March,2018 - Humanitarian ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

March,2018

Acronyms
BNA Bottleneck Analysis
BSFP Blanket Supplementary Feeding Program
CBNP Community Based Nutrition Package
CHW Community Health Worker
CHF Common Humanitarian Fund
CSO The Central Statistics Office
DFID Department for International Development
HRP Humanitarian Response Plan
IPD Inpatient Department
IMAM Integrated Management of Acute Malnutrition
IDP Internally Displaced person
IYCF Infant and young child feeding Practices
MAM Moderate Acute Malnutrition
MoPH Ministry of Public Health
OPD Outpatient Department
PLW Pregnant and Lactating women
PND Public Nutrition Department
PPHD Provincial Public Health Department
RUTF Ready to Use Therapeutic Food
SAM Severe Acute Malnutrition
SEHAT System Enhancement for Health Action in Transition
USAID United States Agency for International Development
Acknowledgement
The lifesaving nutrition assistance provided to over 593,827 children under five and women was
made possible by the generous support of the American people through United States Agency
for International Development (USAID), through the support of DFID, Government of Canada,
and Common Humanitarian Fund (CHF).

3

SITUATION OVERVIEW
Humanitarian Context ation in Nimroz province was found to be less severe with a
GAM rate of less than 10 per cent, which doesn’t warrant sig-
Afghanistan is one of the world’s most complex humanitarian
nificant scale up of emergency nutrition services. However
emergencies characterized by escalating conflict causing over
improvements in access to safe water, optimal hygiene practic-
one million people to be living in new and prolonged displace-
es, better access to secure livelihoods are required to prevent
ment. In the year 2017,438,000 people have been internally
a further deterioration of the nutrition status in the three prov-
displaced. Since 2016 a total of 775,000 refugee and undocu-
inces.
mented Afghans returned from neighboring countries (OCHA
2017 displacement tracking). Such combined high level of The findings of the nutrition assessments which were carried
population movements have had a profound impact in parts of out during 2017 were used as a basis for 2018 humanitarian
the country; overloading health facilities, schools, depressing response plan needs analysis. The 2018 nutrition needs analy-
labour wages and increasing rents. A combined effect of con- sis using the most recent nutrition assessment information
flict ,natural disaster and cross-boarder movement resulted in identified 24 priority provinces (Badakhshan, Badghis,
persistently high humanitarian needs. In 2018, 3.3 million peo- Daykundi, Ghazni, Ghor, Hilmand, Jawzjan, Kandahar, Kapisa,
ple will need lifesaving assistance( OCHA Afghanistan HRP Khost, Kunar, Laghman, Nangarhar, Nimroz, Nuristan, Paktika,
2018) . Paktya, Panjsher, Parwan, Samangan, Takhar, Uruzgan,
Wardak, and Zabul). An estimated 1.6 million acute malnour-
Nutrition Situation
ished children under five Including 546,000 that suffer from
The Afghanistan nutrition situation remains precarious. Seven
severe acute malnutrition and 443,000 pregnant and lactating
SMART nutrition surveys and four rapid SMART nutrition
women (PLW) will be in need of treatment services in 2018.
assessments were conducted in 2017.
There is an increase of about 300,000 acute malnourished
The SMART surveys were conducted in Bamyan, Daikun- children under five as compared to estimated caseload at the
di ,Farah ,Jawzjan ,Nimroz ,Samangan, and Takhar provinces beginning of 2017. It is evident that more scale up of acute
while the rapid assessments were carried out in Laghman (in malnutrition treatment services is required to meet the needs
districts of Baba Sahib ,Khairo khail ,Gambiri) and Helmand of the most at risk children and PLW.
(Lashkargah and Nawa districts) provinces. The findings of
Capacity to respond
the assessments in Bamyan ,Daikundi ,Jawzjan ,Helmand
(Lashkar gah and Nawa districts ) , Laghman ( Baba Sahib Currently, out of 1,922 health facilities across the country
districts) and Takhar provinces showed an emergency level 1,028 (53 percent) provide outpatient services for the treat-
acute malnutrition among children under five. Subsequently ment of severe acute malnutrition (SAM ).In addition, 145 in-
provincial nutrition response plans were developed and priority patient facilities and 668 (34 percent of heath facilities) Outpa-
life-saving nutrition services were scaled up across the prov- tient facilities provide services to complicated SAM and mod-
inces wherever gap analysis showed significant unmet needs. erate acute malnourished (MAM) children respectively. In order
The nutrition assessments conducted in Saman- to provide services in hard to reach areas about 12 integrated
gan,Farah ,provinces and districts of Leghman ( Khairo mobile nutrition teams were established in 2017. Additional 25
Khail, Gambiri districts) province showed a global acute mal- integrated mobile nutrition teams are planned to be estab-
nutrition (GAM) rate that can be categorized as ‘Serious’ mal- lished in 2018.Overall it is evident that there is still significant
nutrition situation. According to WHO, a GAM rate between 10- gap between the needs of the affected population and the
14.9 per cent is categorized as ‘Serious’. Nutrition cluster part- access to life saving nutrition services. The influx of IDPs and
ners took into account the finding of these surveys in making returnees especially in urban and peri-urban areas further
planning decision for scaling up, strengthening preventive and overstretches the nutrition partners’ capacity to provide ser-
referral services in the respective provinces. The nutrition situ- vices.
4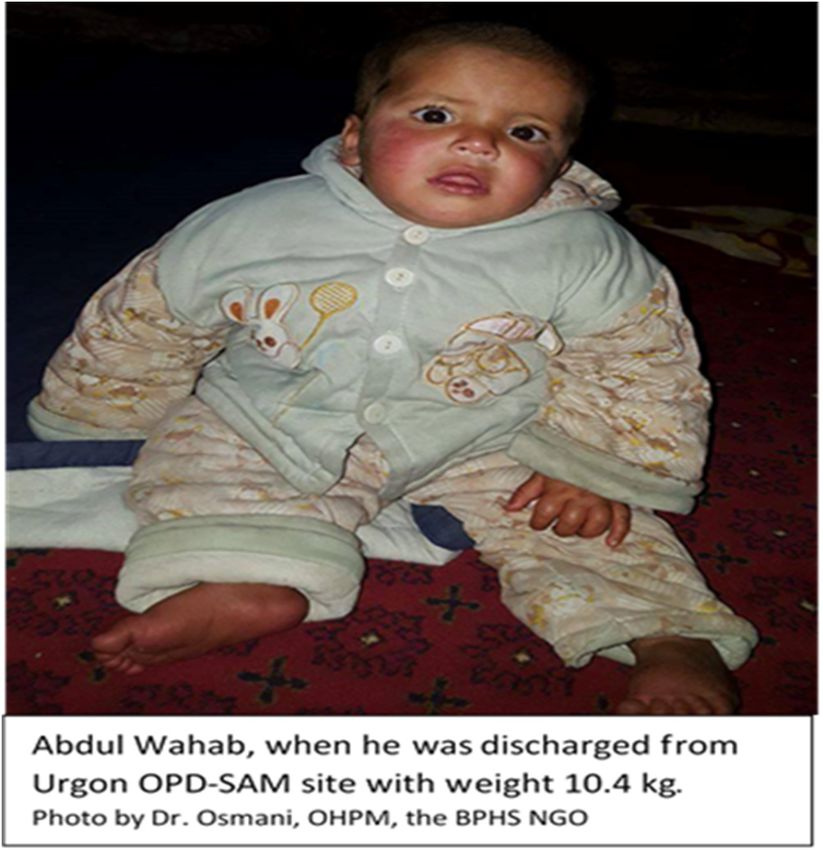
NUTRITION CLUSTER HRP 2017 ACHIEVEMENTS
supplements
⇒ Nutrition cluster partners received less than 50% of the funding required and 10,720 returnee
for lifesaving children in
nutrition services between 24-59
2017. Funding
shortfall was a major challenge which resulted in provision of months received
incomplete deworming
package tables
of nutrition (50 per cent of target).
services.
Overall the nutrition cluster reached a total of 593,827 people
through lifesaving nutrition services. This achievement repre-
In 2017 Afghanistan nutrition cluster partners targeted to reach sents 89.7 percent of the nutrition cluster HRP 2017 target. By
662,176 children under the age of five as well as pregnant and December 2017, nutrition cluster partners received funding
lactating women (PLW) through life saving and preventive amounting US$22.6 Million for life saving nutrition services out
services in top priority districts across the country. The Ministry of US$48 Million required for 2017 response. As a result of
of Public Health (MoPH) and over 40 partners including UN funding shortfall, the nutrition cluster couldn’t reach its target of
agencies, national and international NGOs have been engaged providing full package of nutrition services. The moderate acute
in the provision of curative and preventive emergency nutrition malnutrition (MAM) treatment program in particular was able to
services. The nutrition interventions included treatment of se- reach 74% of the annual target.
vere and moderate acute malnutrition, blanket supplementary
feeding program( BSFP), micronutrient supplementation and Major Challenges
deworming to children under five and PLW affected by rapid
⇒ During the 1st quarter of 2017 the border with Pakistan was
onset emergencies.
closed. It was a huge challenge for timely supplies delivery
From January to December 2017, 235,000 (115,150 boys and particularly for WFP supported MAM treatment and BSFP
119,850 girls) severe acute malnourished (SAM) children 0-59 services . As a result continued delivery of services of the
months of age were identified and admitted to treatment pro- BSFP and MAM treatment was affected .
gram through OPD-SAM(209,631 ) and IPD-SAM( 25,307) facil-
ities . The number of SAM children treated reached 99.6% of
⇒ Insecurity situation limits frequent program monitoring and
supportive supervision. To address this challenge , MoPH/
the HRP 2017 target for SAM treatment services. Through the
targeted supplementary feeding program (TSFP) 162,816 PND and partners such as UNICEF depended on external-
ly contracted third party monitors.
(79,780
. boys and 83,036 girls) moderate acute malnourished
(MAM) children under the age of five and 157,797 pregnant and
⇒ The cluster faced challenge in getting timely and complete
lactating women (PLW) with moderate acute malnutrition (MAM)
data/reports from partners, despite constant follow-ups and
have received treatment services between January and De-
reminders. In 2018, the nutrition database will be upgraded
cember 2017. The number MAM children treated during 2017
as per the Nutrition Cluster work plan. In addition a regu-
reached 74% of the annual HRP target while the number of
lar partner updates will be incorporated as a standing
PLW reached through targeted supplementary feeding pro-
agenda item in the meetings of cluster and Assessment
gram was 130% of the HRP target. Nutrition cluster partners
and Information Management (AIM) working Group (WG)
have also been responding to rapid onset emergencies such as
whereby all the partners who are not reporting will be fol-
Afghan returnees from neighboring countries. The nutrition
lowed up on regular basis. Wherever necessary orientation
services to vulnerable children and PLW affected by rapid onset
to the focal points on reporting process and system will be
emergency are mainly prevention oriented to avert deterioration
carried out by cluster information management officer.
of nutrition status. During 2017, 13,520 (45 per cent of the tar-
get) returnee children aged 6-59 months received Vitamin A
.
5
PERFORMANCE OF INTEGRATED MANAGEMENT OF ACUTE MALNUTRITION PROGRAM
Up to December 2017, 235,000 children with severe acute malnutrition (SAM) have been admitted to outpatient therapeutic pro-
gram (OTP) across the country. This is 99.6% of the targeted 236,000 SAM cases in 2017. An increase of 12.1% and 41.4 % in the
rates of admission have been recorded in 2017 as compared to SAM admissions during 2016 and 2015 respectively. The number of
children who had access to treatment of severe acute malnutrition services in 2017 is more than double as compared to 2014. The
increase in admission is mainly due to the expansion in treatment facilities as a result of the scale up of IMAM services in low cover-
age provinces. The number of SAM treatment facilities has increased from 962 in 2016 to 1028 by end of December 2017. In Addi-
tion the development and rolling out of mobile health and nutrition teams guidelines helped in scaling up nutrition services in hard-to
-reach areas. The mobile nutrition services scaled up through integrated health and nutrition mobile teams in Faryab and in Kanda-
har are examples of good initiatives that will be replicated in 2018.
.
The performance of SAM treatment services has been main- rate was 0.02 per cent and defaulter rate was 12 per cent. For
tained within SPHERE minimum standards parameters across IPD-SAM admitted children the average cure rate was 86 per
most of nutrition (health) facilities. According to SPHERE cent; with a death rate and defaulter rate being 3 per cent and
standard cure rate greater than 75%,death rate greater than 10 per cent respectively. Nationally the performance parame-
10% and defaulter rate less than 15% of all children discharged ters of SAM treatment met SPHERE minimum standards. The
from the program are considered acceptable level of perfor- better performance on SAM treatment services in Afghanistan
mance. Out of the 1028 nutrition facilities, 60 percent (616) can be attributed mainly to the IMAM trainings provided to
.
met SPHERE minimum standards on cure rate while 97 per- health workers and relative improvement in the IMAM reporting
cent (997) nutrition facilities achieved death rates below the and follow up system. In addition monitoring and supportive
SPHERE minimum standard. In addition 72 percent (740) of supervision on the implementation of standard guidelines has
nutrition facilities met the SPHERE minimum standard for de- contributed to maintaining acceptable level of performance in
faulter rate. In 2017, the average national level cure rates SAM treatment services.
among OPD-SAM admitted children was 84 per cent; the death
6
PERFORMANCE OF INTEGRATED MANAGEMENT OF ACUTE MALNUTRITION PROGRAM
7
BOTTLENECK ANALYSIS (BNA) OF SEVERE ACUTE MALNUTRITION
TREATMENT SERVICES IN AFGHANISTAN
Background and Objectives recent nutrition survey results. For the analysis of human re-
source determinant indicators, the number of clinicians, Commu-
The bottleneck analysis (BNA) approach is an analytical process
nity Health Supervisors (CHS), and Community Health Workers
which thoroughly assesses the six coverage determinants of
(CHW) trained on the new IMAM protocol since its introduction in
health and nutrition services. The determinants are grouped in
January 2014 was used. As a proxy indicator to assess the out-
three categories—Supply ,demand and effective coverage. From
reach activities the BNA analysis team explored the possibility
supply side availability of essential health commodities, availabil-
of using the proportion of children 6 to 59 months screened for
ity of trained human resource and geographic accessibility to
acute malnutrition and referred to facilities. However it was
service delivery points are considered. On demand side initial
dropped later on as the screening activities by CHWs were not
and continuous utilization of services. Effective coverage which is
properly documented.
related to quality of the services is another important determinant
considered for analysis . Findings
The BNA approach undergoes through key steps which includes 2017 BNA reported a significant improvement in most of the indi-
selecting a tracer (the most representative services out of several cators assessed as compared to 2015 . The proportion of trained
activities in IMAM) interventions, defining indicators, reviewing clinicians (Doctors and nurses) working in functional health facili-
the programme performance , identifying bottlenecks & dispari- ties increased from 34.8% in 2015 to 61.9% in 2015. Similarly
ties, conducting analysis of the causes of bottlenecks, identifying the community health supervisors increased from 36.5% to
the solutions & strategies to tackle barriers, preparing detailed 78.5%.
action plan, Implementation of the prioritized solutions and also
Improvement on geographical access to OPD-SAM services was
establishing monitoring as well as feedback mechanisms.
observed. The geographic access to SAM services increased
As part of improving the coverage and quality of severe acute from 38.0% in 2015 to 40.6% in 2017 with the outreach activities
malnutrition (SAM) treatment services in Afghanistan, UNICEF coverage of 50.7% in 2015 to 66.4% in 2017. In terms of service
headquarter team advised and supported the Bottleneck Analy- utilization and quality, the ‘initial utilization’ showed increase
sis (BNA) exercise for the first time in 2015. The main objective from 34.5% to 53.8% while ‘continued utilization’ reached 48.6
of the BNA exercise was to identify and address key obstacles % from 33.1% in 2015. Effective coverage of services almost
affecting the utilisation and expansion of quality SAM treatment doubled (24.7% in 2015 and 47.1% in 2017) from the level in
services. Since 2015 there has been significant scale up of Inte- 2015. Moreover, slight improvement on the status of no stock out
grated management of acute malnutrition (IMAM) services in of commodities (RUTF) was seen. Sixty four percent of facilities
Afghanistan as such it was necessary to identify the current barri- didn’t face stock out of RUTF as compared to 60.5 % in 2015.
ers to scale up of IMAM and address appropriately. Therefore , in
2017 MoPH/PND along with nutrition partners undertook the BNA
exercise through the technical support of UNICEF.
Methods
The BNA for SAM management services was designed to do the
analysis of the supply, demand and effective coverage determi-
nants by covering all the provinces and accessible districts. The
BNA exercise was conducted over a six month period of time
starting from October 2016 to end of March 2017. The BNA used
the existing data from national IMAM (nutrition) database. In addi-
tion, the data needed to calculate the commodities , human re-
source and outreach determinants were gathered using a struc-
tured questionnaire administered to health facility staff. The data
required for the analysis of determinant indicators of demand
and effective coverage was extracted from SAM admission statis-
tics of children 6 to 59 months old and the Nutrition Cluster SAM
caseload estimate which was determined based on the most
8
BOTTLENECK ANALYSIS (BNA) OF SEVERE ACUTE MALNUTRITION
TREATMENT SERVICES IN AFGHANISTAN
is going on in the right direction. The program implementation
and performance has shown significant improvement as com-
pared to the findings of 2015 BNA. There still exists the need for
improvement in various aspects of the IMAM program by tackling
the major bottlenecks. It is necessary to develop a detailed
IMAM scale up operational plan in a manner that addresses equi-
ty by taking into account the findings of the BNA.
• It is evident that more frequent oversight and technical sup-
port is required facility and districts level. The MoPH/PND and
partners should have clear plan for provision of technical support
at provincial level.
• Wide dissemination of the findings of the BNA to partners
and relevant stakeholders is required so that current and future
IMAM programs take into account the important determinants of
The qualitative analysis and consultative validation workshop
IMAM services utilisation and effective coverage in the planning
identified the following barriers to IMAM service utilisation:
and implementation of IMAM services. .
• Gap in stock management • MoPH/PND and nutrition cluster have to push for possible
inclusion of reporting indicators needed for BNA exercise in to the
• RUTF hasn’t yet been included in the national essential
drugs list. There is no predictable and reliable funding for IMAM databases so that the additional effort required to collect
procurement of RUTF. data for the BNA exercise will be avoided in the future.
• Lack of proper mapping of scale up ; and inadequate moni- • The MoPH/PND need to give due attention in addressing
toring of IMAM programme expansion at provincial level,
the gap in the Community-IMAM component and work closely
• No Standard Operation Procedure (SOP) or guideline or with nutrition cluster and partners to explore how the data related
training package for CHWs on the community component of to community IMAM activities can be documented in good quality
IMAM,
at all levels.
• Less attention given for community outreach and mobilisa-
tion component of IMAM • In future the BNA should not be exercised as a stand-alone
approach; rather it should be integrated in to the existing routine
• Shorter time of consultation with beneficiaries because of programme monitoring system, which requires commitment and
high admission rate ,and limited number of dedicated nutri-
tion staff in Health facilities. leadership from MoPH/PND side as well as continued technical
assistance from UNICEF and nutrition partners.
The key prioritized solutions to address the barriers were :
• Trainings on supply chain management .
Lessons Learned
• Advocating for inclusion of RUTF in the MoPH essential
drugs list, and inclusion of cost of RUTF into MOPH Basic The validation workshop which reviewed the findings of the BNA
Package of Health Services (BPHS) budget, . helped in identifying additional important bottlenecks, root causes
• Developing a comprehensive IMAM scale up plan in consul- and recommended solutions. Without the consultative session the
tation with all relevant stakeholders and improve monitoring findings of the BNA merely based on secondary data review and
and follow up mechanism . health workers interviews could have been incomplete. In future
• Advocacy for prioritization of CHWs training on nutrition ac- such consultative sessions should remain as part of the BNA
cording to new developed package of Community Based exercise.
Nutrition Package (CBNP)
The ability to utilize current available data sources saved time
• Hiring one nutrition nurse or nutrition counsellor in each and financial resources that could have been spent for gathering
health facilities , and simplification (harmonisation ) of nutri- the necessary data. However, it is important that routine monitor-
tion reporting tools. ing and reporting systems are also strengthened to include as
much data as possible that can be further utilized for bottleneck
Conclusion and Recommendations analysis, and avoid resource intensive coverage surveys.
• Overall, the IMAM programme implementation in Afghanistan 9SAVING LIVES THROUGH INTEGRATED MANAGEMENT OF ACUTE MALNUTRITION :
SUCCESS STORY FROM THE FIELD
PAKTIKA, Afghanistan, 8 Feberuary 2017 – It was a hot sum- The UNICEF-supported unit was able to provide the correct
mer morning in August 2016 when eight-month old Abdul treatment during the first 19 days of hospitalization after which
Wahab reached the hospital. At 5.3 kg weight for his 55 cm Abdul Wahab weighed 6.0 kg.
length, he was in critical condition.
He had made past the critical life-threatening phase but still
“My child was getting thinner by the day, he was so sick with needed close monitoring and care.
severe diarrhoea and couldn’t eat or drink anymore,” Abdul
As such, he was referred to the outpatient unit in the same hos-
Wahab’s father, Lal Mohammad, said to doctors. “I even carried
pital where he was fed exclusively with ‘Ready-to-Use Thera-
him to Ghazni province and to Pakistan several times to get
peutic Foods’ – also known as RUTF, a high-energy paste used
treatment, but nothing was effective.”
to treat severe acute malnutrition.
A lifeline emerged when he connected with Mr. Azizurahman, a
“His weight continued to increase slowly and the doctors, nurs-
Community Health Worker (CHW) who had started providing
es, and midwives checked in regularly,” said Lal Mohammad.
services in his neighbourhood.
Simultaneously, his mother received counselling on ‘Infant and
“He checked my child and measured his upper arm with a spe-
Young Child Feeding’, which would help the family sustain the
cial band and it showed he was in the red area,” Lal Moham-
progress made in the hospital after they returned home.
mad recalled. “He told me that my child was severely malnour-
ished and needed to be hospitalized immediately.” When Dr. Osmani, Nutrition Officer for the Organization for
Health Promotion & Management – UNICEF’s implementing
partner for the Basic Package of Health Services in Afghanistan
– visited Abdul Wahab two months later, his weight had in-
creased dramatically to 8.7 kg. By November, he was dis-
charged at a healthy 10.4 kg.
Severe acute malnutrition (SAM) is a life threatening condition.
According to WHO severe Acute malnutrition if left untreated
may result in death in about 50% of children affected by severe
acute malnutrition. In Afghanistan about 85 percent of SAM
affected children admitted to treatment programs implemented
by UNICEF, Ministry of Public Health (MoPH) and partners
recover from the situation.
Baby Abdul Wahab was taken to the Urgon District Hospital’s In
-Patient Department for the treatment of Severe Acute Malnutri-
tion.
102018 NUTRITION CLUSTER PRIORITIES AND RESPONSE STRATEGY
The nutrition cluster aims ered through development partners.
to contribute to the re-
duction of the risk of ex- Response targets
cessive mortality and
The nutrition cluster will target 674,755 of the most vulnerable
morbidity by improving
children under the age of five and pregnant as well as lactating
the nutritional status of
women among returnees, IDPs and resident populations. This
vulnerable groups. The
includes 209,000 children with SAM, 239,675 children with MAM
2018 nutrition cluster
and 137,040 women with acute malnutrition. In addition, 43,151
response plan is orga-
children aged 6-59 months among populations affected by new
nized under three cluster
crises will receive Vitamin-A supplementation and will be
objectives :
screened for acute malnutrition. Through the blanket supplemen-
tary feeding program (BSFP), nutritional supplementation will be
Objective 1. Improving equitable access to quality lifesaving cu-
provided to 53,359 children aged 6-69 months and PLW. A total of
rative nutrition services through systematic identification, referral
49,248 mothers of children 0-23 months affected by rapid onset
and treatment of acutely malnourished cases
crisis are targeted for infant and young child feeding counselling
services.
Objective 2. Deliver timely lifesaving nutrition services for vulner-
able population groups affected by new crisis focusing on appro- Coordination and linkage with development
priate infant and young child feeding practices in emergency, mi- The nutrition response coordinated by the Nutrition Cluster com-
cronutrient interventions, nutritional supplementation and optimal plements the long term preventive efforts of government and de-
maternal nutrition; velopment partners. The currently ongoing preventive programs
such as Initiative for Hygiene Sanitation and Nutrition (IHSAN),
Objective 3. Strengthen system, capacity, partnership and coordi- community based nutrition program as well as the micronutrient
nation for robust evidence based decision making for timely emer- supplementation and deworming program through the bi-annual
gency nutrition response national immunization days (NID) will help prevent the risk of
acute malnutrition among vulnerable women and children under
Prioritization and target population five. Nutrition cluster partners will strengthen referral linkages
between the preventive and life-saving services. Mothers of chil-
Children under five and pregnant and lactating women (PLW) dren identified as at risk of acute malnutrition during facility based
suffering from acute malnutrition among resident population are mid-upper arm circumference (MUAC) screening and children
primary targets of the nutrition response. In addition, vulnerable who recover from treatment of acute malnutrition program will also
children and PLW at heightened risk of malnutrition and mortality be referred to community based nutrition counselling services. In
among returnees, refugees, IDPs and host populations are also addition, the Nutrition Cluster is committed to working with other
prioritized for nutrition response. The nutrition cluster targets are nutrition sensitive clusters (Health, WASH, Food security and oth-
set with an aim of achieving at least 50 percent coverage in emer- ers) to support multi-sectorial assessments and integrated pro-
gency nutrition (NiE) services. This is in line with the Sphere gramming.
standards minimum coverage for NiE services in predominantly
rural populations. Fifty percent of children with severe acute mal-
nutrition (SAM) and moderate acute malnutrition (MAM), children
under five and PLW are targeted in 2018. An estimated 10 per-
cent of SAM children are targeted for inpatient care. In addition,
50 percent of children and PLW affected by rapid onset crisis are
targeted for emergency nutrition response. For treatment of acute
malnutrition services, 24 provinces (Badakhshan, Badghis,
Daykundi, Ghazni, Ghor, Hilmand, Jawzjan, Kandahar, Kapisa,
Khost, Kunar, Laghman, Nangarhar, Nimroz, Nuristan, Paktika,
Paktya, Panjsher, Parwan, Samangan, Takhar, Uruzgan, Wardak,
and Zabul) with serious levels of acute malnutrition and with ag-
gravating factors such as recent displacement and increased inci-
Taking Ghulam’s height measurement in SAM service delivery site in Mazar city of Balkh province
dence of conflict are targeted. The remaining 10 provinces,
though not part of the HRP, will still have nutrition activities cov-
11Nutrition cluster HRP 2018 targets and financial Requirement
Cluster Objective 1: Improving equitable access to quality lifesaving curative nutrition services through systematic identification, referral and treatment of acutely malnour-
ished cases
12
Result Indicators G. Target H. Baseline Funding
Number and proportion of severe acutely malnourished boys and girls 0-59 months
20,900 23,834
with medical complications admitted for treatment in inpatient facilities
Number and proportion of severe acute malnourished boys and girls 0-59 months
209,000 201,470
admitted for treatment
Number and proportion of moderate acute malnourished boys and girls 6-59 months
239,675 199,018
admitted for treatment
Number and proportion of acutely malnourished pregnant and lactating women admit-
137,040 216,272
ted for treatment
Number of districts with hard to reach communities provided integrated nutrition ser-
25 8
vices through mobile teams
Proportion of boys and girls aged 0-59 months discharged cured from management
75 % 86 %
of severe acute malnutrition programs
I. Total Activity
Cost
Activity 1: Admit and treat severe acutely malnourished boys and and girls 0-59 months with medical $ $
20900
complication in targeted provinces 100.00 2,090,000.00
Activity 2: Admit and treat severe acutely malnourished boys and and girls 0-59 months in targeted
209,000 $100 $20,900,000
provinces
Activity 3: Admit and treat moderate acutely malnourished boys and and girls 6 -59 months in targeted
239,675 $37 $8,867,975
provinces
Activity 4: Admit and treat acutely malnourished pregnant and lactating women in targeted provinces 137,040 $105 $14,389,200
Activity 5: Establish emergency mobile teams in priority provinces*** 25 $84,000 $2,100,000
SUB TOTAL $48,347,175.00Nutrition cluster HRP 2018 targets and financial Requirement
Cluster Objective 2: Deliver timely lifesaving nutrition services for vulnerable population groups affected by new crisis focusing on appropriate infant
and young child feeding practices in emergency, micronutrient interventions, nutritional supplementation and optimal maternal nutrition.
13
Result Indicators G. Target H. Baseline
umber and propor!on of children 6-59 months among new crisis affected popula!ons 43,151 17,148
who received vitamin A supplementa!on
Number and propor!on of returnee children 6-59 among new crisis affected popula!ons 43,151 13,723
screened for acute malnutri!on
Number and propor!on of boys and girls aged 6-59 months and pregnant and lacta!ng 53,359 NA
at risk of acute malnutri!on among new crisis affected popula!ons who received BSFP
Number and propor!on of mothers with children 0-23 months among new crisis affect- 49,248 NA
ed popula!on who received counseling on IYCF in Emergency op!mal prac!ces
I. Total Ac!vity
D. Target E. Unit Cost
Cost
Ac!vity 1: Vitamin A supplementa!on 43,151 $2 $86,302.00
Ac!vity 2: Screening
43,151 $1 $43,151.00
Ac!vity 3: BSFP women and children 53,359 $77 $4,108,643.00
Ac!vity 4: IYCF 49,248 $10 $492,480.00
SUB TOTAL
$4,730,576Nutrition cluster HRP 2018 targets and financial Requirement
Cluster Objective 3: Strengthen system, capacity, partnership and coordination for robust evidence based decision making for timely emergency nutri-
tion response
Result Indicators G. Target H. Baseline
14
Number of MOPH and Partner technical staff trained on Nutrition in Emergencies harmo-
150
nized training package (HTP)
Number of nutrition cluster coordination meetings conducted at national and sub national 72 72
level
28 8
Number of provinces where localized integrated nutrition SMART surveys conducted
4 4
Number of provinces where coverage assessments conducted
5 5
Number of locations where Rapid Nutrition Assessments for new emergencies conducted
Number and proportion of provinces with operational sentinel sites (facility-based and com- 34 34
munity based)
90% 75%
Partner's Nutrition Emergency response reporting rate maintained at acceptable level
I. Total
D. Target E. Unit Cost
Activity Cost
Number of MOPH and Partner technical staff trained on Nutrition in Emergencies harmonized training
150 $1,000 $150,000.00
package (HTP)
Number of nutrition cluster coordination meetings conducted at national and sub national level* 72 $10,972 $789,984.00
Number of provinces where localized integrated nutrition SMART surveys conducted 28 $17,000 $476,000.00
Number of provinces where coverage assessments conducted 4 $15,000 $60,000.00
Number of locations where Rapid Nutrition Assessments for new emergencies conducted 5 $5,000 $25,000.00
Number and proportion of provinces with operational sentinel sites (facility-based and community based) 34 $15,000 $510,000.00
Partner's Nutrition Emergency response reporting rate maintained at acceptable level** 90% $0
SUB TOTAL $2,010,984.00
TOTAL NUTRITION : 55,088,735.00AFGHANISTAN NUTRITION CLUSTER PARTNERS, JANUARY 2018
1516
KEY NUTRITION CLUSTER CONTACTS
Title Location Organization Name Phone number Email
Responsibilities
Director of Public Nutri- PND ,Kabul MoPH Homayoun Ludin +93 700604649 Nutri-
tion Department (Cluster tion.moph@gmail.com
Lead)
Cluster Coordinator UNICEF ,Kabul UNICEF Anteneh +93 730717621 adobamo@unicef.org
(Cluster Lead)
Gebremichael
Dobamo
Information Manager UNICEF, Kabul UNICEF Said M Yaqoob Azi- +93 730717622 sazimi@unicef.org
mi
Nutrition Officer UNICEF, Kabul UNCIEF Nafisa Qani +93(0)730717 nqani@unicef.org
263
(Central zone)
Nutrition Officer UNCIEF, UNCIEF Shafiqullah +93 730717490 sbashari@unicef.org
Jalalabad Bashari
Nutrition Officer UNCIEF, UNCIEF Atiqulla Amiri +93 730717379 aamiri@unicef.org
Mazar Sharif
Nutrition Officer UNCIEF, Herat UNCIEF Qadria Afzal +93 730717698 qafzal@unicef.org
Nutrition Officer UNCIEF, UNCIEF Muzlifa Khan +93 730717572 mkhan@unicef.org
Kandahar
IMAM officer PND ,Kabul MoPH Shafiqullah Safi +93 785 277 588 shafiqkmu.safi@gmail.co
m
Nutrition Coordination PND ,Kabul MoPH Wafiullah Hanani +93 798795370 coordina-
and capacity building tion.pnd@gmail.com
officer
Nutrition Surveillance PND ,Kabul MoPH Noor Rahman Noor +93 777 666 525 drnoor330@gmail.com
Coordinator
Nutrition in Emergencies PND ,Kabul MoPH Hamed zia Dashti +93 785598999 shz_dashti@yahoo.com
Officer
About the Afghanistan Nutrition Cluster Bulletin
The Afghanistan Nutrition Cluster bulletin is produced by the Afghanistan Nutrition Cluster coordination
team and the Public Nutrition Directorate of the Ministry of Public Health in collaboration with partners
including: AADA,ACF, ACTD, AKF,AHDS, AYSO,BARAN, BDN ,CAF,CHA,FEWSET,
HEWAD,IMC,MOVE, HN-TPO, IMC,JI, MEDAIR , MOVE, MMRC-A,OCCD,ORCD,OHPM, PU-
AMI,SAF,SCA, SHRO,RHDO, UNICEF,WFP, WHO, WVI
Nutrition Cluster coordination information can be accessed online at :
https://www.humanitarianresponse.info/en/operations/Afghanistan/nutrition
Disclaimer : The content of this publication doesn’t necessarily reflect the position of Cluster lead
agency (UNICEF) and PND/MoPH
1718
You can also read