MonIToring surve Y - The cu Rrent stat E of Angina popuLation and heart rate
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The cuRrent statE of Angina
treatment in outpatient
popuLation and heart rate
monIToring surveY
Source: Fréquence des infarctus du myocarde
Meyer K. et al., Kardiovask, Med. 2007;10:279–284
http://www.obsandaten.ch/indikatoren/8_3_11/2004
CVD
Heart Disease
CHD
Stroke
Cooper et al., Circulation, 2000: 102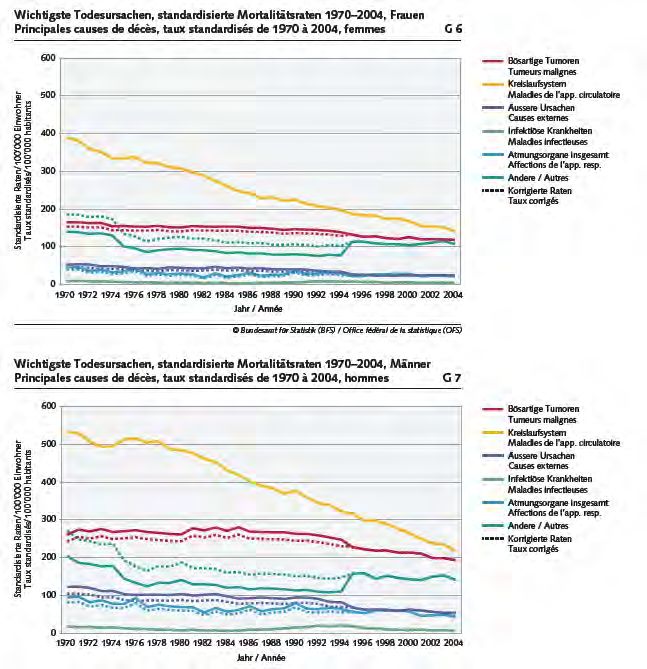
Qu’est qu’un facteur de risque
cardiovasculaire ?
“C’est une condition associée avec un risque augmenté de développer
une maladie cardiovasculaire.
L'association est au début toujours statistique. Ainsi le fait qu'une
personne particulière ait un facteur particulier augmente simplement la
probabilité de développer un certain type de maladie cardio-vasculaire.
cela ne signifie en aucun cas qu’il ou elle soit sûre de développer la
maladie cardiovasculaire.
Réciproquement, le fait qu'un individu n'ait pas un facteur de risque
cardio-vasculaire particulier ne garantit pas la protection contre une
maladie cardiovasculaire”
Dr. William KanneI, premier directeur de l’étude Framingham
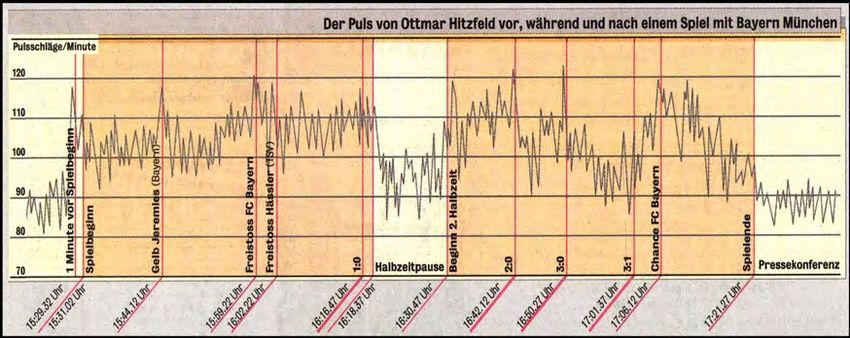
FCR et mortalité chez l’ Homme
Population générale
Insuffisance cardiaque Mort subite
70.0 6.0
Evénements/1000 patients x 2 ans
Evénements/1000 patients x 2 ans
66-94 35-84
52.5 4.5
35.0 3.0
17.5 1.5
15 25 48 63 1.1 2.5 3.1 4.7 5.9
0 0
< 64 65-74 75-84 >85/min 65 74-79 >88/min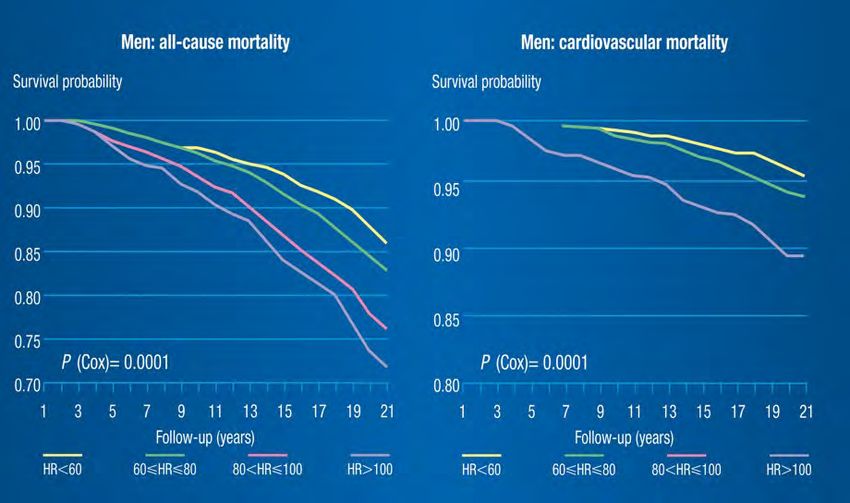
Relationship between heart rate and cardiovascular mortality
in the general and hypertensive population
J Clin Epidemiol 2006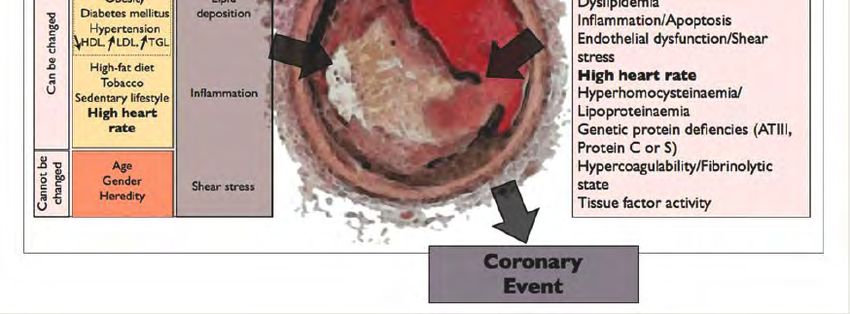
Pouls et pression artérielle humérale
pendant examen final
Facteurs de risque CV
Syndrome
métabolique
Obésité
Diabète sucré Dépôts
Hypertension lipidiques
Modifiables
artérielle
HDL, LDL, TGL
Diète
Tabac Inflammation
Alcool
Exercice
physique
Âge
modifiables
Contraintes de
Sexe
Non-
cisaillement
Hérédité
Uexküll T, Wick E: Arch Kreislaufforsch 39: 236-271; 1962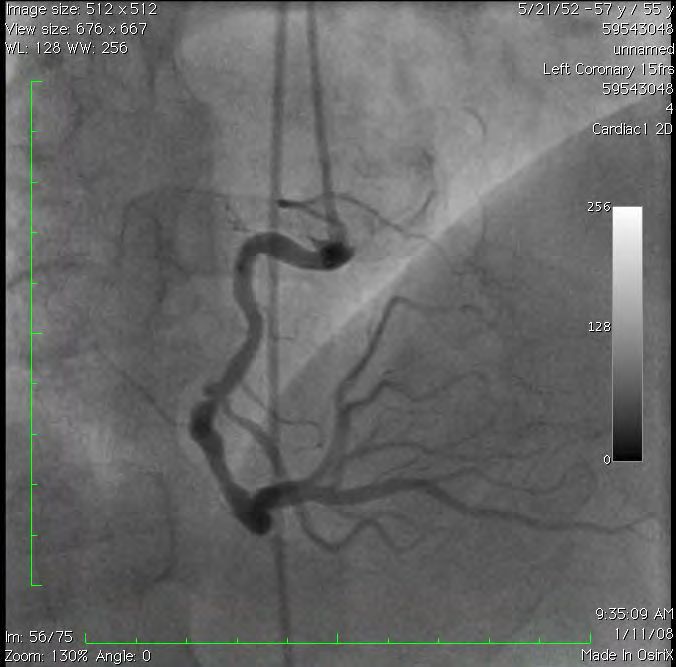

Coronary
Heart
Atherosclerotic Plaque Rupture
Plaque
Plaque Growth Risk Factors for Plaque Rupture
Risk Factors for Plaque Growth Diabetes mellitus
Smoking
Metabolic Dyslipidemia
syndrome
Inflammation/Apoptosis
Obesity Lipid
Diabetes mellitus deposition Endothelial dysfunction/Shear
Can be changed
Hypertension stress
HDL, LDL, TGL High heart rate
High-fat diet Hyperhomocysteinaemia/
Tobacco Lipoproteinaemia
Sedentary lifestyle Inflammation Genetic protein defiencies (ATIII,
High heart Protein C or S)
rate
Hypercoagulability/Fibrinolytic
state
Cannot be
Age Tissue factor activity
changed
Gender Shear stress
Heredity
Coronary
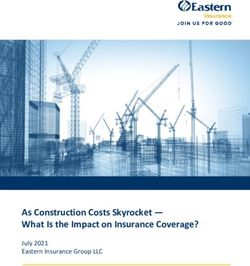
EventCardiovascular events during Soccer
Coronary
Worldcup in Germany
Heart
Atherosclerotic Plaque Rupture
Plaque
Plaque Growth Risk Factors for Plaque Rupture
Risk Factors for Plaque Growth Diabetes mellitus
Smoking
Metabolic Dyslipidemia
syndrome
Inflammation/Apoptosis
Obesity Lipid
Diabetes mellitus deposition Endothelial dysfunction/Shear
Can be changed
Hypertension stress
HDL, LDL, TGL High heart rate
High-fat diet Hyperhomocysteinaemia/
Tobacco Lipoproteinaemia
Sedentary lifestyle Inflammation Genetic protein defiencies (ATIII,
High heart Protein C or S)
rate
Hypercoagulability/Fibrinolytic
state
Cannot be
Age Tissue factor activity
changed
Gender Shear stress
Heredity
Coronary
Event
NEJM 2008Increased heart rate may contribute to coronary plaque
disruption
2002 2004 2004 2009
Heidland UE, Strauer BE. Circulation. 2001;104:1477-1482.High resting heart rate: an independent predictor
of mortality in the French general population
c a r d ia q u e é le v é e
Fréquence
-
s . F a c te u r d e r is q u e ?
Marqueur de risque v
Benetos A et al.Hypertension. 1999;33:44-52.Ivabradine shifts the patients from
high risk to low risk
8
HR >70 bpm in placebo
(mean HR = 79 bpm)
-36%*
fatal or nonfatal MI (%)
Hospitalization for
4 HR 70 bpm with Procoralan
(mean HR = 66 bpm after treatment)
0 *P=0.001
**P=0.0066
0 0.5 1 1.5 2
Years
Fox K et al. Lancet. 2008;372:807-816.Cascade Stabilité
ischémique de plaque
Contrôle des Contrôle des
symptômes événements
Cook S & Hess OM, European Heart Journal, 2009The cuRrent statE of Angina treatment in outpatient popuLation and heart rate monIToring surveY
Objectives of REALITY To characterize resting heart rate and medication of the population with stable angina pectoris in outpatient clinics To correlate angina pectoris events to heart rate. To evaluate the impact of angina pectoris on quality of life
Study design
Cross-sectional epidemiological study
Data acquisition by 33 Swiss cardiologists in
clinical practice
Mock Sigwart Grobéty
Gillard-Berguer Reynard
Bacchocchi-Suilen
Jaussi
Koerfer Burri Ricou
Pasquier Perret Bérubé
Vulliemin Bosquet Fiori
Savcic Goy DepeursingeBaseline data:
Cardiovascular risk factors
Total 283 coronary disease patients (202 male, 81 female)
Mean heart rate at rest [bpm] 69
(min-max) (46-126)
Smoker 45 (16%)
Mean systolic blood pressure [mmHg] 140.0
(min-max) (98-202)
Mean diasolic blood pressure [mmHg] 80.8
(min-max) (54-100)
Hypertension 191 (67%)
Mean BMI [kg/m2] 26.8
(min-max) (17.9-39.5)
Diabetes Mellitus 74 (26%)CAD
Mean time since diagnosis of a stable
4.25 (0.02-36.7)
angina pectoris [years] (min-max)
Myocardial infarction 84 (30%)
Coronary artery bypass graft (CABG) 35 (12%)
Percutaneous coronary intervention
142 (50%)
(PCI)
PCI & CABG 23 (8%)Cardiovascular risk factors
Mean heart rate at rest [bpm] 69
(min-max) (46-126)
resting resting
heart rate heart rate
70 bpmAssociation of resting heart rate with major
cardiovascular risk factors
70 bpm
(n=157) (n=126)
Atrial fibrillation % 10 13 NS
Heart failure % 8 10 NS
Cerebrovascular diseases % 9 17 p < 0.05
Hypertension % 62 74 p < 0.05
Diabetes mellitus % 21 33 p < 0.05
Dyslipidemia % 83 90 NS
Obesity, BMI > 27 kg/m2 % 37 52 p < 0.01
Patients with heart rate >70 bpm suffer significantly more from additional
cardiovascular risks than patients with heart rateFCR et mortalité chez Physiopathologie -
l’ Homme Acquis
Coronary Artery Surgery Study
24 913 patients avec maladie coronarienne
suspecte ou prouvée
Diaz A, et al., European Heart Journal (2005) 26, 967–974How do angina pectoris events and
heart rate correlate?
Angina pectoris events per week
Angina pectoris events/ week
4
3 3.8
3.3
2.8
2.7
2
n=86 n=71 n=62 n=62
≤60 61-69 70-77 ≥77
Subgroups by bpmFCR et mortalité chez Fréquence cardiaque et
l’ Homme Espérance de vie après
infarctus du myocarde
Analyse de l’étude GUSTO-I
* ECG à l’admission
Admission pour infarctus aigu du 41’021 patients
myocarde Mortalité à 30 jours
*
Hathaway WR,et al. Jama. 1998;279(5):387-391.
GUSTO-I: Global Utilization of Streptokinase
and t-PA (alteplase) for Occluded Coronary
ArteriesClassification of severity of angina by the
CCS: Canadian Cardiology Society Scale
CCS IV = Inability to perform any
activity without angina or
angina at rest, i.e., severe
100% limitation
CCS III = Symptoms with everyday
75%
living activities, i.e.,
moderate limitation
50%
CCS II = Slight limitation, with
angina only during vigorous
25%
physical activity
0% CCS I = Angina only during
≤60 61-69 70-77 ≥77 strenuous or prolonged
physical activity
Subgroups by bpmObjective 2
How does angina pectoris influence
habits and quality of life of CD
patients?Restenosis and Quality
Bénéfices des DES of Life
Functional Status
No Revasc Repeat Revasc
P=0.03 P=Limitation of everyday living activities
Whole p
70 bpm
population difference
(n=157 ) (n=126 )
(n=283 ) 70
Fear of angina pectoris
events leads to limitation
26% 38% 31% p < 0.05
of physical activity
(despite treatment)
Regular physical activity 60% 47% 54% p < 0.05
•Fear from angina pectoris events leads to limitation of everyday living activities in many CD
patients.
Subgroup heart rate >70 bpm significantly more affected than subgroup 70 bpm are significantly less physically active than
patients of the subgroup heart rateEvaluation of CAD treatments in
Switzerland
Whole
70 bpm p Difference
population
(n=157) (n=126) 70
(n=283)
Invasive treatments 75% 67% 72% NS
Nitrates 51% 51% 51% NS
Calcium antagonists 30% 40% 34% NS
Coronary therapy 24% 25% 25% NS
Beta-blockers 81% 67% 75% p < 0.01
No Beta-blockers because of
7% 18% 13% NS
contraindication
Antianginal therapy per
4.26 4.51 4.37 NS
patient (11 months)
Increase of heart rate
3% 17% 9% p < 0.001
since diagnosisHeart rate reduction is associated with
a decrease of post-MI cardiac deaths
Meta-regression of 12 controlled studies
2.0
1.0
Odds ratio
0.5
0.2
β-Blockers PComparison Europe wide –
cardiovascular risk factors
EUROASPIRE II1 2000/2001 EUROASPIRE III1 REALITY CH
Risk factors 1999-2000 Survey CH2 2006-2007 2008
n = 2975 n=565 n = 2392 n=283
Age (years) 59 68 60 69
Angioplasty % 28 62 50 72
Smoker % 21 18 18 16
Obesity % 33 - 38 44
Hypertension % 58 65 61 67
Dyslipidemia % 75 71 46 87
Diabetes % 20 22 28 26
1 Wood DA et coll. Abst. 316. Hot Line I, ESC 2007, Vienne, Autriche - 2 National survey on prescription of cardiovascular drugs among
outpatients with coronary artery disease in switzerland. Swiss Med Wkly 2003;133:88-92Comparison Europe wide - treatment
EUROASPIRE II1 2000/2001 EUROASPIRE III1 REALITY CH
Treatment 1999-2000 Umfrage CH2 2006-2007 2008
n = 2975 n=565 n = 2392 n=283
Antithrombotic
agents % 84 84 93 99
Beta blockers % 69 71 85 75
ACE-blockers &
Sartans % 49 47 74 65
Statins % 57 - 87 84
1 Wood DA et coll. Abst. 316. Hot Line I, ESC 2007, Vienne, Autriche - 2 National survey on prescription of cardiovascular drugs among
outpatients with coronary artery disease in switzerland. Swiss Med Wkly 2003;133:88-92Latéral Inférieur Latéral Inférieur Latéral Antérieur
Aspirine 100 mg/d
CK 3250 U/l Plavix 75 mg/d
LVEF @ D3: 45 % Coversum 5 mg/d
Torem 5mg/d
Medicaments ? Concor 5mg/d
Crestor 10 mg/d
FCR 74 bpm Concor 10mg ou
Procoralan 5mg/d ?Merci
Multiple cardiac effects of heart rate
MVO Neurohormonal
Myocardial systems
perfusion Ion fluxes
Autonomous Myocardial
nervous system Heart rate
relaxation
Arterial Myocardial
compliance contraction
Plaque Myocardial
rupture gene expressionThe Bowditch phenomenon
Contractile force of frog heart increases
when paced at increasing frequency.
Henry Pickering Bowditch
(1840 – 1911)
Bowditch HP. Ueber die Eigenthuemlichkeiten der Reizbarkeit, welche die Muskelfasern
des Herzens zeigen.
Ber Sachs Ges Akad Wiss 1871; 23: 652-689. Courtesy of R. Lerch, MDEffect of long-term therapy with β-blocker on EF
1936 patients enrolled in 15 placebo-controlled trials
Packer et al, Am Heart J 2001; 141: 899-907
Courtesy of R. Lerch, MDForce-Frequency relationship
in normal and failing myocardium
Trabecula from human hearts
Stimulation frequency (/min)
"negative staircase"
Schillinger, Hasenfuss et al, Basic Res Cardiol 1998; 93 (Suppl. 1): 38-45
Courtesy of R. Lerch, MDIvabradine shifts the patients from
high risk to low risk
8
HR >70 bpm in placebo
(mean HR = 79 bpm)
-36%*
fatal or nonfatal MI (%)
Hospitalization for
4 HR 70 bpm with Procoralan
(mean HR = 66 bpm after treatment)
0 *P=0.001
**P=0.0066
0 0.5 1 1.5 2
Years
Fox K et al. Lancet. 2008;372:807-816.IVA
Fréquence cardiaque et Espérance de vie après
infarctus du myocarde
432 patients avec infarctus aigu ECG à l’admission et Holter 24 heures fin hosp.
343 hommes, 89 femmes;58 “Endpoints”: Mortalité et événements arrythmiques
±11 ans (Mort subite, fibrillation ventriculaire, tachycardie
ventriculaire soutenue).
Suivi: 41 mois
Mortalité à 30 jours
Mauss O, et al. J
Electrocardiol. 2005;
38_106-112The effects of a reduction in heart rate Lower oxygen consumption Improved diastolic coronary flow Anti-ischemic effects Increased ventricular fibrillation threshold Antithromboatherosclerotic effects Prevention of plaque rupture Prevention of cardiomyopathy Slower development and progression of IHD Prevention of acute and chronic ischemic events (CV death, sudden death, angina, AMI, CHF)
Implication of heart rate as a simple tool for
mortality risk estimation
Simple (part of routine clinical examination)
Predictive (demonstrated in large number of
epidemiological trials)
Cheap (does not request special equipment)
Easily interpreted
Useful to monitor improvement of managementConclusions CAD patients suffer from angina pectoris despite intensive treatments. Number and severity of angina pectoris events in patients with heart rate >70 is significantly higher than in subgroup heart rate 70 suffering significantly more the patients with 70 than
You can also read