MCRPC Presentation E. David Crawford, MD Professor of Surgery/Urology/Radiation Oncology E. David Crawford Distinguished Endowed Chair in Urology ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

mCRPC Presentation
E. David Crawford, MD
Professor of Surgery/Urology/Radiation Oncology
E. David Crawford Distinguished
Endowed Chair in Urology
Head Urologic Oncology
University of Colorado, Denver
2018
E. David Crawford UC School of Medicine
Outline
• Intro/background
• nmCRPC
• Resistance to hormonal therapy
• Alternative approved treatments
• Moving on in the new era
– Combinations
– Biomarkers
– NEPC / t-NEPC / t-SCNC
– Additional targets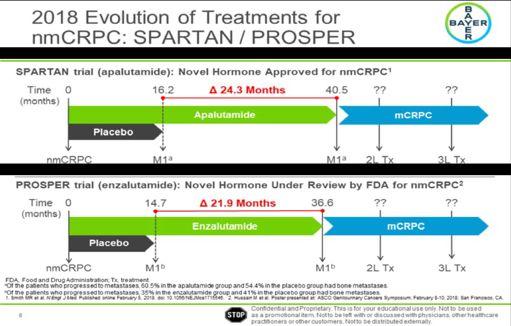
Historical Developments in Prostate Cancer
2003 2018
1940 First GnRH antagonist Apalutamide
Huggins -endocrine 1980s (abarelix) approved
control, use of Long-acting in nmCRPC
1780
orchiectomy, and synthetic
Castration
estrogen treatment LHRH agonists 2011
John Hunter 1904 (Awarded Nobel Abiraterone
First radical
prostatectomy
Prize) approved The future…
New androgen
1900 1940 1970 1980 1990 2000 2010 2020 receptor-targeted
drugs, vaccines,
biomarkers, genetic
1970s
research
Discovery and 1995
characterization of 2008
Bicalutamide
androgen Degarelix
available
receptor approved
1867 1970s
First perineal 1938 Steroidal and
prostatectom Acid non-steroidal 2012
y Phosphatase antiandrogens available Second-generation
1970s antiandrogen approved
Schally and Guillemin- (enzalutamide)
LHRH discovery
(Awarded Nobel Prize)
SOURCE: Dr. ED Crawford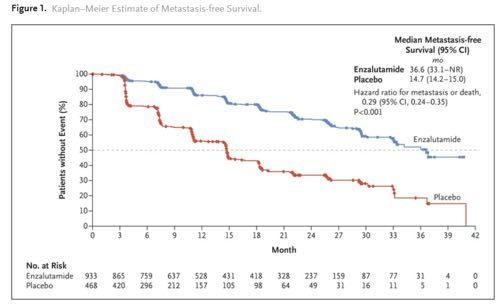
Sources of Androgen Production
Activation of the AR signaling pathway
by androgen is critical for prostate Adrenal
cancer tumor growth and disease Testes glands
progression
Reducing availability of androgen (T) to
bind and activate the AR (lowering
androgen levels or blocking receptor)
decreases tumor cell proliferation Prostate tumor
cells
Therefore, targeting the AR by reducing
serum T to castrate levels via ADT has
become standard of care for patients with
advanced prostate cancer
Androgens are produced at 3 sites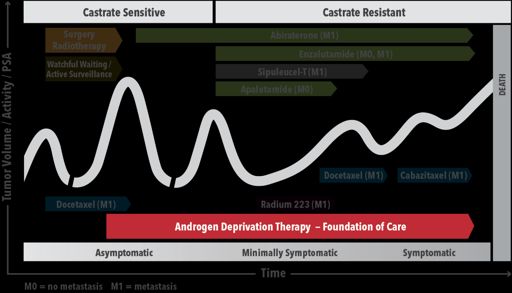
Potential Adverse Events Associated with ADT
QOL ISSUES MEDICAL ISSUES
• Hot flashes • Osteoporosis/ • Thinning of
• Loss of libido skeletal events body hair
• Erectile dysfunction • Diabetes • Testicular
Neurocognitive atrophy
• Fatigue
disease • Cardiovascular
• Anemia disease
• Gynecomastia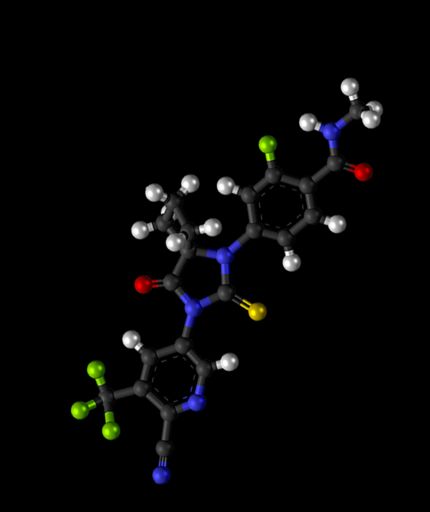
Management of Prostate Cancer Crawford 2018 .
What the Guidelines
Do NOT Tell Us
• Which drug for which patient?
– Options but no specifications
– No comparative data
• What is the best sequence?
– Only docetaxel studies
• When to stop a drug therapy?
– Guidelines tell us when to start, not stop
• Is combination therapy appropriate?
– It is a paradigm used in other cancers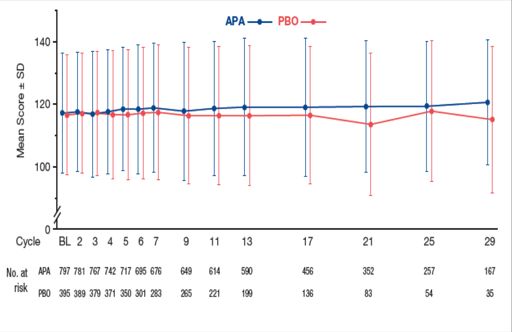
CRPC TREATMENT EVOLUTION
Apalutamide
2004: 2010: 2012: Small, et. al(SPARTAN)
2013:
Docetaxel Cabazitaxel Enzalutamide
Radium 223 Enzalutamide
Tannock et al. de Bono et al. Scher et al. Parker et al. Hussain, et. al (PROSPER)
(TAX 327) (TROPIC) (AFFIRM)
(ALSYMPCA)
2005 2007 2009 2011 2013 2014 2018
2011:
While the greater availability Abiraterone
2013:
2014:
de Bono et al. Enzalutamide
of treatment agents benefits (COU-AA-301) Abiraterone
Ryan et al.
Beer et al.
(PREVAIL)
patients, the multiple 2010:
Sipuleucel-T
(COU-AA-302)
options and sequencing of Kantoff et al.
(IMPACT)
medications complicates
clinical decision-making.
Goals of Therapy in CRPC
PROLONG • Life
• Pain
PREVENT • Complications (e.g. skeletal events)
• Decline in performance status
• Quality of life
PRESERVE
• Performance statusINDEX PATIENT 1 (2017)
Asymptomatic non-metastatic CRPC (M0)
Clinicians should recommend observation with continued androgen deprivation to
patients with non-metastatic CRPC.
(Recommendation; Evidence Level Grade C)
Clinicians may offer treatment with first- generation anti-androgens (flutamide,
bicalutamide and nilutamide) or first-generation androgen synthesis inhibitors
(ketoconazole+steroid) to select patients who are unwilling to accept observation.
(Option; Evidence Level Grade C)
Clinicians should NOT offer systemic chemotherapy or immunotherapy to patients with
outside the context of a clinical trial. (Recommendation; Evidence Level Grade C)DEFINING CRPC IN 3 STEPS
No evidence
nmCRPC
of metastasis
Serum testosterone
Rising PSA levels below
while on ADT 50 ng/dL
Evidence mCRPC
of metastasis
mCRPC=metastatic CRPC; nmCRPC=nonmetastatic CRPC.
Cookson MS, et al; American Urological Association. J Urol. 2015;193(2):491-499. 12nmCRPC IS DEFINED BY BIOCHEMICAL PROGRESSION ONLY—
WITH NO RADIOGRAPHIC PROGRESSION*
CRPC is defined by 1 or more of the following types of disease progression despite castrate levels
of serum testosterone (PSADT CAN HELP RISK STRATIFY PATIENTS WITH
nmCRPC1-3
Faster PSADT is linked to shorter time to metastasis in patients with nmCRPC2*
PSADT (months) Median Time to Metastasis (months)PSADT predicts bone mets or death
• Men with nmCRPC with a
prostate-specific antigen 3.0
doubling time (PSADT) of < 2.8
Relative Risk for Bone
Metastasis or Death
8-10 months are at 2.6
Increasing Risk
2.4
significant risk for 2.2
2.0
metastatic disease and 1.8
prostate cancer–specific 1.6
1.4
death1 20 18 16 14 12 10 8 6 4 2
PSADT (Months)
Shorter PSADT
1. Smith MR, et al. J Clin Oncol. 2013;31:3800-3806.Future Directions: M0 CRPC Many clinical trials are now completing/completed
Newer Therapies: Androgen Pathway Inhibitors
• 1st generation ADT drugs (antiandrogens) target the AR
• 2nd generation ADT drugs (LHRH agonists/antagonists) target LHRH receptors
• 3rd generation drugs have additional mechanisms and are described as
androgen pathway inhibitors (APIs)
• APIs further reduce activation of AR beyond ADT:
– Reduce T levels to almost zero (eg. abiraterone)
– More effectively block AR signaling (eg.
enzalutamide)
• All APIs require concomitant ADT
• APIs initially approved for mCRPC, now also approved in mCSPC and nmCRPC
• Efficacy of APIs demonstrates importance of androgen signaling pathway
across disease continuumANDROGEN TARGETED THERAPY ACROSS THE CONTINUUM OF PROSTATE CANCER 18
Abiraterone Acetate
• Abiraterone inhibits 17 α-hydroxylase/C17,20-lyase
(CYP17)
CYP17 involved in androgen biosynthesis
CYP17 is expressed in testicular, adrenal, and prostatic tumor
tissues
• First approved in 2011 for mCRPC
• Now approved in 2018 for mCSPC
• Concomitant use with prednisone to prevent excess
mineralocorticoid effects
• Food effect requires dosing 1 hour before or
2 hours after a mealAbiraterone Efficacy mCRPC
COU-AA-301 Trial (post-chemotherapy) COU-AA-302 Trial (pre-chemotherapy)
Patients with metastatic CRPC Patients with metastatic CRPC
who had received prior chemotherapy who had not received prior chemotherapy
Median survival (months) 15.8 v 11.2 (placebo) Median survival (months) 34.7 v 30.3 (placebo)
Hazard ratio 0.740 Hazard ratio 0.81
Kaplan-Meier Overall Survival Curves in COU-AA-301 Kaplan Meier Overall Survival Curves in COU-AA-302
100 100
80 80
60 60
% Survival
% Survival
40 40
Placebo
Placebo Placebo
20
Zytiga 20
Abiraterone Abiraterone
0 0
0 3 6 9 12 15 18 21 0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 54 57 60
Time to death, months Months from RandomizationAbiraterone in mCSPC/Newly Diagnosed Metastatic Disease
STAMPEDE Trial LATITUDE Trial
• Improved overall survival by 37% (shown) • Improved overall survival by 38% (shown)
• Improved failure free survival by 71% • Improved PFS by 53%
• Improved symptomatic skeletal events by 55% • Improved PSA progression by 70%
• Improved symptomatic skeletal events by 30%
OS – All Patients OS
HR 0.63 HR 0.62
95% CI 0.52 to 0.76 95% CI 0.51–0.76
P-value 0.00000115
P-value < 0.001Potential Side Effects of Abiraterone
Fatigue Vomiting
Arthralgia URTI
Hypertension Cough and Headache
Nausea Adrenocortical
Edema insufficiency
Hypokalemia Hepatotoxicity
Fluid retention
Hot flush
Diarrhea
Some events relate to concurrent use of prednisoneANDROGEN TARGETED THERAPY ACROSS THE CONTINUUM OF PROSTATE CANCER 22
Enzalutamide
• Enzalutamide is a 3rd generation AR inhibitor
• Has activity at 3 places
•Blocks binding of androgen to AR
•Prevents AR from entering cell nucleus
•Inhibits AR binding to DNA
• First approved in 2012 for mCRPC
• Now approved in 2018 for nmCRPCEnzalutamide Efficacy in mCRPC
Affirm Trial (post- Prevail Trial (pre-
chemotherapy) chemotherapy)
• OS 18.4m for enzalutamide group versus • PFS at 12m: 65% for enzalutamide v
13.6m placebo group 14% placebo (81% risk reduction; HR
• HR for death in enzalutamide group, 0.63 0.19; PPotential Side Effects of Enzalutamide Seizures Edema Ischemic heart disease Fatigue Dyspnea Falls Back pain Musculoskeletal pain Posterior reversible Decreased appetite Weight loss encephalopathy GI disorders, arthralgia Headache syndrome Hot flashes Hypertension URTI Dizziness
ANDROGEN TARGETED THERAPY ACROSS THE CONTINUUM OF PROSTATE CANCER 25
Apalutamide
• Apalutamide is a 3rd generation AR
inhibitor that binds directly to the ligand-
binding domain of the AR
• First approved in 2018 for nmCRPCApalutamide and Enzalutamide in nmCRPC
PROSPER Trial (enzalutamide)
SPARTAN Trial (apalutamide)
• median metastasis-free survival was 36.6m for
• 40.5m v 16.2m for metastasis free survival enzalutamide v 14.7m for placebo group (HR for
• 40.5m v 16.6m to metastasis metastasis or death, 0.29; PPotential Side Effects of Apalutamide
Fatigue Arthralgia
Hypertension Falls and fractures
Rash Hot flush
Hypothyroidism Decreased
Diarrhea appetite
Nausea Peripheral edema
Weight loss SeizuresAPI Conclusions
• Near complete inhibition of AR • Be observant of additional side
activation with APIs produces survival effects
benefit in patients with CRPC and – Hepatotoxicity
CSPC – Falls/fractures
– Seizures
• Continue effective ADT
• Identify drug resistance (ARV-7)
• Additional efficacy seen with APIs
• Personalize therapy for each
reinforces importance of achieving
patient
lowest T by ADT alone
– Selection of initial API
– Lower nadir T in 1st year correlates with
longer time to CRPC and longer CSS
– Modify if necessary
– Patients with higher baseline T derived
greater clinical benefitEffect of treatment on QoL: FACT-P
SPARTAN1 PROSPER2
Caveat: Comparing across studies is problematic. This is
not a head to head comparison.
FACT-P, Functional Assessment of Cancer Therapy–Prostate; 1. Saad F, et al. Poster presented at EAU 2018. abstract 743
HRQoL, health-related quality of life; QoL, quality of life; SD, standard deviation; W, week. 2. Tombal B, et al. Poster presented at EAU 2018. abstract 605The IMAAGEN Study: Effect of Abiraterone Acetate and Prednisone on Prostate Specific Antigen and Radiographic Disease Progression in Patients with Nonmetastatic Castration Resistant Prostate Cancer Charles J. Ryan,*,† E. David Crawford,† Neal D. Shore,† Willie Underwood III, Mary-Ellen Taplin,† Anil Londhe, Peter St. John Francis,† Jennifer Phillips,† Tracy McGowan† and Philip W. Kantoff Results: Of the 131 enrolled patients 44 (34%) remained on treatment with a median followup of 40.0 months. Median age was 72 years (range 48 to 90). Of the patients 82.4% were white and 14.5% were black. Median screening prostate specific antigen was 11.9 ng/dl and median prostate specific antigen doubling time was 3.4 months. Prostate specific antigen was significantly reduced (p
Apalutamide and enzalutamide
extended nmCRPC patients’
median time to metastasis by
roughly 2 years compared to
placebo.1,2 This prolonged
exposure to novel antihormonal
agents prior to metastases adds
complexity to the selection of
initial and subsequent therapies
for treating mCRPC when
patients do develop metastatic
disease
References:
1. Smith MR, Saad F, Chowdhury S, et al. Apalutamide treatment and metastasis-free survival in prostate cancer. N Engl J Med. Published online February 8, 2018. doi:
10.1056/NEJMoa1715546.
2. Hussain M, Fizazi K, Saad F, et al. PROSPER: A phase 3, randomized, double-blind, placebo-controlled study of enzalutamide in men with nonmetastatic, castration-
resistant prostate cancer. Poster presented at: ASCO Genitourinary Cancers Symposium; February 8-10, 2018; San Francisco, CA.
31Antiandrogen Monotherapy
Antiandrogen
Androgen Receptor
AA
AA
AA AA
DHT
T — Testosterone
AA
DHT
AA
DHT
— Dihydrotestosterone
Nucleus
AA
— Antiandrogen
AA
T T DHT
DH
— Androgen Receptor
AA T
SOURCE: Dr. ED CrawfordSide Effects of Anti-Androgen Monotherapy
Gynecomastia
• Flutamide
• Diarrhea, hepatotoxicity (some fatal)
• Nilutamide
• Nausea, dark light accommodation, alcohol
intolerance, hepatotoxicity
• Bicalutamide
• Nausea, diarrhea, constipation, hepatotoxicityConclusions nmCRPC is a heterogeneous disease. nmCRPC patients with PSADT < 10 months are at high risk of developing metastases or death. Apalutamide (2/14/18) and Enzalutamide(7/13/18): now FDA-approved standard for nmCRPC pts. Final analyses pending regarding OS benefit. Additional trials needed regarding sequencing options additional lines of therapy. Additional trials needed regarding implications next generation imaging.
Time to hang it up
Prostate Cancer 2018:
We have seen translational therapy lead
to real, clinically relevant improvements
for patientsYou can also read