Why California Needs Better Data Exchange: Challenges, Impacts, and Policy Options for a 21st Century Health System
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Why California Needs Better Data Exchange:
Challenges, Impacts, and Policy Options for a
21st Century Health System
MARCH 2021
AUTHORS
Jonah Frohlich, Eric Bartholet, and Jonathan DiBello
at Manatt HealthContents
About the Author 3 Introduction
This paper was authored by Jonah Frohlich and
Eric Bartholet, managing directors; and Jonathan 4 Real-Life Scenarios: Challenges and Impacts
DiBello, consultant at Manatt Health. Manatt Disaster Response
Health integrates legal and consulting expertise to
Pandemic Response and Public Health Reporting
better serve the complex needs of clients across
the health care system. Combining legal excel- Serving Patients with Complex Needs
lence, firsthand experience in shaping public policy, Quality Reporting and Value-Based Care
strategy insight, and deep analytic capabilities,
Manatt Health provides professional services to the 10 Key Actions for Consideration
full range of health industry players. This diverse Align Leadership Across State Purchasing, Regulatory,
team of more than 160 attorneys and consultants Health, and Social Service Agencies
from Manatt, Phelps & Phillips and its consulting
Address Data Fragmentation
subsidiary, Manatt Health Strategies, helps clients
advance their business interests, fulfill their mis- Address Exclusion of Exchange Sectors
sions, and lead health care into the future.
14 Conclusion
About the Foundation 15 Appendix. Interviewees
The California Health Care Foundation is dedi-
16 Endnotes
cated to advancing meaningful, measurable
improvements in the way the health care delivery
system provides care to the people of California,
particularly those with low incomes and those
whose needs are not well served by the status quo.
We work to ensure that people have access to the
care they need, when they need it, at a price they
can afford.
CHCF informs policymakers and industry leaders,
invests in ideas and innovations, and connects
with changemakers to create a more responsive,
patient-centered health care system.
ABOUT THE SERIES
This is the second in a series of reports sponsored by
CHCF aimed at helping inform California decision-
makers about statewide data exchange. Other reports
focus on how other states have approached statewide
health information exchange, and on the existing
electronic health record networks, regional health
information organizations, and competing infrastruc-
ture that currently exist in California.
California Health Care Foundation www.chcf.org 2Introduction
T
he efficient, effective, and equitable delivery of To address the shortcomings of the current HIE envi-
care is vital to the well-being of all Californians ronment in California, three key data exchange issues
and is necessary for a strong and vibrant econ- need to be resolved:
omy. To achieve this state, information must easily be
exchanged among medical, behavioral, social ser- 1. Clinical data fragmentation. A range of issues
vices, and public health professionals to allow them results in incomplete and isolated islands of patient
to make informed decisions that impact the lives of data being available through California’s current HIE
every resident. ecosystem. These include a lack of full provider par-
ticipation in HIE in communities served by regional
Today, access to this kind of critical information is lim- HIOs, inclusion of only a subset of EHR data shared
ited, with the exchange of health data confined to a through exchanges, inconsistent participation in
subset of clinical patient information shared mostly and data sharing between national and regional
among larger clinics and hospitals that have federally exchanges, and an array of private, exclusionary
certified electronic health record (EHR) technologies.1 direct exchange solutions. Further, this fragmenta-
The health information exchange (HIE) ecosystem tion creates inequities in how data are accessed.
across California is composed of a combination of There are voids in HIE network coverage in many
direct exchange between providers, the use of national California counties — disproportionately rural and
networks, and over 15 regional health information underserved communities that often find adopting
organizations (HIOs). This fragmented model delivers and using EHR technology to share data prohibi-
inconsistent and incomplete solutions that don’t pro- tively expensive — generally excluding them from
vide all of the critical information needed to care for the benefits of HIE and leaving significant gaps in
the state’s residents, don’t provide access to all the available data. The issue of fragmentation results
service providers who need data, and don’t scale to in incomplete data sharing, creates complexity, and
provide state health care leaders with the access to restricts access and use of critical data, limiting the
data they need. Coupled with restrictive, confusing, value of the exchange platforms and eroding confi-
and ambiguous data exchange rules, the exchange dence in their completeness.
environment does not and cannot adequately enable
initiatives to improve care quality; enhance access to 2. Exclusion of exchange sectors. Regional HIOs
medical, social, and public health services; reduce dis- and national networks were developed to support
parities; and lower costs for residents, counties, and clinical data exchange. By and large, they do not
the state. support the broader requirements associated with
organizing and delivering comprehensive clini-
For an overview of California’s HIE ecosystem and cal, behavioral, social, and emergency services for
context on the different types of HIE, please see California’s residents. By omitting payers and pur-
the recent CHCF publication Health Information chasers, public health, social service, behavioral
Exchange in California: Overview of Network Types health, and in most cases, emergency response
and Characteristics. providers, HIOs and national networks are not able
to capture and deliver critical information vital to
addressing inherent inequities in access, outcomes,
and social determinants of health. As a result,
providers caring for California’s underresourced
populations cannot see and meet all their complex
needs. Additionally, the lack of adequate data shar-
ing among all health care stakeholders, including
Why California Needs Better Data Exchange: Challenges, Impacts, and Policy Options for a 21st Century Health System 3consumers and public and private payers, restricts
their ability to use information to make informed Real-Life Scenarios:
decisions or to design new programs that would
drive down cost while improving outcomes. Further, Challenges and Impacts
many of these sectors, especially social services, This report includes four real-life scenarios that high-
behavioral health services, and even public health light the shortcomings of the current HIE ecosystem,
departments, lack updated data infrastructure that its challenges and impacts on Californians, and direc-
enable electronic data capture and interoperability. tion on specific actions policymakers may consider to
address these issues.
3. Complex and onerous data exchange rules and
regulations. There are a range of restrictive, con-
fusing, and ambiguous state and federal laws and Disaster Response
rules that govern different types of data access and California continues to see a dramatic increase in
exchange. As a result, stakeholders are prevented natural and human-caused disasters that impact its
from using and maximizing the value of available residents. Recent wildfires are an especially salient
data. Worse yet, many elect not to participate in example, resulting in loss of life and the incalculable
data exchange, fearing liability and the conse- loss of land, homes, and personal property. Victims of
quences associated with not adhering to privacy disasters often find themselves evacuated to unfamiliar
regulations they don’t fully understand. environments and become heavily reliant on medical
and social services for care and basic necessities. HIE
These three core data exchange issues are evident is a critical tool to ensure that providers have access
every day when physical, behavioral health, and social to patients’ clinical records, enabling the providers to
service providers, public health, and emergency deliver safe and appropriate treatment.
response agencies seek to organize and deliver ser-
vices. To better appreciate how these issues directly As an illustrative example, a senior resident of
affect the lives of California’s residents, over a dozen Northern California is evacuated due to a wildfire that
interviews were conducted with leaders from state engulfs his home and destroys his community, includ-
and local agencies, payers, social, behavioral and clin- ing local businesses and the clinic where he receives
ical care providers, health care purchasers, emergency most of his care. He has a sore throat, headache, mild
response organizations, HIE providers, and other key chest pain, and difficulty breathing. He is evacuated
stakeholders. The purpose was to gain an under- by ambulance, where he’s treated for his symptoms
standing of how data exchange issues affect their and transported to an evacuation center in the next
ability to deliver critical services, and importantly, the county. The patient is slightly disoriented, emotion-
impact these issues have on the people they serve. ally distressed, and unable to communicate his other
This report summarizes the views represented through medical conditions, including asthma and chronic
these interviews, along with supporting research and heart disease, which are exacerbated by the inhaled
insights gained through a review of other state HIE smoke. Additionally, he is without his medications and
programs. can’t remember when he last took them. The emer-
gency responder doesn’t have access to the patient’s
electronic medical record because the emergency
medical services (EMS) medical record system is not
linked to the medical record at the patient’s clinic.
Once the patient arrives at the evacuation center,
additional treatment is provided, but the center also
doesn’t have access to his medical record. As a result,
the local provider is reliant on a disoriented patient to
California Health Care Foundation www.chcf.org 4provide critical information on his preexisting condi- requires access to their social services and behav-
tions and the type and dosing level of his medications. ioral health data so emergency responders can
The provider is uncertain about the severity of the make more informed decisions and get disaster
patient’s health condition and transfers the patient victims what they need.
to an overwhelmed local emergency department as
$ Complex and onerous data exchange rules and
a precaution. Upon arrival, the patient is diagnosed,
regulations. The issues of data access are com-
treated, and eventually transferred to temporary hous-
pounded by consent requirements that may
ing. If each provider had access to the patient’s clinical
prohibit data sharing, especially for patients unable
record, the patient would have received better care,
to provide written consent in an emergency.
avoided a costly and stressful emergency room visit,
and the burden on critical health care emergency
infrastructure during a natural disaster would have
been reduced. Pandemic Response and Public
Health Reporting
Each year, natural and human-caused disasters The pandemic elevated awareness of the importance
including wildfires displace hundreds of thousands of robust HIE to rapidly identify, track, and respond to
of California residents and cause billions of dollars in surges in COVID-19 cases and to mobilize resources
damage. In 2020 alone, California had five of the six to contain its spread and impact. Leaders need access
largest wildfires in the state’s history, with 6,500 square to timely testing information from labs, providers, and
miles burned. In the LNU and SCU Lightning Complex hospitals to identify new case clusters and to know
fires alone, an estimated 200,000 people were dis- where critical resources such as ICU beds and venti-
placed.2 As large-scale natural disasters increase in lators are. With this information, they can coordinate
frequency and severity, the need for HIE infrastructure responses with state and county public health agen-
that enables care providers to diagnose, treat, and cies and providers to better direct resources where
triage the victims becomes an even greater priority. they are most needed. Managing the rollout of state-
Factors limiting the effective use of HIE in support of wide testing, contact tracing, isolation support, and
disaster response include: vaccination programs similarly requires reliable and
timely information so that state, county, and health
$ Data fragmentation. While regional HIOs have
care delivery system leaders can organize and coordi-
been able to demonstrate the success of their
nate their pandemic response efforts.
service by compiling information for residents evac-
uated from the 2018 Camp Fire, the fragmented
As an illustrative example, a woman in Los Angeles
HIO landscape results in vast expanses of the state
County exhibits symptoms associated with the onset
not having critical HIO services, or where data are
of COVID-19, including a slight fever, fatigue, and
not shared between HIOs. These gaps in available
body aches. She contacts her primary care physician,
clinical data impact providers’ ability to properly
who directs her to get tested, self-quarantine, and
diagnose and treat patients, resulting in higher
continue to monitor her condition. The patient restricts
costs, inferior outcomes, and an increased burden
her activities but has to leave her apartment to get
on critical health system infrastructure.
food at a grocery store, her prescriptions at a phar-
$ Exclusion of exchange sectors. Most information macy, and a COVID-19 test. Within days she receives
exchange efforts today don’t capture and provide a positive test result and her condition declines, with a
access to important social services information or worsening fever, shortness of breath, and pressure in
link medical and behavioral health data with emer- her chest. At the advice of her physician, she calls for
gency response systems. Like the gaps in clinical an ambulance and is rushed to the nearest emergency
data, supporting the complete needs of people room. Although her conditions are considered severe,
displaced by natural or human-caused disasters all ICU beds are filled with other COVID-19 patients,
Why California Needs Better Data Exchange: Challenges, Impacts, and Policy Options for a 21st Century Health System 5and no ventilators are available. She is kept in the communities. And without a reliable means for public
emergency room for an extended period as her condi- health agencies to rapidly access social services infor-
tion deteriorates. Eventually, an ICU bed and ventilator mation to understand what services infected residents
are made available and her condition stabilizes, but were using, it was difficult to understand their basic
she is required to stay in the hospital for many days to needs and to mobilize services such as meal and med-
recover. Once she is stabilized, a public health investi- ication delivery to support them once quarantined.
gator contacts her and tries to reconstruct where she
had been and with whom she had been in proximity The inability for state and county leaders to access
during her contagious period. However, over a week reliable, real-time data also hinders the state’s vacci-
has passed so attempts to trace her interactions at nation strategy and its ability to identify and address
the grocery store and pharmacy are in vain. If public disparities in how COVID-19 response programs are
health officials and emergency responders had better implemented. The lack of real-time data exchange
information about hospital capacity, she could have between state and county agencies, health care pro-
been triaged to a hospital with more ICU and venti- viders, and mass vaccination sites is also restricting
lator capacity and received critical treatment sooner, the ability of state and local officials and providers to
and contact tracers could have had better information understand vaccine supply and demand needs and
to inform her employer of her positive COVID test so coordinate an immensely complex logistical challenge.
they could take immediate precautionary steps.
These challenges have had a disproportionate impact
In the early stages of the pandemic, the failure of the on racial and ethnic minorities — particularly Black,
California Reportable Disease Information Exchange Latinx, and Native American communities — that have
system (CalREDIE) — which was not designed to con- suffered from higher infection and mortality rates.3
sume data from HIOs or EHRs at the scale needed to Adequate HIE infrastructure would enable leaders
address a global pandemic — hampered the ability of to understand these disparities so they could better
state and local public health agencies and health sys- deploy resources to ensure that critical services, ven-
tem partners to understand and respond to regional tilators, and vaccines could be more efficiently and
COVID-19 case surges. It also highlighted a funda- equitably allocated.
mental disconnect between the state’s public health
and health care data systems; without accurate and California has experienced a myriad of challenges
timely disease surveillance information moving from associated with the COVID-19 crisis, including
the delivery system to CalREDIE, it was unclear where undercounting of COVID-19 cases that likely led poli-
ICU beds were available or how ventilators and other cymakers and health care providers to base decisions
supplies procured by public agencies should be on inaccurate information.4 Although it is difficult to
deployed to hospitals and clinics most impacted by calculate the entirety of the impact these gaps have
local surges. And without efficient, automated mecha- had on the care delivered to California’s residents,
nisms for hospitals to report admission, discharge, and with over 3.5 million documented COVID-19 cases
transfer alerts and ICU bed availability, overwhelmed and more than 50,000 deaths in the state at the time
facilities were required to hand tally and manually of this writing, the potential impact that the current
report capacity to local and state public health agen- fragmented data exchange model has had is substan-
cies. Similarly, the lack of reliable information exchange tial.5 The core underlying issues include:
infrastructure adversely impacted coordination across
public health, social service, and health care providers $ Exclusion of exchange sectors. CalREDIE and
in their implementation of contact tracing and isola- the California Immunization Registry (CAIR) sys-
tion support programs. Without timely test results, tems were not designed to connect, consume,
contact tracers couldn’t track down infected residents and incorporate health information from HIOs or
before they came into contact with others in their directly from EHRs at the scale needed to tackle
California Health Care Foundation www.chcf.org 6a global pandemic. As a result, critical informa- affordable housing. He receives most of his care
tion is not readily accessible, including timely from a mental health provider who helps manage his
tracking of new cases, hospital emergency depart- schizophrenia and maintains his record on a protected
ment and ICU bed capacity, data that would allow electronic charting system. His primary care provider
public health officials to identify disparities in how helps manage his blood sugar levels through medi-
the virus impacts different communities, or how cation and insulin therapy and maintains his physical
resources are being deployed. Without these data, health record in a separate EHR. Neither provider can
public health officials are challenged in organizing access the other’s records nor are they aware of the
their response to the crisis and don’t have a com- complete set of medications prescribed. When a new
plete picture of where to direct critical resources to schizophrenia treatment causes metabolic side effects
support overwhelmed local providers. Further, a that exacerbate his diabetes, the man is hospital-
lack of available social and behavioral health data ized and experiences serious complications including
restricts public health officials’ ability to identify and impaired vision and potential nerve damage. With his
address gaps in social and mental health supports. worsened medical condition, he is unable to retain
These are especially critical for those most in need, employment and is forced to seek supportive housing,
including underserved communities and residents but the housing support specialist doesn’t have access
seeking social services — among them food and to either his behavioral health or his physical health
housing — while self-isolating. records and underestimates his needs, slotting him in
a lower-priority tier for housing placement. Without a
$ Complex and onerous data exchange rules and coordinated care team supported by shared access to
regulation. Navigating complex data exchange his complete record, the man struggles to receive the
regulations and patient consent requirements can care he needs to regain stability and effectively manage
be difficult to obtain and manage, particularly dur- his health. If his mental health, primary care provider,
ing an emergency and a fast-paced pandemic, and housing support specialist had complete access
prohibiting sharing of certain types of information. to his records, they could have worked together and
made more informed decisions to address his social,
behavioral health, and clinical needs so he could man-
Serving Patients with age his co-occurring conditions and continue working
Complex Needs and living in a low-income housing unit.
Patients with serious medical and behavioral health
conditions and social needs are among the most Tragically, an estimated seven million people in
underresourced residents in California. They typically California have multiple chronic conditions and
receive care from networks of unaffiliated primary care, account for almost 60% of over $367 billion that the
specialty care, behavioral health, and social service state spends on health care; approximately 8%, or
providers, each of whom is providing services tailored 3.2 million, have substance use disorders; and 4% of
to aspects of the patient’s unique needs. To deliver California’s population, or 1.5 million people, have
the safest and most effective care, providers need to a serious mental illness.6 People with a serious and
coordinate care and have access to information from persistent mental illness and chronic disease have a
all the providers serving their patients. reduced life expectancy — sometimes on the order
of decades.7
As an illustrative example, a man being treated
for schizophrenia also has diabetes and a history of The current HIE ecosystem is not sufficient to support
chronic housing instability. His co-occurring condi- the effective management of patients with complex
tions have hampered his ability to remain employed, conditions. The core issues include:
and without consistent treatment to control those
conditions, he often finds himself losing access to
Why California Needs Better Data Exchange: Challenges, Impacts, and Policy Options for a 21st Century Health System 7$ Data fragmentation. Smaller safety-net providers and quality information can also empower consumers
often lack adequate infrastructure, such as a certi- to make more informed decisions regarding their care
fied EHR, that would allow them to participate in choices.
data exchange. Since the cost of participating can
be prohibitive for some, secure information sharing As an illustrative example, a woman is diagnosed
is often limited to larger health systems and clin- with early-stage glaucoma that can be treated by a
ics, resulting in a lack of coordination across the full moderate-risk surgical procedure. Her insurance plan
clinical care team. covers 80% of the cost for the procedure. The patient
receives a referral, but the surgeon she is referred to
$ Exclusion of exchange sectors. Behavioral health has a four-month wait, and she needs to have the
and social service providers also typically lack procedure done as soon as possible. She searches
adequate technology infrastructure, including online for other specialists in her area and identifies
EHRs that would allow them to participate in data several. Unable to differentiate them based on qual-
exchange. These providers often have limited ity and cost, and relying solely on consumer ratings,
resources and were ineligible to participate in prior she selects one with favorable reviews who is close
national programs including HITECH (based on the by and can schedule her quickly. After the proce-
Health Information Technology for Economic and dure is completed, her vision is mostly restored, but
Clinical Health Act), which incentivized the adop- within months she experiences vision distortions that
tion of certified EHR technologies. As a result, grow progressively worse. She requires a second sur-
current data exchange is mostly limited to the gery, but her insurance carrier is hesitant to pay for a
physical health record and does not include mental repeat procedure that should have been unnecessary.
health, substance use disorder (SUD), or social ser- After lengthy negotiations and appeals, they agree
vices information. to cover the service, but her copays and deductibles
far exceed her budget, and she is forced to establish
$ Complex and onerous data exchange rules and a multiyear payment plan difficult for her to afford.
regulations. Restrictive and often confusing federal With better information on quality, her insurance car-
and state data privacy policies regarding appropri- rier could have developed networks of providers with
ate use of patient information, including SUD data, demonstrably better outcomes, providing improved
often prevent access or create significant enough service to its customers and potentially lowering the
concerns about liability that providers elect not to cost of care. And if she had access to her own clinical
connect to or access information from other provid- information and a more complete picture of cost and
ers even when it is available through a national or quality information up front, she could have made a
regional HIO network. more informed decision resulting in a better outcome
and not leaving her with crippling debt.
Quality Reporting and California spent $367.5 billion on health care in
Value-Based Care 2016, representing approximately 14% of the state’s
Value-based care initiatives, including quality economy.9 Most of that spending has no correlation
improvement and price transparency programs, to outcomes; two-thirds of health care payments in
can significantly drive down costs and deliver bet- the US are not tied to quality of care or value.10 The
ter clinical outcomes.8 Data exchange can support impact to the state is significant. General fund spend-
these initiatives by providing payers and health care ing alone on Medi-Cal and CalPERS (California Public
purchasers with greater access to information nec- Employees’ Retirement System) in 2019 totaled
essary to assess and measure quality of care and to $101.7 billion and represented over 17% of the state’s
validate models that decrease unnecessary costs and general fund expenditures.11
improve outcomes. Improving access to clinical, cost,
California Health Care Foundation www.chcf.org 8Quality reporting and value-based care initiatives are care purchasers, and health plans generally don’t
often impeded by a lack of access to clinical outcomes have access to them. As a result, basic information
data that patients and payers including Medi-Cal, a consumer would need to make critical health care
CalPERS, and private insurance companies can under- decisions based on cost and quality is not made
stand and use. These challenges are primarily driven available. Health care purchasers and health plans
by the following issues: often must rely on administrative data from claims
rather than clinical data to understand outcomes.
$ Data fragmentation. Lacking access to clinical infor- Claims are useful to document prices paid for ser-
mation from all providers who deliver care, patients, vices or to indicate that an encounter took place,
payers, and purchasers have an incomplete health such as a vision screening or a glaucoma surgery,
record and can’t make fully informed decisions but they cannot be used to understand the out-
based on quality, outcomes, and costs. come of that visit or procedure. Without access to
clinical data, purchasers and health plans are lim-
$ Exclusion of exchange sectors. Regional HIOs and ited in their ability to detect and address disparities
national networks are primarily designed to share in outcomes, identify best practices, develop new
clinical data between providers. Consumers, health innovative payment models, organize and manage
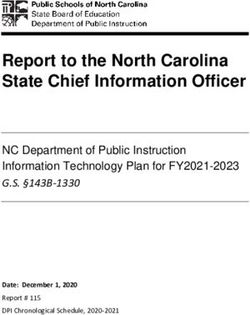
Table 1. Core Challenges to HIE in California Across Four Scenarios
PANDEMIC RESPONSE AND PUBLIC SERVING PATIENTS WITH QUALITY REPORTING AND
DISASTER RESPONSE HEALTH REPORTING COMPLEX NEEDS VALUE-BASED CARE
Clinical Data Inaccessible clinical data Lack of adequate Incomplete clinical data
Fragmentation from providers without infrastructure, includ- available to patients and
certified EHRs results in ing certified EHRs and payers to inform cost,
incomplete information funding for many safety- quality, and outcomes.
for displaced patients. net providers that
would allow them to
share data and help
coordinate care.
Exclusion of Emergency response CalREDIE and CAIR were not Behavioral health and Patients, payers, and
Exchange systems do not have designed to consume and social service providers purchasers lack access
Sectors access to electronic provide complete and real-time typically lack adequate to complete clinical
behavioral and social clinical data on the scale neces- technology, including data, limiting their
service data needed to sitated by COVID-19 response. EHRs, that would allow ability to identify high-
support displaced and them to participate in quality providers,
Behavioral health and social
affected residents. information exchange develop innovative
service data are not available
and to access physical payment models based
in real time, restricting public
health data. on clinical outcomes,
health and provider capabilities
and manage provider
to identify and address behav-
network quality.
ioral and social needs.
Complex and Navigating complex data exchange regulations and Lack of understanding
Onerous Data patient consent requirements can be difficult to obtain and liability concerns,
Exchange and manage, particularly during an emergency and a especially for organi-
Rules and fast-paced pandemic, prohibiting sharing of certain zations without the
Regulations types of information. capacity to interpret
state and federal law,
result in entities choos-
ing not to participate
in HIE or to access
information available to
HIOs or other providers.
Why California Needs Better Data Exchange: Challenges, Impacts, and Policy Options for a 21st Century Health System 9high-quality provider networks, or just understand laws, promulgated rules to encourage or require HIE,
fundamentally which providers they contract with established HIE contracting provisions in public pur-
deliver high-quality care. chasing programs, and directed state investment in
technology, services, and training. The following is a
Table 1 on page 9 summarizes the major challenges summary of challenges in California’s HIE ecosystem
and actors implicated in the four scenarios above. and actions policymakers could consider to address
them.
Align Leadership Across State
Key Actions for Purchasing, Regulatory, Health,
Consideration and Social Service Agencies
Health information exchange can provide criti- Beyond the three common problems of clinical data
cal capabilities to mobilize data so they’re available fragmentation, exclusion of exchange sectors, and
when residents are displaced by natural disasters. complex and onerous data exchange rules and regu-
The COVID-19 pandemic also demonstrated the lations, these scenarios also show that a wide range
need to build more robust information exchange of sectors and organizations need to participate
capabilities, enabling public health response to in HIE to provide “whole person” care. In order to
coordinate statewide testing, supports, and vaccine address these challenges across the scenarios, rule-
efforts. Comprehensive HIE that extends beyond the making authority and policy levers for financing and
exchange of physical health data is also needed to incentivizing participation must sit across many state
assemble a complete patient record, so a provider departments. Research into states with more robust
serving a person with complex needs can see all the HIE suggests that strong state leadership and a gov-
patient’s medical, behavioral, and social service infor- ernance structure empowered to align the various
mation and can develop care plans that take into policy, contracting, and financing levers at its disposal
account all the patient’s needs. And value-based pay- can significantly advance HIE.12
ment programs are dependent on clinical information
exchange to empower patients and purchasers to
$ Establish an office and advisory board within state
make better-informed decisions.
government charged with advancing HIE through
alignment of financing, contracting, and policy
Each of the scenarios described in this report evokes
levers across state agencies.
a complex set of HIE challenges, and highlights sig-
nificant gaps in California’s information exchange California could establish an office within state gov-
capabilities that have serious implications for resi- ernment charged with establishing the state’s vision,
dents, the providers who care for them, and the public goals, and priorities for advancing health informa-
and private agencies who cover and support them. tion exchange. The office could be endowed with
rulemaking authority that aligns regulatory, contract-
Interviews with numerous stakeholders and extensive ing, licensing, and financing levers available to state
research into other states’ HIE activities suggest that government agencies to advance HIE. It could also
comprehensive statewide HIE is best supported when be charged with developing recommendations to har-
a range of policy, contracting, and financing levers monize state law that conflicts with federal law. And
are used together to advance data exchange. States statute could direct the office to develop clear HIE
with more robust HIE have established strong leader- guidance and technical assistance to state agencies
ship structures within government to guide policy and and stakeholders, building upon existing efforts includ-
program actions, address HIE gaps, and overcome ing the State Health Information Guidance issued by
barriers. In most cases, these states have enacted new the California Health & Human Services Agency.13
California Health Care Foundation www.chcf.org 10The office’s authority could be crafted to be broad federal grant programs have supported some pro-
enough to direct health plans funded through pub- vider participation in HIE, but it has not been enough
licly purchased coverage programs (e.g., Medi-Cal, to encourage all hospitals and clinics to electronically
Covered California, CalPERS) and both health plans share health information. A combination of state man-
and providers licensed by the state to ensure consis- dates and provider HIE participation requirements in
tency in the implementation and enforcement of HIE public and private purchasing programs in Maryland,
rules the office enacts. The office’s authority could also New York, North Carolina, and others have been used
allow it to define consistent HIE contracting require- to advance HIE.
ments so that the purchasing power of state agency
procurements can be aligned to direct contractors
$ Establish statewide health information exchange
to consistently carry out state priorities. The author-
requirements, incentives, and penalties to encour-
ity could extend to health plan and provider licensing
age broad HIE participation by health plans and
agencies to help ensure HIE rules are enforced and
providers in health care, social service, emergency
followed by entities they oversee that provide cover-
response, and public health programs.
age and deliver services. And the office could guide
and help secure state and federal financing streams to Despite billions that have been spent to implement
fund HIE infrastructure, services, and training. certified EHRs through HITECH, many providers still
do not share information. The state could pass new
To get input from experts and affected stakehold- laws requiring hospitals, providers, and health plans
ers, the office could be guided by a multistakeholder to participate in HIE activities that meet specified
Health Information Exchange Advisory Board that state health care, public health, social service, and
brings together state and county agencies; physical, emergency response goals. Requirements could be
behavioral, and social service providers; consumers; designed by the new office with input from its advi-
and others with HIE expertise. The board could be sory board that align with and reinforce federal rules
charged with developing recommendations to the established under the 21st Century Cures Act and
office’s leadership regarding state HIE goals and strat- elsewhere.15 A number of other states have passed
egies, prioritizing information exchange initiatives and legislation or promulgated rules requiring participa-
programs, and offering input into how the state can tion in information-sharing activities and can serve as
effectively utilize policy, financing, and contracting examples to California.16
levers at its disposal. The board could also review and
provide feedback on the office’s recommendations States with more comprehensive HIE have used mul-
specifying where California health and safety codes tiple policy levers, like mandates with contracting and
could be updated to overcome information exchange financing levers, to stimulate participation in data-
barriers. sharing activities.17 To complement HIE participation
requirements in California, state purchasers including
the California Department of Health Care Services
Address Data Fragmentation (DHCS), Covered California, and CalPERS could
While millions of patient health records are shared establish contracting requirements with payer part-
electronically in California every day, significant gaps ners requiring their provider networks to participate in
in the state’s HIE ecosystem remain, especially in HIE activities that meet state policy goals. Those could
rural regions and underserved communities. Many be reinforced with incentive programs, including the
regional HIOs have emerged but still only serve a Medicare Merit-based Incentive Payment System and
fraction of the state; the nine largest regional HIOs Medicaid performance improvement programs that
support exchange in 35 of 58 counties in California, can leverage state and federal funding to encour-
representing approximately 22 million of the state’s 40 age HIE participation.18 They could also be coupled
million residents.14 HITECH incentives and state and with quality collaboratives, such as the Integrated
Why California Needs Better Data Exchange: Challenges, Impacts, and Policy Options for a 21st Century Health System 11Healthcare Association’s “Align. Measure. Perform.” use paper-based records. And while most hospitals,
program, or Blue Cross Blue Shield of Michigan’s providers, and specialists now have certified elec-
Collaborative Quality Initiatives.19 tronic health records (EHRs), many still don’t routinely
exchange information with other providers who care
Quality and value-based payment programs could for the same patients. As a result, critical physical,
leverage the Health Care Payments Data Program behavioral, and social service information remains
(HDP) of OSHPD (California Office of Statewide Health locked in siloes, inaccessible to the broader care team,
Planning and Development). The HDP will collect public health agencies, and emergency responders.
administrative health care data from health plans and California policymakers could establish financing pro-
other payers in California and support greater health grams to help providers implement robust information
care cost transparency to inform policy decisions technology to support the secure sharing of data with
regarding the provision of health care and to reduce other physical, behavioral, and social service provid-
health care costs and disparities.20 Ultimately, using the ers and public health agencies. And it could direct the
full complement of policy, financing, and contracting new office and its advisory board to identify financing
levers could help provide more complete information streams and align program requirements to maximize
to consumers — in alignment with new federal rules their impact.
requiring health plans to provide health information to
their members — to help them make more informed The state could model the program after the 2009
choices about providers and provide health plans with federal Health Information Technology for Economic
better information to develop value-based payment and Clinical Health (HITECH) Act that established
programs and high-quality networks.21 funding for primary care providers, specialists, and
hospitals to implement EHRs that can securely share
information.22 That program enabled the migration of
Address Exclusion of the industry’s antiquated paper-based clinical record-
Exchange Sectors keeping system to interoperable electronic health
Federal HITECH programs omitted thousands of records. No such program exists for a large segment
behavioral health and social service providers, leav- of behavioral health and social service providers. The
ing them without electronic recordkeeping systems state could leverage existing funding sources, such as
capable of sharing mental health, substance use, and the 2004 Mental Health Services Act, which funds a
social service information with other providers. Pilot broad continuum of service needs including improv-
programs including California’s Whole Person Care ing or replacing behavioral health provider technology
Section 1115 Medicaid waiver have demonstrated systems.23 California could also build upon and signifi-
that these providers can be supported through com- cantly scale up successful state programs, including
munity information exchange initiatives. But the CalHOP (California Health Information Exchange
demonstrations are temporary and insufficient on their Onboarding Program), which invested $5 million in
own to meet the needs of all providers that support California general fund resources and drew down $45
the complex needs and address disparities of millions million in federal funding to help providers connect to
of patients and families in California. HIOs.24
As DHCS establishes CalAIM (California Advancing
$ Establish financing programs that support state-
and Innovating Medi-Cal) program, it could con-
wide physical, behavioral, and social service data
sider ways to tap into Medicaid Enterprise System
exchange.
(MES) funding to leverage and reuse technology
Most behavioral health and social service providers that can advance HIE and expand programs, such as
don’t use information systems that can meet national Medi-Cal’s Section 1115 waiver Whole Person Care
data exchange standards, and many continue to demonstration that supported behavioral and social
California Health Care Foundation www.chcf.org 12service information exchange, including the successful
Overcome Complex and
Alameda County Community Health Record pro-
gram.25 Those efforts could be significantly reinforced
Onerous Data Exchange
with requirements that public payers, including DHCS Rules and Regulations
and CalPERS, Covered California, and state-licensed The four scenarios described above require access to
commercial health plans, expand HIE incentive some combination of physical and behavioral health
programs to include behavioral and social service pro- and social service data, which are subject to a large and
viders. All these efforts will require significantly more complex set of federal and state privacy laws, most of
state investment than has been made to date to fill which were not written with data exchange in mind.26
the significant information exchange gaps that exist Harmonizing state law with federal privacy and security
today. rules and providing more clarity about what is required
to support informed consumer consent could foster
greater participation in HIEs and lower legal barriers to
$ Upgrade California’s public health and emergency
accessing and using data available through HIE.
response information exchange infrastructure.
The pandemic laid bare the inadequacies of California’s
$ Harmonize state privacy rules and regulations with
public health information exchange infrastructure
federal law.
in responding to the pandemic. CalREDIE was not
designed to handle data on the scale necessitated by Many state laws were written before electronic data
COVID-19, and the California Immunization Registry sharing was even possible, making it difficult for orga-
(CAIR) was designed primarily to track childhood nizations to interpret and understand data-sharing
immunization records, not a statewide vaccination implications, including the threat of liability for violat-
campaign for all residents. The state’s ongoing experi- ing rules they may not be aware of. California could
ence with wildfires has also made clear the need to enact law based on recommendations made by the
expand state and local EMS data exchange infrastruc- new office and its advisory board to identify conflict-
ture. Policymakers could leverage federal funding from ing and ambiguous state health information privacy
the Centers for Disease Control and Prevention (CDC), and security rules, and update California health and
supplementing them with state resources to upgrade safety codes to harmonize them with federal law.
state and county surveillance, reporting, and emer-
gency response systems. Publicly funded purchasers
$ Establish statewide, universal consent policies.
could also incentivize providers to share patient infor-
mation with emergency response, public health, and The lack of a comprehensive and consistent state pri-
syndromic surveillance systems. Upgrading state and vacy and security framework and universal informed
county infrastructure and designing incentives for consent policies that supports physical, behavioral,
providers to send patient information including race, social service, and public health information sharing
ethnicity, and demographic data would provide county impedes data exchange. The byzantine privacy land-
and state leaders with data to identify outbreaks; moni- scape and lack of clear and consistent data-sharing
tor the efficacy of pandemic and emergency response; and consent policies result in institutions exhibiting
organize statewide programs to manage the spread of justifiable protectionist behaviors, short-circuiting
COVID-19, including vaccine distribution; and identify efforts to exchange vital information. New state law
and address disparities. Funding could include train- could direct the new office and its advisory board to
ing for public health agency staff and providers on the define requirements for a statewide universal informed
use of the required infrastructure to ensure a capable consent model and set of standard consent authoriza-
and well-equipped workforce. tion forms. And by applying contracting and licensing
levers at their disposal, state agencies can incentivize
Why California Needs Better Data Exchange: Challenges, Impacts, and Policy Options for a 21st Century Health System 13and require their use by contractors and licensed
entities. New law could also require participation in Conclusion
CTEN (California Trusted Exchange Network) to sup- To achieve the promise of health information
port exchange between California HIOs and national exchange, California needs bold leadership, a clear
networks, and adopt the California Data Use and vision, and measurable goals that guide policy and
Reciprocal Support Agreement (CalDURSA) as part of financing decisions and programs that enable com-
a broader set of data-sharing and consent policies.27 prehensive statewide data exchange. The scenarios
outlined in this report highlight the impacts that frag-
Establishing a universal statewide consent model mented HIE has on the lives of Californians and the
would reduce the legal burden and encourage HIE challenges providers face when serving them. To
participation by providing clarity and bright lines that address these challenges, California could enact a
describe allowed and prohibited HIE activities and new law that establishes an office within state govern-
data uses. ment with the authority to direct state agencies and
to use a variety of financing, contracting, and policy
levers to stimulate HIE infrastructure and programs.
But the state will need to provide enduring leadership
Health Insurance Portability and and financial support to incentivize the adoption and
Accountability Act use of technology that securely connects providers to
Physical health information exchange is subject each other. Whether it is to address the challenges
to the Health Insurance Portability and Account-
of managing a pandemic, responding to a natural or
ability Act (HIPAA), which envisions disclosures of
protected health information between “covered
human-caused disaster, supporting the needs of our
entities” that include health care providers and most underresourced residents, or helping advance
payers. Federal rules including 42 C.F.R. Part 2 and quality and value-based care for all Californians, the
state rules including the California Health & Safety time for strong state leadership to coordinate collab-
Code 11845.5 regulate certain forms of behav- orative efforts to overcome them is now. There has
ioral health data with narrower allowances for data
never been a better or more pressing time to act.
sharing that require more rigorous patient consent.
Homeless Management Information Systems (HMIS)
data is subject to the Housing 2004 HMIS Data and
Technical Standards, which permits disclosure of
data only among housing agencies.
California Health Care Foundation www.chcf.org 14Appendix. Interviewees
ORGANIZATION INTERVIEWEES
Alameda County Care Connect Jennifer Martinez, MPH, program development director
California Department of Public Health Scott Fujimoto, MD, public health medical officer
Daniel Daugherty, PhD, research scientist manager
Sandra Shewry, MPH, MSW, former acting director
California Emergency Medical Leslie Witten, MA, chief of the office of health information exchange
Services Authority
California Public Employees’ Heather Readhead, MD, MPH, medical director of clinical programs
Retirement System
Cedars-Sinai Darren Dworkin, senior vice president of enterprise information services and
chief information officer
Covered California Alice Chen, MD, MPH, chief medical officer
James DeBenedetti, director of plan management
Isaac Menashe, MPP, associate director, evaluation & research
Margareta Brandt, MPH, manager of quality improvement
Integrated Healthcare Association Jeff Rideout, MD, president & chief executive officer
Northeast Valley Health Corporation Stephen Gutierrez, chief information officer
QueensCare Health Centers Arnel Mendoza, director of information systems
SacValley MedShare Elizabeth Steffen, MBA, executive director
Sierra Vista Hospital Mike Zauner, MBA, chief executive officer
Why California Needs Better Data Exchange: Challenges, Impacts, and Policy Options for a 21st Century Health System 15Endnotes
1. “Certified EHR Technology,” Centers for Medicare & 10. “APM Measurement Effort,” Health Care Payment Learning
Medicaid Services (CMS), last modified December 21, 2020. & Action Network, n.d.; Sorensen, Nonzee, and Kominski,
Public Funds; and “Regional Data: GDP and Personal
2. “2020 Incident Archive,” Cal Fire, n.d.; and “California
Income,” Bureau of Economic Analysis, n.d.
Wildfires: Urban Expansion and the Risk of Displacement”
(PDF), in 2019 Global Report on Internal Displacement, Internal 11. Medi-Cal Explained: The Medi-Cal Budget Process Fact
Displacement Monitoring Centre, May 2019. Sheet, CHCF, February 2019; and “The 2019‑20 Budget:
California Spending Plan — Debt and Liabilities,” Legislative
3. Don Bambino Geno Tai et al., “The Disproportionate Impact
Analyst’s Office, October 17, 2019.
of COVID-19 on Racial and Ethnic Minorities in the United
States,” Clinical Infectious Diseases 72, no. 4 (Feb. 15, 2021): 12. Jonah P. B. Frohlich, Kier A. Wallis, and Jonathan DiBello,
703–6, doi:10.1093/cid/ciaa815. Expanding Payer and Provider Participation in Data
Exchange: Options for California, CHCF, November 2019;
4. “State’s COVID Data Flawed; Technical Issue Cited,”
and Sandeep Kapoor, JoAnne Hawkins, and Dawn R.
Techwire, August 4, 2020.
Gallagher, Designing a Statewide Health Data Network:
5. “Tracking COVID-19 in California,” California All, last What California Can Learn from Other States, CHCF,
updated February 24, 2021. February 2021.
6. Paul M. Brown, Mariaelena Gonzalez, and Ritem Sandhu 13. “State Health Information Guidance (SHIG),” California
Dhaul, “Cost of Chronic Disease in California: Estimates at Health & Human Services Agency, n.d.
the County Level” (PDF), Journal of Public Health Management
14. Walter Sujansky, Promise and Pitfalls: A Look at California’s
Practice 21, no. 1 (2015): E10–E19; Andrea Sorensen, Narissa
Regional Health Information Organizations, CHCF,
J. Nonzee, and Gerald F. Kominski, Public Funds Account
January 2019.
for Over 70 Percent of Health Care Spending in California
(PDF), UCLA Center for Health Policy Research, August 2016; 15. “21st Century Cures Act: Interoperability, Information
Gerard F. Anderson and Katherine B. Wilson, Chronic Disease Blocking, and the ONC Health IT Certification Program,”
in California: Facts and Figures, California Health Care 85 Fed. Reg. 25642 (May 1, 2020).
Foundation (CHCF), October 2006; Wendy Holt, Substance
16. “State Health IT Policy Levers Compendium,” Office of the
Use in California: A Look at Addiction and Treatment, CHCF,
Coordinator for Health Information Technology (ONC); and
October 2018; and Behavioral Health Barometer: California,
”Article 29B: Statewide Health Information Exchange Act,”
Volume 5: Indicators as Measured Through the 2017 National
N.C. Gen. Stat. §§ 90.414.1–12 (2015).
Survey on Drug Use and Health and the National Survey of
Substance Abuse Treatment Services (PDF), Substance Abuse 17. Expanding Payer and Provider Participation in Data
and Mental Health Services Administration, 2019. Exchange: Options for California, CHCF, November 2019;
and Brittany L. Brown-Podgorski et al., “The Association
7. Eva H. DuGoff et al., “Multiple Chronic Conditions and Life
Between State-Level Health Information Exchange Laws
Expectancy: A Life Table Analysis,” Medical Care 52, no. 8
and Hospital Participation in Community Health Information
(Aug. 2014): 688–94, doi:10.1097/MLR.0000000000000166;
Organizations,” AMIA Annual Symposium Proceedings
and Promoting Chronic Disease Management: A Guide for
Archive (Dec. 5, 2018): 313–20.
Behavioral Health Care Teams (PDF), University of Washington,
n.d. 18. “Participation Options Overview,” CMS, n.d.; and 42 C.F.R.
438.6(b)(2).
8. Rajender Agarwal et al., “The Impact of Bundled Payment
on Health Care Spending, Utilization, and Quality: A 19. “Align. Measure. Perform.,” Integrated Healthcare Assn.,
Systemic Review,” Health Affairs 39, no. 1 (Jan. 2020): n.d.; and “Collaborative Quality Initiatives,” Blue Cross Blue
50–57, doi:10.1377/hlthaff.2019.00784; Zirui Song et al., Shield of Michigan, n.d.
“The ‘Alternative Quality Contract,’ Based on a Global
Budget, Lowered Medical Spending and Improved Quality,” 20. “Health Care Payments Data Program,” Office of Statewide
Health Affairs 31, no. 8 (Aug. 2012): 1885–94, doi:10.1377/ Health Planning and Development, n.d.
hlthaff.2012.0327; and F. P. Vlaanderen et al., “Design and 21. See the Interoperability and Patient Access Final Rule,
Effects of Outcome-Based Payment Models in Healthcare: A 85 Fed. Reg. 25510 (May 1, 2020).
Systemic Review,” European Journal of Health Economics 20
(2019): 217–32, doi.org:10.1007/s10198-018-0989-8. 22. 2018 Report to Congress: Annual Update on the Adoption of
a Nationwide System for the Electronic Use and Exchange of
9. Sorensen, Nonzee, and Kominski, Public Funds. Health Information (PDF), ONC, n.d.; and Medicaid Incentive
Payments (PDF), CMS, October 2018.
California Health Care Foundation www.chcf.org 16You can also read