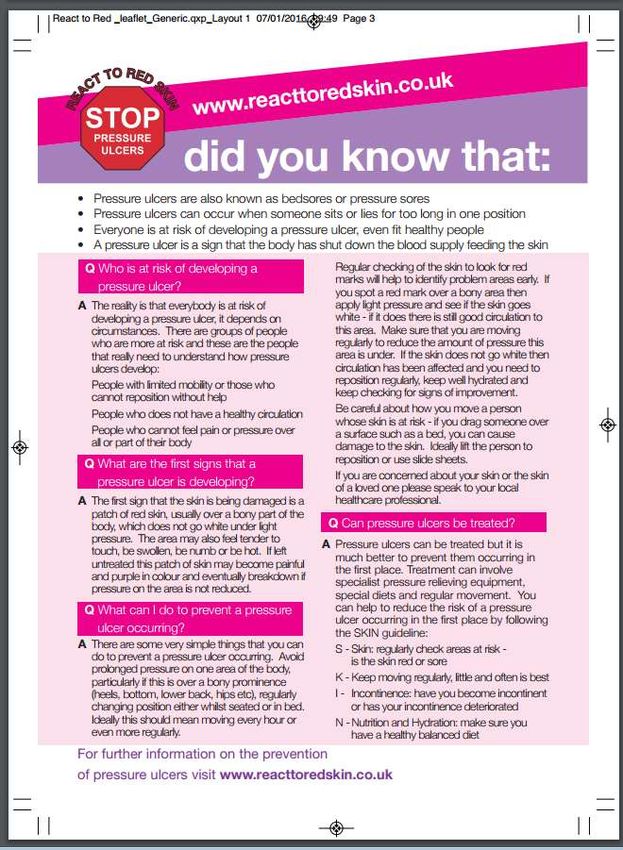
The skin is the largest organ in the human body and is a protective barrier. It shields the
body against heat, light, injury, and infection. The skin also helps regulate body temperature
and gathers sensory information from the environment e.g. touch, pain, pressure, vibration
and temperature. The skin stores water, fat and vitamin D, and plays a role in the immune
system protecting us from disease. The skin is naturally acidic with a pH of 4.5-6.5 which
inhibits the growth of bacteria and fungi. The skin is made up of three layers which are
outlined in table 1 below.
Table 1: Layers and function of the skin
Layer Thickness Components Function
Epidermis 0.1mm Skin cells Protective shield
Dermis 2 mm Connective tissue, blood Structure and support
vessels, lymph vessels, nerve Temperature regulation
fibres, sweat glands, hair Sensation e.g. touch, pain
follicles, sebaceous (oil) glands Skin hydration and nourishment
Hypodermis variable Fat cells Insulation from cold
Connective tissue Shock absorption
Storage of nutrients and energy
What happens to the skin as we get older?
As the skin ages it becomes thinner and loses elasticity so it becomes more wrinkled and
saggy. The amount of fat under the skin tends to decrease, making the skin more prone to
bruising, more fragile and easily damaged. There is often a reduced blood supply which
means any injuries to the skin may be slow to heal and regulation of body temperature is not
as effective. The loss of natural moisturising factors in the older person’s skin also reduces
skin hydration and causes it to become dry and flaky. Dry skin is itchy and this can lead to
scratching and skin breakdown.
3
What causes damage to the skin?
The skin can be damaged by cuts, bruises, scrapes, tearing, constant moisture, friction,
unrelieved pressure and shearing forces (the skin moving in one direction and the body
moving in the opposite direction) as outlined in Table 2 below. In older people, the skin is
more fragile and less resilient and therefore is at high risk of damage from any of the above.
This resource folder contains information on the prevention and management of pressure
ulcers, moisture lesions and skin tears.
Table 2: Causes of skin damage
*Definition from Oxford English dictionary (online)
Pressure* Continuous physical force exerted on or against an object by something in
contact with it
Shear* A strain produced by pressure in the structure of a substance, when its layers
are shifted laterally (sideways) in relation to each other (the skin and
underlying body are pulled in different directions, e.g. when a person slips
down the bed)
Friction* The action of one surface or object rubbing against another, e.g. heels
rubbing against a sheet
Moisture Water or other liquid, e.g. urine, faeces and sweat in contact with the skin
Trauma Physical injury for example due to cutting, tearing or burning
2.0 Pressure Ulcers
What is a pressure ulcer?
A pressure ulcer (also known as a pressure sore or bed sore) occurs when the skin and
underlying tissue gets damaged by unrelieved pressure. Essentially the skin, its blood supply
and underlying tissue are squashed between the hard surface (the cause of pressure) and
the underlying bone. The extent of the damage is dependent on which of the skin layers (see
section 1 above) are affected and in serious cases; the underlying muscle and bone can also
be damaged. What you see at the skin’s surface is often the smallest part of the ulcer, and
the tissues under the skin near the bone suffer the greatest damage. Every pressure ulcer
seen on the skin, no matter how small, should be regarded as serious because of the
probable damage below the skin surface. Damage can result from high pressure for a short
period of time or low pressure for a longer period of time.
In 95% of cases, pressure ulcers are completely preventable with good care and therefore
they are classified as an ‘avoidable harm’. This is why skin damage and pressure ulcers
have to be reported- see section 5.
The areas that are most at risk of developing pressure ulcers are the parts of the body that
are not covered by a high level of body fat (bony prominences) and are in direct contact with
a supporting surface, such as a bed or chair. Common areas are the heels, toes, sacrum,
hips, elbows, shoulders and back of the head as shown in picture 1 below. Pressure damage
can be caused by items other than hard surfaces, for example tight clothes and buttons,
support stockings, wrinkles in the bed sheets, medical devices such as urinary catheters and
oxygen tubing, or body parts laying on each other such as knees/ankles when in bed. Being
observant whilst caring for your residents will help you identify other potential risks to their
skin.
4
Picture 1: Common areas at risk of
developing pressure ulcers
Pressure ulcers can have a significant impact
on the wellbeing of your residents, including
long-term pain and distress, embarrassment
(some pressure ulcers smell), restricted
lifestyle whilst the ulcer is healing and an
increased risk of life-threatening infection,
such as widespread infection of the blood
(sepsis). Pressure ulcers are categorised into
different stages depending on the extent of
damage to the skin and underlying tissues.
Appendix A illustrates the different stages of
pressure ulcers (please note some images
may be distressing to look at).
How do I know if my resident is at risk?
There are many factors that increase the risk of developing a pressure ulcer and these are
outlined in table 3 below. Generally anyone living in a care home will be at risk due to a
combination of factors such as their age, reduced independence and levels of mobility and
long term health conditions. Early recognition of individuals at risk of pressure damage is an
essential part of prevention and formal assessment enables the correct interventions to be
started and maintained (see management guidelines below).
Table 3: Risk factors for developing pressure ulcers
Risk factor Rationale
Age The older you are the more fragile and thin your skin is.
Sex Women are at higher risk due to distribution of body fat compared to men.
Body shape/weight Being underweight means the skin has less fat to provide protection
whereas being overweight means the additional body weight adds extra
pressure.
Appetite and diet Good nutrition and hydration are important to keep the skin healthy and to
promote healing in any damaged areas.
Reduced/restricted The less able a person is to move independently, the less able they are to
mobility relieve pressure.
Poor moving and handling techniques can increase a person’s risk,
particularly moving someone up in the bed/chair as there is an increased
risk of both shear and friction forces on the skin.
Incontinence Exposure to constant moisture damages the skin; urine and faeces are
particularly irritating.
Condition of the skin Skin that is already compromised or damaged is at greater risk of further
including previous breakdown.
pressure ulcers A history of previous pressure ulcers constitutes high risk
Reduced sensory Reduced sensitivity to feeling pain and pressure (due to a medical
function condition or nerve damage) makes it harder to recognise that something is
wrong.
Medicines Some medicines affect the thickness of the skin e.g. steroids and anti-
inflammatories or make the skin more prone to bruising e.g.
anticoagulants.
Other health conditions Some medical conditions affect the blood supply to the skin and therefore it
receives less oxygen and nutrients to keep it healthy. Examples include
5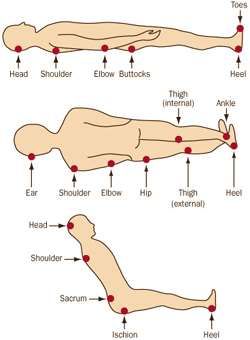
diabetes, organ failure, peripheral vascular disease and anaemia.
Neurological conditions (affecting the brain and/or spine) such as stroke
and multiple sclerosis impact on the skin due to a combination of reduced
mobility, changes to sensation, blood circulation and medicines.
Being completely immobile for a period of time (usually 2 days or longer)
increases the risk. Examples for care home residents include a period of
illness requiring bed rest, a visit to A+E where they will be lying or sitting
on a trolley, waiting in transport lounge.
Every resident should be assessed to determine their risk of developing pressure ulcers.
This should be completed within 6 hours of admission to the care home (NICE 2014). The
risk should also be reassessed as frequently as required. Any resident identified to be at
risk should be referred to the community nurse for a full assessment using the Waterlow risk
assessment scale (Appendix B).
To use the Waterlow tool, training is required however carers can use the first six sections to
inform a risk assessment as this is information you already know about your resident. These
sections are:
Gender
Age
Build/weight
Appetite
Mobility
Continence
The risk level should also be reassessed when there is a clinical concern or change in the
person’s mental or physical status, for example in the following situations:
• weight loss or change to appetite
• changes to the skin e.g. bruises, cuts
• changes to continence e.g. diarrhoea or incontinent episodes
• prolonged or recurrent illness or infection
• changes to mobility levels
If your resident has been in hospital (or another care setting), it is good practice to reassess
their risk of pressure ulcers (and other risk assessments) when they return to the care home,
in case they have changed whilst in hospital.
What to do next?
Any resident identified to be at risk should be referred to the community nurse. For every
resident, it is important to initiate prevention measures which can be remembered by the
abbreviation SSKIN: Surface, Skin, Keep moving, Incontinence, Nutrition (see
http://nhs.stopthepressure.co.uk). The SSKIN preventative measures relate to the risk
factors that can be addressed and modified and they are discussed further below. Health
conditions that affect the risk of developing pressure ulcers are unlikely to go away but their
treatment and management should be optimised in liaison with the GP (e.g. good control of
diabetes and blood glucose levels). A medication review can identify medicines that are
affecting the risk score and consider whether this risk can be reduced.
6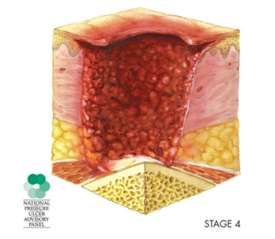
Start taking pressure ulcer prevention measures (using SSKIN principles outlined below).
Refer to the community nurse for provision of pressure relieving equipment, wound
management and further advice on preventative measures for that resident.
3.0 Minimising risk using SSKIN prevention guidance
3.1 Surface
This refers to the surface that residents are sitting or lying on, in other words, the chair
cushion and bed mattress. The surface underneath the resident needs to provide the right
amount of support and comfort and no resident at risk of pressure ulcers should be nursed
on anything less than a high density foam mattress. Residents are at greater risk of pressure
damage when seated than they are when lying in a bed due to the distribution of their body
weight. Continue to move residents frequently whatever the type of support surface used
and make sure bedclothes and clothing are smooth under the resident when repositioning.
Don’t use too many Inco sheets or plastic-backed Inco sheets as this may make the skin
sweat more and add risk of moisture on the skin (see section 4.1). It is important to use the
correct moving and handling techniques as tissue damage may also occur when a resident
slips down the bed during repositioning or slumps in a chair.
Support surfaces may also be described as pressure relieving equipment that work by either
spreading out the pressure (redistribution) or removing pressure regularly from different
parts of the body (alternating). These are expensive sophisticated products which, in the
case of residents at high and very high risk, can make all the difference to their susceptibility
to pressure ulcer damage.
It is important that you know how to check and document that the support surface being
used is in good working order so that it provides the support your resident requires.
How to check a foam mattress
The amount of support a mattress/cushion will provide is dependent on it being fit for
purpose. After a period of use, mattresses/cushions can ‘bottom out’. This can be tested for
by spreading the hands and pushing down on the middle third of the mattress. It should not
be possible to feel the base of the bed. Though a very simple test, it is one that is easily
carried out, and gives you a very good idea of the state of the mattress. Mattresses and
mattress covers should be examined for damage or staining, which will create a risk of cross
infection. Further information for care home managers regarding checking mattresses can
be found in Appendix C.
How to check a pressure-relieving mattress
There are several things that need checking to ensure the mattress will provide the support
that is required. These are outlined in the table below and should be explained in the
manufacturer’s instruction booklet.
Table 4: Things to consider when checking a mattress
Power supply Check it is plugged in and switched on
Weight-setting Is it set correctly for the weight of your resident?
7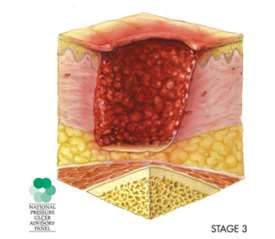
Is there a ‘static’ button Is the static button switched to ‘Off’?
(not all mattresses have this)
Settings/buttons What are the other settings- should they be on/off?
Alarms What do the different alarms mean?
What do you need to do to correct the problem?
Cover Is it damaged or stained?
To check that the air mattress is working effectively:
With the resident on the mattress, place a hand underneath the residents heaviest
part (i.e. their pelvis/buttocks)
Press to see if you can feel air supporting the resident. You should not be able to
feel the hard bed-base
If you can feel the hard bed-base, your resident will also feel the bed-base and the
mattress is not providing adequate support.
Pressure relieving equipment should be checked every time the resident is assisted to
change their position and this can be easily documented on a repositioning/turning chart,
see Appendix D. If the equipment is not working as expected, urgent action is required to
rectify the problem to ensure your resident still receives pressure-relief.
Any resident at risk needs a referral to community nursing for full assessment and provision
of suitable pressure relieving equipment. You will need to know the weight of your resident
and whether they have any moving and handling requirements. When the mattress is
delivered, ensure you know how to check the settings, alarms and that it is working. The
mattress settings should be clearly documented on a pressure ulcer prevention care plan
(see section 3.6).
3.2 Skin
How to inspect the skin
Routine skin inspection plays a role in decreasing the incidence of pressure ulcers. All
residents should have their skin assessed on admission as part of a holistic assessment and
then checked at least every day. Inspect all areas of the skin regularly, with particular
attention paid to bony prominences (see picture 1) and areas of skin that come into contact
with devices such as catheters, compression stockings etc. A compact mirror is helpful to
visualise difficult to see areas such as the heels when the resident is in a chair.
Encourage and educate residents who are willing and able to inspect their own skin and
ensure relatives know how they can help. A resident and carer information leaflet can be
found in Appendix E.
When inspecting the skin, look for any of the following (early signs of pressure damage):
Reddened areas of skin on light skinned people
Blue/purple patches on dark skinned people
Blisters
Hot or cool areas
Swelling
8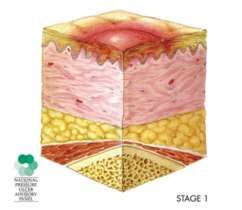
Signs of irritation, or scratches
Patches of hard skin
Where an area of redness or skin discolouration is noted, it is important to check the integrity
of the skin using the finger test below:
Apply light finger pressure to the area for approximately 3 seconds and then release
If the area you pressed is white and then returns to its original colour, there is
probably an adequate blood supply
If the area remains red it indicates pressure damage (called non-blanching erythema)
For individuals with dark skin pigmentation, it may be more difficult to identify changes in
skin colour. Alternative signs such as localised heat (inflammation) or coolness may indicate
pressure damage. The presence of skin blisters over bony prominences is another marker of
early pressure damage. Do not ignore any signs of early skin damage or assume an area of
discolouration is simply superficial damage; deep tissue damage may present as an area of
purple discolouration.
Where skin is intact:
Keep the skin healthy and well hydrated
Continue to inspect the skin daily
Continue to use SSKIN prevention measures
For areas at risk of breakdown, consider using appropriate skin protection products
to maintain skin integrity
Initiate a pressure ulcer prevention care plan
Where an area of redness, discolouration or breakdown is noted:
If non-blanching erythema is noted (see finger test above), the skin should be reassessed
every 2 hours until resolved (NICE 2014).
Document what you see on a body map (see example in Appendix F), including the location
and size. If your resident consents, take a photograph for your records. Refer to the
community nurse for a full assessment. Document areas of pressure damage in the health
records and implement a pressure ulcer prevention care plan (see section 3.6). Increase the
frequency of skin inspection, initiate a repositioning/turning chart and initiate other
preventative strategies immediately to reduce pressure to affected areas. Pressure ulcers
can be very painful, particularly when the dressing is changed so complete a pain
assessment and ask the GP to review the residents’ pain relief. The community nurse will
initiate the ‘Community pressure ulcer care bundle’ and a treatment plan for the pressure
ulcer.
Any damage to resident’s skin, including pressure ulcers are notifiable to the CQC and local
safeguarding team- see section 5.
How to keep the skin healthy
Dry, fragile skin should be rehydrated using a simple, unperfumed moisturiser. Application of
the moisturiser should follow the direction of the body hair and be gently smoothed onto the
9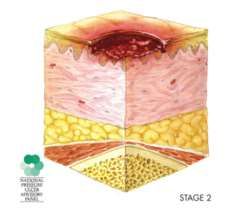
skin. Skin cleansers can be used to clean the skin without rinsing (traditional soaps should
be avoided as they can irritate the skin) and be dried gently. Eating well and drinking enough
water can also keep skin healthy and is vital for wound healing. Fragile skin is at high risk of
tearing and therefore if dressings or tapes are needed, these should be non-adherent (non-
sticky) dressings. Residents should be encouraged to keep their nails clean and short to
reduce the risk of accidental skin tears and infection.
If skin becomes too wet, it can become soggy and more easily damaged. It is important to
protect the skin from contact with urine and faeces and the harmful irritants in them. Where
skin changes are due to excessive moisture, barrier films or creams may also be used to
create a protective layer (see section 4.1).
Particular care should be taken to ensure that areas of skin folds e.g. buttocks, under
breasts and in tummy folds are thoroughly dried. For residents who have contractures (a
disorder in which there is abnormal shortening of a muscle so it becomes permanently
tightened (contracted), there is a higher risk of skin breakdown due to it being more difficult
to keep the area clean and dry. Seek advice for residents who have contractures of the
hands due to the risk of their fingernails digging into the palm of the hand and causing
pressure ulcers.
3.3 Keep moving
To prevent skin damage and pressure ulcers it is important that your resident keeps moving
as much as possible and residents who are immobile are at highest risk of developing
pressure ulcers. Regular movement or repositioning will redistribute pressure and help
prevent pressure damage. Residents who are being cared for on a support surface still need
to be repositioned.
Residents who are able to get out of bed or their chair should be encouraged to do so
whenever possible. Teach residents to change position (offload) every 15 minutes. These
movements need only be small but may give a significant difference in pressure. Changing
position can be incorporated into everyday activities, e.g. standing up to get a drink,
walking/transferring to the toilet.
For residents who need help, reposition at least every 1-2 hours when sitting in a chair or in
bed e.g. on their left side, then on their back, then on their right side. Residents who have
actual damage to their sacral area should only sit out for 45mins-1 hour at a time (depending
on severity). When deciding how frequently repositioning is required, consider the wishes of
the resident and what they are able to tolerate. Changes to position should be recorded on a
repositioning/turning chart, see example in Appendix D. It is important that manual handling
aids are used when moving residents e.g. sliding sheets, to avoid dragging the resident
along the mattress. To help residents maintain their position when in bed, use a
wedge/pillow to maintain a 30-degree side-lying position. Raise the head of the bed to less
than 30 degrees to prevent them slipping down the bed. A 30-degree tilt can also be
achieved in a reclining chair using a wedge/pillow. This will reduce the risk of placing
additional pressure on the hip area.
Ensure the resident knows why they are being repositioned and encourage those who can
do it for themselves. Ensure relatives know how they can help to reduce the risk. Sometimes
10residents refuse to move or have their position changed for them and further advice on how
to manage this situation is outlined in section 5.
3.4 Incontinence
Both urine and faeces are highly irritating to the skin, making it more susceptible to pressure
damage and therefore it is important to maintain continence and actively manage
incontinence. Incontinence is not a normal or inevitable part of ageing and has many
different causes. Always check whether your resident has a urinary tract infection (UTI) as
this can be a cause of incontinence in the elderly or make incontinence worse. Where
continence problems are identified, refer to the community nurse for a full continence
assessment to identify the cause and develop a management plan.
There are a few easy ways to promote continence and reduce the risk of moisture sitting on
the skin:
Take the ‘Toilet First’ approach, ensuring residents can access toilet facilities, wear
clothing that is easy to remove and are regularly offered support to visit the toilet
(every two to four hours). For residents who are regularly incontinent, it may be
helpful to develop a timetable that offers a reminder for going to the toilet.
Gently clean and dry the skin when continence pads are changed or accidents
happen. Wash gently, do not rub.
Avoid using traditional soaps as they can irritate the skin. Skin cleansing products
can be used to clean the skin without rinsing or use a low pH soap which is less
irritating.
Apply a barrier cream or spray, following manufacturers’ instructions on how to apply.
Prevent the resident becoming too hot and sweaty.
Ensure your resident is not constipated as this may have an impact on continence;
monitor their bowel activity using the Bristol stool chart.
Ensuring residents drink enough fluids to prevent them becoming dehydrated.
Consider asking the care home pharmacist for a medication review as some
medicines can affect continence
If using pads, use 1 pad only, folding length-ways to form a channel. Continence
pads should be changed as often as is necessary.
Do not use thick creams, ointments or talcum powder as these can reduce the
absorbency of the continence pad.
If the resident has a catheter, ensure the bag is emptied regularly to prevent it
becoming too heavy. Catheter tubing should be secured safely and any problems
with the catheter addressed quickly.
Continence aids:
Using continence aids can help to keep the resident comfortable and protect skin when used
appropriately. Incontinence pads and pull-up pants can be worn day and night, or during the
night only, to draw fluids away from the skin. It is important to find the right type and
absorbency for the individual. They should be comfortable without chafing the skin or
leaking. They should be changed as often as necessary. Male residents may benefit from
11using a male continence sheath. This is a silicone condom which drains into a bag attached
to the leg and may be particularly helpful when worn at night.
3.5 Nutrition
Adequate nutrition and hydration is important for preventing as well as healing pressure
ulcers. A nutritional assessment, for example using MUST, will identify residents who are not
receiving enough nutrition in the form of calories, protein, vitamins and minerals.
Encourage residents to eat a healthy balanced diet and have regular drinks, ensuring
residents have a choice and variety available. Encouraging participation in the activities
surrounding preparing and serving meals will also keep your residents moving. Assist
residents who find eating meals difficult and ensure those at risk of malnutrition are referred
to a dietician. A resident who develops a pressure ulcer must be referred to the dietician to
ensure their diet is sufficient to enable the ulcer to heal.
More information about nutritional assessment and helping residents to eat and drink
enough can be found in ‘Nutrition and Hydration- Guidance for nursing and residential care
homes’.
3.6 How to write a care plan for residents at risk of/ with pressure ulcers
Residents who are at risk of developing pressure ulcers need to have a care plan that
concisely outlines what specific support is required to enable that person to prevent pressure
damage and reduce their risk score. Those who have skin damage or a pressure ulcer will
also need a care plan that outlines how the pressure ulcer is being managed and how to
promote healing and prevent further damage. Care plans should be written in discussion
with the resident and their family and should be specific, measurable, achievable, realistic
and time-framed (SMART). You may also want to discuss the care plan with the community
nurse.
The care plan for prevention should outline the following:
1. How often you will reassess their risk of developing pressure ulcers
2. What support surface the resident should be using in the bed/chair, how often this
will be checked that it is working properly and how you will know if it is not working or
intact. If they are using a pressure-relieving mattress, the correct settings should be
documented.
3. How often you will inspect their skin and what you are looking for that indicates
potential skin damage. If they have specific items that pose a pressure risk, such as
support stockings or a catheter, how will these areas be checked
4. How will you encourage the resident to change position (or support those who are
unable to move themselves), how often this needs to happen and where will this be
documented e.g. turning chart. For those who are unable, include the moving and
handling equipment required to change their position and refer to their moving and
handling care plan
125. If there are continence issues, how are these being managed to reduce the impact of
urine/faeces on the skin and refer to their continence care plan. If barrier
creams/sprays are being used, where and how often should these be applied
6. If nutrition and hydration are contributing to the risk level, what steps are you taking
to address this, e.g. fluid chart or additional protein snacks. Refer to their
nutrition/hydration care plan
7. If they are using any other pressure relieving equipment e.g. heel protectors, when
should it be used and for how long
8. How you will monitor whether the care plan interventions are successful
9. What to do if interventions are not having the impact expected i.e. when and how to
refer to the community nurse for further advice
The care plan for those with a pressure ulcer should outline the following:
Elements 1-9 above
The care plan should also state how often the community nurse will visit to reassess
and re-dress the pressure ulcer, what to do if the dressing comes off and when and
how to contact them if you are concerned or notice other changes. The community
nurse will leave a ‘Community pressure ulcer care bundle’ document in the resident’s
record which contains all the assessments and treatment plans for that pressure
ulcer to ensure continuity of care if a different community nurse visits the resident.
4.0 Other types of skin damage
4.1 Moisture lesions
What is a moisture lesion?
A moisture lesion is defined as erosion of the skin due to excessive moisture. The moisture
is usually caused by urine, faeces or perspiration. The skin is naturally acidic and both urine
and faeces are alkaline, thus changing the acidity of the skin and causing it to breakdown.
Exposure to excessive moisture causes the skin to become damp, soggy and clammy and
increases the risk of infection and damage due to other reasons e.g. pressure, shearing and
friction. The skin affected by a moisture lesion can be described as excoriated (red and dry)
or macerated (red and white, soggy and shiny). Moisture lesions are most likely to develop in
skin folds e.g. between the buttocks and groin area (particularly with urine and faeces) or
underneath the breasts or folds of tummy (particularly with perspiration). Moisture lesions
can be extremely painful.
Moisture lesions are sometimes confused with pressure ulcers however there must be
moisture present before you develop a moisture lesion. Moisture lesions also look different
to pressure ulcers; they are superficial, with irregular edges, look red or pink and are
‘blotchy’. Appendix G shows what a moisture lesion might look like and Table 5 below
outlines the difference between a moisture lesion and a pressure ulcer. Be aware that
residents can have both a moisture lesion and a pressure ulcer.
Table 5: Differentiating between a moisture lesion and a pressure ulcer
Characteristic Moisture lesion Pressure ulcer
Cause Moisture must be present e.g. shiny wet Pressure and/or shear must be present
13skin caused by urinary incontinence or
diarrhoea
Location Skin folds, particularly buttocks, inner Most common over bony prominences
thigh and groin area (unless the pressure has been caused
Less likely over bony prominences by a piece of equipment e.g. urinary
catheter)
Shape Irregular shape Usually circular
May be linear or mirror image Regular shape
Diffuse, in several superficial spots
Depth Superficial skin loss Superficial or deep, dependent on
stage of ulcer
Colour Non-uniform redness Uniform redness
Blanchable or non-blanchable erythema
Pink/white surrounding skin
Edges Diffuse or irregular edges Distinct edges, may be raised
Necrosis No necrosis A black necrotic scab may be present,
dependent on stage of ulcer
How to prevent and manage a moisture lesion
The best way to prevent and manage a moisture lesion is to ensure that all skin areas are
kept clean and dry. For residents with continence problems, ensure they are offered regular
toileting and that the skin is gently cleaned and dried when continence pads are changed or
accidents happen. Wash gently, do not rub and use a cleansing wash rather than soap and
water (unless low pH soap). Residents whose skin is a risk from exposure to moisture (e.g.
those with episodes of urinary or faecal incontinence) may benefit from using a barrier cream
or spray (e.g. Conotrane) on certain areas such as the buttocks. These provide a waterproof
protective layer to prevent moisture coming into contact with the skin. Ensure you read the
instructions for any barrier cream or spray as different brands require a different frequency of
application to the skin. Some residents will benefit from a referral to the continence service
to ensure their continence is being optimally managed. For severe moisture lesions, a
referral to the TVN may be required.
4.2 Trauma- skin tears
What is a skin tear?
The skin of older people is thin and fragile and is therefore at high risk of cuts and tears. The
skin is easily torn when in contact with sharp edges and objects such as jewellery,
wheelchair levers and footplates and watches. The risk factors for developing skin tears are:
Previous history Shearing, friction and pressure
Older age Bruising
Impaired mobility Dry or fragile skin
Impaired vision Medications
Cognitive impairment, Health conditions affecting the kidneys,
e.g. dementia heart or lungs
Impaired sensation Poor nutrition and hydration
How to prevent a skin tear
Skin tears are painful and if not managed properly could develop into a nasty wound with a
high risk of infection. There are many things you can do to prevent your residents tearing
their skin. These include:
14 Keep fingernails short (residents and staff)
Beware of jewellery (residents and staff)
Use the correct moving and handling techniques
Beware of wheelchairs, particularly foot plates and levers
Use padding to protect vulnerable areas e.g. bed rails and wheelchair arms
Ensure good lighting
Keep residents skin moisturised
Ensure good nutrition and hydration
Encourage long-sleeved clothing
Be vigilant
What to do if you notice a skin tear
Rinse with sterile normal saline (0.9%NaCl)
Pat dry (clean gauze), applying gentle pressure if bleeding
Ensure the flap of skin is returned to its normal position
Cover with a soft silicone-coated atraumatic net dressing (e.g. Atrauman; Silfix etc.)
Indicate the direction of the skin fold
Leave dressing intact, keep dry
Refer to community nursing/community prevention of admissions teams (CPAT) for
urgent review
Monitor for indicators of non-healing e.g. signs of infection, hot, redness, behaviour
change
4.3 Skin changes at end of life
As a person reaches end of life, all the organs of the body start to shut down and slowly stop
functioning. This includes the skin. Changes at the end of life may affect the skin and soft
tissues and changes in skin colour, texture or integrity can be seen. These changes may
also cause pain and may be unavoidable despite appropriate interventions.
Signs and symptoms associated with Skin Changes At Life’s End (SCALE) may include:
Muscle weakness and loss of mobility/unable to move independently
Loss of appetite, weight loss, not eating or drinking.
Reduced supply of blood and oxygen to the skin
The management of skin changes at end of life are exactly the same and the prevention of
skin damage and management of pressure ulcers should follow the SSKIN principles
discussed above. The goals of care are prevention of skin breakdown, promoting healing of
existing wounds, providing palliation and comfort (managing pain, minimising odour and risk
of infection) and responding to residents’ preferences and wishes.
The supportive care home team can provide further advice and guidance around
individualised care planning to support residents at end of life.
155.0 Safeguarding your residents
Reporting incidents and safeguarding
The majority of pressure ulcers can be prevented and therefore when they happen, they
need to be reported, either as an incident or as a safeguarding. Care Quality Commission
(CQC) Regulation 18 outlines that all incidents that affect the health, safety and welfare of
people who use services are reportable to the CQC and should also be reported to the
commissioner for that bed (e.g. local authority or continuing healthcare).
Regulation 18 states:
Any injury to a service user which, in the reasonable opinion of a health care
professional, has resulted in
o changes to the structure of a service user's body,
o the service user experiencing prolonged pain or prolonged psychological
harm
Injuries include those that lead to damage to
o any major organ of the body (including the brain and skin)
o bones
o muscles, tendons, joints or vessels
o the development after admission of a pressure ulcer of stage 3 or above (or
multiple stage 2) that develops after the person has started to use the service
It is good practice to report all incidents of resident harm, including all stages of pressure
ulcers to the local authority and CQC. The Safeguarding Vulnerable Adults team at the local
authority will determine whether incidents relating to the development of skin damage and
pressure ulcers require a safeguarding investigation. Stage 3 or 4 pressure ulcers,
‘unstageable’ ulcers and multiple stage 2 ulcers must be reported as a safeguarding alert.
Care providers also have a Duty of Candour (honesty) to inform the resident and their family
members or appropriate others who are involved regarding any pressure damage acquired
at the home.
Managing residents’ choice and capacity
It is not unusual for residents to refuse to change position or allow care staff to help them
turn in bed. For residents with the capacity to make decisions, it is important that you help
them to understand what pressure ulcers are, why they are at risk and what they can do to
prevent skin damage occurring. You may find the resident information leaflet in Appendix E
helpful. If the person has capacity and refuses care, their reasons for refusal should be
addressed and clearly documented in their notes. They should continue to be offered the
care daily (or again later the same day as appropriate) as people do change their mind.
For residents who lack the capacity to make decisions regarding their pressure area care, a
best interests meeting must be arranged by the care home to discuss this element of their
care requirements. The best interest meeting should involve the family members or
advocate, the GP and any other people involved in the care of that resident (e.g. allocated
social worker, local authority if they are funding the placement, community nurse). The
outcome must be clearly documented in their care notes. If additional restrictions are
subsequently put in place in order to deliver care in the persons best interests, and they are
16subject to a DoLS (deprivation of liberty safeguard) the relevant Best Interest Assessor
should be informed.
Clear documentation of discussions about pressure area care with residents and their family
members or appropriate others who are involved will reduce the chances of the home being
accused of poor care in the event of a resident developing pressure ulcers.
6.0 Residents transferring between care settings
For residents who are at risk or have identified damage to their skin for example a pressure
ulcer, moisture lesion or bruising, it is important that this information is communicated if the
resident has to go to another care setting e.g. hospital, outpatient appointment, day centre,
hospice or other. Staff in these settings will be responsible for ensuring your residents skin
integrity is maintained whilst they are there, however they will not know the specific care
requirements for your resident. In these situations, it is important to send with them the
Waterlow score, a body map and/or wound chart and copies of their skin integrity/pressure
ulcer care plans. This will ensure your resident is supported to keep their skin healthy (or
have their pressure ulcers/ wounds appropriately managed) whilst they are out of your care.
Good documentation and communication with other care settings also helps to prevent the
potential for a safeguarding alert for residents attending hospital with skin damage.
7.0 References
Alzheimer’s Society. 2016. Continence and using the toilet. Available at:
https://www.alzheimers.org.uk/download/downloads/id/1792/factsheet_continence_and_usin
g_the_toilet.pdf 2016
Beldon, P. 2010. Skin changes at life’s end (SCALE): a consensus document. Wounds UK
6(1). http://www.wounds-uk.com/pdf/content_9356.pdf
Care Quality Commission. 2009. Regulation 18: Notification of other incidents. Available at:
http://www.cqc.org.uk/guidance-providers/regulations-enforcement/regulation-18-notification-
other-incidents#full-regulation
European Pressure Ulcer Advisory Panel. 2009. SCALE: Skin changes at life’s end, final
consensus statement. Available at: http://www.epuap.org/wp-
content/uploads/2012/07/SCALE-Final-Version-2009.pdf
Guy, H. 2012. The difference between moisture lesions and pressure ulcers. Wounds
Essentials, Volume 1. Available at: http://www.wounds-uk.com/pdf/content_10448.pdf
NHS Midlands and East. (date unknown). How to: keep residents’ skin healthy. Available at:
http://www.lovegreatskin.co.uk/downloads/howtogreatskinHEALTHYfinal.pdf
NHS Midlands and East. (date unknown). How to: Use support surfaces appropriately.
Available at: http://www.lovegreatskin.co.uk/downloads/howtogreatskinsupportfinal.pdf
17NHS Midlands and East. (date unknown). How to: maintain high quality nutritional care.
Available at: http://www.lovegreatskin.co.uk/downloads/howtogreatskinnutritionfinal.pdf
NHS Midlands and East. (date unknown). How to: manage incontinence/moisture. Available
at: http://www.lovegreatskin.co.uk/downloads/howtogreatskinincontinencefinal.pdf
NHS Midlands and East. (date unknown). How to: Keep patients moving. Available at:
http://www.lovegreatskin.co.uk/downloads/howtogreatskinmovingfinal.pdf
Waterlow, J. 2007. Pressure ulcer prevention aids. Available at: http://www.judy-
waterlow.co.uk/pressure_ulcer_preventative_aids.htm
Wounds UK. 2012. Moisture Lesions Supplement. Wounds UK, London. Available at:
http://www.nhs.stopthepressure.co.uk/docs/WUK%20moisture%20lesion%20supplement%2
02012.pdf
Sources of further information (all of these include resources specifically for carers and
care homes)
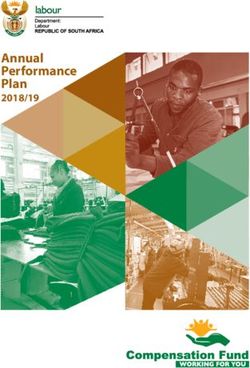
www.reacttoredskin.co.uk
www.nhs.stopthepressure.co.uk
www.lovegreatskin.co.uk
The following factsheets for carers may be useful:
1. Support me, http://nhs.stopthepressure.co.uk/love-great-
skin/LOVE%20GREAT%20SKIN%20support%20me%20factguide.pdf
2. Keep me moving, http://nhs.stopthepressure.co.uk/love-great-
skin/LOVE%20GREAT%20SKIN%20keep%20moving%20factguide.pdf
3. Feed me well, http://nhs.stopthepressure.co.uk/love-great-
skin/LOVE%20GREAT%20SKIN%20nutrition%20factguide.pdf?v=L1WKZwh2Hpg
4. How to manage Incontinence, http://www.nhs.stopthepressure.co.uk/How-
ToGuides/howtogreatskinincontinencefinal.pdf
Acknowledgements:
This guidance document was supported by information provided by The Royal Marsden
Hospital Community Services.
18Appendix A: Different stages of pressure ulcers
Stage 1
Skin is not broken but is red or discoloured or
may show changes in hardness or
temperature compared to surrounding areas.
When you press on it, it stays red and does
not lighten or turn white (blanch). The redness
or change in colour does not fade within 30
minutes after pressure is removed.
On dark skin tones, the redness may not be
easily seen however skin may instead look
purple or blue-ish.
Healing time: approximately 3-7 days
Stage 2
The topmost layer of skin (epidermis) is
broken, creating a shallow open ulcer. The
second layer of skin (dermis) may also be
broken. Drainage (pus) or fluid leakage may or
may not be present.
Healing time: approximately 3 days- 3 weeks
19Stage 3
The wound extends through the dermis
(second layer of skin) into the fatty
subcutaneous (below the skin) tissue. Bone,
tendon and muscle are not visible. Look for
signs of infection (redness around the edge of
the ulcer, pus, odour, fever, or greenish
drainage from the ulcer) and possible necrosis
(black, dead tissue).
Healing time: approximately 4 weeks-6 months
Stage 4
The wound extends into the muscle and can
extend as far down as the bone. Usually lots of
dead tissue and drainage are present. There is
a high possibility of infection.
Healing time: approximately 3 months- 2 years
20Unstageable
Full-thickness skin and tissue loss in which the
extent of tissue damage within the ulcer
cannot be confirmed because it is obscured by
slough (top picture) or eschar (bottom picture).
If slough or eschar is removed, a Stage 3 or
Stage 4 pressure injury will be revealed.
Slough = dead tissue separated from living
tissue, usually yellow, tan, grey, green or
brown colour
Eschar = a scab, usually tan, brown or black
colour in the wound bed
Suspected Deep Tissue Injury
Intact or non-intact skin with localized area of
persistent non-blanchable deep red, maroon,
purple discoloration or epidermal separation
revealing a dark wound bed or blood filled
blister.
This type of pressure ulcer cannot easily be
categorised as the extent of damage to
underlying tissues cannot be determined
Adapted from The National Pressure Ulcer Advisory Panel.
http://www.npuap.org/online-store/home.php?cat=249
21Appendix B: Waterlow risk assessment
WATERLOW RISK ASSESSMENT Residents Name:
Date (Day/Month/Year)
Time
GENDER Male 1
Female 2
14 - 49 1
AGE 50 - 64 2
65 - 74 3
75 - 80 4
81 + 5
Average BMI 20 – 24.9 0
BUILD/WEIGHT Above average BMI 25 – 29.9 1
Obese BMI > 30 2
Below average BMI < 20 3
APPETITE Average 0
(select one option Poor 1
ONLY) N.G Tube/
Fluids only 2
NBM/anorexic 3
Fully 0
MOBILITY Restless/fidgety 1
(Select one option Apathetic 2
ONLY) Restricted/Bed bound 3
Inert (due to ↓consciousness) 4
Chair bound/Wheelchair 5
Continent/catheterised 0
CONTINENCE Occasional incontinence 1
(select one option Incontinent of Urine 2
ONLY) Incontinent of Faeces 2
Doubly incontinent 3
Healthy 0
VISUAL Thin and fragile 1
ASSESSMENT Dry 1
OF AT RISK Oedematous 1
SKIN AREA Clammy (Temp ↑ ) 1
(select one or Previous pressure ulcer or scarring 2
more options) Discoloured Stage 1 2
Broken Stage 2 - 4 3
NEUROLOGICAL Diabetes, CVA, MS, Motor/Sensory
DEFICIT Paraplegia, epidural 4-
(score depends 6
on severity)
Terminal Cachexia 8
TISSUE Multi Organ Failure 8
MALNUTRITION Single Organ Failure
(select one or (Respiratory/Renal/Cardiac) 5
more options) Peripheral Vascular Disease 5
Anaemia HB < 8 2
Smoking 1
MAJOR Above waist 2
SURGERY Orthopaedic, below waist, spinal > 5
TRAUMA 2 hours on theatre table
(up to 48 hours 6 hours on theatre table 8
post-surgery)
MEDICATION Cytotoxics, high dose/long term 4
Steroids, Anti-inflammatory
TOTAL SCORE
INITIALS
Risk Score: 10+ AT RISK 15+ HIGH RISK 20+ VERY HIGH RISK
22Appendix C: Mattress checking- guidance for care home managers
The support surface underneath the resident is an important factor in preventing skin
damage due to pressure. ‘Support surface’ applies to chair cushions and bed mattresses
and includes ‘regular’ cushions/mattresses as well as those specifically designed to be
‘pressure-relieving’.
There are many different products available, each of which will have specific characteristics
and instructions for appropriate use and care. There are a couple of principles that apply,
regardless of the product selected for purchase.
All covers should be made of 2-way stretch material, to reduce the risk of adding to the
shearing forces on a resident’s skin.
Every care environment needs a mattress monitoring plan which identifies the time intervals
for testing and replacement. All mattresses should be dated at the time of first use. The ends
of the bed should be identified from 1- 4 to give an easy reference to systematic turning, end
to end, and top to bottom. Some companies supply pressure mattresses already marked
with this information.
Further information on selecting a suitable support surface can be found at the Disabled
Living Foundation http://www.dlf.org.uk/factsheets/pressure-relief or Wounds-UK
http://www.wounds-uk.com/pdf/content_10638.pdf
23Appendix D: Example Repositioning / Turning Chart
Repositioning chart Residents name:
Week beginning:
Sunday Monday Tuesday
Time Side Pressure Mattress Sig. Side Pressure Mattress Sig. Side Pressure Mattress Sig.
areas working? areas working? areas working?
checked? checked? checked?
0100
0200
0300
0400
0500
0600
0700
0800
0900
1000
1100
1200
1300
1400
1500
1600
1700
1800
1900
2000
2100
2200
2300
2400
Key: L= left side, R= right side, B= on back
Pressure areas to check: head, shoulders, elbows, buttocks/sacrum, hips, knees, ankles, heels and other (please specify)
Equipment checks: Plugged in and switched on? All settings at correct level? Working?
24Repositioning chart Residents name:
Week beginning:
Wednesday Thursday Friday Saturday
Time Side Pressure Equipment Sig. Side Pressure Equipment Sig. Side Pressure Equipment Sig. Side Pressure Equipment Sig.
areas working? areas Working? areas working? areas working?
checked? checked? checked? checked?
0100
0200
0300
0400
0500
0600
0700
0800
0900
1000
1100
1200
1300
1400
1500
1600
1700
1800
1900
2000
2100
2200
2300
2400
Key: L= left side, R= right side, B= on back
Pressure areas to check: head, shoulders, elbows, buttocks/sacrum, hips, knees, ankles, heels and other (please specify)
Equipment checks: Plugged in and switched on? All settings correct? Working?
25Appendix E: Information for residents and family
26Appendix F: Example body map
27Appendix G: Pictures of moisture lesions
28You can also read