National Drug Policy 2015 to 2020 - Minimise alcohol and other drug-related harm and promote and protect health and wellbeing - Ministry of Health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
National Drug Policy 2015 to 2020 Minimise alcohol and other drug-related harm and promote and protect health and wellbeing
Citation: Inter-Agency Committee on Drugs. 2015.
National Drug Policy 2015 to 2020. Wellington: Ministry of Health.
Published in August 2015 by the Ministry of Health
PO Box 5013, Wellington 6145, New Zealand
ISBN: 978-0-478-44856-6 (print)
ISBN: 978-0-478-44857-3 (online)
HP 6239
This document is available at health.govt.nzForeword
The Government’s approach to implement are both proportionate There is still, however, a lot to do.
minimising harm from alcohol and to the potential for harm and The Government has set a range of
other drug misuse needs to be evidence-based. Better Public Services targets and
compassionate, innovative and other social sector initiatives to
In relation to alcohol, the
proportionate. This recognises make New Zealand a better place to
Government has already responded
that alcohol and other drug live for all New Zealanders. These
by tightening the rules on the sale
problems are first and foremost targets and initiatives include
of alcohol and putting more control
health issues. reducing long-term welfare
in the hands of local communities
dependence, supporting vulnerable
Compassion is crucial. Help through the Sale and Supply of
children, boosting skills and
needs to be available for those Alcohol Act 2012, reducing the
employment, and reducing crime.
who need it, interventions need blood-alcohol limit for driving and
When we dig beneath the surface
to happen early, and the stigma increasing alcohol screening and
of many of the issues we need to
that acts as a barrier to help brief interventions in primary care.
address to achieve these outcomes,
seeking and recovery needs to be
Actions are also included in this we find that misuse of alcohol and
reduced. This National Drug
National Drug Policy as the drugs is a contributing factor.
Policy emphasises the need for
Government’s response to the Law
a people-centred intervention There is no quick fix. Progress will
Commission’s recommendations
system that is responsive to take time, and will require
on the Misuse of Drugs Act 1975.
people’s circumstances, coordinated action across the social
These relate to ensuring the Expert
environment and life stages. sector and other agencies to
Advisory Committee on Drugs has
understand where to target
We also have to be prepared to appropriate decision-making
resources and provide wrap-around
challenge traditional approaches guidance, ensuring appropriate
support. Partnership with non-
and ways of thinking about these access to controlled drugs for
governmental organisations,
issues. Innovation is essential medical purposes (while minimising
businesses, communities and
in a world where new drugs are the risk of diversion), and assessing
families will also be vital in
detected every week and the black options for possession and utensils
minimising alcohol and other drug
market has gone digital. The offences to incorporate an
related harm. As Minister
international landscape has also enhanced health response.
responsible for this Government’s
shifted, with a growing recognition
New Zealand continues to make policy on alcohol and other drugs,
that the harms we are trying to
strong progress in minimising I will work with my ministerial
prevent can come from our
alcohol and other drug harm. colleagues to ensure not only that
approach to drugs as much as
Hazardous consumption of alcohol agencies have a coordinated
from their use.
has decreased over the last six approach to this issue, but that we
Different drugs have different risk years from 18 percent in 2006/07 to work with those who deliver
profiles and our responses to them 16 percent in 2013/14. The Prime services and interventions to make
need to reflect this. In some cases, Minister’s Methamphetamine New Zealand a better place.
such as with methamphetamine, Action Plan has helped to more
we want to eradicate all supply and than halve the reported rates of
use. For alcohol, we want those who amphetamine use. The combined
choose to drink to do so moderately focus on restricting the supply of
and those who are pregnant or methamphetamine and its
planning pregnancy not to drink at precursors, with treatment and Hon Peter Dunne
all. When legislating to try and community-based initiatives has Associate Minister of Health
reduce harmful behaviour we need contributed to this reduction.
to ensure the rules and penalties we
National Drug Policy 2015 to 2020 iiiContents
Foreword iii
Introduction 1
New Zealand has high rates of alcohol and other drug use 1
Misuse of AOD harms individuals, communities and society 1
Taking action to minimise harm means looking at the whole picture 2
An investment-based approach ensures support goes where it will make the biggest difference 2
A collaborative response to AOD harm is needed 3
The Government is committed to getting results 3
Our approach for the next five years 4
A shared goal provides a foundation for collaboration 4
Clear objectives focus us on results 6
Evidence-based strategies ensure we are doing the right things 6
Our priorities enable us to achieve results 7
Our objectives 8
Delaying the uptake of AOD by young people 8
Reducing illness and injury from AOD 10
Reducing hazardous drinking of alcohol 12
Shifting our attitudes towards AOD 14
Our strategies 16
Our priorities for Government action 18
Priority area 1: creating a people-centred intervention system 18
Priority area 2: shifting thinking and behaviour 20
Priority area 3: getting the legal balance right 21
Priority area 4: disrupting organised crime 22
Priority area 5: improving information flow 24
Summary of Government actions 25
References 27
Further resources 30
National Drug Policy 2015 to 2020 vIntroduction
The National Drug Policy sets out our response as a society to alcohol and other
drug1 (AOD) issues. The Government will use the Policy to prioritise its resources
and assess the effectiveness of the actions taken by government agencies and
frontline services.
The Policy aims to guide, influence and support decision-making by local
services, communities and non-governmental organisations, and in doing so,
improve collaboration and maximise the effectiveness of the system as a whole.
New Zealand has Some people are psychologically Misuse of AOD
or physiologically dependent on
high rates of alcohol these substances. This means they
harms individuals,
and other drug use have become so used to having communities and
Over a lifetime 44 percent of
AOD in their system they need to society
keep using them in order to
New Zealanders will have tried an While not every instance of
function normally. It is estimated
illegal drug and 93 percent will AOD use is harmful, the effects
that 12 percent of the population
have drunk alcohol (Ministry of of these substances can be
will experience a substance use
Health 2015b). A number of adults significant. Immediate harms
disorder at some stage in their
aged 15+ use illegal drugs: related to AOD use include falls,
lives (Wells et al 2007).
→→1 in 13 smoke cannabis at Additionally, a recent study found road accidents and the clogging
least once a month (Ministry that approximately 11 percent of up of hospital accident and
of Health 2015b)2 New Zealand secondary school emergency departments. Harms
→→1 in 37 have used ecstasy students use substances at a level can also arise over the long term,
in the last year(Ministry of that are likely to cause them such as AOD-related health
Health 2015b) significant current harm and may conditions, relationship issues
→→1 in 100 have used amphetamine cause long-term problems (The and difficulty obtaining and
in the last year (Ministry of University of Auckland 2014). maintaining employment.
Health 2014c).
1. Other drugs include: substances classified under the Medicines Act 1981 or Misuse of Drugs Act 1975 and not used within the controls set out in legislation
or for their intended purpose; substances captured by the Psychoactive Substances Act 2013; and other substances such as solvents and aerosols.
2. Data for cannabis and ecstasy use in the last 12 months (as at 2012/13) are provisional and potentially subject to revision or change until they have been
through the full quality assurance process and received final approval for release.
National Drug Policy 2015 to 2020 1For example, approximately 4500
people receiving a health-related
Taking action to An investment-
benefit have a primary diagnosis minimise harm based approach
of alcohol or substance abuse means looking at ensures support
and a quarter of these people the whole picture goes where it will
have received a benefit for at least
10 years. AOD policy cannot be viewed in make the biggest
AOD-related harm does not occur
isolation from social factors (such difference
as income, employment, housing
in a vacuum. The harm experienced Harmful use of AOD has been
and education) that may make
depends on a complicated web of estimated to cost our country
people more at risk of being
factors, including the substance(s) around $6.5 billion each year
affected, directly or indirectly, by
involved, the extent of use, the (Business and Economic Research
harm from AOD. Effective
method of use, the vulnerabilities Limited 2009). This includes the
government intervention requires
of the person using AOD, and the cost to healthcare of responding
a cross-agency response. Health
environment in which AOD is used. to AOD related accidents, illnesses
care, education and social services,
Harmful impacts of AOD are not and injuries, the cost of welfare
alongside the justice system,
restricted to the individual using payments for people who have
communities, families and whānau
the substance. Examples of become incapacitated through
play critical roles in minimising
AOD-related harm to others substance dependence and the
harm from AOD.
include violence, foetal AOD costs to the criminal justice
The complexity of these issues system of enforcing AOD-related
exposure, family break-up and
means that our responses need legislation.
child neglect, property crime and
to be flexible, targeting the
public health issues such as the By focussing on prevention and
needs of different populations,
spread of hepatitis. early intervention at the
family and whānau situations and
Problematic AOD use is often population level, through to
environments, and responding
multi-generational and can be targeted, people-centred
to emerging issues early.
normalised within family and responses for those individuals
Approaches need to be evaluated,
whānau groups. Such patterns of who need greater support, we can
tested and refined using domestic
behaviour may also normalise reduce these harms and their flow
and international evidence and
actions that will bring people, on effects to families, whānau,
best practice.
particularly young people, into communities and the wider public.
New Zealand is not alone in The Policy’s first Priority Area for
contact with the criminal justice
facing the challenge of reducing action is targeted specifically at
system, such as cannabis offences
harm caused by AOD. We can learn ensuring a people-centred
or drink driving.
from international practice, policy intervention system.
Particular populations often and structures. This includes
experience a disproportionate international agreements, such
amount of harm. For this Policy to as the United Nations Drug
be successful, harm needs to be Conventions, trade agreements and
minimised for all populations. human rights instruments. The
Government will monitor innovative
approaches as they are tested
internationally, including
experimental regimes that make
cannabis available for medicinal use.
2 National Drug Policy 2015 to 2020A collaborative →→Employers can offer a chance
to people who are in the process
the Ministries of Health, Justice,
Social Development, and Education,
response to AOD of recovering from substance the New Zealand Police, the
harm is needed dependence. Department of Corrections, and
the New Zealand Customs Service.
There are many people and →→Frontline services can provide
The Accident Compensation
organisations – including district appropriate interventions, plans
Corporation, National Drug
health boards, service providers, iwi and treatment for those who
Intelligence Bureau, Health
and hapū groups, schools, churches need help.
Promotion Agency and Te Puni
and community organisations – Government agencies have a Kōkiri also participate at the
making a difference by minimising role by collaborating, supporting working group level. This collection
AOD-related harm and working and partnering with others to of agencies will ensure integration
to promote and protect health achieve common goals. In between the delivery of this Policy
and wellbeing. Indeed, everyone particular, the principles of and broader Social Sector
can have a role in minimising partnership, participation and objectives.
AOD harm. protection will continue to
The IACD will report to the
→→Individuals can take action underpin the relationship between
Government annually. Their
to reduce harmful use. government and Māori to achieve
advice will cover progress on
pae ora3 and health equity by
→→Family, whānau and friends implementing actions, whether
supporting the health and
can support someone to make objectives are being achieved, and
wellbeing aspirations of Māori.
changes in their use. any changes to actions and
timelines that may be required as
→→Community members and
leaders can advocate for The Government is evidence emerges. The IACD will
also provide advice on whether
positive AOD policies in committed to achieving the objectives of this
community settings such as
a local sports club, and also
getting results Policy is helping to drive progress
on the government’s broader social
model responsible AOD use. The Government has instructed the
sector goals, including the Better
Inter-Agency Committee on Drugs
→→Educational institutions can Public Services Result Areas.
(IACD) to oversee the
introduce policies to support
implementation of actions and
students struggling with
monitor progress made against the
AOD issues to stay engaged
objectives set out in this Policy. The
in education.
Inter-Agency Committee on Drugs
brings together chief executives of
3. Pae ora is a holistic concept including three interconnected elements of mauri ora (healthy individuals), whanau ora (healthy families) and wai ora (healthy
environments). Pae ora is also the Government’s vision for Māori health and can be accessed through http://www.health.govt.nz/our-work/populations/
maori-health/he-korowai-oranga/pae-ora-healthy-futures.
National Drug Policy 2015 to 2020 3Our approach for
the next five years
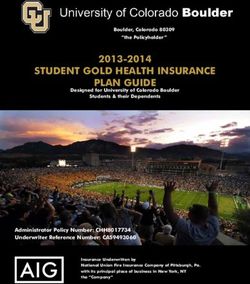
The Government’s approach over the next five years includes a shared goal,
objectives, strategies and priorities for action. This approach, and its
contribution to wider social sector outcomes, is summarised in Figure 1 and
discussed in detail in the rest of the chapter.
A shared goal
provides a
foundation for
collaboration
The goal of this Policy is to Making progress towards this
minimise AOD-related harm and goal will impact on wider social
promote and protect health and objectives, and in particular four
wellbeing for all New Zealanders. of the Better Public Services
The idea of harm minimisation Result Areas in relation to
encompasses the prevention and reducing welfare dependency,
reduction of health, social and supporting vulnerable children,
economic harms experienced by boosting skills and employment
individuals, their families and and reducing crime.
friends, communities and society
from AOD use. The promotion and
protection of wellbeing integrates
physical, mental and social needs
to strengthen protective factors
for individuals, families and
communities.
4 National Drug Policy 2015 to 2020Figure 1: The framework for the National Drug Policy 2015–2020
Contribution to social sector outcomes
Reducing welfare Supporting Boosting skills and
Reducing crime
dependency vulnerable children employment
Goal
To minimise AOD-related harm and promote and protect health and wellbeing.
Objectives
Delaying the uptake of Reducing illness and Reducing hazardous Shifting our attitudes
AOD by young people injury from AOD drinking of alcohol towards AOD
Strategies
Problem limitation Demand reduction Supply control
Barriers to people accessing People have the knowledge, Access to AOD for harmful
and receiving support or skill and support to make use is minimised
treatment for their own or good decisions about their
others’ AOD use are removed AOD use
Priority areas
Creating a
Shifting Getting the Improving
people-centred Disrupting
thinking and legal balance information
intervention organised crime
behaviour right flow
system
National Drug Policy 2015 to 2020 5Clear objectives Evidence-based
focus us on results strategies ensure
As well as having a shared goal, we are doing the
we need clear objectives to provide right things
a focus over the entire life of the Demand reduction aims to
This Policy provides a structure
Policy. These objectives are: reduce the desire to use AOD.
for the wide range of activity
It includes activities that delay
→→delayed uptake of AOD by already being undertaken by
or prevent uptake. This means
young people the Government and others to
reducing use through education,
minimise harm and to promote and
→→reduced AOD-related illness health promotion, advertising and
protect wellbeing. The activities can
and injury marketing restrictions, and
be categorised under three broad
influencing the conditions that
→→reduced hazardous drinking strategies, or ‘pillars’: problem
make people turn to AOD through
of alcohol limitation, demand reduction and
community action, such as keeping
→→a shift in attitudes towards supply control. These pillars are
children in school.
AOD. underpinned with high quality
data to ensure the right balance
Progress on these objectives will and targeting of activity. These
mean progress on reducing overall strategies also act as a guide for
harm from AOD. To know whether new initiatives.
progress is being made, high-level
indicators and measures have The approach is similar to that used
in other countries, including the Supply control aims to prevent
been developed. These will be
United Kingdom, Australia and many or reduce the availability of
based on the latest available data
nations in the European Union. AOD. It includes controlling
and will enable high-level trends
New Zealand’s borders to prevent
to be assessed.
illegal drugs being imported,
and shutting down domestic
growing, manufacturing and
supply. It also aims to control
and manage the supply of legal
Problem limitation aims to drugs through things like
reduce harm that is already prescribing guidelines, age
occurring to those who use AOD or restrictions, licensing conditions
those affected by someone else’s and permitted trading hours.
AOD use. It includes activities that
provide safer equipment and
environments for AOD use, ensure
access to quality AOD treatment
services through New Zealand’s
health system, and support people
in recovery. It also includes
activities that support others who
are affected, such as the children of
people with dependence problems.
6 National Drug Policy 2015 to 2020Our priorities enable Each priority area has an initial set
of actions to be undertaken by
us to achieve results 2017/18. These actions are drawn
This Policy identifies five areas from across the three strategies
that will require additional focus and build on, rather than replace,
over the next five years if the the significant contributions
Government is to make meaningful government, communities and
progress against the objectives: individuals already make to the
goal and objectives of this Policy.
→→Priority area 1: creating a people-
centred intervention system Many of the initial actions are
designed to enhance collaboration
→→Priority area 2: shifting thinking and links across government,
and behaviour service providers and communities
→→Priority area 3: getting the legal in order to achieve better outcomes
balance right collectively than can be achieved
alone. This collaborative approach
→→Priority area 4: disrupting recognises that everyone has a role
organised crime in minimising AOD-related harm,
→→Priority area 5: improving but that the Government has a
information flow. responsibility to lead.
The initial actions are also
designed to build a foundation to
better enable individuals, families
and communities to contribute to
the Policy’s goals and objectives,
and to support prevention and
intervention activity, particularly
for young people.
National Drug Policy 2015 to 2020 7Our objectives
Delaying Early uptake of AOD
is a predictor for
ongoing problems,
the uptake including substance
use and dependence.
of AOD by Early use of AOD raises very
serious issues for our children
young people
and society. The brain does not
fully mature until the third decade
of life, and the evidence suggests
that exposure to AOD during
adolescence and young adulthood
may interrupt important
neurological processes and natural
Around 75 percent of people who develop a brain maturation. This can have
consequences for social and
substance use disorder (eg. substance abuse neurobiological functioning in
or dependence) will do so by the age of 25 adulthood (Squeglia et al 2009;
(Wells et al 2007). Office of the Prime Minister’s
Science Committee and Gluckman
2011). This is more likely when
By age 15 one in four people have drunk alcohol people start using AOD earlier
(early onset) and do so regularly
and one in six have used an illegal drug (Ministry
or heavily.
of Health 2015a and 2015b).
Early onset of alcohol consumption
tends to increase the likelihood of
By the age of 21 approximately 80 percent of young regular and heavy use and has been
associated with increased rates of
New Zealanders will have used cannabis, with
violence and injury, unprotected
10 percent developing a pattern of heavy, dependent sex, mental health problems,
use (Office of the Prime Minister’s Science Advisory suicide, poorer educational
outcomes and problem drinking
Committee and Gluckman 2011). later in life (Dawson et al 2008;
Fergusson et al 1994; Hingston et al
2006, 2009; Komro et al 2010;
Office of the Prime Minister’s
Science Advisory Committee, 2011;
Swahn et al 2010). Of adults aged
15 years and over who reported
drinking hazardously in the past
12 months 48 percent had first
used alcohol before age 15
(Ministry of Health 2015b).
8 National Drug Policy 2015 to 2020The evidence highlights that early can also influence use. We know were the second most prevalent
onset of cannabis use also tends people are more likely to use drugs reason cited by school boards for
to increase the likelihood of such as cannabis when their peers exclusions4 in 2013, accounting for
misuse, as well as mental health are doing so (Kuntsche and 17 percent, and the main reason for
issues, other illicit drug use, school Delgrande 2006) and that social expulsions5, at 34 percent (Ministry
drop-out and educational and parental modelling influences of Education 2013). Not being able
underachievement, neurocognitive youth AOD use. There is also a to participate fully in school life
deficits and injury (Meier et al. strong genetic component to AOD can limit a young person’s ability
2012; Office of the Prime Minister’s issues (Office of the Prime to gain employment, sustain
Science Advisory Committee 2011; Minister’s Science Advisory relationships and make life
Silins et al 2014). Committee 2011). choices. Similarly, consequences
from interaction with the criminal
Early use and misuse of AOD is The way that we respond to young
justice system from low-level
linked to a range of social and people’s use of AOD can have
AOD-related offending can be far
environmental factors, including life-long consequences.
reaching. During 2013/14 (ie, fiscal
exposure to traumatic life Accordingly, the Prime Minister’s
year ending 30 June 2014) 2410
experiences such as child abuse Chief Science Advisor warns
police proceedings6 for illicit drug
and neglect, family violence and against responding punitively to
possession or use against youth
household dysfunction (Office of behaviours that reflect incomplete
(aged 5–24) were recorded, with
the Prime Minister’s Science maturation (Office of the Prime
approximately a quarter resulting
Committee and Gluckman 2011). Minister’s Chief Science Advisor
in court action.7
The way young people socialise 2011). Drugs (excluding alcohol)
Table 1: Indicator for delaying the uptake of AOD by young people
Indicator of success Delayed uptake of alcohol and other drugs by young people
Measure Initiation of first use as reported by adults aged 15+ years
Data source New Zealand Health Survey (5 yearly)
(Alcohol) Baseline 2012/13
Under 15: 27%; 15-19: 60%; 20-24: 10%
(Other drugs) Baseline: 2012/138
14 and under: 16%; 15-17: 33%; 18-20: 29%
4. Exclusion means the formal removal of a student aged under 16 from the school and the requirement that the student enrol elsewhere.
5. Expulsion means the formal removal of a student aged 16 or over from the school. If the student wishes to continue schooling, he or she may enrol
elsewhere.
6. Proceedings include court action, formal and informal warnings, non-court referred conferences and other non-court action.
7. These figures have been produced from a statistical dataset that is still under development, and which will, in the future be used to produce Recorded
Crime Offender Statistics. Those Tier 1 statistics should be available from 1 July 2015.
8. Data for other drug use in the last 12 months (as at 2012/13) are provisional and potentially subject to revision or change until they have been through
the full quality assurance process and received final approval for release.
National Drug Policy 2015 to 2020 9Reducing AOD misuse
has serious
consequences
illness for the health of
New Zealanders.
and injury AOD taken recreationally produces
physiological changes to the body.
from AOD
These effects are generally
intended to be pleasurable, but
they also have the potential to
cause considerable harm to the
people that use them and to
others. Each year about 150,000
New Zealanders aged 16 and older
Approximately 12 percent of New Zealanders will experience substance use problems
that could benefit from an
experience a substance use disorder at some stage intervention (Mental Health
in their lives (Oakley et al 2006). Commission 2011). Different drugs
also carry different risk profiles and
the impact on individuals will vary
AOD use accounts for about 5 percent of all health depending on their vulnerabilities,
loss9 experienced by New Zealanders and 23 percent environmental and social
circumstances and patterns of use.
of mental illness, mainly through substance use
Around 800 deaths per year are
disorders. Alcohol comprises the majority of this attributable to alcohol. Injuries are
loss (3.9% and 18% respectively) (Ministry of Health the dominant cause of alcohol-
2013b). attributable deaths for people
under 45, with alcohol-induced
cancers becoming increasingly
Sharing needles and other drug utensils remains dominant from the age of 45
the key route for hepatitis C virus transmission in (Connor et al 2013). Alcohol-
attributable injuries are estimated
New Zealand. Eighty-three percent of people with to account for 11 percent of all ACC
hepatitis C virus infection report a history of claims, at a cost of $350 million
per year (Accident Compensation
intravenous drug use (Gane et al 2014). Corporation 2012).
Regular and heavy cannabis
smokers are at increased risk of
contracting chronic bronchitis,
respiratory infections and
pneumonia when compared to
9. Health loss is a measure of how much healthy life is lost due to early death, illness or disability.
10 National Drug Policy 2015 to 2020non-smokers and may suffer communicable diseases. Availability transition plans between services
cancers of the lung (Room et of clean equipment will reduce – for example from specialist care
al 2008). harm: the introduction of the 1-for-1 to primary care – are important
needle exchange has reduced the tools to assist people with recovery.
Large doses of methamphetamine
rate of hepatitis C infection among
can cause potentially life- Reducing illness and injury from
people who currently inject drugs
threatening conditions, such as AOD includes having a focus on
by around 25 percent (Noller and
hypothermia, renal and liver failure, other people who are affected by
Henderson, 2014; Henderson
cardiac arrhythmias, heart attacks, an individual’s use, particularly
et al 2011).
strokes and seizures (Krasnova children. For example:
& Cadet, 2009; Drake et al 2008). Additionally, stopping use of
→→AOD misuse is a factor in
The long-term health impacts of alcohol or other drugs after daily
25 percent of families with
frequent methamphetamine use or frequent use over a couple of
children in Child, Youth and
can include respiratory problems, months can trigger withdrawal
Family care (Office of the Chief
stroke, irregular heartbeat, symptoms. Most people will
Social Worker 2014)
anorexia, and neurotoxicity as well experience mild to moderate
as affecting cardiovascular health, symptoms, but for some, the →→alcohol was a contributing
and cognitive functioning (Drake effects will be more serious (for factor in 34 percent of all family
et al 2008). example, alcohol and violence incidents in 2007/08
benzodiazepine withdrawal can be (Ministry of Justice 2010).
Rates of accidental poisonings
fatal (Bayard et al 2004; Lann and →→for every 100 alcohol or drug-
(including overdose) are higher for
Molina 2009)). impaired drivers or riders who
opioids such as heroin, methadone
and codeine than for any other Relapse is common, and people died in road crashes, 47 of their
illegal drug in New Zealand. These who have stopped using even for passengers and 17 sober road
substances are also the most likely a short period of time are at risk users died with them (Ministry
to be injected, which can cause vein of over-dosing should they resume of Transport 2014).
damage and increase exposure to use. Relapse prevention plans and
Table 2: Indicator for reducing illness and injury from AOD
Indicator of success Reduced AOD-related illness and injury
Measure Alcohol-related emergency department presentations
Data source Ministry of Health National Collections data (annual)
Baseline to be established in 2015/16
Measure Accidental poisoning by exposure to opioids
Data source Mortality collection, Ministry of Health
2011 baseline: 39
Measure People receiving a health-related benefit where primary diagnosis
is listed as alcohol or substance abuse
Data source Ministry of Social Development
March 2015 baseline: 4,435
National Drug Policy 2015 to 2020 11Reducing One in six
New Zealand adults
have hazardous
hazardous drinking patterns.10
drinking of
It is encouraging that both total
and hazardous consumption of
alcohol by New Zealanders aged
15+ has reduced over the last six
alcohol
years (Ministry of Health, 2014b).
→→The proportion of the adult
population who drink has
decreased from 84 percent in
2006/07 to 80 percent in
2013/14.
Men (22 percent) are twice as likely as women →→The proportion who drink
(11 percent) to drink hazardously. hazardously has decreased from
18 percent in 2006/07 to 16
percent in 2013/14.
One in three 18–24-year-olds drink at levels that are
Despite these positive trends, the
hazardous to their health (Ministry of Health 2014b). rates of hazardous drinking
continue to be high. Approximately
575,000 New Zealanders report
Alcohol contributes to around 30 percent of
drinking in a way that carries a risk
New Zealand’s fatal road crashes (Ministry of of harm to themselves and others
Transport 2014). around them. Additionally, while
total and hazardous consumption
of alcohol by young people aged
Approximately 10 percent of women drink heavily 18-24 also decreased between
during pregnancy (Ministry of Health 2015a). 2006/07 and 2013/14 (from 89 to
84 percent and 43 to 33 percent
respectively) this group remains
most likely to drink hazardously
(Ministry of Health, 2014b).
Hazardous drinking can contribute
to a number of social harms – not
just to individuals, but also to
those around them. The most
common harmful effects reported
10. Ministry of Health, 2014b. The Alcohol Use Disorders Identification Test (AUDIT) developed by the World Health Organization is used to identify hazardous
drinking patterns. The AUDIT is a 10-item questionnaire covering alcohol consumption, alcohol-related problems, and abnormal drinking behaviour.
Each question is scored from 0 to 4, so the questionnaire has a maximum score of 40. An AUDIT score of 8 or more is defined as hazardous drinking.
12 National Drug Policy 2015 to 2020by adults due to someone else’s (FASD), but they are preventable. There is also evidence that
drinking are damage to friendships For women who are pregnant or parental alcohol use can harm
and social life, and damage to planning a pregnancy, the safest children. Children with parents or
home life and financial position option is to avoid drinking alcohol. caregivers who drink heavily are
(Ministry of Health 2010). Alcohol likely to suffer from a greater
New Zealand has relatively high
consumption is also a factor in number of hospital admissions for
rates of alcohol consumption
offending behaviour. Police physical injuries (Families
during pregnancy, with up to a third
estimate that at least one-third of Commission 2006). Children raised
of New Zealand women consuming
recorded violent offences and by caregivers who are alcohol
some alcohol while pregnant, and
15 percent of sexual offences occur dependent can have higher levels
around 10 percent drinking heavily
after the offender has consumed of anxiety, behavioural problems
(Morton et al, 2010; Mallard et al,
alcohol (New Zealand Police 2009). and other mental health issues
2013; Ministry of Health 2015a). The
than children who do not have
Babies exposed to alcohol before Health Select Committee’s Inquiry
alcohol-dependent parents
birth can develop lifelong into Improving Child Health
(Maynard 1997). Research also
problems, including behavioural Outcomes and Preventing Child
suggests that children of alcohol-
problems, intellectual disability Abuse, with a Focus from Pre-
dependent parents are more
and heart defects. This can lead to conception until Three years of
likely to become alcohol
poor life outcomes and increased Age identified estimates of the
dependent themselves, creating
risk of involvement with the number of babies born each year
generational impacts (Jennison
criminal justice and welfare in New Zealand with FASD ranging
and Johnson 1998).
systems. There is no cure for Fetal from 173 to 3000.
Alcohol Spectrum Disorders
Table 2: Indicator for reducing hazardous drinking of alcohol
Indicator of success New Zealand past-year drinkers who report hazardous drinking patterns
Measure Hazardous drinking score (AUDIT) in past-year drinkers
aged 15 years and over
Data source New Zealand Health Survey (annual)
2011/12 Baseline: 19%
Measure Women who had been pregnant in the last 12 months
and drank during most recent pregnancy
Data source New Zealand Health Survey (5 yearly)
2012/13 Baseline: 19%
National Drug Policy 2015 to 2020 13Shifting our Social attitudes
towards AOD can
promote misuse and
attitudes act as barriers to
help-seeking and
recovery.
towards AOD Our attitudes are a key predictor of
our behaviour. They are shaped by
our individual values and beliefs,
the values and beliefs of our peers
Six percent of all adult past-year drinkers planned to and people of influence, and by our
surroundings, such as the
get drunk on their most recent drinking occasion, messages we are exposed to and
and 12 percent reported having ‘got drunk or had the rules set by the Government.
too much to drink’ on their most recent drinking People use AOD for many reasons,
occasion (Research New Zealand 2014). including enjoyment of the effects,
relaxation, alleviation of stress or a
depressed mood, to enhance an
Twenty-five percent of high school age students activity, to better bond with peers,
thought it was okay for people their age to drink and to keep awake at night to
socialise (Boys et al 2001; Duff
alcohol, and 10 percent thought it was okay to use 2008; Jay 1999). Young people
cannabis (almost the same number as for cigarettes) have also reported that they have
used drugs to ‘fit in’ with peers, to
(Adolescent Health Research Group 2013). cope with problems, to relieve
boredom, and to rebel (Ministry
Around 50,000 people wanted help to reduce of Health 2009b).
their AOD use in the past 12 months but had, for a Environmental factors contribute
to AOD use and can be a barrier to
variety of reasons, not received it (Mental Health help-seeking and recovery. These
Commission 2011). factors include ease of access to
substances, the presence of
violence in the home, peer
pressure, unemployment, and/or
mental health issues. Such factors
can in turn be exacerbated by
AOD use.
14 National Drug Policy 2015 to 2020In most cases AOD use is not of Health 2009b). For example, a control over their lives. This means
problematic. For example, many dedicated methamphetamine being able to be better parents, to
people enjoy moderate telephone helpline service found be employed, and to live as others
consumption of alcohol in social that many callers were deeply do. This can be difficult if they
settings with few ill effects. concerned about confidentiality encounter discrimination for their
However, harm can result when because of such fears. Information past actions. As well as their AOD
people misuse AOD, particularly that allowed them to self-manage use, their offending histories can
when social patterns of misuse and their issues was often considered severely limit future possibilities,
intoxication become entrenched. more important than seeing a for example, cannabis convictions
counsellor. Offering people a can limit someone’s ability to
There are many reasons why
variety of choices for treatment is travel overseas, or to get a job.
people who feel they need help for
more likely to change behaviour
their AOD use might not seek Over the medium to long term,
than limiting support to only a few
assistance to do so. These include achieving our objectives will
options. Several studies have
not being ready to stop use, not require shifting the attitudes of
found that substance use
knowing where to go for help or individuals and communities to
disorders are more highly
encountering long waiting lists, AOD use and misuse, and to
stigmatised than other health
and being concerned about the seeking help. But, as we have seen
conditions (Livingston et al 2012).
potential negative effects on with tobacco and drink-driving,
employment, or that receiving help Stigma can also impact people’s it is possible to shift attitudes
might cause others to have a recovery journey. For many people, over time.
negative opinion of them (Ministry recovery means assuming some
Table 4: Indicator for shifting our attitudes towards AOD
Indicator of success Shifting our attitudes towards AOD
Measure Adults aged 15+ who sought or have been given advice,
information or help on how to cut back their drinking
in the last 12 months11
Data source HPA Alcohol Behaviours and Attitudes Survey (annual)
Baseline 2013: 5%
Measure AOD outcome measure for AOD treatment services
Data source AOD treatment services reporting requirements to the
Ministry of Health
Baseline to be established in 2015/16
11. Note that this question is only asked of people who had consumed two or more drinks on their last drinking occasion (within the last three months).
National Drug Policy 2015 to 2020 15Our strategies
In order to achieve these objectives and move towards the goal of minimising
AOD harm and promoting and protecting health and wellbeing, we need clear
strategies for action. This Policy carries over from previous policies the three
strategies for action of problem limitation, demand reduction and
supply control.
Current activities by government, communities, families and individuals can
be categorised under one or more of these strategies, and these strategies
act as a guide for the development of new initiatives. The three strategies,
and examples of activities, are described in Table 5.
Table 5: National Drug Policy strategies and example activities
Problem limitation
Barriers are removed to people accessing and receiving
support or treatment for their own or others’ AOD use
New Zealand is working in this area to:
→→provide effective, high-quality, compassionate, timely, accessible,
and age- and culture-appropriate support and treatment services
→→address the factors that have an impact on people’s ability
to access treatment and support, including destigmatising
help-seeking
→→provide AOD services that are responsive to people with
co-existing problems
→→ensure all frontline services (justice, health, education, etc.)
provide an entry point to AOD support, referral and treatment
(including for the child affected by a parent’s addiction)
→→support and strengthen harm reduction approaches such as the
needle exchange programme
→→ensure continuity of care for people transitioning from one service
or environment to another, including from youth to adult services,
and between justice facilities and the community.
16 National Drug Policy 2015 to 2020All three strategies
Demand reduction are needed
People have the knowledge, skill and support to make good Often they work well together,
decisions about their AOD use but sometimes they come into
conflict and require a balancing
New Zealand is working in this area to: act. For example, fear of the legal
consequences of using an illegal
→→ensure messages about AOD harm, harm reduction and help-
drug can act as a barrier to some
seeking (including information about less harmful consumption
people seeking the help they need.
and means of administration) are consistent, evidence-based,
In these instances, assessment
accessible and relevant
of the best available evidence is
→→tailor messages, resources and services appropriately to respond needed to determine which mix
to different cultures, populations and communities of approaches is required to best
→→encourage women to abstain from AOD use (or use less harmful address social, economic and
substitutions, such as methadone, where appropriate) during health harms. This is harm
pregnancy and while breast feeding minimisation in action.
→→bring about a societal shift in attitudes about harmful AOD use.
Supply control
Access to AOD for harmful use is minimised
New Zealand is working in this area to achieve:
→→legislation and enforcement that can respond to changing
environments and new technologies
→→enforcement action that seeks prevention and has broad coverage
(eg. border control), while also targeting substances, environments
and organisations (such as gangs) that cause the most harm
→→effective detection of substances and enforcement of the law
relating to the importation, manufacture and distribution of drugs
for illegal use
→→effective regulation and monitoring of the supply chain for
prescription drugs.
National Drug Policy 2015 to 2020 17Our priorities for
Government action
Five areas have been identified to focus on if we are to make meaningful
progress towards achieving our objectives. These have been labelled:
→ Priority area 1: creating a people-centred intervention system
→ Priority area 2: shifting thinking and behaviour
→ Priority area 3: getting the legal balance right
→ Priority area 4: disrupting organised crime
→ Priority area 5: improving information flow.
This Policy makes a commitment The AOD landscape continues to Priority area 1:
to an initial set of actions, and evolve, and new evidence will
these will be reviewed and continue to emerge about the creating a people-
updated by the end of 2017. The issues that need to be addressed centred intervention
actions are drawn from across the and the effectiveness of the system
three strategies and will build on, interventions aimed at addressing
rather than replace, the significant them. The IACD will review the This priority area involves creating
contributions that government, progress made and emerging an AOD intervention system that
communities and individuals evidence, and will provide advice responds to people at their place
already make to the goal and on a revised set of actions in 2017. of need, as early, efficiently and
objectives of this Policy. This will ensure initiatives are effectively as possible. For people
added, cancelled and amended as living with AOD addiction or
appropriate, to reflect changes in dependence this may mean
AOD issues and evidence on the accessible, high-quality addiction
effectiveness of interventions. treatment services, access to
housing or counselling services.
But we also don’t want to wait for
people to be in crisis, or for young
people to adopt habits that will
become problematic in later life.
18 National Drug Policy 2015 to 2020The Prime Minister’s Youth Mental habits and providing advice. For organisations to prevent and
Health Project introduced national children of parents with addiction reduce AOD-related harm
waiting time targets for 12–19 year issues, it could be that a specific
→→identify and connect referral
olds to be seen within three weeks plan is required to ensure their
pathways so that ‘any door is
of contacting a youth alcohol and needs are looked after.
the right door’
drug service and with eight weeks
In order to make the most of
of referral from a service. Initial →→know what works, including
opportunities to build resilience
results show that youth are being opportunities to intervene
(eg. through peer support, positive
provided with better access to earlier, and tailoring activities
role-modelling and confidence-
timely and appropriate treatment to different populations and
building programmes) and
and follow-up (Ministry of Health needs across life stages
intervene (eg. through the
2014). However, we need to →→identify the settings that
provision of information and by
continue to monitor this to avoid are needed to better support
connecting people to AOD
access slipping. individuals, community
treatment) we will need to:
All many people may need is reliable, organisations and services
→→be clear about the roles,
internet-based information, or their to carry out their roles and
responsibilities and
family doctor or school nurse asking responsibilities for the
opportunities for individuals,
about their drinking and drug-taking greatest impact.
families and community
By 2017/18 the Government will:
Action Date Strategies
Develop a system map of potential resilience and intervention points 2016/17
across a person’s life stages
Develop and implement a strategic framework for adult and youth 2017/18
AOD services
Regularly disseminate case studies of good and innovative practice Annual
Develop common tools and/or forums to share practice and celebrate 2017/18
success to foster system learning and improvement
Develop initiatives and an implementation plan to improve outcomes 2017/18
for the children of parents with mental illness and addiction
These actions will integrate closely government services and provide
with the Government’s Rising to wrap-around responses through
the Challenge plan for mental the Government’s Better Public
health and addiction services, and Services Result Areas.
the new ways of working to target
National Drug Policy 2015 to 2020 19Priority area 2: If we are going to achieve real
change, then, just like smoking,
Making progress in this area will
require sustained effort over a
shifting thinking AOD misuse needs to become less considerable period. Change will be
and behaviour desirable and help-seeking gradual, but efforts in this area will
encouraged with the right support be vital in the long term.
This priority area involves available at the right time. Social Communities play an integral role
encouraging a positive shift in sector agencies also need to work in mobilising and sustaining
thinking and behaviour in New together to identify people who change, so we will also develop a
Zealand in relation to: need additional support and tailor set of actions that builds the
→→the culture of drinking and responses and services to their capacity and capability of
intoxication, including during needs. This includes young people communities, particularly those
pregnancy whose schooling is impacted by most affected by AOD use and
AOD use, people not in education related harm.
→→help seeking
or employment, and people
→→the way in which the system affected by a fetal alcohol
intervenes to help. spectrum disorder.
By 2017/18 the Government will:
Action Date Strategies
Build on existing AOD-related public education campaigns to shift Ongoing
AOD culture, promote help-seeking and address stigma
Publish a Fetal Alcohol Spectrum Disorders Action Plan 2015/16
Provide guidance to support schools dealing with AOD issues and 2015/16
helping students who need it, with a focus on keeping students engaged,
where possible
Develop guidance for improving AOD intervention for services engaging 2016/17
with young people not in education or employment
20 National Drug Policy 2015 to 2020Priority area 3: For example: The enforcement of the Misuse of
Drugs Act 1975 also provides scope
getting the legal →→recent changes to the
to offer low-level offenders
regulation of alcohol and
balance right psychoactive substances have
alternatives to the criminal justice
system. For example, a study into
This priority area involves set national requirements, while
cannabis use offences in New
ensuring we monitor and evaluate giving communities a greater
Zealand between 1991 and 2008
how well legislation – and its say about where and when
found a substantial decline in
implementation – is working for these products will be sold
arrests, prosecutions and
individuals, communities and →→the pilot for the Alcohol and convictions for cannabis use over
society so that we can provide the Other Drug Treatment Court that period. This was despite any
right support and make changes offers offenders the opportunity changes to the statutory penalties
where they are needed. to enter an intensive treatment for cannabis use since the
Legislation and law enforcement programme for their AOD enactment of the Misuse of Drugs
acts to prevent and deter people dependency with frequent, Act in 1975 (Wilkins et al 2012).
from accessing and using AOD random drug testing, and, if their
harmfully. Laws set the boundaries participation is successful, for
of what can be legally sold and this to be taken into account
under what circumstances and when they are sentenced.
whether penalties enable health-
oriented responses where an
offence has been committed.
By 2017/18 the Government will:
Action Date Strategies
Work with the Expert Advisory Committee on Drugs (EACD) to ensure 2015/16
harm minimisation is a central feature of drug classification assessments
Review the regulation of controlled drugs for legitimate purposes 2017/18
(such as medicines) alongside reviews of the Medicines Act 1981 and
other therapeutics legislation
Develop options for further minimising harm in relation to the offence and 2017/18
penalty regime for personal possession within the Misuse of Drugs Act 1975
Release a discussion document seeking feedback on appropriate regulation 2015/16
of drug utensils
Introduce the Substance Addiction (Compulsory Assessment and 2015/16
Treatment) Bill to Parliament
National Drug Policy 2015 to 2020 21By 2017/18 the Government will:
Action Date Strategies
Develop a New Zealand position for the United Nations General Assembly 2015/16
Special Session on Drugs 2016
Review the effectiveness of new police powers to deal with breaches 2015/16
of local alcohol bans introduced through the Local Government (Alcohol
Reform) Amendment Act 2012
Evaluate the Alcohol and other Drug Treatment Court Pilot 2017/18
Commence a review of the policy and operation of the Psychoactive 2017/18
Substances Act 2013
Priority area 4: As well as contributing to broader To successfully disrupt organised
societal harms, certain families and crime enforcement efforts must
disrupting communities are disproportionately be supported by initiatives aimed
organised crime affected by these activities (for at reducing social harm. These
example, children living in initiatives need to address the
This priority area involves taking
clandestine laboratories). social, economic and cultural
a multi-agency approach to disrupt
factors that facilitate the
the ability of sophisticated Disrupting activity as far up the
recruitment of individuals by
domestic and trans-national supply chain as possible is a
organised crime groups. We need
organised crime groups to continuing focus for New Zealand
to place emphasis both on building
operate illicit drug networks in enforcement agencies. For example,
resilience in communities with a
New Zealand. It recognises that ‘Taskforce GHOST’ – an operation
large organised crime presence
these groups drive the importation, in December 2013 conducted by
and supporting individuals and
manufacture and regular supply of New Zealand Police, the Organised
families to turn away from the
chemicals and illicit drugs that both and Financial Crime Agency of
organised crime environment.
sustain and expand the domestic New Zealand and the New Zealand
illicit drug market. Given the illegal Customs Service – prevented
nature of these activities, these 578kg of pseudoephedrine and
groups are also often associated 16kg of ephedrine entering the
with a range of other offending, country and being used in the
including violence, crimes against domestic methamphetamine
property and money laundering. manufacturing process.
22 National Drug Policy 2015 to 2020We need to maintain our focus on: supported by improved multi- →→reducing the availability of
agency information-sharing, chemicals and other specialist
→→making it easier for
analysis and intelligence equipment used by domestic
communities to report illegal
drug manufacturers
activities such as the presence →→reinforcing law enforcement
of tinny houses and clandestine efforts to break supply chains →→targeting the proceeds from
labs and taking prompt action and sophisticated distribution illicit drug networks to remove
to remove these networks the profit motive and prevent
the financing of further crime.
→→reducing social harm through a →→strengthening border protection
range of prevention and law efforts to target drug trafficking
enforcement actions that are networks
By 2017/18 the Government will:
Action Date Strategies
Conduct the National Cannabis and Crime Operation to disrupt the activities Annual
of organised crime groups involved in the cultivation of cannabis
Implement the Whole of Government Action Plan on Tackling Gangs 2017/18
Work with authorities in drug source and transit countries to break Ongoing
precursor chemical and drug supply chains into New Zealand
Continue multi-agency investigations and targeting operations focussed Ongoing
on identified vulnerabilities of key organised crime groups and the drug
supply chain
Implement the Organised Crime and Anti-corruption Legislation Bill 2017/18
provisions (once enacted) which include initiatives that will assist
disruption of illicit drug supply, using:
→→a more effective money laundering offence
→→improved detection of drug supply networks through reporting
of international and large cash transactions to Police
National Drug Policy 2015 to 2020 23Priority area 5: →→collaborate to provide wrap-
around services
target policy, interventions,
services and resources where they
improving will have the greatest impact.
→→assess the effectiveness of
information flow policy and service responses,
Making information accessible is
also crucial in order for
The aim of this priority area is to and make improvements
communities to decide the AOD
improve the use and sharing of →→track overall progress towards issues that are important to them
information we collect so that the objectives and goal of this and that shape their environment,
we, communities and individuals, Policy and its contribution to and for individuals to be able to
can better: the government’s wider social make informed choices about their
→→understand and respond to the objectives. own AOD use.
causes of harmful AOD use Collection, use and sharing of
→→target the right resources and information is vital if we are to
initiatives to people in need at anticipate and respond to AOD
the right time issues early and effectively, and
By 2017/18 the Government will:
Action Date Strategies
develop Tier 1 statistics for alcohol and other drug harm 2015/16
develop a multi-agency Early Warning System for the purposes of 2016/17
monitoring emerging trends and informing both enforcement and harm
reduction strategies
update the New Zealand Drug Harm Index 2016/17
publish a literature review of population-level AOD impacts and unmet needs 2015/16
develop and implement an AOD information plan 2016/17
24 National Drug Policy 2015 to 2020You can also read