MDS Section GG: A Guide for SNF Therapists - RECORDED - LIVE WEBINAR PRESENTED BY: Montero Therapy ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
MDS Section GG:
A Guide for
SNF Therapists
RECORDED – LIVE WEBINAR PRESENTED BY:
MONTERO THERAPY SERVICES
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 1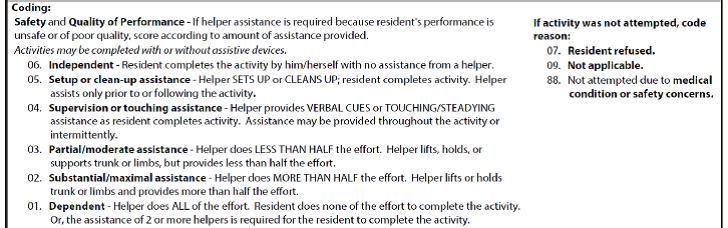
CEU Information
This course has been approved for 1.5 Contact Hours or .15 CEU’s.
Your Certificate of Completion can be printed upon completion of the presentation and quiz.
Your name and license number will be kept on file with Montero Therapy Services for State
Licensing audit purposes. If you have not added your State License/Registration number to your
Account Page, please do so as this is required for CEU credit.
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 3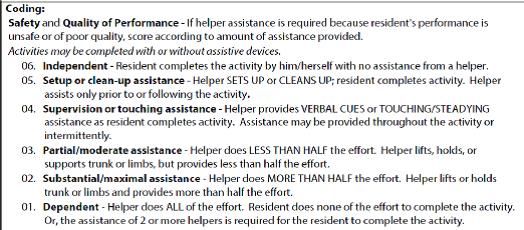
Course Outline
Part 1: History Behind Upcoming Changes, Will Changes Impact All Residents?, How
Will Changes Impact SNF and Therapy?
Part 2: Overview of New Section GG: New Terminology, New Rating Scale, When Is It
Required/Not Required?
Part 3: Self-Care Section: New Questions, Definitions, Coding Scale, Setting Goals and
Case Examples
Part 4: Mobility Section: New Questions, Definitions, Coding Scale, Setting Goals and
Case Examples
Part 5: Recommendations for Implementing Changes Into Your Practice, Q&A
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 5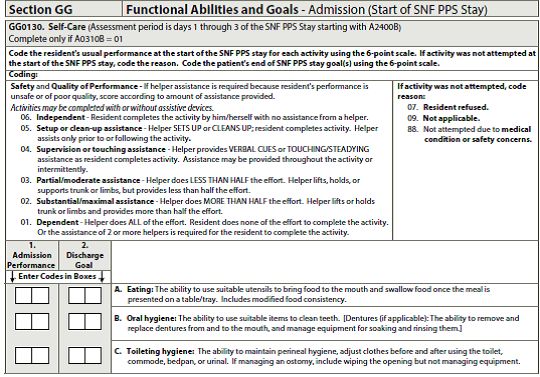
Today’s Objectives
Understand the importance of Section GG and the Therapy’s Role in the MDS in relation to the
transition to Value Based Payment
Recognize when Section GG is required to allow for improved communication and collaboration
with MDS team
Learn accurate rules, coding, documentation and goal setting for Self Care and Mobility Items
Understand when payment penalties will apply due to missing documentation / data in GG
Incorporate Section GG requirements into therapy practice, documentation and rehab
department work flow
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 6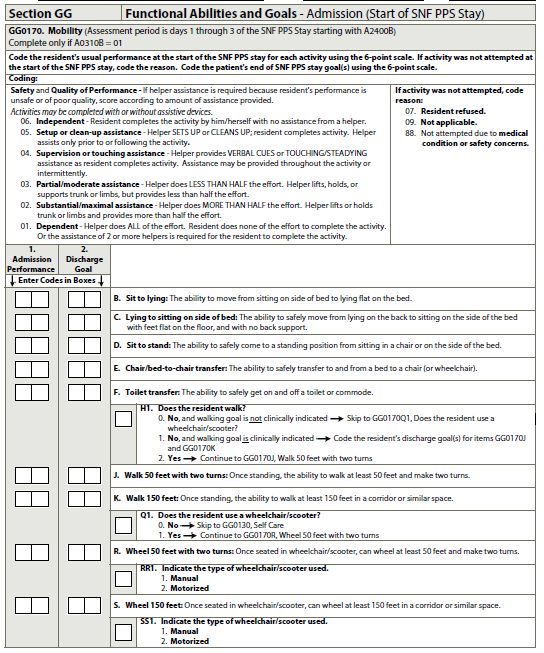
What’s Coming Our Way?
New function-based set of MDS questions that will increase therapy involvement in the MDS
process
These function-based questions are tied to functional outcomes, particularly for short term
rehab residents. Targeting Medicare A residents receiving skilled therapy and/or nursing.
If lack of therapy involvement in the MDS process in the past, NOW is the time to get involved
New/Additional Section GG: Functional Abilities and Goals will be added
*DRAFT RAI Manual was replaced last week with FINAL Manual – This is time sensitive info with expected changes to come in next few weeks
leading up to October 1st due to conflicting information in the Manual with MDS Assessment Instructions
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 7
Why Does This Change Involve Therapy?
How is your current therapy involvement with facility MDS process?
Present Section G: Functional Status does not require therapy input
Questions are populated based on daily documentation from direct caregivers based on resident performance
Nursing takes responsibility of this Section as it is based on resident status 24/7 over 7 day lookback
New Section GG: Functional Abilities and Goals will require input from PT and OT
Coding for Self Care and Mobility Sections are based on an “Assessment”
Responsibility for this Section rests primarily with Therapy and Nursing
MDS coding will be based on an “Assessment” completed in a specific 3 day window.
Involves looking at Therapy and Nursing Data and making a clinical decision as to how to code function
Involves setting goals and predicting functional outcomes for end of Medicare stay/coverage
Goal setting is not new for therapists, but new for the MDS and may be challenging for nursing initially as predicting functional outcomes is
not common
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 8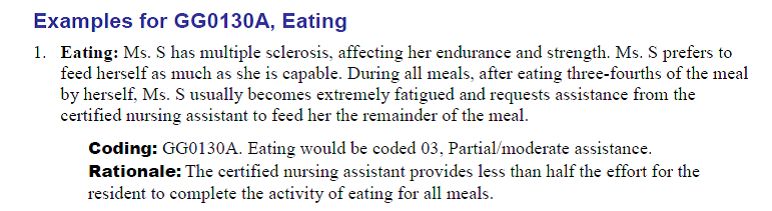
Let’s look at
WHY this change is occurring
and
HOW it will shape the future of SNF’s
…before we look at Section GG in detail
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 9
Why MDS Changes Now?
Change stems from the IMPACT ACT of 2014
Improving Medicare Post-Acute Care Transformation Act of 2014
Link to article explaining IMPACT ACT as it pertains to SNF Therapists
http://www.monterotherapyservices.com/clinical-information/impact-act-snf-therapists-need-know
ACT established a quality reporting program (QRP) for SNF’s (Different from QM’s = Stars)
ACT requires standardization of data between SNF,HH, IRF, LTCH
Develop and implement quality measures and a way to report them
Step toward Value Based Payment
Payment based on Outcomes vs Volume
Step toward Quality Improvement in SNF – Focus on Medicare Beneficiaries
Unify data, improve quality and outcomes through better sharing of info, coordinating care and dc’s
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 10
How GG Came About: QRP
IMPACT ACT required focus on areas of measure and a timeframe to collect the data.
Decision to focus on 3 areas to measure:
1. Falls (% of residents experiencing 1 or more falls with major injury)
2. Skin (% of residents with pressure ulcers that are new or worse)
3. Function (% of residents with an admission and discharge functional assessment (GG) and a
care plan that addresses function)
Needed new questions to measure function – goal to standardize across all setting (IRF, Home
care, SNF, Acute care, etc.)
Section GG as born!
GG will be tied to outcome tracking, progress, change in function, QRP and $$
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 11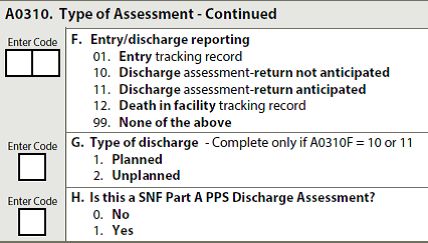
Timelines and Timeframes
Data collection start date is 10/1/16 – for residents admitted on or after 10/1/16
Data will be collected from 10/1/16 through 12/31/16 for “Round 1”
Will be used for FY 2018 payment (Oct 1 2017-Sept 30 2018)
Penalties will be applied to any SNF that has missing data during this time period
MISSING DATA is identified by DASHES on the MDS for certain questions
MISSING DATA during the 3 month collection period will result in a large payment penalty lasting 1 year
80% of all submitted MDS’s need to contain 100% of all data items
Penalty: 2% reduction for SNF Part A revenue (market basket %) for the ENTIRE FY 2018
No penalty for poor outcomes yet
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 12Timelines and Timeframes
Data collection using Section GG will occur at specified intervals:
1. On admission to the SNF
2. On discharge from the SNF
3. On “discharge” from PPS Part A services
Traditional Medicare Part A residents only (not Medicare Advantage)
Tracking outcomes of those primarily admitted for Part A coverage whether plan is to discharge
back to community or stay long term care
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 13A Look at Section G:
Functional Status
Existing Section G: Functional Status before looking
at GG
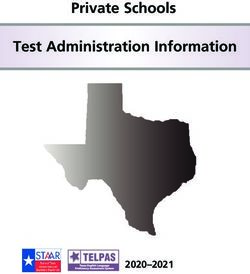
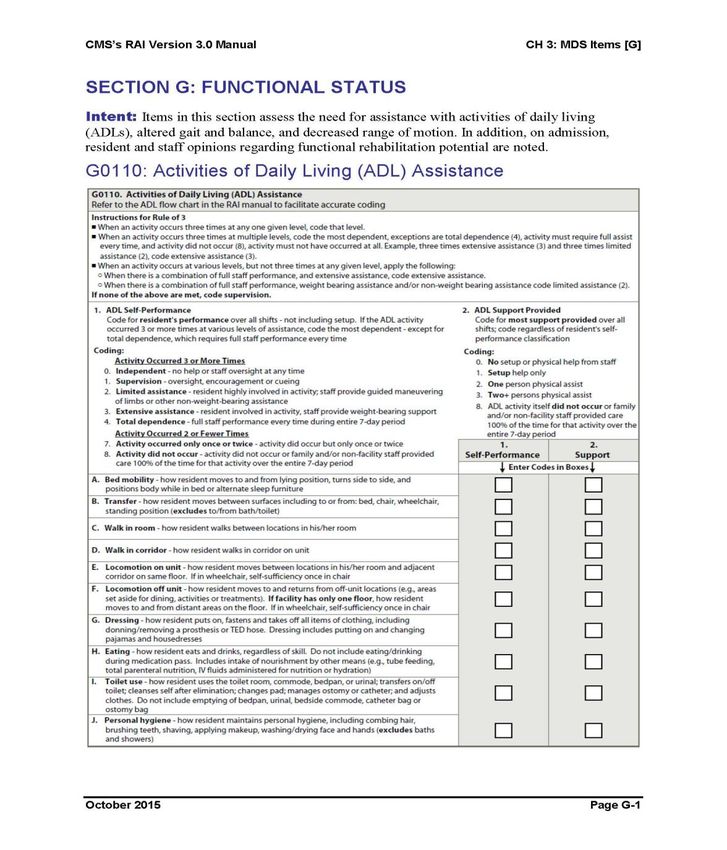
Question G0110: ADL Assistance
See Handout
Filled in by nursing based on actual performance
over 7 day lookback, coded based on Rule of 3
Note the Items
Note the Coding Scale
Important Section = 4 Items Determine ADL Score
for RUG (RUA vs RUB vs RUC) = $$$
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 14Intro to Section GG:
Functional Goals and
Abilities – Self Care
New Section on PPS 5 Day, OBRA DC and on
new Part A PPS Discharge MDS
Questions GG0130: Self Care
See Handout
Will be filled in based on “Assessment” done
in specific 3 day window (1st 3 days of Part A
and last 3 days of Part A)
Note the Items
Note the Coding Scale
Note 2nd Column for Discharge Goal
Important= Performance Section = Missing
data will result in penalty
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 15Intro to Section GG: Functional
Abilities and Goals - Mobility
New Section on PPS 5 Day, OBRA DC
and on new Part A PPS Discharge MDS
Question GG0170 Mobility
See Handout
Will be filled in based on “Assessment”
done in specific 3 day window (1st 3
days of Part A and last 3 days of Part A)
Note the Items
Note the Coding Scale
Note 2nd Column for Discharge Goal
Important= Performance Section =
Missing data will result in penalty
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 16Section G vs GG Comparison
SECTION G= ADL ASSISTANCE SECTION GG=FUNCTIONAL MOBILITY AND GOALS
Determines ADL score Determines QRP status
Populates based on actual performance, not Assessment of data needed to score based on
an assessment resident “usual performance”
7 day look back based on ARD No look back, only 3 day window to assess, not
based on ARD, based on specific days in PPS
On every MDS, regardless of payer cycle
5 point scoring scale, 0=Independent On select MDS’s, for Med A only
6 point scoring scale, 6=Independent
Lack of therapy terminology
Uses therapy terminology (see next slide)
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 17Section G vs GG Scoring Scales
SECTION G: 5 POINT SCALE SECTION GG: 6 POINT SCALE
6 = Independent
0 = Independent
5 = Set-up / Clean-up help
1 = Supervision 4 = Supervision / Touching Assist
2 = Limited Assist 3 = Partial / Moderate Assist (Helper < half)
3 = Extensive Assist 2 = Substantial / Max Assist (Helper > half)
4 = Total Dependence 1 = Dependent (Helper does 100%) OR 2 Assist is
needed (ie: Walk 1 A with w/c follow would be coded Dependent)
7 = Only occurred 1-2 times
9 = Not applicable
8 = Activity did not occur 8 = Not attempted due to medical condition or safety concerns
7 = Resident refused
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 18When Will GG Be Required?
At the start of Medicare Part A coverage (Start=PPS Day 1)
◦ Will be captured on the 5-day PPS MDS
◦ Assessment of status and coded in the 1st 3 days of the Part A stay (won’t go by ARD)
At the end of the Medicare Part A stay/coverage if resident is staying in facility
◦ This a new MDS Assessment specific to this circumstance “Part A PPS Discharge MDS”
◦ Assessment of status and coded in the last 3 days of Part A stay (won’t go by ARD)
When resident is discharged from the facility after a Medicare Part A stay
◦ The OBRA DC MDS will be combined with the Part A PPS Discharge MDS
◦ Section GG will be required when the DC is planned vs unplanned
◦ *** Inconsistencies in DRAFT vs FINAL Manual and PPS MDS Instructions-expect change prior to Oct 1st
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 19RAI Manual Definition of “Discharged”
Already confusion around the word “discharged” between therapy and nursing. Therapy DC
refers to the last day of therapy program, or the day the DC Summary is completed. Nursing
refers to DC as the day the resident left facility
Now RAI Manual redefining “discharge” by correlating “discharge” to the Last Covered Part A
Day (New MDS called “PPS Part A Discharge”) done when resident is “staying”
◦ Discharged……from Medicare Part A = Last covered day
◦ Discharged….from Facility = Typically the day after the last covered day
◦ Discharged….from Therapy= Typically the last day of Part A coverage, but does not need to be
Need to ensure when using term “discharge” that both therapy and nursing are talking about
the same thing
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 20Exceptions – Section GG Not Needed When…
1. Unplanned Discharge from SNF (can’t truly judge functional improvements)
2. DC to acute hospital
3. Stay at SNF is less than 3 days total (Med A coverage is less than 3 days total)
*Does not mean the PPS Part A Discharge Assessment is not needed, only that Section GG
should not be required within that Assessment …..still need to complete falls, skin, etc
*This is the issue in the Final RAI Manual release that may change = GG may be required for
unplanned discharges in the future
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 21GG Will be Needed For: Start of Medicare Part A Stay
When “5-day assessment” is selected as
the type of MDS in Section A, Section
GG will open up
Can be a stand alone 5-day PPS MDS or
an Admission/5-day PPS combined
assessment
Dates entered into A2400 will set the
Admission 3-day assessment windows
Window is always PPS Day 1,2,3 to
review data and complete assessment
May have ARD as Day 8 but GG needs to
be completed by Day 3
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 22GG Will Be Needed For: Part A PPS Discharge
(Resident stays in SNF)
Done when resident is discharged from
Medicare A and stays in facility (cut or BE)
New MDS created for this purpose
Can be combined with other MDS’s
GG will open if “yes” is answered A0310
Dates entered into A2400 will set the
Discharge 3-day assessment window
Window is always last 3 days of Part A stay
for review of data and completion of
assessment
ARD of MDS will match the Medicare End
Date for the DC MDS
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 23GG Will Be Needed For:
Discharge from SNF After
Part A Stay
Existing OBRA DC MDS done when resident is
discharged from SNF
Can be combined with other MDS’s. Required in
some instances.
GG will open if discharge is Planned and if SNF
Part A Discharge is Yes **Currently some
discrepancy in Final Manual released vs
Instructions of Forms ** May change to
included Planned and Unplanned**
Dates entered into A2400 will set the Discharge
3-day assessment window
Window is always last 3 days of Part A stay for
review of data and completion of assessment
Medicare End Date may not match LCD in this
scenario – depends on reason for DC
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 24Medicare Stay End
Date Accuracy
A2400 Medicare Stay End Date NEEDS to be
accurate for proper scoring
RAI Manual - See attached algorithm
Biggest culprit of Short Stay issues
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 25Was the Discharge Planned or Unplanned?
IMPORTANT QUESTION WITH POTENTIAL
PAYMENT IMPLICATIONS
Therapy should have input into this answer
RAI Manual defines Unplanned DC
Unplanned is MORE than discharges to the
hospital or leaving AMA. It also includes a
discharge from facility where the resident
decided to leave prior to the date recommended
by therapy/team.
When coded “unplanned” the GG data will be ** Keep an eye out for more
excluded from the QRP outcomes discussion on this – Final RAI
Manual release has discrepancy for
Not fair to include DC performance outcomes if
resident is leaving before therapy is complete GG completion ** Clarification
likely in next few weeks
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 26GG0130: SELF CARE
1. Review of MDS questions / item set definitions
2. Coding Scale
3. Admission Performance and Discharge Goal
4. Discharge Performance
5. Case Examples
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 27GG0130: SELF
CARE
Eating
◦ Function of food to mouth
◦ Does not include tube feeding like
Section G
Oral Hygiene
◦ Specific to oral hygiene, including
management of dentures
◦ Section G “Personal Hygiene”
Toileting Hygiene
◦ Similar to Section G “Toilet Use”
◦ Excludes transfers to toilet (G)
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 28Coding Scale vs Therapy Documentation
Intermittent Supervision,
Supervision, Stand By
Guard, Contact Guard,
Cues Only
Min Assist, Mod Assist of 1
Max Assist of 1
Total Assist, Dependent, or
Assist x 2 at any level
Important for therapist to know MDS definitions of assist level (and tasks) even if they will
have no contact with MDS. Therapy will be discussing resident status with MDS nurse and
understanding of terminology is critical.
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 29“Usual Performance”
Coding for GG is based on “Usual Performance”
New MDS Term
“Not best”
“Not worst”
Lacks objectivity!
Need to have documentation to back up how GG is coded
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 30Admission Performance
& DC Goal
Admission Performance and Discharge
Goal:
◦ Assessment completed on PPS Day 1, 2 or 3
◦ Usual Performance
◦ DC Goal refers to projected status / goal
upon completion of Medicare A
stay/coverage
◦ Keep in mind resident may not have 100
days and may need days beyond Medicare
Days to reach full potential
◦ Ensure DC Goal correlates with Therapy Goal
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 31Some Good News….
The requirement for DC Goal setting is at least 1 Self Care OR Mobility goal
must be coded on 5 day MDS. Do not need to set goals for each item, even if
goals exist in therapy documentation or care plan.
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 32More Good News….
Only place in GG it is OK to have DASHES - No Penalty in DC GOAL SECTION
…NEVER DASHES in PERFORMANCE SECTION
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 33Admission Case Example #1 - EATING
03 04
On the Admission Assessment, 03 (Mod Assist) was coded based on review of Day 1 and Day 2
documentation. OT Eval was completed on Day 2 and found that resident had potential to feed self
full meal independently with occasional steadying, with addition of AFE and OT program. DC Goal
of 04 was selected and matched Long Term Goal on OT Initial Evaluation.
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 34Discharge Case Example #1 - EATING
On the Admission Assessment, 03 (Mod Assist) was coded.
OT Eval was completed on Day 2 and found that resident
had potential to feed self full meal independently with
intermittent steadying with addition of AFE and OT program.
DC Goal of 04 was selected and matched Long Term Goal on
OT Initial Evaluation. Upon completion of Occupational
Therapy and 30 days of Medicare Part A, the resident is
being cut from Part A due to no further skilled needs. Upon
DC the resident was able to feed herself independently with
intermittent adjustment and steadying of AFE by staff.
04
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 35Admission Case Example #2 - EATING
88 - -
On the Admission Assessment, 88 was coded. Codes 07, 09 and 88 are not
allowed in the DC Goal box. Dashes are allowed in this section without
penalty. If SLP was going to work on a return to PO and had goals set for
eating, a DC Goal could be coded here.
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 36GG0170: MOBILITY
1. Review of MDS questions / item set definitions
2. Coding Scale
3. Admission Performance and Discharge Goal
4. Discharge Performance
5. Case Examples
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 37GG0170:
MOBILITY
Sit to lying and Lying to sitting:
◦ Includes full movement in supine – sit
and unsupported sitting
Chair/bed-to-chair transfer:
◦ Includes standing lift and mechanical
lifts
Toilet Transfer:
◦ Includes bedside commode
Walk/Wheel 50 feet with 2 turns:
◦ Turns are 90 degrees any direction
◦ If resident walks and wheels, both
should be coded
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 38Coding Scale vs Therapy Documentation
Intermittent Supervision,
Supervision, Stand By
Guard, Contact Guard,
Cues Only
Min Assist, Mod Assist of 1
Max Assist of 1
Total Assist, Dependent, or
Assist x 2 at any level
SAME CODING SCALE FOR SELF CARE AND MOBILITY
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 39Admission Performance
& DC Goal
Admission Performance and Discharge
Goal:
◦ Assessment completed on PPS Day 1, 2 or 3
◦ Usual Performance
◦ DC Goal refers to projected status / goal
upon completion of Medicare A
stay/coverage
◦ Keep in mind resident may not have 100
days and may need days beyond Medicare
Days to reach full potential
◦ Ensure DC Goal correlates with Therapy Goal
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 40REMEMBER….
The requirement for DC Goal setting is at least 1 Self Care OR Mobility goal
must be coded on 5 day MDS. Do not need to set goals for each item, even if
goals exist in therapy documentation or care plan.
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 41REMEMBER….
Only place in GG it is OK to have DASHES - No Penalty in DC GOAL SECTION
…NEVER DASHES in PERFORMANCE SECTION
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 42Admission Case Example #1 - Chair Transfer
04 06
On the Admission Assessment, 04 was coded based on review of Day 1 and Day 2 documentation.
PT Eval was completed on Day 2 and found that resident had potential to progress to prior level of
function - independent. DC Goal of 06 was selected and matched Long Term Goal on PT Initial
Evaluation.
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 43Discharge Case Example #4 - Chair Transfer
On the Admission Assessment, 04 was coded based on review of
Day 1 and Day 2 documentation. PT Eval was completed on Day 2
and found that resident had potential to prior level of function -
independent. DC Goal of 06 was selected and matched Long Term
Goal on PT Initial Evaluation.
Upon DC Assessment review on the Last Med A Day (Last Day of
Therapy), a review of therapy and nursing documentation reveals
the resident is independent with Bed-Chair transfers.
06
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 44Admission Case Example #2 - Toilet Transfer
88 03
On the Admission Assessment, 88 based on review of Day 1 and Day 2 documentation. OT Eval was
completed on Day 2 and found that resident had potential to progress to Min Assist after acute
medical issue resolved. DC Goal of 03 was selected and matched Long Term Goal on OT Initial
Evaluation.
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 45Admission Case Example #3 - Walk 50’ with 2 Turns
01 - -
On the Admission Assessment, 01 was coded based on review of Day 1 and Day 2 documentation.
PT Eval was completed on Day 2 and found that resident had potential to progress to prior level of
function - independent. This was reflected in PT documentation. Team chose not to set DC Goal in
this area as DC Goals were set in 2 other areas.
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 46Documentation to Support GG
Performance codes need to be backed up by documentation
CMS / RAI Manual will not dictate how, will be up to each facility
Surveyor needs to be able to come up with same coding
GG is tied to QRP and could be subject to manipulation
Ensure your SNF has a MDS Policy and Procedure in place that outlines how the SNF is handling
documentation and coding of Admission and Discharge Assessments
Include specifics on Section GG
MDS focused surveys
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 47Documentation to Support GG
Section GG Admission and Discharge Performance sections are “Assessments” for the MDS vs a look-
back calculation
Intent is to look at more than 1 data source to decide (Therapy, Nursing, etc)
◦ Not intended to use C.N.A. documentation as main source – like Section G
Need to record date of Assessment
◦ If Admission Assessment can be done PPS Day 1, Day 2 or Day 3 and you choose Day 2, the resident’s
performance on Day 3 is not factored into coding decision
◦ Can sign MDS Section GG date it is done (similar to BIMS)
◦ Can document Assessment and scoring elsewhere and enter into MDS when coding other sections after ARD
(as long as you can reproduce document)
DC Goal can be done by 1 discipline, can be in Care Plan or Therapy Notes
◦ Ensure DC Goal on MDS matches Care Plan goal and/or Therapy goal
◦ Do not need to rewrite goals somewhere else
**See Sample Data Collection Tool in Handouts
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 48Sample Data
Collection Tool
*See handout for full size
sample
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 49WHO Should Code GG? Therapy? Nursing?
RAI Manual will not dictate who, only that Federal and State regulations are followed
Keep in mind….this is considered an “Assessment”
Should be a team approach to decide based on the sharing of information from each discipline
and review of written record
◦ Can keep it simple and have a team discussion for those in 3 –day assessment windows at morning
huddle – designate 1 person to write an “Assessment Note” with decision for coding and why
◦ Tough for Friday and Saturday admissions
How each SNF handles this should be based on individual circumstances
◦ Goal is to have 1 person oversee GG to be the “gatekeeper” for consistency, inappropriate dashes, etc
◦ Typically should be the MDS Nurse to sign off on Section GG, though Therapist would not be out of the
question
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 50The Flow of GG
Sample Scenario
New Medicare Part A Admission arrives on 10/3/16
◦ Day 1: PT Evaluation
◦ Day 2: OT Evaluation
◦ Day 3: Last day Admission Performance Assessment & Discharge Goals can be completed on the MDS
◦ Therapy and nursing review current documentation and determine “usual performance” for GG
◦ DC Goal is set in 1 area of Mobility based on PT Evaluation Goals
Resident receives skilled therapy and nursing services
Therapy, Social Worker and resident discuss status and projected DC date based on progress. Date is
selected for the following week for return home.
Team sets reminder of 3 day Assessment window for Discharge
Team reviews documentation and determines “usual performance.” Assessment completed on Last
Covered Medicare A Day and recorded on MDS
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 51Food for Thought….
CMS will begin acquiring data on Function at the Start and End of Medicare Part A stays
◦ Track status at the start and compare to end
◦ Was progress achieved? Was it the progress that was predicted?
◦ Models Functional Limitation Reporting (G-Codes) for Part B
What if….
◦ What if 100 days of Medicare Part A are used, a Rehab RUG was maintained the whole time, and there is no
difference in Self Care / Mobility from the Admission Assessment to Discharge?
◦ What if there was minimal progress noted in Performance, and the RUG was RUB the whole time?
CMS can see if progress, or lack of, in multiple functional areas was made just by looking at MDS
coding
◦ Will this be cause for denial? Or trigger more/less ADR’s?
We now have multiple MDS sections that have data collected for Self Care, Mobility
◦ Go110 ADL’s, G0300 Balance during transfers and walking, GG
◦ Will they match???? Should they???
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 52Key Points to Remember….
Section GG on pertains to Medicare Part A residents (for now)
For admissions, decision on coding for GG, “Assessment,” must be done by PPS day 3
For residents discharged from Part A, whether they are staying LTC or leaving, GG “Assessment” must be done within
the last 3 covered days of the stay.
For now, unplanned discharges are excluded from GG, though this may change prior to Oct 1st
NEVER DASHES in Admission or DC Performance Sections
OK DASHES in DC Goal Section
Make sure you have AT LEAST 1 DC GOAL in any area of function – only need 1 for now
Important for therapy to understand requirements of Section GG and be involved in MDS coding as FUNCTIONAL
OUTCOMES are tied to Rehab Progress
Want GG to reflect therapy documentation to show true outcomes…what if MDS does not show progress but therapy
documentation does??
Payment methodology structure headed for change…therapists should be ahead of the curve!
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 53References: Use Your PDF for Live Links
Sources in addition to the hyperlinks provided throughout the material include:
www.cms.gov
AANAC.ORG
RAI Manual – Final – Released 8/25/16 https://downloads.cms.gov/files/MDS-30-RAI-Manual-V114-October-2016.pdf
IMPACT ACT Article: http://www.monterotherapyservices.com/clinical-information/impact-act-snf-therapists-need-know
MDS SECTION GG Article: http://www.monterotherapyservices.com/clinical-information/mds-changes-impacting-snf-
therapists-section-gg
RAI State Coordinator List (updated 8/25/16) – can email to ask specific questions as needed
Section GG: Four-Part CMS YouTube Training Video Series (8/16)
1. https://www.youtube.com/watch?v=pNgQ3OSaxYg
2. https://www.youtube.com/watch?v=M1JdQxjNOqE
3. https://www.youtube.com/watch?v=ok3U2-mQymk
4. https://www.youtube.com/watch?v=oRmMT_uYS8Y
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 54Can’t think of a question now? Email us later at
MemberSupport@MonteroTherapyServices.com. All
our courses include Q&A on the material as needed.
Individual Members.. You can ask a question any time…Visit our
JustAsk! Q&A Forum
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 55Continuing Education
Program Evaluation
Click here to complete online now: www.MonteroTherapyServices.com/course-evaluation
Title: MDS Section GG: Guide for SNF Therapists
Location: Live Webinar
Date Course Completed: September 1, 2016 12:00-1:15 EST
Presenter(s): Dolores Montero, PT,DPT,GCS, RAC-CT
Please rate the continuing education presentation you have just completed.
I. Please rate the following areas:
A. Course Content: Excellent____ Good____ Fair____ Poor____
B. Organization of the material: Excellent____ Good____ Fair____ Poor____
C. Objectives of course were met: Excellent____ Good____ Fair____ Poor____
D. Level of difficulty was appropriate: Excellent____ Good____ Fair____ Poor____
E. Likelihood material will enhance my skills: Excellent____ Good____ Fair____ Poor____
F. Knowledge and effectiveness of presenter: Excellent____ Good____ Fair____ Poor____
II. Did this course meet your expectations? If no, why not?
_____________________________________________________________________________________________
III. Suggestions for future topics / Comments:
_____________________________________________________________________________________________
Please return your responses so we can continue to improve our service to you.
Fax (844) 582-8326, email MemberSupport@MonteroTherapyServices.com
Or complete online @ http://www.monterotherapyservices.com/course-evaluation
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 56Disclaimer
This information for this presentation was current at the time it was published. Source
documents and links are provided. Due to the frequent change in Medicare policy, participants
should verify policy change prior to implementing information into practice.
This presentation was prepared to provide general information on the subject material.
Participants are encouraged to further review the specific statutes, regulations and other
materials for a full understanding of how to utilize this information in practice.
Montero Therapy Services is available for consulting on specific practice issues or concerns
related to this or any other material.
COPYRIGHT 2016 WWW.MONTEROTHERAPYSERVICES.COM 59You can also read