Medicare Part D: A Model for Future Entitlement Reform
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
A not-for-profit health and tax policy research organization
March 27, 2015
Medicare Part D: A Model for Future Entitlement Reform
By Grace-Marie Turner
When Congress created the original Medicare $400 billion 10-year price tag. But Congress
program in 1965, physicians had a limited was going to pass a drug benefit. It was only a
arsenal of medicines available to treat chronic matter of how it was structured. Would it be
and acute maladies. Like most health insurers another government-run benefit program,
at the time, Medicare did not include laden with micromanagement and price
coverage for prescription drugs. controls? Or could we try something new to
engage consumer choice and competition in
But an explosion of pharmaceutical research delivering the benefit? The Republican
and innovation over the next several decades Congress opted for the latter.
led virtually all private health insurers to add
the coverage to their plans. They saw the The design of Medicare Part D was unique
evidence: If people took their medicines, they in government programs, calling on private
stayed healthier longer, they could avoid more plans to compete for customers based upon
invasive treatments including surgeries and flexible benefit designs and prices. In
hospitalizations, and overall health care addition, the MMA allowed creation of tax-
spending often could be reduced. preferred Health Savings Accounts, and it
rescued the then-flailing program, now called
But it took 38 years for Medicare to catch Medicare Advantage, which allows seniors to
up. In 2003, Congress passed and President choose to receive comprehensive medical
George W. Bush signed the Medicare services through competing private plans.
Modernization Act (MMA) which created the
Medicare Part D Prescription Drug Benefit. It Today, more than 1,001 stand-alone Part D
started operating in 2006. plans are offered across the country, and
beneficiaries in each region have a choice of
Today, about 38 million seniors and disabled an average of 30 stand-alone drug plans.
Americans on Medicare are enrolled in Part D Seniors can select the plans that provide the
plans, including employer-only group plans. medicines they need at the best value –
More than 60 percent of them are enrolled in transparency that seniors value. The Part D
private prescription drug plans and the rest portal allows them to see the specific drugs
receive drug coverage through Medicare each plan offers and to select the plan that
Advantage plans. 1 covers their drugs and offers the best price.
During debate over passage of the law, Because seniors have choices, private Part D
Medicare Part D was opposed by many for its plans have strong incentives to offer the
P.O. Box 320010 • Alexandria, VA 22320 • Phone 703-299-8900 • Fax 703-299-0721 • www.galen.org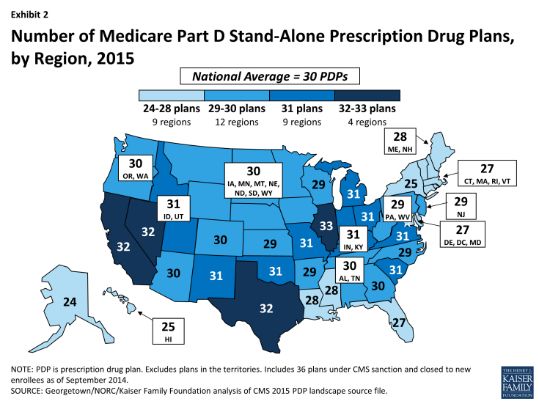
lowest costs and best benefit structures to setting the basic parameters and providing
attract the largest number of enrollees. seniors with information and premium
The structure is designed to minimize subsidies. It is precisely this hands-off, non-
government micro-management, with the interference approach that is the foundation of
Centers for Medicare and Medicaid Services Part D’s success.
Saving seniors and taxpayers money
Competition is critical to Part D’s success. where there are more drug plans, competition
Drug plans negotiate discounts directly with is more intense and prices are lower.
drug companies and have incentives to pass According to a recent report from the
those savings along to consumers, pricing Congressional Budget Office, plans submitted
their premiums attractively to gain larger lower bids in areas with more plans and
enrollment. Plans can then offer greater therefore more competition. 2
volume to drug companies in exchange for the
more deeply-discounted prices. This And the Part D program has saved taxpayers
competitive cycle has been able to keep money as well. In 2003, the CBO projected
premiums low while giving seniors access to that net federal spending for the Medicare
a wide variety of medicines. Part D prescription drug program would be
$99 billion in fiscal year 2013; actual
In 2004, the Medicare Trustees had estimated spending was $50 billion, or nearly 50 percent
that Medicare beneficiaries would pay an less than anticipated. 3
average of $61 a month for their Part D
benefit by 2013. Instead, the average A study published in the Journal of the
premium has remained steady at about $30 a American Medical Association in 2011 found
month for the last several years. In regions that, for those with limited prior drug
2coverage who subsequently enrolled in as long as they meet the same actuarial tests
Medicare Part D, there was an average as the basic plan. Some offer lower
savings of $1,200 per beneficiary in total non- deductibles but more generics and fewer
drug medical costs in both 2006 and 2007. 4 brand name drugs. Seniors can select plans
These offsetting savings coupled with the fact that may have lower costs than the average to
that 11 million seniors gained comprehensive reduce their premium. Other plans offer a
prescription drug coverage when Part D was greater choice of brand name drugs so other
implemented implies an overall savings of seniors may choose to pay more and receive a
$13.4 billion on other Medicare services in richer benefit.
2007, the first full year of the program.
In 2015, for the first time since the program
By providing better coverage to prescription started in 2006, all Part D PDPs will offer an
drugs, Part D improves the health of patients alternative design to the defined standard
and helps keep seniors out of the hospital benefit, which has a $320 deductible in 2015
while reducing spending for other healthcare and 25 percent coinsurance for all covered
services covered by Medicare. drugs. Some plans modify or eliminate the
deductible, and all PDPs use some type of
CBO uses these Part D savings when it varying cost-sharing tiers for covered generic
calculates overall Medicare savings and and brand-name drugs. 6
projects future costs. In a rare move, the non-
partisan Congressional Budget Office Financing for Part D comes from general
changed its methodology to take into account revenues (73%), beneficiary premiums (14%),
the effect that prescription medicines can and state contributions (13%) for those
have on spending in Medicare. For every one beneficiaries who are dually-eligible for
percent increase in the number of Medicare and Medicaid. The monthly
prescriptions filled by Medicare recipients, premium paid by enrollees is set to cover
spending on Medicare and other federal 25.5% of the cost of standard drug
programs that include drug utilization is coverage. Medicare subsidizes the remaining
anticipated to decrease by roughly .2 percent. 5 74.5%, based on bids submitted by plans for
their expected benefit payments. Low-
income beneficiaries receive assistance to
How does Medicare Part D work? cover premiums and deductibles and reduced
cost-sharing. Part D enrollees with higher
The basic design of the original Medicare Part incomes ($85,000/individual;
D program contained comprehensive drug $170,000/couple) pay a greater share of
coverage for routine and major drug costs, but standard Part D costs, ranging from 35% to
there was a sizeable “donut hole” in the 80%, depending on income. 7
middle – a gap in coverage between about
$2,500 and $5,500 a year in drug spending in How do you measure success?
2007. Few seniors hit the donut hole, but
after they made it through, they paid only The Part D program is unique in that private
about 5% of their drug costs. plans submit competitive bids each year to
determine the cost of the benefit. This is the
But few seniors are in traditional plans novel structure that sets it apart from the
because the law gives companies significant traditional Medicare fee-for-service model in
flexibility in how they design their drug plans which the government sets individual prices.
3Seniors have shown they are smart shoppers, accounted for about half the growth in
and they are the ones that have driven down Medicare spending.
the cost of the program. Evidence shows that
beneficiaries are successfully selecting plans According to the Centers for Disease Control
that minimize their out-of-pocket premium and Prevention, chronic disease accounts for
and drug costs. A recent study found that nearly 75% of overall health spending in the
beneficiaries reduced their average annual United States. But the real cost is even higher
out-of-pocket costs by almost $300 from 2006 since the CDC doesn’t take into account
to 2007 by switching to a new plan. secondary factors such as lost productivity
and impact on families. 8 Chronic diseases are
And better access to the right medicines can less deadly when patients stick to their regular
help reduce the cost of health care. From treatment program. If people take their
1987 to 2006, 10 chronic diseases – including medicines, they can control their diseases and
hypertension, diabetes, and arthritis – avoid expensive hospital stays.
What is next for Part D?
Opinion polls consistently show high Nonetheless, the pharmaceutical industry
beneficiary satisfaction with Part D, with frequently is targeted in political and budget
nearly 90% saying they are satisfied with the battles. In particular, many legislators and
program. 9 administration officials continue to call for
the federal government to intervene in private
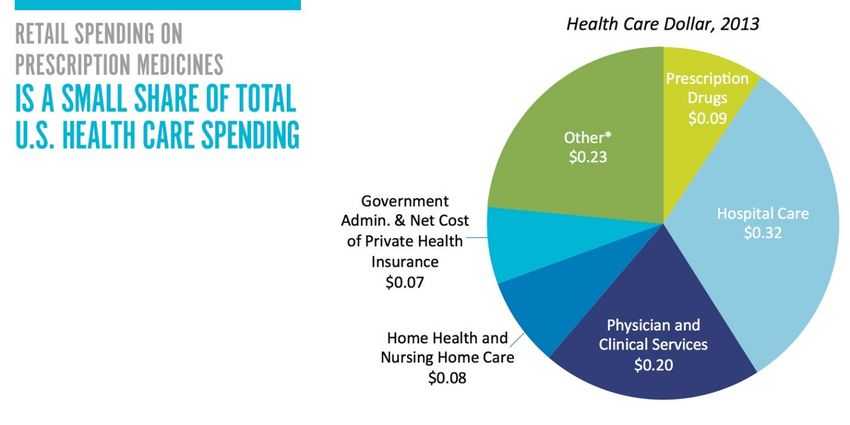
For reasons that defy the facts, spending on contract negotiations.
pharmaceuticals is seen as the primary driver
of the rise in health care spending. But drug The provision in the MMA that they want to
spending makes up only 9% of overall health change is the “non-interference” clause. This
spending in the United States. part of the law prevents the government from
intruding on private price negotiations
between pharmaceutical companies, Part D
4insurers, and pharmacies. These negotiations A generic may cost a beneficiary only 90
frequently result in rebates of as much as 20 cents but a brand name drug could cost them
to 30% for brand-name medicines, savings as much as $12 in copayments. For
which are passed on to beneficiaries and beneficiaries on multiple prescriptions, this
taxpayers. cost differential could be significant.
Those who advocate giving government a role Nearly 60 patient groups wrote to Congress to
in negotiating prices offer a false promise. oppose the proposal. This is a policy solution
Government does negotiate: it sets prices. in search of a problem: In 2012, LIS
And because it is such a big purchaser, beneficiaries filled 78% of their prescriptions
government interference quickly leads to with generics, versus 83% for the rest of the
price controls with all of their damaging Part D population. 10 That, despite the fact that
consequences of market distortions, LIS beneficiaries often have multiple chronic
shortages, and reduced investment in research conditions, higher rates of diabetes, and more
for new treatments. impairments than other beneficiaries, for
whom this proposed change would be
A new threat is emerging that would erode particularly problematic.
access to certain medicines for Medicare Part
D beneficiaries who receive Low Income There are many generics available, but only
Subsidies (LIS). Individuals with incomes up brand name drugs may work for an individual
to 150% of the federal poverty level and with patient. Increasing copayments for brand
limited assets are eligible for this low-income medicines for this population could
subsidy. It reduces their out-of-pocket compromise access to care, reduce adherence,
spending by paying some or all of the Part D and increase overall Medicare costs.
monthly premium and annual deductibles and
limiting their co-insurance or copayments.
Part D can be a model for Medicare
The Obama administration has called for reform
lower copayments for the generic drugs that
LIS beneficiaries receive and wants to double When addressing entitlement reform, it is
their copayments for brand name drugs. This impossible to ignore Medicare, a program that
policy will be harmful. Drug plans already covers nearly 54 million Americans and
have checks and balances in place to push which is projected to spend $626 billion in
seniors toward using more generic drugs. 2015. 11
Most employ step therapy that requires
patients to use generic drugs first, then if they President Obama has acknowledged the need
don’t work, their physician must apply for to reform our nation’s entitlement programs,
prior authorization so they can receive specifically citing the need for “modest
branded medicines. By the time the branded reforms” of Medicare and Social Security so
drug is approved, it’s clear that is the one the they don’t “crowd out the investments we
patient needs. The proposed co-payment need for our children and jeopardize the
change interferes with medical decisions by promise of a secure retirement for future
increasing the costs of the drugs that may be generations.”
the only ones that work for particular patients.
House Ways and Means Chairman Paul Ryan
(R-Wis.) and many others have proposed
5plans to modernize Medicare following the working and has a successful track record. It
Part D model to put it on a path to long-term can be a model for future Medicare reform,
sustainability. engaging an army of seniors in getting better
value for their health care dollars –as they
If Medicare is going to be preserved for future have proven they can do with the prescription
generations – and even for current retirees – drug benefit. Medicare can be preserved,
spending must be controlled and red tape taxpayers can be protected, and seniors can
untangled. 12 continue to have access to the treatments and
medicines they need, with lower costs driven
Policymakers can be guided by data and not by government price controls and
experience in making the next generation of micromanagement but by competition,
policy decisions about Medicare. Part D is consumer choice, and innovation.
Grace-Marie Turner is president of the Galen Institute. She can be reached at
gracemarie@galen.org or (703) 299-8900. Policy analyst Kirby Greissing assisted in the
preparation of this paper.
ENDNOTES
1 Hoadley J, Cubanski J, Hargrave E, and Summer L. “Medicare Part D: A First Look at Plan Offerings in 2015,” Oct 10, 2014.
Kaiser Family Foundation. http://kff.org/report-section/medicare-part-d-a-first-look-at-plan-offerings-in-2015-key-findings/
2Congressional Budget Office, “Competition and the Cost of Medicare’s Prescription Drug Program,” July 30, 2014,
http://www.cbo.gov/sites/default/files/45552-PartD.pdf
3 Congressional Budget Office, “Competition and the Cost of Medicare’s Prescription Drug Program.”
4McWilliams J, Zaslavsky AM, Huskamp HA. “Implementation of Medicare Part D and Nondrug Medical Spending for Elderly
Adults With Limited Prior Drug Coverage.” July 27, 2011. Journal of the American Medical
Association. http://jama.jamanetwork.com/article.aspx?articleid=1104150
5 Congressional Budget Office. “Offsetting Effects of Prescription Drug Use on Medicare’s Spending for Medical Services,”
November 2012.
6 Hoadley, et al. Kaiser. “A First Look…”
7 Kaiser Fact Sheet. http://kff.org/medicare/fact-sheet/the-medicare-prescription-drug-benefit-fact-sheet/
8 National Center for Chronic Disease Prevention and Health Promotion. The Power of Prevention: Chronic disease . . . the public
health challenge of the 21st century. 2009.
http://www.cdc.gov/chronicdisease/pdf/2009-Power-of-Prevention.pdf
9KRC Research. “Seniors’ Opinions About Medicare Prescription Drug Coverage: 9th Year Update,” July 2014.
http://www.medicaretoday.org/MT2014/KRC%202014%20SURVEY/KRC%20Survey%20of%20Seniors%20for%20%20Medicare
%20Today%2007-25-2014%20FINAL.pdf
10 Medicare Payment Advisory Commission, “Report to Congress: Medicare Payment Policy,” March 2015. P. 374.
11 Congressional Budget Office, March 2015 Medicare Baseline, March 9, 2015.
http://www.cbo.gov/sites/default/files/cbofiles/attachments/44205-2015-03-Medicare.pdf
12Turner, GM, “Part D can be a model for Medicare reform,” The Hill. March 14, 2013. http://thehill.com/blogs/congress-
blog/healthcare/288147-part-d-can-be-a-model-for-medicare-reform
6You can also read