Oil's Well That Ends Well Understanding the Differences in Lipid Emulsions - Kathleen M Gura PharmD, BCNSP, FASHP, FPPAG, FASPEN Center for ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Oil’s Well That Ends Well
Understanding the Differences in Lipid Emulsions
Kathleen M Gura PharmD, BCNSP, FASHP, FPPAG, FASPEN
Center for Intestinal Rehabilitation (CAIR)
Kathleen.Gura@childrens.harvard.edu
1
Disclosures
• B.Braun – advisory board, consultant
• Fresenius Kabi – consultant, research support
• Pronova/BASF – advisory board, research support
• Sancilio & Company -advisory board, research support
A licensing agreement exists between Boston Children’s Hospital &
Fresenius Kabi for the use of Omegaven in IFALD.
I will be discussing unapproved and off labeled use of
medications.
Learning Objectives
• Discuss challenges of bringing new intravenous lipid
emulsions (IVLE) to the U.S. market
• Understand the what data was used to approve IVLE in
the U.S.
• Describe the differences in the currently used products in
the U.S.
3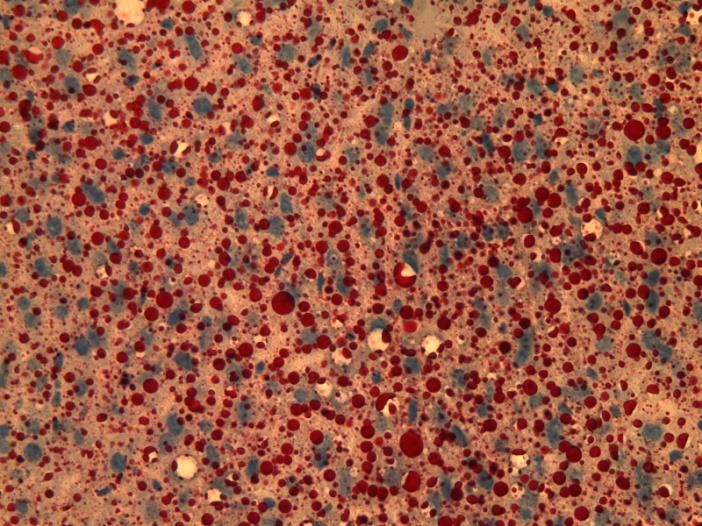
IV Lipid Emulsions are Not New
• William Courten 17th century
– Intravenous olive oil 1g/kg given to a dog
– Fatal outcome
• Severe respiratory distress
• ? Embolism
• Edward Hodder -1873 (Canada)
• Milk infusion in 3 patients with cholera
– 2/3 survived “effect magical”
• Could not be reproduced by others
– unmodified fats could not be given IV
4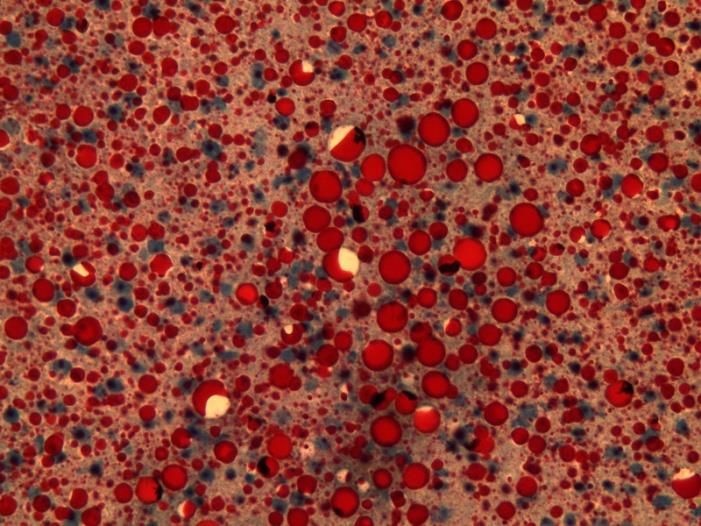
20th Century Lipid Research
1920-1960
Yamakawa
Nomura
Stare
Geyer
Meng
Canham
5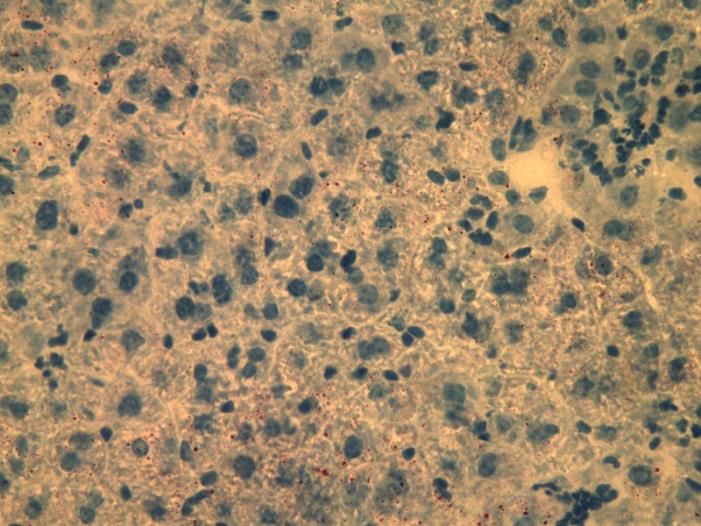
Lipid Emulsions
• Formed as artificial chylomicrons
– Spherical form (200-500nm in diameter)
• Need an emulsifier to allow the
dispersion of the oil into the water and
ensure a stable emulsion
– Emulsifiers similar to phospholipids in
natural chylomicrons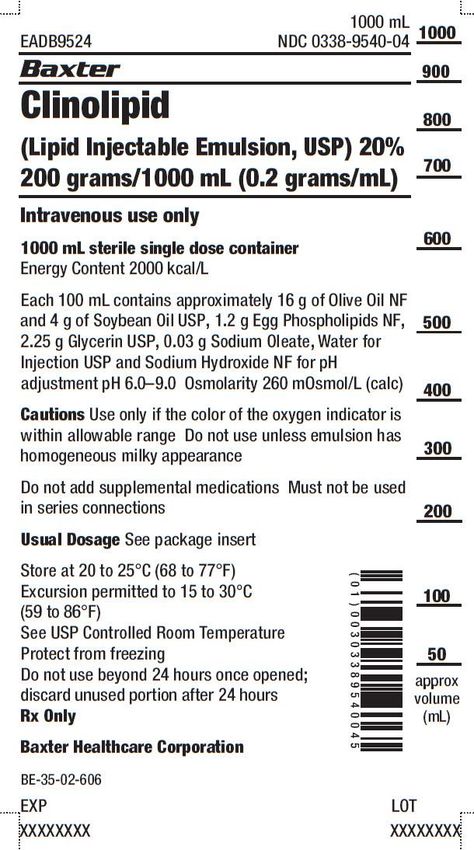
Lipomul
Upjohn Co (Kalamazoo, MI)
• 15% cotton seed oil /4% soy phospholipids/0.3% ploxamer
• Numerous serious adverse effects
– chills, fever, nausea, vomiting
– dyspnea, hypoxia, and hypotension
• Product removed from the market after several years
• Negative US experience dampened the interest in fat
emulsions worldwide
• Only dextrose available as a parenteral energy source
7
Arvid Wretlind
“Father of Complete Nutrition” - 1961
8
What’s Common to ALL IVLE Products • Water for injection • 1.2% egg yolk phospholipids • 2.25%-2.5% glycerin • Sodium hydroxide
What’s Different
• Phytosterol content
• Vitamin E content
• Inflammatory characteristics
due to oil source
Typically not noted on the product label!Phytosterols
• Plant sterols
• Typically only small amounts
absorbed by GI tract
• Undergo hepatic metabolism
• IV phytosterols reduce bile
acid flow
http://www.avfchem.com/images/04.gif
11Comparison of Lipid Emulsions (10 g fat / 100 mL)
OIL Intralipid Omegaven SMOFlipid
Soybean 100% 30%
MCT 30%
Olive 25%
Fish 100% 15%
Glycerol 2.25 2.5 2.5
Egg Phospholipid 1.2 1.2 1.2
Phytosterols (mg/L) 439+ 5.7 3.66 207
12Vitamin E (alpha–tocopherol)
• Anti-oxidant
• Prevents hepatic injury (animal models)
• Prolonged use of soybean oil IFE may reduce α-
tocopherol concentrations in plasma lipoproteins
– Soybean oil contains γ-tocopherol
• Less bioactive than α-tocopherol
13Comparison of Lipid Emulsions
OIL Intralipid Omegaven SMOFlipid
Soybean 100% 30%
MCT 30%
Olive 25%
Fish 100% 15%
Vitamin E mg/L 38mg 150-296mg 163-225mg
14OIL SOURCES
Soybean (SO) • Oil source in first successful IFE (1961) • 50% linoleic acid (ω -6 fatty acid) – Must be converted to arachidonic acid • 25% oleic acid (ω-9 fatty acid) • 10% alpha-linolenic acid (ω-3 fatty acid) – Must be converted to EPA and DHA • Very low Vitamin E content • Rich in phytosterols
Intravenous Fat Dosage
Pure Soybean Oil
• neonates
initial: 0.5 gm/kg/day
max: 3 gm/kg/day *
• Infants
initial: 1 gm/kg/day
max: 2-3 gm/kg/day*
• 8-10% total calories should be provided as fat to prevent
EFAD (0.5-1g/kg/day)
• Consider lipid restriction (i.e.., 1g/kg/day in patients at risk
for IFALDMedium Chain Triglycerides (MCT) • Derived from coconut oil • Mainly caprylic and capric acids • Readily oxidizable • Devoid of pro-inflammatory properties • May be protein sparing • Does not impair hepatic function or immune function • Resistant to peroxidation CONTAIN NO ESSENTIAL FATTY ACIDS
Olive Oil • Introduced in Europe 1990’s • 5% of fatty acid profile linoleic acid (ω-6) • “neutral” pro inflammatory properties • Lower phytosterol content • Higher α-tocopherol content • Oleic acid is fairly resistant to peroxidation • May leach more DEHP in comparison to soybean oil
Fish Oil
• Rich in ω-3 fatty acids
– Primarily DHA, EPA
• Contains some arachidonic acid
• Little to no phytosterols
• Rich in Vitamin E
• Considered to have nutritional as well as therapeutic benefits
• Potential MOA in IFALD: GPR120 agonist
– mediates anti-inflammatory effects
(J Hepatology 2014:60:625–632)Function of Each Oil Type • Soybean oil: provides essential fatty acids • MCT: source of rapidly available energy, spares larger amounts of essential fatty acids for incorporation into cell membranes • Olive oil: indirect anti-inflammatory effect by replacing omega-6 fatty acids with oleic acid and is less prone to peroxidation than PUFAs • Fish-oil: influence inflammatory reaction -inhibit inflammatory gene induction, cytokine release and adhesion molecule, source of DHA
Rationale for Reducing Soybean Oil Intake
• Decreases linoleic acid load
• 2 ways to achieve this
– Dilute with another inert oil
– Partially replace some soybean oil with another type of oil that
has different inflammatory propertiesProposed Benefits of a Mixed Oil ILE • Favorable omega-6/omega-3 fatty acid ratio – ratio 2.5:1 (Intralipid 7:1) – Mixing four different oils optimizes the fatty acid profile • Emulsions enriched with alpha-tocopherol maintain an adequate antioxidant status – avoids lipid peroxidation
Comparison of Lipid Emulsions
OIL Intralipid Omegaven SMOFlipid
Soybean 100% 30%
MCT 30%
Olive 25%
Fish 100% 15%
EFA % by weight
Linoleic 50 4.4 21.4
α-Linolenic 9 1.8 2.5
EPA 0 19.2 3
DHA 0 12.1 2
Arachidonic acid 0 1 -4 0.15-0.6
24
EPA: Eicosapentaenoic Acid; DHA: Docosahexaenoic AcidBRINGING IV LIPID EMULSIONS TO THE
UNITED STATES
25Intralipid
1962 (Sweden)
• Soybean oil based
– Linoleic acid (52%), linolenic acid (8%), and oleic acid (22%).
• Vitrum Company
– Swedish a family-owned enterprise committed to PN
• Numerous generics quickly followed but not in US
– European PN: 50% calories as lipid emulsion and the remainder
as dextrose (i.e., the fat system)
– Dudrick 1968 US PN: high dextrose / NO FAT (i.e. dextrose
system)
26IVLE Development Challenges • IVLEs have been approved based on ability to provide calories and essential fatty acids • To date, IVLE trials have been underpowered to show statistically significant changes in clinical outcomes • Original product goals: – provide concentrated ENERGY – To secure delivery of ESSENTIAL FATTY ACIDS – … and do it SAFELY No product has been approved based on therapeutic efficacy
FDA Medical Officer Review of Fat Emulsions 1993
“The oils contained in these emulsions are ones found in
diet, and the fatty acid distribution is similar to that found in
dietary vegetable oils. It seems that the efficacy is really
that of a nutrient source of calories. Clearance of
triglycerides is probably an acceptable measure of effective
use of the fat for energy in muscle or storage in adipose
tissue.”
Tabor E. Nutr Clin Pract. 2013 Dec;28(6):770-2
28Intralipid in the U.S.
10% Intralipid approved by FDA (1975); 20% (1981) 30% (1993)
After the first application for 20% Intralipid in January 1980:
• FDA requested data collected by the US Army & Riker Laboratories in the 1960’s
US Army data:
• 47 patients
500 ml Intralipid 20%/day - 6 – 21 days (596 infusions)
• Parameters measured:
Hematology, Coagulation, LFTs, TG, Cholesterol, phospholipids
• US Army and Stockholm data:
Liver and spleen biopsies (after Intralipid infusions)
• Data collected from other centers: 664 patients/1850 infusions
FDA Workshop October 29th, 2013Intralipid: Pediatric Data for Approval
• Children < 4 years of age
• No adolescents studied
FDA Workshop October 29th, 2013
30Liposyn
• Developed by Abbott Laboratories
• 3 products
– Liposyn 10% – 100% safflower oil (77% LA /0.1% ALA)
– Liposyn II - 50/50 soybean – safflower oil blend
– Liposyn III 100% soybean oil
FDA Workshop October 29th, 2013
31Liposyn (original)
• 10% approved 1979; 20% 1981
• Approval based on:
– Prevent S&S of EFAD in PN patients
– Source of calories
– T/T ratio used to assess EFA status
– Studies:
• Adult
– 50 patients 14-28 days duration (566 infusions) 15 trials/5 protocols
– Used LA dosing as variable
• Pediatric
– 5 patients, up to 28 days
• Discontinued in 1984 FDA Workshop October 29th, 2013
32Liposyn Liposyn 20% – Administration of Liposyn 20% providing about 1/3 to half of caloric requirements will maintain or improve nutritional status without causing undue side effects – Provide calories in smaller fluid volume – Two week duration – Hematology, chemistry, urinalysis • Adults – 2 protocols; n=116, 1907 infusions • Pediatrics, 1353 infusions – Infants/children n=43 – Premature infants n=17 FDA Workshop October 29th, 2013
Liposyn II and Liposyn III
• Liposyn II
– Clearance studies and prior approvals of Liposyn original
• Liposyn III
– No clinical trials on 10% and 20% concentrations
– 2 uncontrolled studies on Liposyn III 30%
FDA Workshop October 29th, 2013
34Nutrilipid (B. Braun)
• 10% and 20% approved May 1993
– Was discontinued but reintroduced in
2014
• Approved based on noninferiority
studies to Intralipid and Liposyn III
35Pharmacopeial Specifications
• Helps determine embolic risk and assists in determining beyond
use dating
– Larger (> 5 μm ) particles can become trapped in the lungs
– Values that outside USP 729 established ranges suggest an unstable
emulsion
• USP 729
– Mean Droplet Diameter
• 5 μm (PFAT5)
• Must not exceed 0.05%NEW LIPID EMULSIONS IN THE US
37What’s Different with FDA Approval
Process
• Nutrition noninferiority study endpoints still used
– Weight gain
– Weight maintenance
– Serum levels of free fatty acids/triglycerides
• Other studies may be needed if deemed absolutely
necessary
– ? Phytosterol content
– PFAT5 if packaging changes
– Pediatric specific studies
38WHAT’S APPROVED
39Clinolipid
(Baxter)
• Newest IFE product approved in US (2013)
• Lower % PUFAs but still providing an adequate amount of EFAs
– 80% refined olive oil and 20% refined soybean oil
• Lower soybean oil content in order to ↓ LA levels
• Contains the same 5 major fatty acids, including the same EFA
components as the soybean oil
• Approved as a non-inferiority product to Intralipid
FDA workshop October 29, 2013Clinolipid
• No pediatric indication (black box
warning can be fatal in premature
infants)
– Increase risk of essential fatty acid
deficiency (EFAD)
• Only available in 1000mL containers
– Not listed as pharmacy bulk package
– Provides 200 grams fat (typical adult
dose 67 g/day)
• Must be administered with 1.2 micron
inline filter
• Cannot be used with some PN
compounding devices
– Increases particle generationSMOFlipid
(Fresenius Kabi)
• Approved in Europe 2000; US July 13, 2016
• Lipid Source: 30% soybean oil; 30% medium chain
triglyceride (MCT) oil; 25% olive oil; 15% fish oil
• May provide anti-inflammatory, immune protection
and pro-oxidant properties compared to Intralipid
20%
• May be a better energy source for the critically ill
who would benefit from the addition of n-3 fatty
acids
42SMOFlipid ® - Composition
Koletzko B, Goulet O, Hunt J. et al. J Pediatr Gastroenterol Nutr 2005;41(2):1-87
Oliveira OR, Santana MG, Santos FS et al. Lipids Health Dis 2012;11:157
Koletzko B, Rodriguez-Palmero M, Demmelmair H et al. Early Hum Dev 2001;65:3-18
Rayyan M, Devlieger H, Jochum F et al. J Parenter Enteral Nutr 2012;26(1):81-94Current Approval
SMOFlipid approved in adults
- as a source of calories and essential fatty acids
Pediatric indication
- submission of postmarketing pediatric studies deferred to 2019
http://www.accessdata.fda.gov/drugsatfda_docs/appletter/2016/207648Orig1s000ltr.pdfPediatric Dosing
• SMOFlipid NOT suitable for lipid restriction protocols
• Recommended dosing:
– 2-4 g/kg/day (Goulet O, et al. JPEN 2010; 34:485-495)
45WHAT’S BEING USED
INVESTIGATIONALLY/
COMPASSIONATE USE
46Omegaven
(Fresenius Kabi)
• Approved in Europe
• 100% fish oil (10% IVLE)
• Typically used in combination with Intralipid
• Max labeled dose 0.2g/kg/day
• Dose used in PNALD: 1g/kg/day as monotherapy
• Not indicated for use in children
• Not intended to be used as monotherapy
• Not FDA approved
47July 2002
• 16 year old male s/p BMT with a soy allergy requiring PN/lipids
• Developed essential fatty acid deficiency
• Treated with Omegaven® as monotherapy for 50 days until able
to resume enteral feeds
• No adverse events associated with its use despite having
several listed contraindications (hypertriglyceridemia,
hyperglycemia)
Gura KM, Parsons SK, Bechard LJ, Henderson T, Dorsey M, Phipatankul W,
Duggan C, Puder M, Lenders C. Clin Nutr. 2005 Oct;24(5):839-47Omegaven Compassionate Use Protocol • Conventional fat emulsions are discontinued • Omegaven® dosing: advanced to 1 g/kg/day for remainder of time on PN • Additional non protein calories provided as carbohydrate
Comparison of
Oil Red-O4 IVLEs
Chow Intralipid
Clinoleic Omegaven
SMOFlipid
J Pediatr Surg. 2011 Apr;46(4):666-73Conclusions
• New products are currently
only approved for use in
ADULTS
• There is still no perfect IVLE
• Progress is being made
• We still have a long way to go
52THANK YOU!
Thank you!
54References
• Waitzberg DL, Torrinhas RS, Jacintho TM. New parenteral lipid emulsions for clinical use. JPEN J Parenter
Enteral Nutr. 2006;30:351-367.
• Le HD, Meisel JA, de Meijer VE, Gura KM, Puder M. The essentiality of arachidonic acid and
docosahexaenoic acid. Prostaglandins Leukot Essent Fatty Acids. 2009;81:165-170.
• Serhan CN. Controlling the resolution of acute inflammation: a new genus of dual anti-inflammatory and
proresolving mediators. J Periodontol. 2008;79(8)(suppl):1520-1526.
• Driscoll DF. Lipid injectable emulsions: 2006. Nutr Clin Pract. 2006;21: 381-386.
• Pianese P, Salvia G, Campanozzi A, et al. Sterol profiling in red blood cell membranes and plasma of
newborns receiving total parenteral nutrition. J Pediatr Gastroenterol Nutr. 2008;47:645-651.
• Ling WH, Jones PJ. Dietary phytosterols: a review of metabolism, benefits and side effects. Life Sci.
1995;57:195-206.
• Ostlund RE Jr, McGill JB, Zeng CM, et al. Gastrointestinal absorption and plasma kinetics of soy Delta(5)-
phytosterols and phytostanols in humans. Am J Physiol Endocrinol Metab. 2002;282:E911-E916.
• Socha P, Koletzko B, Demmelmair H, et al. Short-term effects of parenteral nutrition of cholestatic infants with
lipid emulsions based on medium chain and long-chain triacylglycerols. Nutrition. 2007;23:121-126.
• Lehner F, Demmelmair H, Röschinger W, et al. Metabolic effects of intravenous LCT or MCT/LCT lipid
emulsions in preterm infants. J Lipid Res. 2006;47:404-411.References
• de Meijer VE, Le HD, Meisel JA, Gura KM, Puder M. Parenteral fish oil as monotherapy prevents essential fatty
acid deficiency in parenteral nutrition–dependent patients. J Pediatr Gastroenterol Nutr. 2010;50:212-218.
• Puder M, Valim C, Meisel JA, et al. Parenteral fish oil improves outcomes in patients with parenteral nutrition–
associated liver injury. Ann Surg. 2009;250:395-402.
• Lee SI, Valim C, Johnston P, et al. Impact of fish oil–based lipid emulsion on serum triglyceride, bilirubin, and
albumin levels in children with parenteral nutrition–associated liver disease. Pediatr Res. 2009;66(6):698-703.
• Diamond IR, Sterescu A, Pencharz PB, Kim JH, Wales PW. Changing the paradigm: omegaven for the treatment
of liver failure in pediatric short bowel syndrome. J Pediatr Gastroenterol Nutr. 2009;48:209-215.
• de Meijer VE, Gura KM, Meisel JA, Le HD, Puder M. Parenteral fish oil monotherapy in the management of
patients with parenteral nutrition– associated liver disease. Arch Surg. 2010;145:547-551.
• Vanek VW, Seidner DL, Allen P, Bistrian B, Collier S, Gura K, Miles JM, Valentine CJ, Kochevar M; Novel Nutrient
Task Force, Intravenous Fat Emulsions Workgroup; American Society for Parenteral and Enteral Nutrition
(A.S.P.E.N.) Board of Directors .A.S.P.E.N. position paper: Clinical role for alternative intravenous fat emulsions.
Nutr Clin Pract. 2012 Apr;27(2):150-92.
• Nehra D, Fallon EM, Carlson SJ, Potemkin AK, Hevelone ND, Mitchell PD, Gura KM, Puder M. Provision of a
Soy-Based Intravenous Lipid Emulsion at 1 g/kg/d Does Not Prevent Cholestasis in Neonates. JPEN J Parenter
Enteral Nutr. 2012 Jul 5.You can also read