Oral Cholera Vaccine stockpile for cholera emergency response
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Oral Cholera Vaccine stockpile for cholera emergency response ICG 9/16/2013
Table of Contents
1. Background ...................................................................................................................................... 2
1.1. Global burden of cholera ......................................................................................................... 2
1.2. World Assembly resolution and WHO technical consultations ............................................... 2
2. Characteristics of currently prequalified OCV ................................................................................. 3
2.1. General information................................................................................................................. 3
2.2. Key features and performance of WHO pre-qualified oral cholera vaccines .......................... 4
3. When to consider the use of OCV? WHO position paper ............................................................... 6
3.1. Vaccination and cholera control .............................................................................................. 6
3.2. Control of endemic cholera ..................................................................................................... 6
3.3. Control of cholera outbreaks ................................................................................................... 7
3.4. Surveillance .............................................................................................................................. 9
4. Previous experience on OCV in mass vaccination campaigns ....................................................... 10
5. Stockpile mechanism overview ..................................................................................................... 16
5.1. Objectives of OCV stockpile ................................................................................................... 16
5.2. Use of the stockpile................................................................................................................ 17
5.3. Management and governance of the OCV stockpile for emergency response7 .................... 17
5.4. Application procedure to OCV in IGC stockpile ..................................................................... 18
5.5. Decision criteria for the release of OCV. ................................................................................ 20
5.6. Monitoring and evaluation of the OCV stockpile................................................................... 23
6. References: .................................................................................................................................... 24
1Background
Global burden of cholera
The real global burden of cholera is unknown. In cholera endemic countries, an estimated 1.4 billion
people are at risk of cholera each year1 and 2.8 million cholera cases (uncertainty range: 1.4–4.3) and 91
000 cholera deaths (uncertainty range 28,000 to 142,000) occur every year. Another 87 000 cases and
2500 deaths are expected in non-endemic countries annually.1
Slow progress in providing access to safe water and sanitation to underserved populations, limitations of
surveillance systems for early detection of cholera outbreaks, and lack of access to timely and appropriate
healthcare have contributed to this burden of disease.Other factors contributing to make cholera a public
health priority are the emergence in 1992 of new strains of V. cholerae more virulent and causing more
severe clinical manifestations2, the increased antimicrobial resistance, climate change and rapid and
unplanned urbanization.3Children under five bear the greatest burden of cholera and account for about
half of the estimated cholera deaths.4
Effective cholera prevention and treatment regimens are well established, yet cholera remains poorly
controlled in both outbreak and endemic contexts.
In recent years two large national cholera epidemics in Zimbabwe and Haiti, which resulted in thousands
of cases and deaths, focused the world’s attention on the need not only to control endemic disease but also
to put in place improved epidemic cholera preparedness and response measures.
World Assembly resolution and WHO technical consultations
Recognizing the importance of cholera as a continuing public health problem, the World Health
Assembly adopted Resolution 64.15 in May 2011.5 This resolution calls for implementation of an
integrated and comprehensive approach to cholera control, which may include the use of oral cholera
vaccines (OCV) “where appropriate, in conjunction with other recommended prevention and control
methods and not as a substitute for such methods.”
In September 2011, the World Health Organization (WHO) Secretariat organized a technical consultation
which recommended the creation of an OCV stockpile for outbreak control.6
In April 2012, the WHO convened a Technical Working Group (WG) to address the creation of an oral
cholera vaccine stockpile and to develop the implementation framework.
2The WG agreed that the focus would be specifically to respond to outbreaks, as a means to complement
but not replace existing guidance on other critical cholera outbreak prevention and control measures.7
Characteristics of currently prequalified OCV
General information
For the creation of an immediate stockpile, two OCVs are currently prequalified by WHO: Dukoral® and
Shanchol™. There is no known comparison of the two vaccines up to now. Their key attributes are
briefly outlined below and summarized in table 1.
Overall, both WHO pre-qualified are oral killed whole-cell vaccines (WC) that provide sustained
protection of >50% for at least two years in endemic populations8-10 induce an immune response relatively
quickly (7-10 days after the 2nd dose) and have a good safety profile.11 Shanchol™ has demonstrated
longer term protection in children less than six years of age, as compared to Dukoral,® and therefore does
not require booster dose after six months in this age group, as does Dukoral®.12 On the other hand,
Dukoral® has been shown to provide better short-term protection against cholera, particularly among
children 2-5 years old and also confers significant short-term protection against ETEC.
In terms of logistics and handling, both vaccines have a two-dose regimen between 1 and 6 weeks apart.
(3 doses for Dukoral in children aged 2–5 years) and require a cold chain.
3Key features and performance of WHO pre-qualified oral cholera vaccines
Table 1.Characteristics of WHO pre-qualified oral cholera vaccines.
Characteristics Oral cholera vaccines
Trade name Dukoral® Shanchol™
Type of vaccine Killed whole cell vaccine V.cholerae Killed bivalent (O1 and O139
O1 serogroup + recombinant B serogroups ) whole-cell vaccine
subunit of cholera toxin (WC/rBS) suspension. (BivWC)
Presentation (or 3 ml single dose vials and 5.6 g of 1.5ml single dose vials (in 3 ml glass
packaging) effervescent granules of sodium vial with aluminium cap)
bicarbonate buffer in a sachet
Age From 2 years of age From 1 year of age
Administration - Adults and children 6 years and - 2 doses given orally 2 weeks apart.
course or (Dosing) older: 2 doses given orally 1-6 - A period of +3 days is accepted for
weeks apart. - Booster dose after 2 second dose.
years.
- No official recommendation on
- Children 2-5 years: booster yet.
3 doses given orally 1-6 weeks
apart. Booster dose after 6
months.
- Fasting required 1 hour before
and after vaccination.
4Buffer Dilution in 150ml of water (75ml - No buffer needed
for children 2-5 years) mixed with
- Water may be offered following
buffer
ingestion of the vaccine, but is not
required.
Protection/efficacy Earliest onset of protection 7 days - Earliest onset of protection 7-10
after 2nd dose. days after 2nd dose.
- 67% protection for at least 2 years
in all ages
Adverse effects -No major adverse effects - No major adverse effects reported.
/contraindications reported. - Currently not recommended in
pregnancy (limited data )
-Currently not recommended for
- Currently not recommended in
use in pregnancy (no specific
HIV/AIDS or other immuno-
studies performed) compromised states (No clinical data)
-Administration may be considered - Administration may be considered
after benefit- risk evaluation. after benefit- risk evaluation.
-Can be given to HIV-infected
persons.
Shelf life, storage - 3 year shelf life at 2-8° C. - 30 months shelf life at 2-8° C
and cold chain - Do not freeze
- Stable for 1 month at 37 ° C . 2
weeks at < 27 ° C - VVM of type 14.
- Do not freeze - Stable for 14 days at 37oC
- Packed volume per dose in 35-dose
- No VVM.
pack:16.8cm3 (140 mm x105 mm x40
- Packed volume per dose: 136cm3 mm)
(in 2-dose pack; also available in
single and 20-dose pack)
Manufacturer Crucell, (Sweden) Shantha Biotechnics, (Hyderabad,
India) Sanofi Company
5Current production 2 million doses per year 2 million doses per year
capacity (2012)
Countries licensed Licensed in 60 countries India, Nepal, Malaysia, Philippines,
(June 2013) Ivory Coast
Year first licensed 1991 2009
Date of WHO 25 Oct 2001 29 Sep 2011
prequalification
Estimated prices per ~ $ 4.7-9.4 per dose $1.85
dose (2013)
When to consider the use of OCV? WHO position paper 24
Vaccination and cholera control
Cholera control should be a priority in areas where the disease is endemic.
Given the availability of 2 oral cholera vaccines and data on their efficacy, field effectiveness, feasibility
and acceptance in cholera-affected populations, immunization with these vaccines should be used in
conjunction with other prevention and control strategies in areas where the disease is endemic and should
be considered in areas at risk for outbreaks.
Vaccination should not disrupt the provision of other high-priority health interventions to control or
prevent cholera outbreaks. Vaccines provide a short-term effect that can be implemented to bring about an
immediate response while the longer term interventions of improving water and sanitation, which involve
large investments, are put into place.
Although all age groups are vulnerable to cholera, where resources are limited immunization should be
targeted at high-risk children aged ≥1 year (Shanchol™ or mORCVAX) or ≥2 years (Dukoral®). (For
vaccine schedules and administration, see recommendations made by the manufacturers).
Control of endemic cholera
The following definition for endemic cholera has been suggested: “the occurrence of faecal culture-
confirmed cholera diarrhoea in a population in at least 3 of the past 5 years”. 25 Even in endemic settings
there may be surges in cholera incidence for which intensive public health interventions are required.
While such surges might be termed endemic, in public health terms they are often treated as epidemic
cholera.
6In cholera-endemic countries, vaccinating the entire population is not warranted. Rather, vaccination
should be targeted at high-risk areas and population groups.
The primary targets for cholera vaccination in many endemic areas are preschool-aged and school-aged
children.
Other groups that are especially vulnerable to severe disease and for which the vaccines are not
contraindicated may also be targeted, such as pregnant women and HIV-infected individuals. Countries
should also consider vaccinating older age groups if funding is available.
Periodic mass vaccination campaigns are probably the most practical option for delivering cholera
vaccines.
Schools, health-care facilities, religious institutions and other community settings may be appropriate
venues for vaccination campaigns. Incorporating cholera vaccination into routine vaccination schedules
may be an alternative or complementary strategy to mass vaccination campaigns, for example to reach
young children between campaigns.
Since the documented duration of significant protection for the oral cholera vaccine is 2 years, it is
recommended that initial vaccination with 2 doses be followed by a booster dose every second year. Once
data on the longer-term efficacy of any oral cholera vaccine become available, the recommended interval
between initial and booster vaccination may be extended.
Control of cholera outbreaks
The mainstays of control measures to be implemented during ongoing epidemics should remain (i)
providing appropriate treatment to people with cholera, (ii) implementing interventions to improve water
and sanitation and (iii) mobilizing communities.
Pre-emptive vaccination should be considered by local health authorities to help prevent potential
outbreaks or the spread of current outbreaks to new areas. Finalizing of predictive risk-assessment tools to
help countries determine when pre-emptive cholera vaccination might be used is needed urgently; these
tools should be made available and field-tested as soon as possible.
Given the recent large and prolonged outbreaks of cholera (for example, in Angola and Zimbabwe),
reactive vaccination could be considered by local health authorities as an additional control measure,
depending on the local infrastructure and following a thorough investigation of the current and historical
epidemiological situation, and clear identification of geographical areas to be targeted.
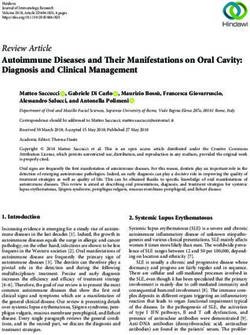
The 3-step decision-making tool developed for crisis situations26 should guide health authorities in their
decisions on whether or not to use cholera vaccine during complex emergencies:
78
Fig 1 Decision-making tree for Oral cholera vaccine use in complex emergencies.26
Source: Oral cholera vaccine use in complex emergencies: what next? WHO Meeting Report 2005
http://www.who.int/cholera/publications/cholera_vaccines_emergencies_2005.pdf
Considering the lack of experience with implementing reactive vaccination against cholera, the feasibility
and impact of vaccination in halting ongoing outbreaks should be documented and widely disseminated.
Vaccination should cover as many people as possible who are eligible to receive the vaccine (for
example, children aged ≥1 years or ≥2 years, depending on the vaccine), and should be conducted as
quickly as possible.
Surveillance
It is strongly recommended that surveillance for microbiologically confirmed cases of cholera be
instituted and integrated into already existing surveillance systems or networks to measure the burden of
disease and monitor the seasonality and the impact of vaccination and other interventions in high-risk
populations.
9Previous experience of OCV use in mass vaccination campaigns
(Excluding randomized clinical trials)
Mass vaccination campaigns using oral cholera vaccines have been documented on 12 occasions over the
last 15 years, either pre-emptively in endemic settings (n=3) or in post-crisis situations (n=4), or
reactively as part of the response to a cholera outbreak (n=5). Vaccine effectiveness observed after
vaccination campaigns was between 78% and 84% after the second dose at 5-6 months
In cholera endemic settings, Vietnam has included an OCV component in its strategy to control cholera
since 1998 and has by far the largest experience of using OCVs as a public health tool. Zanzibar took a
similar decision in 2012 after piloting the project on a small scale. The other pre-emptive uses of OCVs
that have been documented so far were essentially demonstration or pilot projects aimed at testing the
feasibility of mass campaigns (Mozambique). When used in the context of complex emergencies, no
cholera outbreak was reported following pre-emptive vaccination campaigns.
Reactive mass vaccination campaigns with OCVs in response to outbreaks have been organized up to 1
year after the report of the first cases of cholera. Although their impact remains difficult to evaluate for
the time being, vaccine effectiveness was high when evaluated and cholera cases were absent or
decreased in most vaccinated areas. Where reported, acceptance of OCVs by the communities targeted for
vaccination was good, in both endemic and epidemic settings. The most commonly reported constraints
are logistic and mention the important volume of the vaccines and the corresponding cold room storage
capacities, and the handling of buffer / water during delivery. With 2 exceptions, reported from very
specific contexts, the cost of delivery varies between $0.5 and $2.5 per fully immunized person.
Cost effectiveness studies were conducted in several endemic countries and concluded that cholera
vaccination would be “cost effective” particularly when targeting children27 or when herd protection is
taken into account.28
10Table 2 Historical summary of mass vaccination campaigns using oral cholera vaccines (excluding randomized clinical trials)
Location/dates Situation Target Vaccine No. persons Vaccine Costs per fully Vaccine effectiveness
population used vaccinated coverage immunized (VE) and potential impact
Pre-emptive mass vaccination campaigns in endemic settings
Vietnam (1998 Endemic area. Children 1-15 ORC-Vax® >20 million From 75% to Vaccine VE of 50% at 3 to 5 years
29,30
to present) Yearly years old, and doses 95%, for 2 price/dose: $0.4
Vietnamese
campaigns used residents of all delivered doses
killed OCV
pre-emptively ages during depending on
before the peak floods years and
cholera season to place
control endemic
cholera in high-
risk areas and
also used pre-
emptively during
floods
11Location/dates Situation Target Vaccine No. persons Vaccine Costs per fully Vaccine effectiveness
population used vaccinated coverage immunized (VE) and potential impact
Beira, Endemic area >2 years old Dukoral® > 98,000 54% fully $2.1per fully VE between 78% and 84%
Mozambique with frequent residents doses immunized in immunized for two doses over a five-
31,32
(2003/04) outbreaks (n=19,550) delivered targeted area (vaccine month period
53,700 shipment and
Campaign before Non-pregnant
received 1 delivery).
rainy season.
dose; 44,000 Vaccine
received 2 donated
doses
(including
many outside
the targeted
area)
Zanzibar Endemic area >2 years old Dukoral® 23,921 50% fully $25.3 per fully VE of 79% 15 months after
(2009) 33-35 with frequent among 48,178 persons immunized immunized the campaign for recipients
outbreaks inhabitants received 2 ($20.0 for the of 2 doses
Non-pregnant doses vaccines + $5.3 Evidence of herd protection
for delivery)
Pre-emptive use in post-crisis situations
Uganda Stable refugee Around 44,000 Dukoral® >35,000 for 83% for 1st $0.53 per fully No cases reported from the
(1997)36,37 setting refugees in 6 1st dose; dose; 76% for immunized for vaccinated settlements
12Location/dates Situation Target Vaccine No. persons Vaccine Costs per fully Vaccine effectiveness
population used vaccinated coverage immunized (VE) and potential impact
camps 27,600 for 2nd 2nd dose delivery. during a cholera outbreak
dose Vaccine in the district one year after
donated the campaign
Darfur, Sudan Stable refugee >2 years old Dukoral® 47,302 IDPs 87% fully $7.1 per fully N/A
38,26
(2004) setting among >53,000 received 2 immunized immunized,
No outbreak reported
IDPs in 2 doses including $0.7
camps for delivery
Aceh, Indonesia Complex ≈79,000 IDPs Dukoral® 54,627 69% fully $17.6 per fully N/A
(2005) 38,39 emergency living in camps received 2 immunized immunized,
No outbreak reported
following in 3 areas doses including $8.2
tsunami for delivery
Haiti (2012)40 Post-earthquake ≈70,000 Shanchol™ 41,193 76.7% and $3.33 per dose N/A
and nationwide residents of 2 received 2 62.4% fully administered
cholera outbreak rural areas > 1 doses immunized including $2.13
year old. for vaccine and
$1.20 for
delivery
Reactive campaigns during cholera outbreaks
Micronesia Ongoing > 2 years old Orochol® N/A 47% of target $1.23 per VE of 79%
13Location/dates Situation Target Vaccine No. persons Vaccine Costs per fully Vaccine effectiveness
population used vaccinated coverage immunized (VE) and potential impact
(2000)41 outbreak on the among 34,486 single-dose population person Decrease of cholera attack
island since 5 residents non- live- vaccinated for rate
months pregnant attenuated delivery Not spread to surrounding
CVD 103- islands
HgR vaccine
(not
marketed
anymore)
Mayotte Ongoing >2 years old Dukoral® 93,000 64% 26.9€ per Only sporadic cases
42-44
(2000) outbreak in the among 175,000 persons person reported after the campaign
archipelago residents and vaccinated vaccinated (all
since 1 year illegal migrants included), i.e.
Sporadic cases about $24.5 in
on the island 2000
since 9 months
Marshall islands Ongoing Vulnerable Orochol® N/A 32% total N/A Outbreak ended during the
(2000)45 outbreak on the groups among population month following the
island since < 1 9345 campaign and did not
month inhabitants spread to surrounding
islands
14Location/dates Situation Target Vaccine No. persons Vaccine Costs per fully Vaccine effectiveness
population used vaccinated coverage immunized (VE) and potential impact
Hanoi, Vietnam Ongoing 462,570 ORC-Vax® N/A 80% for at N/A VE of 76% for at least one
46
(2008) outbreak in an residents of 2 least one dose dose 3 to 4 months after the
Vietnamese
urban setting hard hit districts campaign.
killed OCV
since 3 months age >=10 years, New wave of the outbreak
non-pregnant reported 3 months after the
campaign
Guinea Conakry Ongoing >1 year old Shanchol® 172,544 for 76% fully $7.4 per fully VE of 84% for 2 doses
(2012) 47 outbreak in a among 1st dose, immunized, immunized 6 months after vaccination
Controlled
rural setting ≈200,000 143,706 for >90% with at ($4.9 for the (Data analysis ongoing
Temperature
since 3 months residents of 2 2nd dose least one dose vaccines + $2.5 Luquero F)
Chain (CTC)
rural districts. for airfreight
strategy was Cases remained low in
Non-pregnant and delivery
used on the vaccinated districts during
day of Cost per dose of rainy season compared to
vaccination. vaccine other parts of Guinea
delivered $2.89
incluisng £1.85
for the vaccine
and $1 for
direct costs
15Stockpile mechanism overview
The OCV stockpile has been created on the principle that vaccines have a role in the prevention and
control of cholera outbreaks when used in conjunction with accessible healthcare and improvements in
water and sanitation. It has also been established with the understanding that the stockpile will have a
limited number of doses relative to the need for vaccine and that the use of OCV through the stockpile
will not significantly alter global cholera disease trends. However, evidence generated through
stockpile OCV use may help indicate the vaccine’s potential to control outbreaks and to impact
disease trends when used on a larger scale.
Given the limited global supply of licensed, WHO-prequalified cholera vaccines, a global stockpile is
likely to improve the timely access of OCV for countries that may benefit from its use. Moreover,
increased OCV use may lead to a larger global vaccine supply through more consistent and predictable
demand for vaccine.
Objectives of OCV stockpile
The use of the vaccine in emergency response situations is expected to help reduce cholera morbidity
and mortality in epidemic situations and alleviate the disease burden on at-risk populations.
While vaccines provide a short-term effect as an immediate intervention to a potential cholera
outbreak, expanding access to improved drinking-water sources and sanitation constitutes a longer-
term solution for most waterborne diseases, including cholera.
The use of OCV from the stockpile should not detract attention from the key established responses to
cholera outbreaks, which are: detection, diagnosis, and treatment of cases with oral rehydration and
antibiotic treatment; establishment of a safe water supply; and implementation of adequate waste
disposal and sanitation.
The main objective of the OCV stockpile is to ensure the timely and targeted deployment of
OCV such that vaccine can be used as an effective outbreak response where it is most needed.
16Use of the stockpile
The main use of this stockpile will be for outbreak response, either in the form of reactive
campaigns in areas experiencing an active outbreak or pre-emptive vaccination campaigns
among populations at elevated risk for cholera due to outbreaks in adjacent areas or at
heightened vulnerability due to humanitarian crisis.
Reactive vaccination occurs after the start of an outbreak and aims to limit the extent of the outbreak
in communities at imminent risk (i.e., neighbouring communities - across borders, or linked by river
systems or water and sanitation systems), provided the local infrastructure allows it, and an in-depth
analysis of past cholera data and identification of a defined target area have been performed.48,49
“An outbreak of cholera at the national level commonly consists of a succession of several outbreaks
as it spreads through the country or across borders. Vaccinating communities in areas at imminent risk
during such a succession would have greater impact than in areas where the transmission has already
been active for several weeks or months. Many of the individuals in a community where there is active
transmission may have already been infected with cholera even if they are asymptomatic. In fact, an
estimated 80 per cent of infected individuals will be asymptomatic but still shed the bacteria. This
reactive strategy is particularly important in areas where response mechanisms cannot deliver typical
cholera control measures” 49
Pre-emptive vaccination of populations takes place before likely upsurges in cholera transmission or
outbreaks. It may be considered, based on risk assessment and epidemiological data, to limit the spread
of outbreaks to new areas at risk.
Ideally pre-emptive and reactive vaccination, during an outbreak response, should cover as many
people as possible who are eligible, and should occur as quickly as possible.
Management and governance of the OCV stockpile for emergency response7
The International Coordinating Group (ICG) comprising Médecins Sans Frontières (MSF), the
International Federation of Red Cross and Red Crescent Societies (IFRC), the United Nations
Children’s Fund (UNICEF), and WHO will be the decision-making body for deployment of OCV
through the stockpile. This group also coordinates vaccine release from the international Yellow Fever
and Meningococcal vaccine stockpiles.
17Additional expertise and technical advice might be sought on a case-by-case base from a range of
partners. A meeting with participation of key stakeholders is organized annually.
The ICG manages the global stock, liaison with manufacturers and ensures that emergency supplies
are available at the global level. The ICG decision-making body uses, and promotes the need for,
epidemiological and operational criteria for vaccine release. Standard operating procedures are
followed, which are transparent and allow lessons to be learned and activities to be improved. The
ICG mechanism has also contributed to reinforce surveillance and laboratory confirmation since
countries must demonstrate an ongoing epidemic to access the ICG stockpile.
The OCV stockpile initially comprises two million doses of vaccine per year for an initial period of 2-
3 years (2013 – 2015). Start-up funding for the stockpile will be provided by donors. A revolving fund
will be established as with other ICG stockpiles, to assure longer-term financial stability.
Collected funds will support the procurement of vaccine, country preparedness and planned
operational costs for the use of the OCV stockpile vaccination campaign and evaluation of the
stockpile mechanism initial period of 3 years.
After an intermediate evaluation, an extension could be made up to 5 years with additional
investments and/or with funds generated through the revolving fund mechanism.
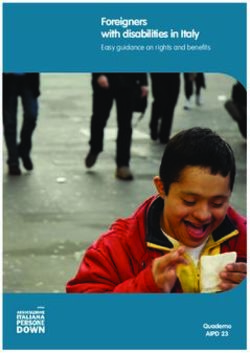
Application procedure to OCV in IGC stockpile
Vaccine requests may be made by any national or international organization, and the ICG will provide
a decision of approval or denial of vaccine release within 48 hours of request receipt, depending on
whether additional information is required. Vaccine and supplies then will be deployed if approved
(Fig 2).
The minimum situational requirements for a request to be considered are:
The reporting of a culture-confirmed cholera outbreak (with consideration for the number of
specimens collected, type of strain, and laboratory capacity) in any given area. Diagnosis of
cholera is confirmed by isolating V. cholerae O1 or O139 from faeces through laboratory testing.
To ensure the quality of samples, Cary Blair transport medium should be used for transport and
storage of rectal swabs.
18 An OCV campaign has NOT been conducted in the previous 2 years in the same area (with
consideration for the quality of the campaign, the vaccine coverage, and any population
movements).
19Figure 2- Request process and roles of ICG and partners
Decision criteria for the release of OCV
Once an outbreak of cholera has been laboratory confirmed in a given area, a number of indicators
may be considered to estimate the projected severity of the cholera outbreak and the potential
impact of the vaccination campaign.
Severity is, in this context, defined by the anticipated morbidity, mortality and the likelihood
of spread of cholera from an affected area to a non-affected area.
The impact of vaccination would depend on: (table 3)
o Susceptibility of the population, i.e. the level of herd immunity that may have been
conferred by earlier exposure to cholera (i.e. from previous outbreaks or from
endemic situations) or by vaccination in a particular population.
o Vulnerability of the population, i.e., behavioural, social, and environmental factors
likely to impact on the risk of acquiring infection and engaging in risk minimization
20(e.g. mobility; health-seeking behaviours; hygienic practices; and access to safer food,
water, and sanitation).
o Risk of spatial extension, i.e. the projected likelihood of geographic spread when
susceptibility and vulnerability are taken into account.
The list of indicators presented in Table 3 will be used to inform decision-making but none should
be considered sufficient to make a final decision.
Deployment of vaccines from the OCV stockpile will also take into consideration programmatic
factors such as the local capacity to organize a campaign and the prevailing security
conditions.
Table 3: Epidemiological and demographic considerations for OCV stockpile deployment7
Criterion Indicator Decision threshold Potential
impact of
vaccination
campaign
High Low
Susceptibility of Number of cases reported in the No or few cases X
the population affected area(s) during the past 2– reported
3 years
High number of cases X
reported
Attack rate of previous outbreaks High attack rate X
1
in the affected area(s)
Low attack rate X
Vulnerability of Case-fatality rate (CFR) of High CFR X
the population previous outbreaks in the affected
Low CFR X
area(s)2
1
The calculation of attack rates will rely on the availability of population figures. In some instances, cholera attack rates are
overestimated because all cases of acute watery diarrhoea are included in the numerator. In general, the quality of the data
should be checked when using this indicator. According to Médecins Sans Frontières (MSF) 50 guidelines, the maximum
expected attack rate (i.e. the “worst case scenario”) would be 5% of the entire population in refugee settings and urban slums,
and 2% in rural areas. These figures might however be exceeded in completely naive population as occurred in 2010 in Haiti.
2
The CFR is likely to be underestimated if all cases of acute watery diarrhoea (and not only cases of cholera) are included in
the denominator. Only deaths occurring in health care facilities are usually reported. In general, the quality of the data should
51
be checked when applying this indicator. According to WHO, CFR should remain below 1% with proper treatment.
21Refugee camp, internally Yes X
displaced people, or slums present
No X
in the affected area(s)
Area(s) with important population Yes X
movements (border, market hub,
No X
etc.)
Population density in the affected High density X
area(s)
Low density X
Access to water, sanitation, and Poor access X
hygiene
Good access X
Risk of spatial Time elapsed / maturity of the Few weeks X
extension outbreak since first case reported3
Few months X
Attack rate since the start of the Low attack rate X
current outbreak (i.e. cumulative
High attack rate X
cases)1
Proportion of health units in the Low proportion X
4
district reporting cases
High proportion X
Time at which first cases were First cases notified X
notified during the epidemic early in the season
season5
First cases notified late X
in the season
3
The duration of cholera outbreaks within a given area present a high degree of variability. Examples include Mozambique:
range 1–25 weeks, mean 7.2 weeks; 12 and Uganda: range 4–27 weeks52
4
The localisation of the health units is used as a proxy indicator for the localisation of the cases to estimate the current
extension of the outbreak, since the exact addresses of cases would most likely be unavailable at national level. Countries
applying for stockpile vaccines should actively seek reliable information about cases of acute watery diarrhoea from all
health units in the affected district(s).
5
In some areas, cholera outbreaks occur on a regular basis, every year or so, usually during the rainy season
22Monitoring and evaluation of the OCV stockpile
While there is evidence that the use of OCV in pre-emptive and preventive campaigns will have a
positive impact on reducing mortality and morbidity, there is currently insufficient evidence to
determine the role of the vaccine in outbreak response.
Given the limited global supply of OCV compared with the potential need, it will be crucial to
document the impact of the stockpile on cholera prevention and control plans and on disease burden,
both locally and globally.
Documenting both the decision and outcomes of use or non-use of OCV will also be vital to
developing evidence-based guidance and strengthening recommendations for future OCV use.
To address this need a rigorous system for monitoring and evaluating should be embedded within the
OCV stockpile mechanism.53
Findings will be reported to all relevant stakeholders, including stockpile decision-makers, past and
potential requesting countries or organizations, donors, and technical partners.
As one of the objectives of the 3 years period stockpile is to gather the evidence of the impact of
vaccination on cholera epidemics, countries requesting access to OCV-ICG stockpile will be requested
to implement and/or provide the necessary data for M&E purpose. Specific M&E protocols will be
available for their implementation.
23References:
1. Ali M, Lopez AL, Young YA, Kim YE, Sah B, Maskery B, Clemens J. The global burden of cholera. Bull World Health
Organ 2012;90:209-218A
2. Siddique AK, Nair GB, Alam M, Sack DA, Huq A, Nizam A, Longini IM Jr, Qadri F, Faruque SM, Colwell RR, Ahmed S,
Iqbal A, Bhuiyan NA, Sack RB. El Tor cholera with severe disease: a new threat to Asia and beyond. Epidemiol
Infect. 2010 Mar;138(3):347-52.
3. Background Paper on the Integration of Oral Cholera Vaccines into Global Cholera Control Programmes
http://www.who.int/immunization/sage/1_Background_Paper_Cholera_Vaccines_FINALdraft_13_oct_v2.pdf
4. Deen JL et al. The high burden of cholera in children: comparison of incidence from endemic areas in Asia and
Africa. PLoS Neglected Tropical Diseases, 2008, 2(2):e173.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2254203/pdf/pntd.0000173.pdf
5. Resolution WHA64.15. Cholera: mechanism for control and prevention. In: Sixty-fourth World Health Assembly,
Geneva, 16–24 May 2011. Volume 1. Resolutions, decisions and annexes. Geneva: World Health Organization;
2011 (WHA64/2011/REC/1). Available from: www.who.int/entity/cholera/.../Resolution_CholeraA64_R15-en.pdf
[accessed 5 September 2012].
6. WHO Consultation on oral cholera vaccine (OCV) stockpile strategic framework: potential objectives and possible
policy options. 2012. Geneva: Department of Immunization, Vaccines and Biologicals, World Health Organization;
2012 (WHO/IVB/12.05). http://www.who.int/immunization/documents/innovation/WHO_IVB_12.05/en/
7. WHO Technical Working Group on creation of an oral cholera vaccine stockpile
Meeting report - Geneva, 26–27 April 2012. http://www.who.int/cholera/publications/oral_cholera_vaccine/en/
8. Jertborn M, Svennerholm AM, Holmgren J. Evaluation of different immunization schedules for oral cholera B
subunit-whole cell vaccine in Swedish volunteers. Vaccine, 1993, 11:1007–1012.
9. Trach DD et al. Investigations into the safety and immunogenicity of a killed oral cholera vaccine developed in Viet
Nam. Bulletin of the World Health Organization, 2002, 80(1):2–8
10. Grading table II (effectiveness. Available from http: http://www.who.int/immunization/
cholera_grad_effectiveness.pdf
11. Grading table I (safety) with key references. Available from http: http://www.who.int/immunization/
cholera_grad_safety.pdf
12. Grading table II (duration of protection). Available from
http://www.who.int/immunization/cholera_grad_duration.pdf
13. http://www.who.int/immunization_standards/vaccine_quality/117_Dukoral_PI_updated_2012-07-05.pdf
14. http://www.who.int/immunization_standards/vaccine_quality/pq_250_cholera_1dose_shantha_insert.pdf
15. Sur D, Kanungo S, Sah B, Manna B, Ali M, Paisley AM et al. Efficacy of a low-cost, inactivated whole-cell oral
cholera vaccine: results from 3 years of follow-up of a randomized, controlled trial. PLoS Neglected Tropical
Diseases. 2011; 5(10):e1289
16. Clemens JD, et al. Field trial of oral cholera vaccines in Bangladesh: results of one year of follow-up. J Inf Dis
1988;158:60-9.
17. Clemens JD, et al. Field trial of oral cholera vaccines in Bangladesh. Lancet 1986;2(8499):124-7.
18. Clemens JD et al. Field trial of oral cholera vaccines in Bangladesh: results from three-year follow-up. Lancet,
1990, 335:270–273.
19. Ali M, Emch M, von Seidlein L, Yunus M, Sack DA, Rao M et al. Herd immunity conferred by killed oral cholera
vaccines in Bangladesh: a reanalysis. Lancet. 2005; 366(9479):44–49.
20. Longini IM et al. Controlling endemic cholera with oral vaccines. PLoS Medicine,2007, 4(11):e336.
21. Sack DA. Herd protection and herd amplification in cholera. Journal of Health, Population and Nutrition, 2006,
24(1):1–5.
22. Sur D et al. Efficacy and safety of a modified killed-whole-cell oral cholera vaccine in India: an interim analysis of a
cluster-randomised, double-blind, placebo-controlled trial. Lancet 2009; 374: 1694-1702
23. Ali et al. Herd Protection by a Bivalent Killed Whole-Cell Oral Cholera Vaccine in the Slums of Kolkata, India. CID
2013 ; 56 :1123-31
24. WHO. Cholera vaccines: WHO position paper Weekly Epidemiologic Record (WER) No 13, 2010, 85, 117-128
http://www.who.int/wer/2010/wer8513.pdf
25. WHO- Strategic Advisory Group of Experts.Meeting of the Strategic Advisory Group of Experts on immunization,
October 2009 – conclusions and recommendations. Weekly Epidemiologic Record (WER) No 50, 2009, pp. 517-
532. http://www.who.int/wer/2009/wer8450.pdf
26. World Health Organization. Oral cholera vaccine use in complex emergencies: what next? WHO Meeting Report
2005 http://www.who.int/cholera/publications/cholera_vaccines_emergencies_2005.pdf
27. Maskery B et al Oral Cholera Vaccine : an investment case.
http://www.who.int/immunization/sage/SAGE_April_2011_cholera_investment_case.pdf (accessed on 12
September 2013)
2428. Jeuland M, Cook J, Poulos C, Clemens J, Whittington D, DOMI cholera economics study group. Cost-effectiveness
of new-generation oral cholera vaccines: a multi-side analysis. Value in Health, 2009, 12(6):899-908.
29. Vu DT, Hossain MM, Nguyen DS, Nguyen TH, Rao MR, Do GC, Naficy A, Nguyen TK, Acosta CJ, Deen JL, Clemens JD,
Dang DT. Coverage and costs of mass immunization of an oral cholera vaccine in Vietnam.J Health PopulNutr.
2003, 21(4):304-8.
30. Thiem V., Deen J, Von Seidlein L, Canh D, Anh D, Park J, Ali M, Danovaroholliday M, Son N, Hoa N. Long-term
Effectiveness against Cholera of Oral Killed Whole-cell Vaccine Produced in Vietnam. Vaccine, 2006, 24(20):4297-
303.
31. Cavailler P et al. Feasibility of a mass vaccination campaign using a two-dose oral cholera in an urban cholera-
endemic setting in Mozambique. Vaccine, 2006 24(5):4890-
http://fieldresearch.msf.org/msf/bitstream/10144/18822/1/feasibilty%20of%20a%20mass%20vaccination.pdf
32. Lucas Marcelino ES et al. Effectiveness of Mass Oral Cholera Vaccination in Beira, Mozambique. New England
Journal of Medicine, 2005, 352(8):757-67.
33. Schaetti C et al. Improving Community Coverage of Oral Cholera Mass Vaccination Campaigns: Lessons Learned in
Zanzibar. PLoS ONE, 2012, 7(7):e41527.
34. Schaetti C et al. Costs of Illness Due to Cholera, Costs of Immunization and Cost-Effectiveness of an Oral Cholera
Mass Vaccination Campaign in Zanzibar. PLoS Neglected Tropical Diseases. 2012, 8(10) :e1844.
35. Khatib AM et al. Effectiveness of an oral cholera vaccine in Zanzibar: findings from a mass vaccination campaign
and observational cohort study. Lancet Infectious Diseases, 2012, 12(11):837-44.
36. Legros D, Paquet C, Perea W, Marty I, Mugisha NK, Royer H et.al. Mass vaccination with a two-dose oral cholera
vaccine in a refugee camp. Bull World Health Organ 1999; 77(10):837-41.
37. Dorlencourt F, Legros D, Paquet C, Neira M, Ivanoff B, Le Saout E. Effectiveness of Mass Vaccination with WC/rBS
Cholera Vaccine during an Epidemic in Adjumani District, Uganda. Bulletin of the World Health Organization, 1999,
77(11):949-50.
38. Chaignat CL, Monti V, Soepardi J, Petersen G, Sorensen E, Narain J. Cholera in disasters: do vaccines prompt new
hopes? Expert Rev Vaccine 2008; 7(4):431-35.
39. World Health Organization. Use of the Two-dose Oral Cholera Vaccine in the Context of a Major Natural Disaster.
Report of a mass vaccination campaign in Aceh Province, Indonesia, 2005.
http://www.who.int/topics/cholera/publications/final_tsunami.pdf
40.
Ivers LC, Farmer PE, Pape WJ. Oral Cholera Vaccine and Integrated Cholera Control in Haiti. The Lancet, 2012,
379(9831):2026-8.
41. Calain P, Chaine JP, Johnson E, Hawley ML, O'Leary MJ, Oshitani H, Chaignat CL. Can oral cholera vaccination play
a role in controlling a cholera outbreak? Vaccine. 2004, 22(19):2444-51.
42. Conrad S. Le risque de choléra à Mayotte: étude de l’accès à l’eau des populations en situation de pauvreté et
suggestions de surveillance sanitaire et environnementale. Mémoire de l’Ecole Nationale de Santé Publique.
Rennes, 2002.
43. De Brettes A, Carsalade GY, Petinelli F, Benoit-Cattin T, Coulaud X, Sassier D, Polycarpe D. Le choléra à Mayotte.
BEH, 2001, 8:33-5.
44. Sissoko D, Receveur MC, Medinger G, Coulaud X, Polycarpe D. Mayotte: situation sanitaire à l’ère de la
départementalisation. Med Trop, 2002, 62:583-8.
45. Beatty ME, Jack T, Sivapalasingam S, Yao SS, Paul I, Bibb B, Greene KD, Kubota K, Mintz ED, Brooks JT. An
Outbreak of Vibrio Cholerae O1 Infections on Ebeye Island, Republic of the Marshall Islands, Associated with Use
of an Adequately Chlorinated Water Source. Clinical Infectious Diseases, 2004, 38:1-9.
46. Anh DD, Lopez AL, Thiem VD, Grahek SL, Duong TN, Park JK, Kwon HJ, Favorov M, Hien NT, Clemens JD. Use of
oral cholera vaccines in an outbreak in Vietnam: a case control study. PLoSNegl Trop Dis. 2011, 5(1):e1006.
47. Ciglenecki I, Sakoba K, Luquero FJ, Heile M, Itama C, et al. (2013) Feasibility of Mass Vaccination
Campaign with Oral Cholera Vaccines in Response to an Outbreak in Guinea. PLoS Med 10(9): e1001512.
doi:10.1371/journal.pmed.1001512
48. WHO : Oral cholera vaccines in mass immunization campaigns: guidance for planning and use.
http://whqlibdoc.who.int/publications/2010/9789241500432_eng.pdf
49. UNICEF. Guidance note on use of Oral Cholera vaccines for UNICEF.
http://www.unicef.org/immunization/files/UNICEF_OCV_Guidance_20_July2012_final.pdf
50. Cholera guidelines, second edition. 2004. Available from:
http://www.bvsde.paho.org/texcom/cd045364/choleraguide.pdf, accessed May 22 2012.
51. Cholera. Fact sheet no. 107. 2011. Available from:
http://www.who.int/mediacentre/factsheets/fs107/en/index.html, accessed May 21 2012.
2552. An investment case for the accelerated introduction of oral cholera vaccines. 2012. Available from:
http://www.ivi.int/publication/IVI_Global_cholera_case.pdf
53. World Health Organization. Framework for monitoring and evaluation of an oral cholera vaccine stockpile.
WHO Oral Cholera Vaccine Stockpile Evaluation and Monitoring Working Group September 2012
26You can also read