OLDER ADULTS: STANDARDSOF MEDICALCAREINDIABETESD2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
S168 Diabetes Care Volume 44, Supplement 1, January 2021
12. Older Adults: Standards of American Diabetes Association
Medical Care in Diabetesd2021
Diabetes Care 2021;44(Suppl. 1):S168–S179 | https://doi.org/10.2337/dc21-s012
The American Diabetes Association (ADA) “Standards of Medical Care in Diabetes”
includes the ADA’s current clinical practice recommendations and is intended to provide
the components of diabetes care, general treatment goals and guidelines, and tools to
evaluate quality of care. Members of the ADA Professional Practice Committee, a
multidisciplinary expert committee (https://doi.org/10.2337/dc21-SPPC), are responsi-
ble for updating the Standards of Care annually, or more frequently as warranted. For a
12. OLDER ADULTS
detailed description of ADA standards, statements, and reports, as well as the evidence-
grading system for ADA’s clinical practice recommendations, please refer to the Standards
of Care Introduction (https://doi.org/10.2337/dc21-SINT). Readers who wish to comment
on the Standards of Care are invited to do so at professional.diabetes.org/SOC.
Recommendations
12.1 Consider the assessment of medical, psychological, functional (self-
management abilities), and social geriatric domains in older adults to provide
a framework to determine targets and therapeutic approaches for diabetes
management. B
12.2 Screen for geriatric syndromes (i.e., polypharmacy, cognitive impairment,
depression, urinary incontinence, falls, and persistent pain) in older adults, as
they may affect diabetes self-management and diminish quality of life. B
Diabetes is a highly prevalent health condition in the aging population. Over one-
quarter of people over the age of 65 years have diabetes and one-half of older
adults have prediabetes (1,2), and the number of older adults living with these
conditions is expected to increase rapidly in the coming decades. Diabetes
management in older adults requires regular assessment of medical, psycho-
logical, functional, and social domains. Older adults with diabetes have higher
rates of premature death, functional disability, accelerated muscle loss, and coexisting
illnesses, such as hypertension, coronary heart disease, and stroke, than those without
diabetes. Screening for diabetes complications in older adults should be individualized
and periodically revisited, as the results of screening tests may impact targets and
therapeutic approaches (3–5). At the same time, older adults with diabetes are also at
greater risk than other older adults for several common geriatric syndromes, such as Suggested citation: American Diabetes Association.
polypharmacy, cognitive impairment, depression, urinary incontinence, injurious 12. Older adults: Standards of Medical Care in
falls, and persistent pain (1). These conditions may impact older adults’ diabetes self- Diabetesd2021. Diabetes Care 2021;44(Suppl.
management abilities and quality of life if left unaddressed (2,6,7). See Section 4 1):S168–S179
“Comprehensive Medical Evaluation and Assessment of Comorbidities” (https://doi © 2020 by the American Diabetes Association.
.org/10.2337/dc21-S004), for the full range of issues to consider when caring for older Readers may use this article as long as the work is
properly cited, the use is educational and not for
adults with diabetes. profit, and the work is not altered. More infor-
The comprehensive assessment described above may provide a framework to mation is available at https://www.diabetesjournals
determine targets and therapeutic approaches (8–10), including whether referral for .org/content/license.care.diabetesjournals.org Older Adults S169
diabetes self-management education is Despite the paucity of therapies to
be ascertained and addressed at
appropriate (when complicating factors prevent or remedy cognitive decline, iden-
routine visits. B
arise or when transitions in care occur) or tifying cognitive impairment early has
12.5 For older adults with type 1 di-
whether the current regimen is too com- important implications for diabetes care.
abetes, continuous glucose mon-
plex for the patient’s self-management The presence of cognitive impairment
itoring should be considered to
ability or the caregivers providing care. can make it challenging for clinicians to
reduce hypoglycemia. A
Particular attention should be paid to help their patients reach individualized
complications that can develop over short glycemic, blood pressure, and lipid tar-
periods of time and/or would significantly gets. Cognitive dysfunction makes it dif- Older adults are at higher risk of hypo-
impair functional status, such as visual and ficult for patients to perform complex glycemia for many reasons, including in-
lower-extremity complications. Please re- self-care tasks (22), such as monitoring sulin deficiency necessitating insulin therapy
fer to the American Diabetes Association glucose and adjusting insulin doses. It and progressive renal insufficiency (30). As
(ADA) consensus report “Diabetes in Older also hinders their ability to appropriately described above, older adults have higher
Adults” for details (2). maintain the timing of meals and content rates of unidentified cognitive impairment
of diet. When clinicians are managing and dementia, leading to difficulties in
patients with cognitive dysfunction, it is adhering to complex self-care activities
NEUROCOGNITIVE FUNCTION
critical to simplify drug regimens and to (e.g., glucose monitoring, insulin dose
Recommendation facilitate and engage the appropriate sup- adjustment, etc.). Cognitive decline has
12.3 Screening for early detection of port structure to assist the patient in all been associated with increased risk of
mild cognitive impairment or de- aspects of care. hypoglycemia, and conversely, severe
mentia should be performed for Older adults with diabetes should be hypoglycemia has been linked to in-
adults 65 years of age or older at carefully screened and monitored for creased risk of dementia (31,32). There-
the initial visit and annually as cognitive impairment (2). Several simple fore, as discussed in Recommendation
appropriate. B assessment tools are available to screen 12.3, it is important to routinely screen
for cognitive impairment (23,24), such older adults for cognitive impairment
Older adults with diabetes are at higher as the Mini Mental State Examination and dementia and discuss findings with
risk of cognitive decline and institution- (25), Mini-Cog (26), and the Montreal the patients and their caregivers.
alization (11,12). The presentation of cog- Cognitive Assessment (27), which may Patients and their caregivers should
nitive impairment ranges from subtle help to identify patients requiring neu- be routinely queried about hypoglyce-
executive dysfunction to memory loss ropsychological evaluation, particularly mia (e.g., selected questions from the
and overt dementia. People with diabe- those in whom dementia is suspected Diabetes Care Profile) (33) and hypogly-
tes have higher incidences of all-cause (i.e., experiencing memory loss and de- cemia unawareness (34). Older patients
dementia, Alzheimer disease, and vascu- cline in their basic and instrumental ac- can also be stratified for future risk for
lar dementia than people with normal tivities of daily living). Annual screening is hypoglycemia with validated risk calcu-
glucose tolerance (13). The effects of hy- indicated for adults 65 years of age or lators (e.g., Kaiser Hypoglycemia Model)
perglycemia and hyperinsulinemia on older for early detection of mild cognitive (35). An important step to mitigating hy-
the brain are areas of intense research. impairment or dementia (4,28). Screen- poglycemia risk is to determine whether
Poor glycemic control is associated with a ing for cognitive impairment should ad- the patient is skipping meals or inadver-
decline in cognitive function (14,15), and ditionally be considered when a patient tently repeating doses of their medica-
longer duration of diabetes is associated presents with a significant decline in clinical tions. Glycemic targets and pharmacologic
with worsening cognitive function. There status due to increased problems with regimens may need to be adjusted to
are ongoing studies evaluating whether self-care activities, such as errors in cal- minimize the occurrence of hypoglyce-
preventing or delaying diabetes onset culating insulin dose, difficulty counting mic events (2). This recommendation is
may help to maintain cognitive function carbohydrates, skipped meals, skipped supported by observations from multi-
in older adults. However, studies exam- insulin doses, and difficulty recognizing, ple randomized controlled trials, such as
ining the effects of intensive glycemic and preventing, or treating hypoglycemia. Peo- the Action to Control Cardiovascular Risk
blood pressure control to achieve specific ple who screen positive for cognitive impair- in Diabetes (ACCORD) study and the Vet-
targets have not demonstrated a reduc- ment should receive diagnostic assessment erans Affairs Diabetes Trial (VADT), which
tion in brain function decline (16,17). as appropriate, including referral to a be- showed that intensive treatment proto-
Clinical trials of specific interventionsd havioral health provider for formal cogni- cols targeting A1C ,6.0% with complex
including cholinesterase inhibitors and tive/neuropsychological evaluation (29). drug regimens significantly increased
glutamatergic antagonistsdhave not shown the risk for hypoglycemia requiring as-
positive therapeutic benefit in maintain- sistance compared with standard treat-
ing or significantly improving cognitive func- HYPOGLYCEMIA ment (36,37). However, these intensive
tion or in preventing cognitive decline (18). treatment regimens included exten-
Recommendations
Pilot studies in patients with mild cognitive sive use of insulin and minimal use of
12.4 Because older adults with diabe-
impairmentevaluatingthepotentialbenefits glucagon-like peptide 1 (GLP-1) receptor
tes have a greater risk of hypo-
of intranasal insulin therapy and metformin agonists, and they preceded the avail-
glycemia than younger adults,
therapy provide insights for future clinical ability of sodium–glucose cotransporter
episodes of hypoglycemia should
trials and mechanistic studies (19–21). 2 (SGLT2) inhibitors.S170 Older Adults Diabetes Care Volume 44, Supplement 1, January 2021
For older patients with type 1 diabetes, A1C. In these instances, plasma blood
12.10 Treatment of other cardiovas-
continuous glucose monitoring (CGM) glucose fingerstick and sensor glucose
cular risk factors should be
may be another approach to reducing readings should be used for goal setting
individualized in older adults
the risk of hypoglycemia. In the Wireless (Table 12.1).
considering the time frame of
Innovation in Seniors with Diabetes Mel-
benefit. Lipid-lowering therapy
litus (WISDM) trial, patients over 60 years Healthy Patients With Good
and aspirin therapy may ben-
of age with type 1 diabetes were ran- Functional Status
efit those with life expectancies
domized to CGM or standard blood glu- There are few long-term studies in older
at least equal to the time frame
cose monitoring (BGM). Over 6 months, adults demonstrating the benefits of in-
of primary prevention or sec-
use of CGM resulted in a small but sta- tensive glycemic, blood pressure, and lipid
ondary intervention trials. E
tistically significant reduction in time control. Patients who can be expected to
spent with hypoglycemia (glucose level live long enough to reap the benefits of
The care of older adults with diabetes is
,70 mg/dL) compared with routine finger- long-term intensive diabetes management,
complicated by their clinical, cognitive,
stick monitoring using standard BGM who have good cognitive and physical
and functional heterogeneity. Some older
(adjusted treatment difference, 21.9% function, and who choose to do so via
individuals may have developed diabetes
[227 min per day]; 95% CI 22.8% to shared decision-making may be treated
years earlier and have significant com-
21.1% [240 to 216 min per day]; P , using therapeutic interventions and goals
plications, others are newly diagnosed
0.001) (38,39). While the current evi- similar to those for younger adults with
and may have had years of undiagnosed
dence base for older adults is primarily diabetes (Table 12.1).
diabetes with resultant complications,
in type 1 diabetes, CGM may be an option As with all patients with diabetes, di-
and still other older adults may have
for older patients with type 2 diabetes abetes self-management education and
truly recent-onset disease with few or ongoing diabetes self-management sup-
using multiple daily injections of insulin
no complications (40). Some older adults
(see Section 7 “Diabetes Technology,” port are vital components of diabetes
with diabetes have other underlying chronic care for older adults and their caregivers.
https://doi.org/10.2337/dc21-S007).
conditions, substantial diabetes-related Self-management knowledge and skills
comorbidity, limited cognitive or physical should be reassessed when regimen changes
TREATMENT GOALS functioning, or frailty (41,42). Other older are made or an individual’s functional
individuals with diabetes have little co- abilities diminish. In addition, declining
Recommendations morbidity and are active. Life expectan- or impaired ability to perform diabetes
12.6 Older adults who are otherwise cies are highly variable but are often longer self-care behaviors may be an indication
healthy with few coexisting than clinicians realize. Multiple prognostic that a patient needs a referral for cog-
chronic illnesses and intact cog- tools for life expectancy for older adults are nitive and physical functional assessment,
nitive function and functional available (43), including tools specifically using age-normalized evaluation tools, as
status should have lower glyce- designed for older adults with diabetes well as help establishing a support struc-
mic goals (such as A1C ,7.0– (44). Providers caring for older adults with ture for diabetes care (3,29).
7.5% [53–58 mmol/mol]), while diabetes must take this heterogeneity into
those with multiple coexisting consideration when setting and priori- Patients With Complications and
chronic illnesses, cognitive im- tizing treatment goals (9,10) (Table 12.1). Reduced Functionality
pairment, or functional depen- In addition, older adults with diabetes For patients with advanced diabetes com-
dence should have less stringent should be assessed for disease treatment plications, life-limiting comorbid illnesses,
glycemic goals (such as A1C and self-management knowledge, health or substantial cognitive or functional im-
,8.0–8.5% [64–69 mmol/mol]). literacy, and mathematical literacy (nu- pairments, it is reasonable to set less-
C meracy) at the onset of treatment. See intensive glycemic goals (Table 12.1).
12.7 Glycemic goals for some older Fig. 6.2 for patient- and disease-related Factors to consider in individualizing gly-
adults might reasonably be re- factors to consider when determining in- cemic goals are outlined in Fig. 6.2. These
laxed as part of individualized
dividualized glycemic targets. patients are less likely to benefit from
care, but hyperglycemia lead-
A1C is used as the standard biomarker reducing the risk of microvascular com-
ing to symptoms or risk of acute for glycemic control in all patients with plications and more likely to suffer se-
hyperglycemia complications
diabetes but may have limitations in rious adverse effects from hypoglycemia.
should be avoided in all pa-
patients who have medical conditions However, patients with poorly controlled
tients. C
that impact red blood cell turnover (see diabetes may be subject to acute compli-
12.8 Screening for diabetes compli-
Section 2 “Classification and Diagnosis cations of diabetes, including dehydration,
cations should be individual-
of Diabetes,” https://doi.org/10.2337/ poor wound healing, and hyperglycemic
ized in older adults. Particular
dc21-S002, for additional details on the hyperosmolar coma. Glycemic goals should,
attention should be paid to
limitations of A1C) (45). Many condi- at a minimum, avoid these consequences.
complications that would lead
tions associated with increased red blood
to functional impairment. C
cell turnover, such as hemodialysis, recent Vulnerable Patients at the End of Life
12.9 Treatment of hypertension to
blood loss or transfusion, or erythropoi- For patients receiving palliative care and
individualized target levels is in-
etin therapy, are commonly seen in older end-of-life care, the focus should be to
dicated in most older adults. C
adults and can falsely increase or decrease avoid hypoglycemia and symptomaticcare.diabetesjournals.org Older Adults S171
Table 12.1—Framework for considering treatment goals for glycemia, blood pressure, and dyslipidemia in older adults with
diabetes
Fasting or
Patient characteristics/ Reasonable preprandial
health status Rationale A1C goal‡ glucose Bedtime glucose Blood pressure Lipids
Healthy (few Longer remaining ,7.0–7.5% 80–130 mg/dL 80–180 mg/dL ,140/90 Statin unless
coexisting chronic life expectancy (53–58 mmol/mol) (4.4–7.2 (4.4–10.0 mmHg contraindicated
illnesses, intact mmol/L) mmol/L) or not tolerated
cognitive and
functional status)
Complex/ Intermediate ,8.0% 90–150 mg/dL 100–180 mg/dL ,140/90 Statin unless
intermediate remaining life (64 mmol/mol) (5.0–8.3 (5.6–10.0 mmHg contraindicated
(multiple coexisting expectancy, mmol/L) mmol/L) or not tolerated
chronic illnesses* or high treatment
21 instrumental burden,
ADL impairments or hypoglycemia
mild-to-moderate vulnerability,
cognitive fall risk
impairment)
Very complex/poor Limited remaining Avoid reliance on A1C; 100–180 mg/dL 110–200 mg/dL ,150/90 Consider
health (LTC or end- life expectancy glucose control (5.6–10.0 (6.1–11.1 mmHg likelihood of
stage chronic makes benefit decisions should be mmol/L) mmol/L) benefit with
illnesses** or uncertain based on avoiding statin
moderate-to- hypoglycemia and
severe cognitive symptomatic
impairment or 21 hyperglycemia
ADL impairments)
This table represents a consensus framework for considering treatment goals for glycemia, blood pressure, and dyslipidemia in older adults with diabetes.
The patient characteristic categories are general concepts. Not every patient will clearly fall into a particular category. Consideration of patient and caregiver
preferences is an important aspect of treatment individualization. Additionally, a patient’s health status and preferences may change over time. ADL,
activities of daily living; LTC, long-term care. ‡A lower A1C goal may be set for an individual if achievable without recurrent or severe hypoglycemia or undue
treatment burden. *Coexisting chronic illnesses are conditions serious enough to require medications or lifestyle management and may include
arthritis, cancer, congestive heart failure, depression, emphysema, falls, hypertension, incontinence, stage 3 or worse chronic kidney disease,
myocardial infarction, and stroke. “Multiple” means at least three, but many patients may have five or more (50). **The presence of a single end-stage
chronic illness, such as stage 3–4 congestive heart failure or oxygen-dependent lung disease, chronic kidney disease requiring dialysis, or uncontrolled
metastatic cancer, may cause significant symptoms or impairment of functional status and significantly reduce life expectancy. Adapted from
Kirkman et al. (3).
hyperglycemia while reducing the bur- and aspirin therapy, although the ben-
modest weight loss (e.g., 5–
dens of glycemic management. Thus, efits of these interventions for primary
7%) should be considered for
when organ failure develops, several prevention and secondary intervention
its benefits on quality of life,
agents will have to be deintensified or are likely to apply to older adults whose
mobility and physical function-
discontinued. For the dying patient, most life expectancies equal or exceed the
ing, and cardiometabolic risk
agents for type 2 diabetes may be re- time frames of the clinical trials.
factor control. A
moved (46). There is, however, no con-
sensus for the management of type 1
LIFESTYLE MANAGEMENT
diabetes in this scenario (47). See the sec- Diabetes in the aging population is as-
tion END-OF-LIFE CARE below, for additional Recommendations sociated with reduced muscle strength,
information. 12.11 Optimal nutrition and protein poor muscle quality, and accelerated loss
intake is recommended for of muscle mass, which may result in
Beyond Glycemic Control older adults; regular exercise, sarcopenia and/or osteopenia (51,52).
Although hyperglycemia control may be including aerobic activity, weight- Diabetes is also recognized as an in-
important in older individuals with di- bearing exercise, and/or re- dependent risk factor for frailty. Frailty
abetes, greater reductions in morbidity and sistance training, should be is characterized by decline in physical
mortality are likely to result from control of encouraged in all older adults performance and an increased risk of
other cardiovascular risk factors rather who can safely engage in such poor health outcomes due to physio-
than from tight glycemic control alone. activities. B logic vulnerability and functional or psy-
There is strong evidence from clinical 12.12 For older adults with type 2 chosocial stressors. Inadequate nutritional
trials of the value of treating hyperten- diabetes, overweight/obesity, intake, particularly inadequate protein
and capacity to safely exer- intake, can increase the risk of sarcopenia
sion in older adults (48,49), with treat-
cise, an intensive lifestyle in- and frailty in older adults. Management
ment of hypertension to individualized
tervention focused on dietary
target levels indicated in most. There is of frailty in diabetes includes optimal
changes, physical activity, and
less evidence for lipid-lowering therapy nutrition with adequate protein intakeS172 Older Adults Diabetes Care Volume 44, Supplement 1, January 2021
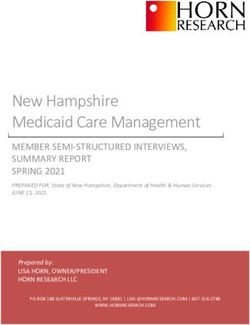
combined with an exercise program that distress without worsening glycemic
order to reduce risk of cost-
includes aerobic and resistance training control (75–77). Figure 12.1 depicts
related nonadherence. B
(53,54). an algorithm that can be used to sim-
Many older adults with type 2 diabetes plify the insulin regimen (75). There
also have overweight or obesity and will Special care is required in prescribing and are now multiple studies evaluating
benefit from an intensive lifestyle inter- monitoring pharmacologic therapies in deintensification protocols that, in gen-
vention. The Look Action for Health in older adults (66). See Fig. 9.1 for general eral, demonstrate that deintensification
Diabetes (Look AHEAD) trial is described recommendations regarding glucose- is safe and possibly beneficial for older
in Section 8 “Obesity Management for lowering treatment for adults with type adults (78). Table 12.2 provides exam-
the Treatment of Type 2 Diabetes” (https:// 2 diabetes and Table 9.1 for patient- and ples of and rationale for situations
doi.org/10.2337/dc21-S008). The trial en- drug-specific factors to consider when where deintensification and/or insulin
rolled patients between 45 and 74 years selecting glucose-lowering agents. Cost regimen simplification may be appro-
of age and required that patients be able may be an important consideration, es- priate in older adults.
perform a maximal exercise test (55,56). pecially as older adults tend to be on
many medications and live on fixed in- Metformin
While the Look AHEAD trial did not achieve
its primary outcome of reducing cardiovas-
comes (67). Accordingly, the costs of care Metformin is the first-line agent for older
and insurance coverage rules should be adults with type 2 diabetes. Recent
cular events, the intensive lifestyle in-
considered when developing treatment studies have indicated that it may be
tervention had multiple clinical benefits
plans to reduce the risk of cost-related used safely in patients with estimated
that are important to the quality of life of
older patients. Benefits included weight
nonadherence (68,69). See Table 9.2 and glomerular filtration rate $30 mL/min/
loss, improved physical fitness, increased
Table 9.3 for median monthly cost in the 1.73 m2 (81). However, it is contraindi-
U.S. of noninsulin glucose-lowering agents cated in patients with advanced renal
HDL cholesterol, lowered systolic blood
and insulin, respectively. It is important insufficiency and should be used with
pressure, reduced A1C levels, and reduced
to match complexity of the treatment caution in patients with impaired hepatic
waist circumference (57). Additionally,
regimen to the self-management ability function or congestive heart failure be-
several subgroups, including participants
of older patients and their available social cause of the increased risk of lactic
who lost at least 10% of baseline body
and medical support. Many older adults acidosis. Metformin may be temporarily
weight at year 1, had improved cardio-
with diabetes struggle to maintain the discontinued before procedures, during
vascular outcomes (58). Risk factor con-
frequent blood glucose monitoring and hospitalizations, and when acute illness
trol was improved with reduced utilization
insulin injection regimens they previ- may compromise renal or liver function.
of antihypertensive medications, statins,
ously followed, perhaps for many deca- Additionally, metformin can cause gastro-
and insulin (59). In age-stratified analyses,
des, as they develop medical conditions intestinal side effects and a reduction in
older patients in the trial (60 to early 70s)
that may impair their ability to follow appetite that can be problematic for
had similar benefits compared with youn-
their regimen safely. Individualized gly- some older adults. Reduction or elimi-
ger patients (60,61). In addition, lifestyle
cemic goals should be established (Fig. nation of metformin may be necessary
intervention produced benefits on aging-
6.2) and periodically adjusted based for patients experiencing persistent gas-
relevant outcomes like better physical
on coexisting chronic illnesses, cognitive trointestinal side effects.
function and quality of life (62–65).
function, and functional status (2).
Tight glycemic control in older adults
Thiazolidinediones
PHARMACOLOGIC THERAPY with multiple medical conditions is
Thiazolidinediones, if used at all, should
considered over treatment and is as-
Recommendations be used very cautiously in those patients
sociated with an increased risk of
12.13 In older adults with type 2 di- on insulin therapy as well as those pa-
hypoglycemia; overtreatment is unfor-
abetes at increased risk of hy- tients with or at risk for congestive heart
tunately common in clinical practice
poglycemia, medication classes failure, osteoporosis, falls or fractures,
(50,70–73). Deintensification of regi-
with low risk of hypoglycemia and/or macular edema (82,83).
mens in patients taking noninsulin
are preferred. B
glucose-lowering medications can be
12.14 Overtreatment of diabetes is
achieved by either lowering the dose Insulin Secretagogues
common in older adults and Sulfonylureas and other insulin secreta-
or discontinuing some medications, as
should be avoided. B gogues are associated with hypoglycemia
long as the individualized glycemic targets
12.15 Deintensification (or simplifica- and should be used with caution. If used,
are maintained. When patients are found
tion) of complex regimens is sulfonylureas with a shorter duration of
to have an insulin regimen with com-
recommended to reduce the action, such as glipizide or glimepiride,
plexity beyond their self-management
risk of hypoglycemia and poly- are preferred. Glyburide is a longer-
abilities, lowering the dose of insulin
pharmacy, if it can be achieved acting sulfonylurea and should be avoided
may not be adequate (74). Simplification
within the individualized A1C in older adults (84).
of the insulin regimen to match an in-
target. B
dividual’s self-management abilities and
12.16 Consider costs of care and in-
their available social and medical support Incretin-Based Therapies
surance coverage rules when
in these situations has been shown to Oral dipeptidyl peptidase 4 (DPP-4) inhib-
developing treatment plans in
reduce hypoglycemia and disease-related itors have few side effects and minimalcare.diabetesjournals.org Older Adults S173
risk of hypoglycemia, but their cost doi.org/10.2337/dc21-S009) and Section aged ,65 years to those aged 65–75 years
may be a barrier to some older patients. 10 “Cardiovascular Disease and Risk Man- and a smaller group aged $75 years (91).
DPP-4 inhibitors do not increase major agement” (https://doi.org/10.2337/dc21- While the evidence for this class for older
adverse cardiovascular outcomes (85). S010) for a more extensive discussion patients continues to grow, there are a
Across the trials of this drug class, there regarding the specific indications for this number of practical issues that should be
appears to be no interaction by age- class. The stratified analyses of several of considered for older patients. These drugs
group (86–88). A challenge of inter- the trials of this drug class indicate a are injectable agents (with the exception
preting the age-stratified analyses of complex interaction with age. In the of oral semaglutide) (92), which require
this drug class and other cardiovas- Liraglutide Effect and Action in Diabetes: visual, motor, and cognitive skills for
cular outcomes trials is that while Evaluation of Cardiovascular Outcome appropriate administration. They may
most of these analyses were prespeci- Results (LEADER) trial with liraglutide, also be associated with nausea, vomiting,
fied, they were not powered to detect those aged $50 years with CVD at base- and diarrhea. Given the gastrointestinal
differences. line had a reduction in primary outcome side-effects of this class, GLP-1 receptor
GLP-1 receptor agonists have demon- (n 5 7,598; hazard ratio [HR] 0.83), agonists may not be preferred in older
strated cardiovascular benefits among whereas those aged $60 years with no patients who are experiencing unexplained
patients with established atherosclerotic established CVD had a significantly ad- weight loss.
cardiovascular disease (CVD), and newer verse outcome (n 5 1,742; HR 1.20, P 5
trials are expanding our understanding 0.04), except in a small subgroup of those Sodium–Glucose Cotransporter 2
of their benefits in other populations aged $75 years (89,90). A similar trend Inhibitors
(85). See Section 9 “Pharmacologic Ap- was seen in the Harmony Outcomes trial SGLT2 inhibitors are administered orally,
proaches to Glycemic Treatment” (https:// with albiglutide, comparing participants which may be convenient for older
(5.0
(5.0
Figure 12.1—Algorithm to simplify insulin regimen for older patients with type 2 diabetes. eGFR, estimated glomerular filtration rate. *Basal insulins:
glargine U-100 and U-300, detemir, degludec, and human NPH. **See Table 12.1. UMealtime insulins: short-acting (regular human insulin) or rapid-
acting (lispro, aspart, and glulisine). §Premixed insulins: 70/30, 75/25, and 50/50 products. Adapted with permission from Munshi and colleagues
(75,79,80).S174 Older Adults Diabetes Care Volume 44, Supplement 1, January 2021
Table 12.2—Considerations for treatment regimen simplification and deintensification/deprescribing in older adults with
diabetes (75,79)
When may treatment
Patient characteristics/ Reasonable A1C/ When may regimen deintensification/
health status treatment goal Rationale/considerations simplification be required? deprescribing be required?
Healthy (few coexisting A1C ,7.0–7.5% (53–58 c Patients can generally c If severe or recurrent c If severe or recurrent
chronic illnesses, intact mmol/mol) perform complex tasks to hypoglycemia occurs in hypoglycemia occurs in
cognitive and maintain good glycemic patients on insulin therapy patients on noninsulin
functional status) control when health is (even if A1C is appropriate) therapies with high risk of
stable c If wide glucose excursions hypoglycemia (even if A1C
c During acute illness, are observed is appropriate)
patients may be more at c If cognitive or functional c If wide glucose excursions
risk for administration or decline occurs following are observed
dosing errors that can acute illness c In the presence of
result in hypoglycemia, polypharmacy
falls, fractures, etc.
Complex/intermediate A1C ,8.0% (64 mmol/mol) c Comorbidities may affect c If severe or recurrent c If severe or recurrent
(multiple coexisting self-management hypoglycemia occurs in hypoglycemia occurs in
chronic illnesses or 21 abilities and capacity to patients on insulin therapy patients on noninsulin
instrumental ADL avoid hypoglycemia (even if A1C is appropriate) therapies with high risk of
impairments or mild- c Long-acting medication c If unable to manage hypoglycemia (even if A1C
to-moderate cognitive formulations may complexity of an insulin is appropriate)
impairment) decrease pill burden and regimen c If wide glucose excursions
complexity of c If there is a significant are observed
medication regimen change in social c In the presence of
circumstances, such as loss polypharmacy
of caregiver, change in
living situation, or financial
difficulties
Community-dwelling Avoid reliance on A1C c Glycemic control is c If treatment regimen c If the hospitalization for
patients receiving care Glucose target: 100–200 important for recovery, increased in complexity acute illness resulted in
in a skilled nursing mg/dL (5.55–11.1 mmol/L) wound healing, during hospitalization, it is weight loss, anorexia,
facility for short-term hydration, and avoidance reasonable, in many cases, short-term cognitive
rehabilitation of infections to reinstate the decline, and/or loss of
c Patients recovering from prehospitalization physical functioning
illness may not have medication regimen during
returned to baseline the rehabilitation
cognitive function at the
time of discharge
c Consider the type of
support the patient will
receive at home
Very complex/poor Avoid reliance on A1C. c No benefits of tight c If on an insulin regimen and c If on noninsulin agents
health (long-term care Avoid hypoglycemia glycemic control in this the patient would like to with a high hypoglycemia
or end-stage chronic and symptomatic population decrease the number of risk in the context of
illnesses or moderate- hyperglycemia c Hypoglycemia should be injections and fingerstick cognitive dysfunction,
to-severe cognitive avoided blood glucose monitoring depression, anorexia, or
impairment or 21 ADL c Most important events each day inconsistent eating
impairments) outcomes are c If the patient has an pattern
maintenance of inconsistent eating pattern c If taking any medications
cognitive and functional without clear benefits
status
At the end of life Avoid hypoglycemia c Goal is to provide c If there is pain or c If taking any medications
and symptomatic comfort and avoid tasks discomfort caused by without clear benefits in
hyperglycemia or interventions that treatment (e.g., injections improving symptoms
cause pain or discomfort or fingersticks) and/or comfort
c Caregivers are important c If there is excessive
in providing medical care caregiver stress due to
and maintaining quality treatment complexity
of life
Treatment regimen simplification refers to changing strategy to decrease the complexity of a medication regimen, e.g., fewer administration times,
fewer blood glucose checks, and decreasing the need for calculations (such as sliding scale insulin calculations or insulin-carbohydrate ratio calculations).
Deintensification/deprescribing refers to decreasing the dose or frequency of administration of a treatment or discontinuing a treatment altogether.
ADL, activities of daily living.care.diabetesjournals.org Older Adults S175
adults with diabetes. In patients with Older adults in assisted living facilities patient’s family may be more familiar
established atherosclerotic CVD, these may not have support to administer their with diabetes management than the
agents have shown cardiovascular ben- own medications, whereas those living providers. Education of relevant support
efits (85). This class of agents has also in a nursing home (community living staff and providers in rehabilitation and
been found to be beneficial for patients centers) may rely completely on the care LTC settings regarding insulin dosing and
with heart failure and to slow the pro- plan and nursing support. Those receiving use of pumps and CGM is recommended
gression of chronic kidney disease. See palliative care (with or without hospice) as part of general diabetes education (see
Section 9 “Pharmacologic Approaches to may require an approach that emphasizes Recommendations 12.17 and 12.18).
Glycemic Treatment” (https://doi.org/10 comfort and symptom management, while
.2337/dc21-S009) and Section 10 “Cardio- de-emphasizing strict metabolic and blood
TREATMENT IN SKILLED NURSING
vascular Disease and Risk Management” pressure control. FACILITIES AND NURSING HOMES
(https://doi.org/10.2337/dc21-S010) for a
more extensive discussion regarding the SPECIAL CONSIDERATIONS FOR Recommendations
indications for this class of agents. The OLDER ADULTS WITH TYPE 1 12.17 Consider diabetes education for
stratified analyses of the trials of this DIABETES the staff of long-term care and
drug class indicate that older patients Due in part to the success of modern rehabilitation facilities to im-
have similar or greater benefits than youn- diabetes management, patients with prove the management of older
ger patients (93–95). While understand- type 1 diabetes are living longer, and adults with diabetes. E
ing of the clinical benefits of this class is the population of these patients over 12.18 Patients with diabetes residing
evolving, side effects such as volume 65 years of age is growing (96–99). Many in long-term care facilities need
depletion may be more common among of the recommendations in this section careful assessment to establish
older patients. regarding a comprehensive geriatric as- individualized glycemic goals and
sessment and personalization of goals to make appropriate choices of
Insulin Therapy and treatments are directly applicable glucose-lowering agents based
The use of insulin therapy requires that to older adults with type 1 diabetes; on their clinical and functional
patients or their caregivers have good however, this population has unique status. E
visual and motor skills and cognitive ability. challenges and requires distinct treat-
Insulin therapy relies on the ability of the ment considerations (100). Insulin is an Management of diabetes in the LTC
older patient to administer insulin on their essential life-preserving therapy for pa- setting is unique. Individualization of health
own or with the assistance of a caregiver. tients with type 1 diabetes, unlike for care is important in all patients; however,
Insulin doses should be titrated to meet those with type 2 diabetes. To avoid practical guidance is needed for medical
individualized glycemic targets and to avoid diabetic ketoacidosis, older adults with providers as well as the LTC staff and
hypoglycemia. type 1 diabetes need some form of basal caregivers (102). Training should include
Once-daily basal insulin injection ther- insulin even when they are unable to diabetes detection and institutional quality
apy is associated with minimal side ef- ingest meals. Insulin may be delivered assessment. LTC facilities should develop
fects and may be a reasonable option in through an insulin pump or injections. their own policies and procedures for pre-
many older patients. Multiple daily in- CGM is approved for use by Medicare and vention and management of hypoglycemia.
jections of insulin may be too complex for can play a critical role in improving A1C,
the older patient with advanced diabetes reducing glycemic variability, and reduc- Resources
complications, life-limiting coexisting chronic ing risk of hypoglycemia (101) (see Sec- Staff of LTC facilities should receive ap-
illnesses, or limited functional status. tion 7 “Diabetes Technology,” https://doi propriate diabetes education to im-
Figure 12.1 provides a potential approach .org/10.2337/dc21-S007, and Section 9 prove the management of older adults
to insulin regimen simplification. “Pharmacologic Approaches to Glycemic with diabetes. Treatments for each pa-
Treatment,” https://doi.org/10.2337/dc21- tient should be individualized. Special
Other Factors to Consider S009). In the older patient with type 1 management considerations include the
The needs of older adults with diabetes diabetes, administration of insulin may need to avoid both hypoglycemia and the
and their caregivers should be evaluated become more difficult as complications, complications of hyperglycemia (2,103).
to construct a tailored care plan. Impaired cognitive impairment, and functional im- For more information, see the ADA po-
social functioning may reduce these pa- pairment arise. This increases the impor- sition statement “Management of Diabe-
tients’ quality of life and increase the risk tance of caregivers in the lives of these tes in Long-term Care and Skilled Nursing
of functional dependency (7). The patient’s patients. Many older patients with type 1 Facilities” (102).
living situation must be considered as it diabetes require placement in long-term
may affect diabetes management and care (LTC) settings (i.e., nursing homes Nutritional Considerations
support needs. Social and instrumental and skilled nursing facilities), and un- An older adult residing in an LTC facility may
support networks (e.g., adult children, fortunately these patients encounter have irregular and unpredictable meal con-
caretakers) that provide instrumental or providers that are unfamiliar with in- sumption, undernutrition, anorexia, and im-
emotional support for older adults with sulin pumps or CGM. Some providers paired swallowing.Furthermore, therapeutic
diabetes should be included in diabetes may be unaware of the distinction be- diets may inadvertently lead to decreased
management discussions and shared tween type 1 and type 2 diabetes. In food intake and contribute to unintentional
decision-making. these instances, the patient or the weightlossandundernutrition.DietstailoredS176 Older Adults Diabetes Care Volume 44, Supplement 1, January 2021
to a patient’s culture, preferences, and per- END-OF-LIFE CARE basal insulin can be implemented, accom-
sonal goals may increase quality of life, panied by oral agents and without rapid-
Recommendations
satisfaction with meals, and nutrition acting insulin. Agents that can cause gas-
12.19 When palliative care is needed
status (104). It may be helpful to give trointestinal symptoms such as nausea or
in older adults with diabetes,
insulin after meals to ensure that the excess weight loss may not be good choices
providers should initiate con-
dose is appropriate for the amount of in this setting. As symptoms progress,
versations regarding the goals
carbohydrate the patient consumed in some agents may be slowly tapered
and intensity of care. Strict glu-
the meal. and discontinued.
cose and blood pressure con-
Different patient categories have been
trol may not be necessary E,
Hypoglycemia proposed for diabetes management in
and reduction of therapy may
Older adults with diabetes in LTC are es- those with advanced disease (47).
be appropriate. Similarly, the
pecially vulnerable to hypoglycemia. They intensity of lipid management
have a disproportionately high number 1. A stable patient: Continue with the
can be relaxed, and withdrawal
of clinical complications and comorbid- patient’s previous regimen, with a
of lipid-lowering therapy may
ities that can increase hypoglycemia risk: focus on the prevention of hypo-
be appropriate. A
impaired cognitive and renal function, glycemia and the management of
12.20 Overall comfort, prevention of
slowed hormonal regulation and counter- hyperglycemia using blood glucose
distressing symptoms, and pre-
regulation, suboptimal hydration, variable testing, keeping levels below the re-
servation of quality of life and
appetite and nutritional intake, polyphar- nal threshold of glucose. There is very
dignity are primary goals for di-
macy, and slowed intestinal absorption little role for A1C monitoring and
abetes management at the end
(105). Oral agents may achieve glycemic lowering.
of life. C
outcomes in LTC populations similar to 2. A patient with organ failure: Pre-
basal insulin (70,106). venting hypoglycemia is of greater
Another consideration for the LTC significance. Dehydration must be
setting is that, unlike in the hospital setting, The management of the older adult at the prevented and treated. In people
medical providers are not required to end of life receiving palliative medicine or with type 1 diabetes, insulin admin-
evaluate the patients daily. According to hospice care is a unique situation. Over- istration may be reduced as the oral
federal guidelines, assessments should be all, palliative medicine promotes com- intake of food decreases but should
done at least every 30 days for the first fort, symptom control and prevention not be stopped. For those with type 2
90 days after admission and then at least (pain, hypoglycemia, hyperglycemia, and diabetes, agents that may cause
once every 60 days. Although in practice the dehydration), and preservation of dignity hypoglycemia should be reduced
patients may actually be seen more fre- and quality of life in patients with limited in dose. The main goal is to avoid
quently, the concern is that patients may life expectancy (103,107). In the setting of hypoglycemia, allowing for glucose
have uncontrolled glucose levels or wide palliative care, providers should initiate values in the upper level of the de-
excursions without the practitioner being conversations regarding the goals and in- sired target range.
notified. Providers may make adjustments tensity of diabetes care; strict glucose and 3. A dying patient: For patients with
to treatment regimens by telephone, fax, blood pressure control may not be con- type 2 diabetes, the discontinuation
or in person directly at the LTC facilities sistent with achieving comfort and quality of all medications may be a reason-
provided they are given timely notification of life. In a multicenter trial, withdrawal of able approach, as patients are un-
of blood glucose management issues statins among patients in palliative care likely to have any oral intake. In
from a standardized alert system. was found to improve quality of life, while patients with type 1 diabetes, there
The following alert strategy could be similar evidence for glucose and blood is no consensus, but a small amount
considered: pressure control are not yet available of basal insulin may maintain glucose
(108–110). A patient has the right to refuse levels and prevent acute hyperglyce-
1. Call provider immediately in cases of testing and treatment, whereas providers mic complications.
low blood glucose levels (,70 mg/dL may consider withdrawing treatment and
[3.9 mmol/L]). limiting diagnostic testing, including a re-
References
2. Call as soon as possible when duction in the frequency of blood glu- 1. Laiteerapong N, Huang E. Diabetes in older
a) glucose values are 70–100 mg/dL cose monitoring (111,112). Glucose targets adults. In Diabetes in America. 3rd ed. Cowie C,
(3.9–5.6 mmol/L) (regimen may should aim to prevent hypoglycemia and Casagrande S, Menke A, et al., Eds. Bethesda,
need to be adjusted), hyperglycemia. Treatment interventions MD, National Institutes of Health, 2017, pp.
b) glucose values are .250 mg/dL need to be mindful of quality of life. 16.11–16.26 (NIH publ. no. 17-1468)
2. Centers for Disease Control and Prevention.
(13.9 mmol/L) within a 24-h period, Careful monitoring of oral intake is war- National Diabetes Statistics Report: estimates of
c) glucose values are .300 mg/dL (16.7 ranted. The decision process may need to diabetes and its burden in the United States,
mmol/L) over 2 consecutive days, involve the patient, family, and caregivers, 2020. Accessed 9 October 2020. Available from
d) any reading is too high for the leading to a care plan that is both conve- https://www.cdc.gov/diabetes/pdfs/data/
glucometer, or nient and effective for the goals of care statistics/national-diabetes-statistics-report.pdf
3. Kirkman MS, Briscoe VJ, Clark N, et al. Diabetes
e) the patient is sick, with vomiting, (113). The pharmacologic therapy may in older adults. Diabetes Care 2012;35:2650–2664
symptomatic hyperglycemia, or poor include oral agents as first line, followed 4. Young-Hyman D, de Groot M, Hill-Briggs F,
oral intake. by a simplified insulin regimen. If needed, Gonzalez JS, Hood K, Peyrot M. Psychosocial carecare.diabetesjournals.org Older Adults S177 for people with diabetes: a position statement of 20. Freiherr J, Hallschmid M, Frey WH 2nd, et al. a prospective study of hypoglycemic frequency the American Diabetes Association. Diabetes Intranasal insulin as a treatment for Alzheimer’s and associated symptoms. Diabetes Care 1995;18: Care 2016;39:2126–2140 disease: a review of basic research and clinical 517–522 5. Institute of Medicine of the National Acad- evidence. CNS Drugs 2013;27:505–514 35. Karter AJ, Warton EM, Lipska KJ, et al. De- emies. Cognitive Aging: Progress in Understand- 21. Alagiakrishnan K, Sankaralingam S, Ghosh M, velopment and validation of a tool to identify ing and Opportunities for Action, 2015. Accessed Mereu L, Senior P. Antidiabetic drugs and their patients with type 2 diabetes at high risk of 9 October 2020. Available from http:// potential role in treating mild cognitive impair- hypoglycemia-related emergency department or nationalacademies.org/hmd/Reports/2015/ ment and Alzheimer’s disease. Discov Med 2013; hospital use. JAMA Intern Med 2017;177:1461– Cognitive-Aging.aspx 16:277–286 1470 6. Sudore RL, Karter AJ, Huang ES, et al. Symp- 22. Tomlin A, Sinclair A. The influence of cog- 36. Gerstein HC, Miller ME, Byington RP, et al.; tom burden of adults with type 2 diabetes across nition on self-management of type 2 diabetes in Action to Control Cardiovascular Risk in Diabetes the disease course: diabetes & aging study. J Gen older people. Psychol Res Behav Manag 2016;9: Study Group. Effects of intensive glucose low- Intern Med 2012;27:1674–1681 7–20 ering in type 2 diabetes. N Engl J Med 2008;358: 7. Laiteerapong N, Karter AJ, Liu JY, et al. Cor- 23. National Institute on Aging. Assessing cog- 2545–2559 relates of quality of life in older adults with nitive impairment in older patients. Accessed 37. Duckworth W, Abraira C, Moritz T, et al.; diabetes: the diabetes & aging study. Diabetes 9 October 2020. Available from https://www.nia VADT Investigators. Glucose control and vascular Care 2011;34:1749–1753 .nih.gov/health/assessing-cognitive-impairment- complications in veterans with type 2 diabetes. 8. McClintock MK, Dale W, Laumann EO, Waite L. older-patients N Engl J Med 2009;360:129–139 Empirical redefinition of comprehensive health 24. Alzheimer’s Association. Cognitive Assess- 38. Carlson AL, Kanapka LG, Miller KM, et al.; and well-being in the older adults of the United ment: Alzheimer’s Disease and Dementia. Ac- WISDM Study Group. Hypoglycemia and glyce- States. Proc Natl Acad Sci U S A 2016;113:E3071– cessed 9 October 2020. Available from: https://alz mic control in older adults with type 1 diabetes: E3080 .org/professionals/healthcare-professionals/ baseline results from the WISDM study. J Di- 9. Laiteerapong N, Iveniuk J, John PM, Laumann cognitive-assessment abetes Sci Technol 21 December 2019 [Epub EO, Huang ES. Classification of older adults 25. Folstein MF, Folstein SE, McHugh PR. “Mini- ahead of print]. DOI: 1932296819894974 who have diabetes by comorbid conditions, mental state”: A practical method for grading the 39. Pratley RE, Kanapka LG, Rickels MR, et al.; United States, 2005-2006. Prev Chronic Dis cognitive state of patients for the clinician. J Wireless Innovation for Seniors With Diabetes 2012;9:E100 Psychiatr Res 1975;12:189–198 Mellitus (WISDM) Study Group. Effect of con- 10. Blaum C, Cigolle CT, Boyd C, et al. Clinical 26. Borson S, Scanlan JM, Chen P, Ganguli M. The tinuous glucose monitoring on hypoglycemia in complexity in middle-aged and older adults with Mini-Cog as a screen for dementia: validation in a older adults with type 1 diabetes: a randomized diabetes: the Health and Retirement Study. Med population-based sample. J Am Geriatr Soc 2003; clinical trial. JAMA 2020;323:2397–2406 Care 2010;48:327–334 51:1451–1454 40. Selvin E, Coresh J, Brancati FL. The burden 11. Cukierman T, Gerstein HC, Williamson JD. 27. Nasreddine ZS, Phillips NA, Bédirian V, et al. and treatment of diabetes in elderly individuals in Cognitive decline and dementia in diabetes– The Montreal Cognitive Assessment, MoCA: the U.S. Diabetes Care 2006;29:2415–2419 systematic overview of prospective observational a brief screening tool for mild cognitive impair- 41. Bandeen-Roche K, Seplaki CL, Huang J, et al. studies. Diabetologia 2005;48:2460–2469 ment. J Am Geriatr Soc 2005;53:695–699 Frailty in older adults: a nationally representative 12. Roberts RO, Knopman DS, Przybelski SA, 28. Moreno G, Mangione CM, Kimbro L, profile in the United States. J Gerontol A Biol Sci et al. Association of type 2 diabetes with brain Vaisberg E; American Geriatrics Society Expert Med Sci 2015;70:1427–1434 atrophy and cognitive impairment. Neurology Panel on Care of Older Adults with Diabetes 42. Kalyani RR, Tian J, Xue Q-L, et al. Hypergly- 2014;82:1132–1141 Mellitus. Guidelines abstracted from the Amer- cemia and incidence of frailty and lower extrem- 13. Xu WL, von Strauss E, Qiu CX, Winblad B, ican Geriatrics Society Guidelines for Improving ity mobility limitations in older women. J Am Fratiglioni L. Uncontrolled diabetes increases the Care of Older Adults with Diabetes Mellitus: Geriatr Soc 2012;60:1701–1707 the risk of Alzheimer’s disease: a population- 2013 update. J Am Geriatr Soc 2013;61:2020– 43. Pilla SJ, Schoenborn NL, Maruthur NM, based cohort study. Diabetologia 2009;52: 2026 Huang ES. Approaches to risk assessment among 1031–1039 29. American Psychological Association. Guide- older patients with diabetes. Curr Diab Rep 2019; 14. Yaffe K, Falvey C, Hamilton N, et al. Diabetes, lines for the evaluation of dementia and age- 19:59 glucose control, and 9-year cognitive decline related cognitive change. Accessed 9 October 44. Griffith KN, Prentice JC, Mohr DC, Conlin PR. among older adults without dementia. Arch 2020. Available from http://www.apa.org/practice/ Predicting 5- and 10-year mortality risk in older Neurol 2012;69:1170–1175 guidelines/dementia.aspx adults with diabetes. Diabetes Care 2020;43: 15. Rawlings AM, Sharrett AR, Schneider ALC, 30. Lee AK, Lee CJ, Huang ES, Sharrett AR, Coresh 1724–1731 et al. Diabetes in midlife and cognitive change J, Selvin E. Risk factors for severe hypoglycemia in 45. NGSP. Factors that interfere with HbA1c over 20 years: a cohort study. Ann Intern Med black and white adults with diabetes: the Ath- test results. Accessed 9 October 2020. Available 2014;161:785–793 erosclerosis Risk in Communities (ARIC) study. from http://www.ngsp.org/factors.asp 16. Launer LJ, Miller ME, Williamson JD, et al.; Diabetes Care 2017;40:1661–1667 46. Sinclair A, Dunning T, Colagiuri S. IDF Global ACCORD MIND investigators. Effects of intensive 31. Feinkohl I, Aung PP, Keller M, et al.; Edin- Guideline For Managing Older People With glucose lowering on brain structure and function burgh Type 2 Diabetes Study (ET2DS) Investiga- Type 2 Diabetes. Brussels, Belgium, International in people with type 2 diabetes (ACCORD MIND): tors. Severe hypoglycemia and cognitive decline Diabetes Federation, 2013 a randomised open-label substudy. Lancet Neu- in older people with type 2 diabetes: the Edin- 47. Angelo M, Ruchalski C, Sproge BJ. An approach rol 2011;10:969–977 burgh type 2 diabetes study. Diabetes Care 2014; to diabetes mellitus in hospice and palliative 17. Murray AM, Hsu F-C, Williamson JD, et al.; 37:507–515 medicine. J Palliat Med 2011;14:83–87 Action to Control Cardiovascular Risk in Diabetes 32. Lee AK, Rawlings AM, Lee CJ, et al. Severe 48. Beckett NS, Peters R, Fletcher AE, et al.; Follow-On Memory in Diabetes (ACCORDION hypoglycaemia, mild cognitive impairment, de- HYVET Study Group. Treatment of hypertension MIND) Investigators. ACCORDION MIND: results mentia and brain volumes in older adults with in patients 80 years of age or older. N Engl J Med of the observational extension of the ACCORD type 2 diabetes: the Atherosclerosis Risk in 2008;358:1887–1898 MIND randomised trial. Diabetologia 2017;60: Communities (ARIC) cohort study. Diabetologia 49. de Boer IH, Bangalore S, Benetos A, et al. 69–80 2018;61:1956–1965 Diabetes and hypertension: a position statement 18. Ghezzi L, Scarpini E, Galimberti D. Disease- 33. Fitzgerald JT, Davis WK, Connell CM, Hess GE, by the American Diabetes Association. Diabetes modifying drugs in Alzheimer’s disease. Drug Des Funnell MM, Hiss RG. Development and valida- Care 2017;40:1273–1284 Devel Ther 2013;7:1471–1478 tion of the Diabetes Care Profile. Eval Health Prof 50. Arnold SV, Lipska KJ, Wang J, Seman L, 19. Craft S, Baker LD, Montine TJ, et al. Intranasal 1996;19:208–230 Mehta SN, Kosiborod M. Use of intensive insulin therapy for Alzheimer disease and am- 34. Clarke WL, Cox DJ, Gonder-Frederick LA, glycemic management in older adults with di- nestic mild cognitive impairment: a pilot clinical Julian D, Schlundt D, Polonsky W. Reduced aware- abetes mellitus. J Am Geriatr Soc 2018;66:1190– trial. Arch Neurol 2012;69:29–38 ness of hypoglycemia in adults with IDDM: 1194
You can also read