Mechanisms of HDL lowering in insulin resistant, hypertriglyceridemic states: the combined effect of HDL triglyceride enrichment and elevated ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Clinical Biochemistry 36 (2003) 421– 429
Mechanisms of HDL lowering in insulin resistant, hypertriglyceridemic
states: the combined effect of HDL triglyceride enrichment and
elevated hepatic lipase activity
Shirya Rashid, Ph.D., Takehiko Watanabe, M.D., Ph.D.,
Taro Sakaue, MD, Gary F. Lewis, M.D., FRCPC*
From the Department of Medicine, Division of Endocrinology and the Department of Physiology, University of Toronto, Toronto, Ontario, Canada
Received 15 January 2003; received in revised form 9 May 2003; accepted 13 May 2003
Abstract
Hypertriglyceridemia, low plasma concentrations of high density lipoproteins (HDL) and qualitative changes in low density lipoproteins
(LDL) comprise the typical dyslipidemia of insulin resistant states and type 2 diabetes. Although isolated low plasma HDL-cholesterol
(HDL-c) and apolipoprotein A-I (apo A-I, the major apolipoprotein component of HDL) can occur in the absence of hypertriglyceridemia
or any other features of insulin resistance, the majority of cases in which HDL-c is low are closely linked with other clinical features of
insulin resistance and hypertriglyceridemia. We and others have postulated that triglyceride enrichment of HDL particles secondary to
enhanced CETP-mediated exchange of triglycerides and cholesteryl ester between HDL and triglyceride-rich lipoproteins, combined with
the lipolytic action of hepatic lipase (HL), are driving forces in the reduction of plasma HDL-c and apoA-I plasma concentrations. The
present review focuses on these metabolic alterations in insulin resistant states and their important contributions to the reduction of HDL-c
and HDL-apoA-I plasma concentrations. © 2003 The Canadian Society of Clinical Chemists. All rights reserved.
Keywords: Hepatic lipase; High density lipoprotein (HDL); Apolipoprotein A-I; Type 2 diabetes; Insulin resistance syndrome; Metabolic syndrome;
Hypertriglyceridemia; Atherosclerotic cardiovascular disease; Cholesteryl ester transfer protein
Approximately one quarter of the North American pop- highly predictive of insulin resistance than the presence of
ulation has evidence of insulin resistance [1]. Resistance to abdominal obesity [7]. Furthermore, the high TG/low
the normal physiologic actions of insulin (i.e., insulin resis- HDL-c lipid phenotype is highly atherogenic in the setting
tance), with its associated metabolic, inflammatory and co- of insulin resistance [4 – 6,8].
agulation abnormalities, is a major risk factor for Type 2 Low plasma concentrations of HDL-c and its major pro-
diabetes as well as atherosclerotic cardiovascular disease tein component, apolipoprotein A-I (apo A-I), are particu-
(ASCD) [2,3]. The typical dyslipidemia that is associated larly powerful, independent risk factors for ASCD [9 –11].
with insulin resistance is felt to play an important, although Consequently, there is great interest in determining the
not exclusive, role in the accelerated ASCD in affected mechanisms responsible for reduced HDL-c and apo A-I
individuals [4 – 6]. Hypertriglyceridemia, low plasma con- plasma concentrations, particularly in insulin resistant
centrations of high density lipoproteins (HDL) and qualita- states. Putative cardioprotective functions of HDL particles
tive changes in low density lipoproteins (LDL) comprise the include a direct inhibition of pro-atherogenic processes at
typical dyslipidemia of insulin resistant states [4 – 6]. In fact, the arterial wall, including inhibition of LDL oxidation,
a high triglyceride (TG)/HDL-cholesterol (HDL-c) ratio is prevention of monocyte adhesion and chemotaxis, reduction
felt by some investigators to be the single most character- in macrophage formation, and inhibition of endothelial dys-
istic feature of the insulin resistance syndrome, even more function and apoptosis [12]. The protective role of HDL
against ASCD, however, is most widely attributed to its key
* Corresponding author. Tel.: ⫹1-416-340-4270; fax: ⫹1-416-340-
role in mediating the reverse cholesterol transport from
3314. peripheral tissues to the liver for either reutilization or bile
E-mail address: gary.lewis@uhn.on.ca (G.F. Lewis). acid synthesis [13]; in this manner, HDL particles are be-
0009-9120/03/$ – see front matter © 2003 The Canadian Society of Clinical Chemists. All rights reserved.
doi:10.1016/S0009-9120(03)00078-X422 S. Rashid et al. / Clinical Biochemistry 36 (2003) 421– 429
lieved to prevent the accumulation of cholesterol, foam cause-and-effect relationship, but they do suggest that the
cells, and fatty lesions in cells of the arterial intima [13]. variables are closely linked either genetically, metabolically
Although isolated low plasma HDL-c can occur in the or in some other ill-defined manner.
absence of hypertriglyceridemia or any other features of In addition to the above clinical observations, further
insulin resistance (associated with abdominal obesity, glu- evidence that the metabolism of TG-rich lipoproteins and
cose intolerance or Type 2 diabetes), it is a less prevalent HDL are closely linked has been provided by physiologic
clinical occurrence and may be attributed to the presence of studies that have investigated the regulation of HDL metab-
rare genetic disorders that affect HDL metabolism [14,15]. olism. These studies have shown the existence of dynamic
A few examples in which low plasma HDL-c and apoA-I interactions between TG-rich lipoproteins and HDL in
concentrations do not seem to occur as a direct consequence plasma and demonstrated that TG-rich lipoproteins impact
of insulin resistance, include defects in the uptake of free on the metabolism of HDL in at least two important ways.
cholesterol from peripheral cells (mutations in ABC-A1 are One point of interaction is mediated by the lipolytic enzyme
one such example) [16], defects in the esterification of free lipoprotein lipase (LPL) [20,34]. The lipolysis of TG-rich
cholesterol (LCAT deficiency) [15], mutations of lipopro- lipoproteins by LPL results in the formation of redundant
tein lipase or mutations in the apoA-I gene that may either surface materials, which are then transferred to HDL parti-
affect the synthesis or catabolism of HDL [17,18]. The cles, thereby impacting on the maturation of HDL in the
majority of cases of low HDL-c, however, are closely linked circulation and ultimately on plasma HDL lipid and protein
with other clinical features of insulin resistance and hyper- concentrations [34,35]. Second, cholesteryl ester transfer
triglyceridemia [10]. We and other investigators have pos- protein (CETP) mediates a heteroexchange of core neutral
tulated that hypertriglyceridemia, which is a frequent oc- lipids between lipoprotein classes and between lipoproteins
currence in insulin resistant conditions, combined with the and various tissues. In particular, CETP mediates the trans-
action of hepatic lipase (HL), are driving forces in the fer of TGs from TG-rich lipoproteins to HDL (particularly
reduction of HDL-c and apoA-I plasma concentrations HDL2A) in exchange for HDL cholesteryl ester (CE)
[8,19,20]. The present review focuses on these metabolic [36,37]. This produces HDL particles that are TG-enriched
alterations in insulin resistant states and their important within the particle core, and also relatively CE depleted
contributions to the reduction of HDL-c and HDL-apoA-I [38]. These two processes may impact both HDL-c as well
plasma concentrations. as apoA-I plasma concentrations as discussed further below.
Hypertriglyceridemia in Insulin Resistant States and Reduced LPL Activity and Enhanced Transfer of
the Interaction between Triglyceride (TG)-rich Neutral Lipids contribute to the Lowering of Plasma
Lipoproteins and HDL HDL-c in Insulin Resistant, Hypertriglyceridemic
States
Hypertriglyceridemia is perhaps the most common lipid
abnormality in insulin resistance and is primarily due to LPL activity measured in adipose tissue biopsies indicate
increased production of very low density (VLDL) particles that this enzymes may in fact be elevated in obese, hyper-
[21,22]. In addition there is a well described elevation of insulinemic but insulin resistant individuals, whereas the
chylomicrons and VLDL in the postprandial state, in large normal insulin-mediated stimulation of LPL activity, such
part secondary to competition for a saturable removal path- as occurs in the postprandial state, has been shown to be
way for these TG-rich lipoproteins [23–25]. More recently blunted in this condition [39,40]. In Type 2 diabetes, par-
we have described elevated production rates of intestinally ticularly when glycemic control is poor and in patients who
derived lipoproteins in insulin resistance, which may also are relatively insulin deficient, LPL activity may be reduced
contribute to the hypertriglyceridemia [26]. Detailed discus- [41]. Humans with either homo- or heterozygous LPL de-
sion of the mechanisms of the hypertriglyceridemia in in- ficiency have low plasma HDL concentrations. The reduc-
sulin resistance is beyond the scope of this review. Inter- tion in LPL activity could reduce the maturation of HDL
ested readers are referred to three recent reviews on this particles that occurs as a result of the shedding of lipids and
topic [21,22,27]. apolipoproteins from the surface of TG-rich lipoproteins
Several investigators have proposed that the lowering of during LPL-mediated lipolysis [42]. Thus, this theory holds
HDL levels observed in insulin resistant states is largely a that HDL production is reduced in hypertriglyceridemic
consequence of the fasting and postprandial hypertriglycer- states as a result of the reduced LPL activity.
idemia commonly occurring in these states [19,28 –30]. Sig- Kinetic studies in humans, however, have shown that
nificant negative correlations have in fact been demon- hypertriglyceridemic individuals with low HDL-c have a
strated between postprandial plasma TG excursion, HDL significantly increased fractional catabolic rate (FCR) of
TG content and fasting plasma HDL-c and apoA-1 concen- apoA-I but no reduction in apoA-1 production rates, in
trations in humans [8,28,31–33]. Correlations or inverse comparison with normolipidemic subjects [43– 47]. Simi-
correlations between variables, of course, do not prove a larly, in individuals with type 2 diabetes, hypertriglyceride-S. Rashid et al. / Clinical Biochemistry 36 (2003) 421– 429 423
mia was shown to be associated with increased HDL FCR numbers and cholesterol content, potentially by predispos-
[48]. In contrast, the apoA-I FCR in a group of subjects with ing HDL particles to enhanced catabolism [4,8,34,36,56].
low HDL-c levels, but with normal TG concentrations, was Studies have specifically examined the effect of alter-
found not to differ significantly from control subjects [49]. ations in HDL TG content on HDL catabolism. In a series
In hypertriglyceridemic individuals, the increase in apoA-I of in vitro experiments, Liang et al. found that incubation of
FCR, and not an alteration in apoA-I production, demon- HDL with CETP and VLDL (to TG-enrich HDL) produced
strated significant positive correlations with the level of a time-dependent dissociation of apoA-I from HDL [57].
plasma TG, and strong negative correlations with HDL-c We further investigated whether TG enrichment of HDL
and apoA-I concentrations [43,50,51]. directly increases HDL catabolism in vivo. In healthy male
Since the major abnormality in HDL metabolism in hyper- subjects, the clearance of apoA-I associated with HDL iso-
triglyceridemic states (which are frequently associated with lated from the fasting state was compared to the clearance of
underlying insulin resistance) is an enhancement in the clear- HDL that had been TG enriched in vivo using a synthetic
ance of HDL apoA-I rather than a reduction in HDL apoA-I TG emulsion (intralipid) [58]. We observed that a mean
production, reduced production of nascent HDL from a defec- twofold physiological increase in the TG content of HDL
tive LPL-mediated lipolysis of TG-rich lipoproteins, while (from ⬃3% to ⬃6% of HDL mass) resulted in a significant,
perhaps playing a role, is not likely to be the major mechanism 26% increase in the FCR of HDL apoA-I [58]. Furthermore,
whereby HDL-c and apoA-I plasma concentrations are low- the increase in HDL TG content correlated strongly and
ered in hypertriglyceridemic, insulin resistant states. significantly with the increase in apoA-I catabolism [58]. In
An alternate theory accounting for reduced HDL-c and contrast, other changes in HDL composition, similar to
HDL apoA-I plasma concentrations in hypertriglyceridemic, those observed after a high fat meal (changes in phospho-
insulin resistant states include a major role for the ultimate lipids, cholesterol, apoE, apoC-III, and apoC-I), were not
metabolic consequence of the hetero-exchange of TG and CE strongly associated with changes in HDL apoA-I FCR [58].
between TG-rich lipoproteins and HDL that is mediated by Overall, this study demonstrated in humans that TG enrich-
CETP. The mass transfer of these neutral lipids is highly ment of HDL directly increases the catabolism of HDL
dependent on the concentration (pool size) of TG-rich lipopro- apoA-I, particularly in LpA-I particles [58].
teins in the plasma [36,37,52]. Hypertriglyceridemia that oc- A potential mechanism for the enhanced catabolism of
curs in insulin resistance and type 2 diabetes has been shown TG-enriched HDL was provided by Sparks et al. [59]. In a
to be associated with greater transfer of TG from the expanded series of in vitro experiments with reconstituted LpA-I par-
pool of TG-rich lipoproteins (primarily large, CE enriched ticles, the investigators calculated that a decrease in the
VLDL1 particles) into HDL particles, and a concomitant in- CE/TG ratio in LpA-I particles (as when the particles are
crease in the transfer of CE out of HDL into the TG-rich TG-enriched) decreases the thermodynamic stability and
lipoproteins [53,54]. Thus, such a CETP-mediated lipid ex- structural integrity of the particles [59]. This would tend to
change process can per se reduce plasma HDL-c concentra- alter the surface charge and structure of apoA-I, making it
tions, but not apoA-I concentrations, unless it is coupled with more likely to dissociate from the particle [59]. The authors
an additional process that increases the loss of apoA-I from the therefore contended that the dissociation of apoA-I from
TG-rich/CE-depleted particles or increases HDL holoparticle LpA-I particles having a low CE/TG ratio, as when the
uptake by tissues. Thus, CETP-mediated removal of CE from particles are TG-enriched, would be enhanced in hypertri-
HDL particles cannot in and of itself explain the reduction in glyceridemic states [59].
HDL protein (apoA-I) levels and enhanced clearance of HDL Whether this mechanism also applies specifically to hu-
apoA-I that has been observed in hypertriglyceridemic hu- man TG-rich HDL in vivo remains to be determined.
mans, nor is it likely to entirely explain the reduction of HDL-c
in this condition. Instead, as several investigators have pro-
posed, it may be that the compositional changes induced in Does TG Enrichment of HDL Per SE Enhance HDL
HDL by CETP may predispose HDL to greater subsequent Catabolism in the Absence of Lipolytic Modification of
catabolism, which can better explain the reduction in HDL-c the Particles?
and apoA-I plasma concentrations [4,20,34,55].
Overall, the above findings indicated that variations in
the TG content of HDL can have a significant impact on
The Effect of TG Enrichment of HDL on HDL HDL catabolism. The question still remained, however, as
Particle Catabolism to whether TG enrichment of HDL per se destabilizes HDL
particles sufficiently to enhance the subsequent catabolism
We and other investigators have postulated that the in- of HDL in vivo or if TG enrichment merely predisposes
crease in HDL core TG content that occurs as a result of HDL to greater interaction with, and remodelling by,
increased neutral lipid exchange between TG-rich lipopro- plasma factors which regulate HDL metabolism –that is
teins and HDL in hypertriglyceridemic, insulin resistant with intravascular lipolytic enzymes (or lipases). Indeed, in
states plays an important role in the decline in HDL particle the study of Lamarche et al. (described above) in which the424 S. Rashid et al. / Clinical Biochemistry 36 (2003) 421– 429
FCR of TG-rich vs. fasting HDL was examined in humans, enrichment of the particles, in the absence of HL activity, is
we surmised that a sufficient quantity of lipases would be not sufficient per se to enhance HDL particle clearance [61].
expected to be present in the normal human study subjects
to modify and potentially enhance the metabolism of the
TG-rich HDL injected in vivo [58]. Support for this view Increased postheparin plasma HL Activity is an
can also be found in a study by Horowitz et al. using Integral Feature of Insulin Resistant States and Plays
isolated perfused rabbit kidneys (the kidney is a major site an Important Role in the Catabolism of TG-rich HDL
of HDL apoA-I degradation and catabolism in vivo) [45].
The investigators showed that the renal clearance of HDL There are at least three primary lipases tethered to the
apoA-I was not significantly enhanced unless the TG en- vascular endothelium and active against plasma lipoproteins
riched HDL was subsequently treated with partially purified –LPL, HL, and endothelial lipase (EL) [62]. The in vitro
lipases [45]. evidence to date suggests that HL plays an important role in
Most in vitro studies on the subject also support the idea promoting the catabolism of the TG-rich HDL prevalent in
that both TG enrichment of HDL and hydrolysis by lipolytic hypertriglyceridemic, insulin resistant states [60,63]. Al-
enzymes are required to destabilise HDL particles to a though EL has been shown to have a major effect in altering
significant extent. Clay et al., for example, compared the HDL plasma concentrations by enhancing its catabolism,
composition of HDL isolated from normolipidemic human since EL is predominantly a phospholipase and has minimal
plasma with HDL isolated from plasma that had been incu- TG lipase activity [64], it is unlikely to be the primary lipase
bated with CETP and VLDL (to TG enrich the HDL) in the mediating the enhanced catabolism of TG enriched HDL,
presence and absence of the lipolytic enzyme hepatic lipase although this has not specifically been examined. Con-
(HL) [60]. Incubation of human plasma with CETP and versely, incubation of TG enriched HDL with either LPL or
VLDL resulted in a marked increase in HDL TG, a decline HL in vitro have both been shown to mediate a reduction in
in HDL CE, but only minimal changes in apoA-I content vs. HDL size and a loss of apoA-I from HDL [60,65]. In
contrast to LPL, however, HL has a higher affinity for HDL
HDL isolated from plasma alone [60]. The addition of HL
than for VLDL or chylomicrons [66,67]. Furthermore,
to the incubation mixture, however, resulted in loss of
among the different subfractions of HDL, HL has been
virtually all of the acquired TG, a further loss in CE, and a
shown in vitro to selectively hydrolyze the relatively TG-
major loss of apoA-I from HDL (⬃30%) [60].
rich HDL2 and HDL1 subfractions [68,69].
We wished to further determine the roles of HDL TG
HL is a 476 amino acid glycoprotein lipolytic enzyme
enrichment and lipolytic modification of the particle on
that is synthesized by hepatocytes [70,71]. It is found lo-
HDL catabolism in an in vivo setting. We investigated
calized at the surface of liver sinusoidal capillaries anchored
whether TG enrichment of HDL per se is sufficient to
by heparan sulfate proteoglycans [72,73]. In terms of its
enhance HDL catabolism, as some investigators have con- regulation, HL appears to be modulated by several different
tended, or whether this alteration in particle composition genetic and environmental factors such as gender and poly-
must also be accompanied by substantial lipolysis of HDL morphisms in the HL promoter (LIPC) locus [74]. More-
lipids [61]. We specifically compared the metabolic clear- over, as demonstrated in numerous studies, an elevation in
ance of the apoA-I and CE components of TG-enriched and postheparin plasma HL activity is a particularly prevalent
fasting, relatively TG-poor rabbit HDL in the wild-type occurrence in insulin resistant states such as obesity and
New Zealand white (NZW) rabbit, an animal model natu- type 2 diabetes, and appears to be related to the low HDL
rally deficient in the lipolytic enzyme, hepatic lipase (HL) levels in these states [75–79]. Despres et al., for instance,
[61]. Whole rabbit HDL was first enriched with TG by investigated the association between body fat composition,
incubating HDL ex vivo with human VLDL, isolated by as determined by computed axial tomography, and posthep-
ultracentrifugation, and labeled with 131I and 3H-cholesteryl arin plasma HL activity in a sample of 16 obese women
oleyl ether tracers [61]. The tracers were then injected into [79]. The investigators demonstrated significant positive
recipient NZW rabbits. We achieved an 87% mean physi- associations between intra-abdominal fat deposition and HL
ologic increase in the percentage mass of TG in the TG-rich activity (p ⬍ 0.66, p ⬍ 0.005), which in turn correlated
HDL vs. control TG-poor HDL, and apart from the normal negatively with HDL2-c levels (p ⬍ 0.66, p ⬍ 0.05) [79].
physiologic depletion of HDL CE associated with TG en- Conversely, in another study of 21 healthy older men who
richment of HDL, other measured components of HDL underwent diet-induced weight loss, loss of intra-abdominal
(phospholipid, protein, and size) remained unaltered [61]. fat was found to be significantly correlated with a reduction
Nonetheless, we found no significant difference in the FCR in postheparin HL, which in turn was associated with in-
of HDL apoA-I nor in the rate of selective HDL CE clear- creased HDL2-c levels [78].
ance between the tracers [61]. We postulated that HL defi- Other investigators have observed similar correlations
ciency in the rabbit model could account for the lack of between HL and other indices of adiposity in addition to
observed difference between the clearance of TG-rich and intra-abdominal fat content and further contended that the
fasting rabbit HDL [61]. In other words, we showed that TG relation between HL and adiposity reflects the modulatingS. Rashid et al. / Clinical Biochemistry 36 (2003) 421– 429 425
effect of secondary factors associated with increased adi-
posity –namely hyperinsulinemia. Nie et al., for example,
investigated the relation between body mass index (BMI)
and HL activity in a large sample of healthy men stratified
according to genetically defined differences in HL activity
[80]. Results of the study demonstrated highly significant (p
⬍ 0.001) associations between BMI and HL activity in this
cohort [80]. The investigators further observed that mean
BMI tended to be similar in men with varying HL promoter
genotypes, indicating that the relation between BMI and HL
activity was not due to an effect of HL activity on adiposity,
but rather adiposity, or factors associated with adiposity, on
HL activity [80]. More specifically, the authors of this study
surmised that the correlation between BMI and HL activity
reflected an increase in circulating plasma insulin levels,
which tends to accompany increases in BMI [80]. In support
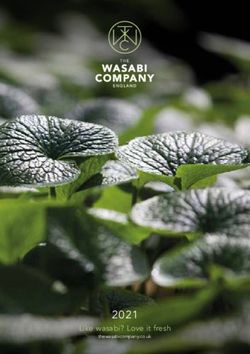
Fig. 1. Schematic design of the proposed mechanisms of HDL lowering in
of this theory, a site at the promoter region of the HL gene
insulin resistant, hypertriglyceridemic states. In insulin resistant, hypertri-
has recently been identified as being similar in sequence to glyceridemic states there is a greater mass transfer of TG from the in-
a motif involved in the binding of insulin-responsive tran- creased pool of apo B-containing, TG-rich lipoproteins, with heteroex-
scription factors [74,81], although the functional signifi- change of CE from HDL to TG-rich lipoproteins. This process results in the
cance of this site is not known. formation of HDL particles that are relatively TG enriched and CE de-
pleted, in itself contributing to the lowering of plasma HDL cholesterol
HL activity, however, unlike LPL, is not upregulated in
concentration. We propose that the TG-rich HDL particles thus formed are
a clear cut fashion by insulin. Studies investigating the also cleared more rapidly from the circulation than non-TG-rich HDL due
effect of insulin on HL activity have shown contradictory to one or all of the following three mechanisms: 1.) TG-rich, CE-depleted
results. For example, while some studies in patients with HDL particles have been shown to be thermodynamically less stable,
type 2 diabetes have shown an increase in HL activity with having their apoA-I in a more loosely bound form; 2.) TG-rich HDL are
more readily lipolyzed by HL, thereby reducing HDL size, and resulting in
hyperinsulinemia [75], others have shown a decline [82]. It
free apo A-I or lipid-poor pre-1 particles (containing apoA-I together with
is more likely that instead of hyperinsulinemia per se, in- a small amount of lipid) being shed from the particles; 3.) the HDL
sulin resistance at the liver secondary to obesity or type 2 ‘remnant’ particles that have been reduced in size may themselves be more
diabetes in some fashion induces the increase in HL activity readily cleared from the circulation. The above processes may then en-
in these states. Consistent with this idea, studies in normal hance HDL apoA-I FCR (fractional catabolic rate). The end result is a
lowering of HDL-c and apoA-I levels in plasma. It should be noted that in
and diabetic rats have shown that increases in liver HL
addition to being irreversibly cleared from the circulation, lipolytically
activity are induced by chronic, but not acute insulin ad- modified HDL or apo A-I that is shed from the particles can also undergo
ministration [83]. The authors of the study concluded that ‘recycling’ to spherical HDL by the re-acquisition of lipid (indicated by the
chronic alterations in metabolic status that occur in response dashed lines).
to prolonged hyperinsulinemia and insulin resistance in-
duced the increase in liver HL activity in the animals [83].
Several more recent studies in humans have reported direct shown to significantly impact on HL activity levels in hu-
correlations between HL activity and indices of insulin mans, has been associated with reduced HDL-c and apoA-I
resistance, such as the plasma insulin response to oral glu- levels in some, but not in all populations studied [50,85–
cose [78,78,84]. Very recently, we have shown that HL 88]. Similarly, interventions that alter HL activity in hu-
activity is increased in fructose-fed Syrian golden hamsters, mans –for example, oral estrogen administration in women-
an animal model of insulin resistance, and reduced with are not consistently associated with variation in HDL-c
rosiglitazone treatment, an insulin sensitizer with PPAR␥ levels [68]. These findings suggest that the effect of HL on
agonist activity (unpublished observations). HDL metabolism is not consistent in physiologically rele-
vant settings, and is subject to modulation by metabolic,
environmental, or genetic factors.
The Effect of HL on HDL Catabolism in the Context Previous studies indicate that the hypertriglyceridemic,
of TG Enrichment of HDL insulin resistant state is a clinical condition in which HL
does exert a consistent, important effect on plasma HDL
While alterations in HL activity are widely believed to concentrations. Studies in humans investigating the role of
play an important role in HDL metabolism, studies inves- HL on HDL metabolism in insulin resistant states, such as
tigating the interaction between HL and HDL in humans those described above, however, have only revealed asso-
have shown conflicting results. For instance, a common ciations between the two. They did not specifically deter-
single nucleotide polymorphism in the promoter region (po- mine mechanisms responsible for the decline in HDL levels
sition ⫺514) of the HL gene locus (LIPC), that has been occurring in association with increased HL activity in insu-426 S. Rashid et al. / Clinical Biochemistry 36 (2003) 421– 429
lin resistance. We have postulated that the TG enrichment of particles results in the formation of smaller, ␣-HDL parti-
HDL and the elevated HL lipolytic action that occur in these cles, which they termed “remnant HDL” [95]. They further
conditions act in concert to promote the increased HDL demonstrated that apoA-I associated with these “remnant
catabolism and decline in HDL-c levels in these states HDL” showed greater high affinity binding and uptake into
(illustrated in Fig. 1). To directly test this hypothesis, we HepG2 cells and isolated perfused liver compared to non-
investigated the combined effects of TG enrichment of HDL lipolyzed TG-rich HDL2 [95,96]. Our studies in the rabbit
and lipolytic transformation of HDL by HL on the subse- provide in vivo support for this concept.
quent metabolic clearance of HDL apoA-I in the HL-defi- It should be noted that our studies and those discussed
cient NZW rabbit [89,90]. More specifically, we compared immediately above have focused on the catabolic processes
the clearance of apoA-I associated with TG-rich and native, of HDL apoA-I clearance and cellular uptake, respectively.
relatively TG-poor rabbit HDL tracers that had been lipo- These studies did not investigate the process of HDL retro-
lyzed by HL using two different methods (1) ex vivo lipol- endocytosis and recycling described in several studies.
ysis by purified human HL and [89] (2) in vivo lipolysis by Studies conducted in various primary cells and cell lines
adenovirus-mediated transfer of the human HL transgene have indicated that a portion of HDL apoproteins bound and
(rHL-Adv) [90]. While previous studies in several animal internalized by cells are resecreted or recycled via a retro-
models have shown a decline in HDL levels with HL ex- endocytosis process [97–100]. Recycling of HDL and its
pression, these studies have generally examined this phe- apolipoproteins is thought to be mediated by the endosome
nomenon in the presence of supraphysiological expression recyling compartment [98] and has been postulated to in-
of HL [91–93]. Those studies also did not determine the role volve the LDL receptor-related protein (LRP) [101], al-
of HL action in the context of TG enrichment of HDL, though this remains to be specifically tested. In future stud-
which would more closely mimic the characteristic of HDL ies, the relative importance of HDL recycling in
in insulin resistant, hypertriglyceridemic states. Our studies determining overall HDL levels will need to be examined in
in the rabbit model, in contrast, investigated both of these vivo across different animal models and in humans.
physiologic processes and involved the use of moderate HL In general, the etiology delineated in this review can
enzyme activity. explain, at least in part, the lowering of HDL levels in
Results of our in vivo studies in the rabbit showed that individuals demonstrating insulin resistance and frank hy-
apoA-I associated with TG-enriched HDL, modified ex vivo pertriglyceridemia, which constitute by far the majority of
by catalytically active HL, and reduced in size, was cleared individuals with reduced HDL concentrations [10]. In indi-
22% more rapidly vs. TG-enriched HDL incubated with viduals with low HDL in the absence of frank hypertriglyc-
heat-inactivated HL and 26% more rapidly than relatively eridemia (i.e., those with isolated low HDL), however, HDL
TG-poor HDL incubated with active HL (p ⬍ 0.05 for both) TG enrichment and elevated HL activity cannot explain the
[89]. In rabbits injected with rHL-Adv, HL activity in- lowering of HDL levels. Subjects with isolated low HDL
creased 2- to sevenfold above endogenous levels. Moreover, have been reported to be insulin resistant in some [102] but
there was a marked 50% enhancement in the metabolic not all populations [103,104] and neither TG enrichment of
clearance of TG-enriched HDL vs. TG-poor HDL in rHL- HDL nor an elevation in HL activity has consistently been
Adv rabbits (p ⬍ 0.01) [90]. In contrast, in rabbits injected reported in these individuals [32,103]. Isolated low HDL
with the control rlacZ-Adv, there was no significant en- has, in fact, been characterized as a metabolic disorder
hancement of apoA-I associated with TG-rich vs. native distinct from the hypertriglyceridemia-low HDL phenotype
HDL [90]. Furthermore, in rabbits expressing human HL, [10], and, as discussed above, has been attributed in many
but not in control rabbits, there was a significant decline in cases to rare familial syndromes [15].
major HDL lipids, including HDL TG, phospholipid, and
HDL-c, and a decrease in HDL particle size [90].
Overall, our studies in the HL-deficient rabbit model Conclusions
established that TG-enrichment of HDL, in the presence,
but not in the absence, of physiologic levels of lipolytically Overall, the interaction between HDL that is TG en-
active HL, is associated with enhanced HDL apoA-I clear- riched and HL action plays an important role in the en-
ance. Shedding of free apoA-1 or the formation of lipid poor hanced catabolism of HDL in insulin resistant, hypertriglyc-
small pre1-HDL during intravascular lipolysis of TG-rich eridemic states, such as occurs in association with
HDL by HL could enhance apoA-1 clearance from the abdominal obesity and type 2 diabetes. It may be argued that
circulation [94]. Alternatively, “remnant HDL” particles the accelerated HDL clearance in these conditions contrib-
produced by this lipolytic process, may be more rapidly utes to reverse cholesterol transport, and may therefore not
removed from the circulation by receptor-mediated uptake be pro-atherosclerotic. It is more logical to infer, however,
[95,96]. Both of these processes may play a role in the that HL-mediated lipolysis of the TG enriched and CE-
lowering of HDL-c and apoA-I in insulin resistant, hyper- depleted HDL particles characteristic of these states will
triglyceridemic states. Barrans et al. had previously demon- contribute quantitatively little to HDL CE uptake and re-
strated that HL-mediated lipolysis of TG enriched HDL2 verse cholesterol transport [105]. Instead, the lowering ofS. Rashid et al. / Clinical Biochemistry 36 (2003) 421– 429 427
HDL plasma concentrations by this mechanism would result [13] von Eckardstein A, Nofer JR, Assmann G. High density lipoproteins
in fewer HDL particles to carry out antiatherosclerotic func- and arteriosclerosis. Role of cholesterol efflux and reverse choles-
terol transport. Arterioscler Thromb Vasc Biol 2001;21:13–27.
tions of HDL, including its inhibitory effects at the arterial [14] Schaefer EJ. Clinical, biochemical, and genetic features in familial
wall on LDL oxidation, cellular proliferation, and macro- disorders of high density lipoprotein deficiency. Arterioscler 1984;
phage formation. Thus, TG enrichment combined with HL- 4:303–22.
mediated lipolysis of HDL likely contributes to the accel- [15] Brewer HB, Santamarina-Fojo S, Hoeg JM. Disorders of lipoprotein
erated rate of atherosclerosis that is characteristic of insulin metabolism. In: In: Degroot LJ, editor. Philadelphia: W.B. Saunders,
1995. p. 2731–53. Endocrinology, volume 3.
resistant conditions. In addition to being unfavourable, and [16] Brooks-Wilson A, Marcil M, Clee SM, et al. Mutations in ABC1 in
likely pro-atherogenic, the TG enriched HDL-elevated HL Tangier disease and familial high-density lipoprotein deficiency. Nat
phenotype is a prevalent, integral feature of insulin resistant, Genet 1999;22:336 – 45.
hypertriglyceridemic individuals. It is important to note that [17] Ng DS, Leiter LA, Vezina C, et al. Apolipoprotein A-I Q[-2]X
multiple pathways of HDL clearance have been identified to causing isolated apolipoprotein A-I deficiency in a family with
analphalipoproteinemia. J Clin Invest 1994;93:223–9.
date, and the hypertriglyceridemic-HDL-lipolysis phenom- [18] Sirtori CR, Calabresi L, Franceschini G, et al. Cardiovascular status
enon may be only one such major pathway perturbed in of carriers of the apolipoprotein A-I(Milano) mutant: the Limone sul
insulin resistant individuals. Other mechanisms may also Garda study. Circulation 2001;103:1949 –54.
contribute substantially to HDL-c and HDL apoA-I lower- [19] Rashid, S, Uffelman, K, Lewis, GF. The mechanism of HDL low-
ing in insulin resistant/hypertriglyceridemic states. Future ering in hypertriglyceridemic, insulin resistant states. J Diabetes
Complications 2002;16:24 –28.
studies are required to elucidate more precisely the pertur- [20] Syvanne M, Taskinen MR. Lipids and lipoproteins as coronary risk
bations and contributions of the various HDL metabolic factors in non-insulin-dependent diabetes mellitus. Lancet 1997;
pathways in the lowering of HDL plasma concentrations in 350(Suppl 1):SI20 –SI23.
insulin resistant, hypertriglyceridemic states. [21] Adeli K, Taghibiglou C, Van Iderstine SC, et al. Mechanisms of
hepatic very low-density lipoprotein overproduction in insulin re-
sistance. Trends Cardiovasc Med 2001;11:170 – 6.
[22] Lewis GF, Carpentier A, Adeli K, et al. Disordered fat storage and
References mobilization in the pathogenesis of insulin resistance and type 2
diabetes. Endocr Rev 2002;23:201–29.
[1] Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syn- [23] Brunzell JD, Hazzard WR, Porte D Jr, et al. Evidence for a common,
drome among US adults: findings from the third National Health and saturable, triglyceride removal mechanism for chylomicrons and
Nutrition Examination Survey. JAMA 2002;287:356 –9. very low density lipoproteins in man. J Clin Invest 1973;52:1578 –
[2] Reaven GM. Banting lecture 1988. Role of insulin resistance in 85.
human disease. [Review] [71 refs]. Diabetes 1988;37:1595– 607. [24] Connelly PW, Maguire GF, Vezina C, et al. Kinetics of lipolysis of
[3] Reaven GM. Pathophysiology of insulin resistance in human dis- very low density lipoproteins by lipoprotein lipase. Importance of
ease. Physiol Rev 1995;75:473– 86. particle number and noncompetitive inhibition by particles with low
[4] Lewis GF, Steiner G. Hypertriglyceridemia and its metabolic con- triglyceride content. J Biol Chem 1994;269:20554 – 60.
sequences as a risk factor for atherosclerotic cardiovascular disease [25] Jansen H, Breedveld B, Schoonderwoerd K. Role of lipoprotein
in non-insulin-dependent diabetes mellitus. [Review] [204 refs]. lipases in postprandial lipid metabolism. Atherosclerosis 1998;
Diabetes Metab Rev 1996;12:37–56. 141(Suppl 1):S31–S34.
[5] Lamarche B, Lewis GF. Atherosclerosis prevention for the next [26] Haidari M, Leung N, Mahbub F, et al. Fasting and postprandial
decade: risk assessment beyond low density lipoprotein cholesterol. overproduction of intestinally derived lipoproteins in an animal
[Review] [104 refs]. Can J Cardiol 1998;14:841–51. model of insulin resistance. Evidence that chronic fructose feeding
[6] Ginsberg HN. Lipoprotein physiology in nondiabetic and diabetic in the hamster is accompanied by enhanced intestinal de novo
states. Relationship to atherogenesis. [Review] [180 refs]. Diabetes lipogenesis and ApoB48-containing lipoprotein overproduction.
Care 1991;14:839 –55. J Biol Chem 2002;277:31646 –55.
[7] Reaven G. Metabolic syndrome: pathophysiology and implications [27] Ginsberg HN. Insulin resistance and cardiovascular disease. J Clin
for management of cardiovascular disease. Circulation 2002;106: Invest 2000;106:453– 8.
286 – 8. [28] Patsch JR, Prasad S, Gotto AM Jr, et al. High density lipoprotein2.
[8] Lamarche B, Rashid S, Lewis G. HDL metabolism in hypertriglyc- Relationship of the plasma levels of this lipoprotein species to its
eridemic states: an overview. Clin Chim Acta 1999;286:145– 61. composition, to the magnitude of postprandial lipemia, and to the
[9] Sacks FM. The role of high-density lipoprotein (HDL) cholesterol in activities of lipoprotein lipase and hepatic lipase. J Clin Invest
the prevention and treatment of coronary heart disease: expert group 1987;80:341–7.
recommendations. Am J Cardiol 2002;90:139 – 43. [29] Ginsberg HN. Diabetic dyslipidemia: basic mechanisms underlying
[10] Despres JP, Lemieux I, Dagenais GR, et al. HDL-cholesterol as a the common hypertriglyceridemia and low HDL cholesterol levels.
marker of coronary heart disease risk: the Quebec cardiovascular Diabetes 1996;45:S27–30.
study. Atherosclerosis 2000;153:263–72. [30] Nikkila EA, Taskinen MR, Sane T. Plasma high-density lipoprotein
[11] Luc G, Bard JM, Ferrieres J, et al. Value of HDL cholesterol, concentration and subfraction distribution in relation to triglyceride
apolipoprotein A-I, lipoprotein A-I, and lipoprotein A-I/A-II in metabolism. [Review]. Am Heart J 1987;113:543– 8.
prediction of coronary heart disease: the PRIME Study. Prospective [31] Lewis GF, O’Meara NM, Soltys PA, et al. Postprandial lipoprotein
Epidemiological Study of Myocardial Infarction. Arterioscler metabolism in normal and obese subjects: comparison after the
Thromb Vasc Biol 2002;22:1155– 61. vitamin A fat-loading test. J Clin Endocrinol Metab 1990;71:1041–
[12] Nofer J, Kehrel B, Fobker M, et al. HDL and arteriosclerosis: 50.
beyond reverse cholesterol transport. Atherosclerosis 2002;161:1– [32] Lewis GF, O’Meara NM, Soltys PA, et al. Fasting hypertriglyceri-
16. demia in noninsulin-dependent diabetes mellitus is an important428 S. Rashid et al. / Clinical Biochemistry 36 (2003) 421– 429
predictor of postprandial lipid and lipoprotein abnormalities. J Clin [53] Guerin M, Le Goff W, Lassel TS, et al. Proatherogenic role of
Endocrinol Metab 1991;72:934 – 44. elevated CE transfer from HDL to VLDL(1) and dense LDL in type
[33] Patsch JR, Karlin JB, Scott LW, et al. Inverse relationship between 2 diabetes: impact of the degree of triglyceridemia. Arterioscler
blood levels of high density lipoprotein subfraction 2 and magnitude Thromb Vasc Biol 2001;21:282– 8.
of postprandial lipemia. Proc Natl Acad Sci U S A 1983;80:1449 – [54] Castle CK, Kuiper SL, Blake WL, et al. Remodeling of the HDL in
53. NIDDM: a fundamental role for cholesteryl ester transfer protein.
[34] Tall AR. Plasma high density lipoproteins. Metabolism and relation- Am J Physiol 1998;274:E1091–E1098.
ship to atherogenesis. [Review]. J Clin Invest 1990;86:379 – 84. [55] Lewis GF, Rashid S, Uffelman K, et al. Mechanism of HDL low-
[35] Eisenberg S. Lipoprotein abnormalities in hypertriglyceridemia: sig- ering in insulin resistant states. In: Angel A, Dhalla N, Pierce G,
nificance in atherosclerosis. Am Heart J 1987;113:555– 61. Singal P, editors. Diabetes and Cardiovascular Disease: Etiology,
[36] Mann CJ, Yen FT, Grant AM, et al. Mechanism of plasma cho- Treatment and Outcomes. New York, NY: Klewer Academic/Ple-
lesteryl ester transfer in hypertriglyceridemia. J Clin Invest 1991; num, 2001. p. 273–7.
88:2059 – 66. [56] Patsch JR, Prasad S, Gotto AM Jr, et al. Postprandial lipemia. A key
[37] Foger B, Ritsch A, Doblinger A, et al. Relationship of plasma for the conversion of high density lipoprotein2 into high density
cholesteryl ester transfer protein to HDL cholesterol. Studies in lipoprotein3 by hepatic lipase. J Clin Invest 1984;74:2017–23.
normotriglyceridemia and moderate hypertriglyceridemia. Arterio- [57] Liang HQ, Rye KA, Barter PJ. Dissociation of lipid-free apolipopro-
scler Thromb Vasc Biol 1996;16:1430 – 6. tein A-I from high density lipoproteins. J Lipid Res 1994;35:1187–
[38] Clay MA, Newnham HH, Forte TM, et al. Cholesteryl ester transfer 99.
protein and hepatic lipase activity promote shedding of apo A-I from [58] Lamarche B, Uffelman KD, Carpentier A, et al. Triglyceride enrich-
HDL and subsequent formation of discoidal HDL. Biochim Biophys ment of HDL enhances in vivo metabolic clearance of HDL apo A-I
Acta 1992;1124:52– 8. in healthy men. J Clin Invest 1999;103:1191–9.
[39] Pulawa LK, Eckel RH. Overexpression of muscle lipoprotein lipase [59] Sparks DL, Davidson WS, Lund-Katz S, et al. Effects of the neutral
and insulin sensitivity. Curr Opin Clin Nutr Metab Care 2002;5: lipid content of high density lipoprotein on apolipoprotein A-1
569 –74. structure and particle stability. J Biol Chem 1995;270:26910 –7.
[40] Yost TJ, Eckel RH. Regional similarities in the metabolic regulation [60] Clay MA, Newnham HH, Barter PJ. Hepatic lipase promotes a loss
of adipose tissue lipoprotein lipase. Metabolism 1992;41:33– 6. of apolipoprotein A-I from triglyceride-enriched human high density
[41] Yost TJ, Froyd KK, Jensen DR, et al. Change in skeletal muscle
lipoproteins during incubation in vitro. Arterioscler Thromb 1991;
lipoprotein lipase activity in response to insulin/glucose in non-
11:415–22.
insulin-dependent diabetes mellitus. Metabolism 1995;44:786 –90.
[61] Rashid S, Uffelman K, Barrett PHR, et al. Triglyceride enrichment
[42] Merkel M, Eckel RH, Goldberg IJ. Lipoprotein lipase: genetics,
of HDL does not alter HDL selective cholesteryl ester clearance in
lipid uptake, and regulation. J Lipid Res 2002;43:1997–2006.
rabbits. J Lipid Res 2001;42:265–71.
[43] Brinton EA, Eisenberg S, Breslow JL. Human HDL cholesterol
[62] Jin W, Marchadier D, Rader DJ. Lipases and HDL metabolism.
levels are determined by apoA-I fractional catabolic rate, which
Trends Endocrinol Metab 2002;13:174 – 8.
correlates inversely with estimates of HDL particle size. Effects of
[63] Hopkins GJ, Barter PJ. Role of triglyceride-rich lipoproteins and
gender, hepatic and lipoprotein lipases, triglyceride and insulin lev-
hepatic lipase in determining the particle size and composition of
els, and body fat distribution. Arterioscler Thromb 1994;14:707–20.
high density lipoproteins. J Lipid Res 1986;27:1265–77.
[44] Brinton EA, Eisenberg S, Breslow JL. Increased apo A-I and apo
[64] Jaye M, Lynch KJ, Krawiec J, et al. A novel endothelial-derived
A-II fractional catabolic rate in patients with low high density
lipase that modulates HDL metabolism. Nat Genet 1999;21:424 – 8.
lipoprotein-cholesterol levels with or without hypertriglyceridemia.
[65] Newnham HH, Barter PJ. Changes in particle size of high density
J Clin Invest 1991;87:536 – 44.
[45] Horowitz BS, Goldberg IJ, Merab J, et al. Increased plasma and lipoproteins during incubation with very low density lipoproteins,
renal clearance of an exchangeable pool of apolipoprotein A-I in cholesteryl ester transfer protein and lipoprotein lipase. Biochim
subjects with low levels of high density lipoprotein cholesterol. Biophys Acta 1992;1125:297–304.
J Clin Invest 1993;91:1743–52. [66] Olivecrona G, Olivecrona T. Triglyceride lipases and atherosclero-
[46] Vajo Z, Terry JG, Brinton EA. Increased intra-abdominal fat may sis. Curr Opin Lipidol 1995;6:291–305.
lower HDL levels by increasing the fractional catabolic rate of Lp [67] Bengtsson G, Olivecrona T. The hepatic heparin releasable lipase
A-I in postmenopausal women. Atherosclerosis 2002;160:495–501. binds to high density lipoproteins. FEBS Lett 1980;119:290 –2.
[47] Pont F, Duvillard L, Florentin E, et al. High-density lipoprotein [68] Thuren T. Hepatic lipase and HDL metabolism. J Lipid Res 2000;
apolipoprotein A-I kinetics in obese insulin resistant patients. An in 11:277– 83.
vivo stable isotope study. Int J Obes Relat Metab Disord 2002;26: [69] Shirai K, Barnhart RL, Jackson RL. Hydrolysis of human plasma
1151– 8. high density lipoprotein 2- phospholipids and triglycerides by he-
[48] Frenais R, Ouguerram K, Maugeais C, et al. High density lipopro- patic lipase. Biochem Biophys Res Commun 1981;100:591–9.
tein apolipoprotein AI kinetics in NIDDM: a stable isotope study. [70] Connelly PW. The role of hepatic lipase in lipoprotein metabolism.
Diabetologia 1997;40:578 – 83. Clin Chim Acta 1999;286:243–55.
[49] Le NA, Ginsberg HN. Heterogeneity of apolipoprotein A-I turnover [71] Doolittle MH, Wong H, Davis RC, et al. Synthesis of hepatic lipase
in subjects with reduced concentrations of plasma high density in liver and extrahepatic tissues. J Lipid Res 1987;28:1326 –34.
lipoprotein cholesterol. Metabolism 1988;37:614 –17. [72] Sanan DA, Fan J, Bensadoun A, et al. Hepatic lipase is abundant on
[50] De Oliveira e Silva ER, Kong M, Han Z, et al. Metabolic and genetic both hepatocyte and endothelial cell surfaces in the liver. J Lipid Res
determinants of HDL metabolism and hepatic lipase activity in 1997;38:1002–13.
normolipidemic females. J Lipid Res 1999;40:1211–21. [73] Ji ZS, Dichek HL, Miranda RD, et al. Heparan sulfate proteoglycans
[51] Pietzsch J, Julius U, Nitzsche S, et al. In vivo evidence for increased participate in hepatic lipaseand apolipoprotein E-mediated binding
apolipoprotein A-I catabolism in subjects with impaired glucose and uptake of plasma lipoproteins, including high density lipopro-
tolerance. Diabetes 1998;47:1928 –34. teins. J Biol Chem 1997;272:31285–92.
[52] Morton RE, Zilversmit DB. Inter-relationship of lipids transferred [74] Perret B, Mabile L, Martinez L, et al. Hepatic lipase: structure/
by the lipid transfer protein isolated from human lipoprotein-defi- function relationship, synthesis, and regulation. J Lipid Res 2002;
cient plasma. J Biol Chem 1983;258:11751–7. 43:1163–9.S. Rashid et al. / Clinical Biochemistry 36 (2003) 421– 429 429
[75] Syvanne M, Ahola M, Lahdenpera S, et al. High density lipoprotein ance of triglyceride-enriched versus native HDL apolipoprotein A-I.
subfractions in non-insulin-dependent diabetes mellitus and coro- Circulation 2003 (In Press).
nary artery disease. J Lipid Res 1995;36:573– 82. [91] Fan J, Wang J, Bensadoun A, et al. Overexpression of hepatic lipase
[76] Laakso M, Sarlund H, Ehnholm C, et al. Relationship between in transgenic rabbits leads to a marked reduction of plasma high
postheparin plasma lipases and high-density lipoprotein cholesterol density lipoproteins and intermediate density lipoproteins. Proc Natl
in different types of diabetes. Diabetologia 1987;30:703– 6. Acad Sci U S A 1994;91:8724 – 8.
[77] Carr MC, Hokanson JE, Deeb SS, et al. A hepatic lipase gene [92] Dugi KA, Amar MJ, Haudenschild CC, et al. In vivo evidence for
promoter polymorphism attenuates the increase in hepatic lipase both lipolytic and nonlipolytic function of hepatic lipase in the
activity with increasing intra-abdominal fat in women. Arterioscler metabolism of HDL. Arterioscler Thromb Vasc Biol 2000;20:793–
Thromb Vasc Biol 1999;19:2701–7. 800.
[78] Purnell JQ, Kahn SE, Albers JJ, et al. Effect of weight loss with [93] Lambert G, Chase MB, Dugi K, et al. Hepatic lipase promotes the
reduction of intra-abdominal fat on lipid metabolism in older men. selective uptake of high density lipoprotein-cholesteryl esters via the
J Clin Endocrinol Metab 2000;85:977– 82. scavenger receptor BI. J Lipid Res 1999;40:1294 –303.
[79] Despres JP, Ferland M, Moorjani S, et al. Role of hepatic-triglyc- [94] Barrans A, Collet X, Barbaras R, et al. Hepatic lipase induces the
eride lipase activity in the association between intra-abdominal fat formation of pre-beta 1 high density lipoprotein (HDL) from tria-
and plasma HDL cholesterol in obese women. Arterioscler 1989;9: cylglycerol-rich HDL2. A study comparing liver perfusion to
485–92. in vitro incubation with lipases. J Biol Chem 1994;269:11572–
[80] Nie L, Wang J, Clark LT, et al. Body mass index and hepatic lipase 7.
gene (LIPC) polymorphism jointly influence postheparin plasma [95] Barrans A, Collet X, Barbaras R, et al. Hepatic lipase induces the
hepatic lipase activity. J Lipid Res 1998;39:1127–30. formation of pre-1 high density lipoprotein (HDL) from triacylglyc-
[81] Botma GJ, Verhoeven AJ, Jansen H. Hepatic lipase promoter activ- erol-rich HDL2. J Biol Chem 1994;269:11572–7.
ity is reduced by the C-480T and G-216A substitutions present in the [96] Guendouzi K, Collet X, Bertrand P, et al. Remnant high density
common LIPC gene variant, and is increased by Upstream Stimu- lipoprotein2 particles produced by hepatic lipase display high-affin-
latory Factor. Atherosclerosis 2001;154:625–32. ity binding and increased endocytosis into a human hepatoma cell
[82] Baynes C, Henderson AD, Richmond W, et al. The response of line (HEPG2). Biochemistry 1998;37:14974 – 80.
hepatic lipase and serum lipoproteins to acute hyperinsulinaemia in [97] Kambouris AM, Roach PD, Calvert GD, et al. Retroendocytosis of
type 2 diabetes. Eur J Clin Invest 1992;22:341– 6. high density lipoproteins by the human hepatoma cell line, HepG2.
[83] Knauer TE, Woods JA, Lamb RG, et al. Hepatic triacylglycerol Arterioscler 1990;10:582–90.
lipase activities after induction of diabetes and administration of [98] Silver DL, Wang N, Tall AR. Defective HDL particle uptake in
insulin or glucagon. J Lipid Res 1982;23:631–7. ob/ob hepatocytes causes decreased recycling, degradation, and se-
[84] Baynes C, Henderson AD, Anyaoku V, et al. The role of insulin lective lipid uptake. J Clin Invest 2000;105:151–9.
insensitivity and hepatic lipase in the dyslipidaemia of type 2 dia- [99] Rahim AT, Miyazaki A, Morino Y, et al. Biochemical demonstra-
betes. Diabet Med 1991;8:560 – 6. tion of endocytosis and subsequent resecretion of high-density li-
[85] Murtomaki S, Tahvanainen E, Antikainen M, et al. Hepatic lipase poprotein by rat peritoneal macrophages. Biochim Biophys Acta
gene polymorphisms influence plasma HDL levels. Results from 1991;1082:195–203.
Finnish EARS participants. European Atherosclerosis Research [100] Rogler G, Herold G, Fahr C, et al. High-density lipoprotein 3
Study. Arterioscler Thromb Vasc Biol 1997;17:1879 – 84. retroendocytosis: a new lipoprotein pathway in the enterocyte
[86] Guerra R, Wang J, Grundy SM, et al. A hepatic lipase (LIPC) allele (Caco-2). Gastroenterology 1992;103:469 – 80.
associated with high plasma concentrations of high density lipopro- [101] Vassiliou G, Benoist F, Lau P, et al. The low density lipoprotein
tein cholesterol. Proc Natl Acad Sci U S A 1997;94:4532–7. receptor-related protein contributes to selective uptake of high den-
[87] Hegele RA, Harris SB, Brunt JH, et al. Absence of association sity lipoprotein cholesteryl esters by SW872 liposarcoma cells and
between genetic variation in the LIPC gene promoter and plasma primary human adipocytes. J Biol Chem 2001;276:48823–30.
lipoproteins in three Canadian populations. Atherosclerosis 1999; [102] Karhapaa P, Malkki M, Laakso M. Isolated low HDL cholesterol.
146:153– 60. An insulin-resistant state. Diabetes 1994;43:411–7.
[88] Tahvanainen E, Syvanne M, Frick MH, et al. Association of varia- [103] Couillard C, Bergeron N, Bergeron J, et al. Metabolic heterogeneity
tion in hepatic lipase activity with promoter variation in the hepatic underlying postprandial lipemia among men with low fasting high
lipase gene. The LOCAT Study Invsestigators. J Clin Invest 1998; density lipoprotein cholesterol concentrations. J Clin Endocrinol
101:956 – 60. Metab 2000;85:4575– 82.
[89] Rashid S, Barrett PH, Uffelman KD, et al. Lipolytically modified [104] Lamarche B, Despres JP, Pouliot MC, et al. Metabolic heterogeneity
triglyceride-enriched HDLs are rapidly cleared from the circulation. associated with high plasma triglyceride or low HDL cholesterol
Arterioscler Thromb Vasc Biol 2002;22:483–7. levels in men. Arterioscler Thromb 1993;13:33– 40.
[90] Rashid S, Trinh DK, Uffelman KD, et al. Expression of human [105] Jansen H, Verhoeven AJ, Sijbrands EJ. Hepatic lipase: a pro- or
hepatic lipase in the rabbit model preferentially enhances the clear- anti-atherogenic protein? J Lipid Res 2002;43:1352– 62.You can also read