Oregon Health Policy Board (OHPB) Draft Meeting Minutes September 7, 2021 Zoom Virtual Meeting
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Oregon Health Policy Board (OHPB)
Draft Meeting Minutes
September 7, 2021
Zoom Virtual Meeting
1. Welcome, Roll Call and Minutes Approval – Chair Bangsberg
OHPB members present:
Chair David Bangsberg, Vice Chair Oscar Arana, John Santa, Kirsten Isaacson, Brenda
Johnson, Bill Kramer, Jessica Gomez, and Ebony Clarke
Oregon Health Authority (OHA) staff present:
Patrick Allen, Jeremy Vandehey, Trilby de Jung, Lori Coyner, Jeff Scroggin, Sara Bartelmann,
Stephanie Jarem, Tara Chetock, Michelle Hatfield, Annette Pierce, Philip Schmidt, Amy Clary,
Annaliese Dolph, Kate Lonborg, Mackenzie Carroll, Trang Weitemier, Stacey Schubert, Alissa
Robbins, Maria Castro, Lisa Parker, Holly Heiberg, Tim Sweeney, Leann Johnson, Laurel
Swerdlow, Megan Auclair, Kyleen Zimber, Steve Allen, Tom Wunderbro, Courtney Johnson,
Tristan Fernandez, Chris DeMars, Dawn Shaw, Zachary Goldman, Jill Gray, Amy Clary, Craig
Mosbaek, Andy Davis, Summer Boslaugh, David Inbody, Lisa A. Parker, Melina Malone, Estela
Gomez, Lisa Krois, Laurel Swerdlow, Kyleen Zimber
Quorum was present. OHPB voted unanimously to approve the August meeting minutes.
2. OHA Director’s Update – Patrick Allen
Patrick notified OHPB that Governor Brown is holding a press conference today with OHA’s Dr.
Sidelinger and partners to review where things are at right now [COVID] with return to school
plans.
Patrick provided an update on the fifth wave of the pandemic driven by the Delta variant.
Encouraging signs in the last couple of weeks that we have possibly plateaued; most indicators
have stopped going up as rapidly as they had before. Most of the worst stress on hospitals is
occurring in the counties that are among the least vaccinated; an upwards of 90% of those who
are hospitalized, who are in ICU, and who are dying, are unvaccinated right now. Using staffing
contracts, OHA deployed ~650 licensed healthcare staff, mostly to hospitals in southwest
Oregon (although not exclusively). Some of the licensed staff are trained from nurses to CNAs to
respiratory therapists. Some have been deployed to long term care, as well as roughly 800
Oregon National Guard members. These are non-medical staff to do things like patient
movement and room cleaning, helping with paperwork, etc. to relieve some of the pressure.
Patrick shared about planning for COVID vaccine boosters; currently doing third doses or
additional doses for people who are immunocompromised to effectively complete their
vaccination series. There is some back and forth going on right now at FDA and CDC, with the
administration on who exactly will be eligible for boosters, beginning September 20, 2021. There
are concerns for when doses for kids under 12 get approved; there’s going to be a dosage issue;
it’s not going to be the same physical dose size for kids is it is for adults. This could cause
resource constraints, depending on availability of those doses. There are exemptions available
based on medical or religious exempt needs. There are forms for folks to use to obtain those
exemptions; requirements take effect on October 18th.
Patrick finished with the work that’s being done beyond the pandemic; the revenue forecast
came out on August 25th and continues to be strong. For the investments we’re making in
behavior health, and Cover All People (COP), particularly COP has $100 million price tag but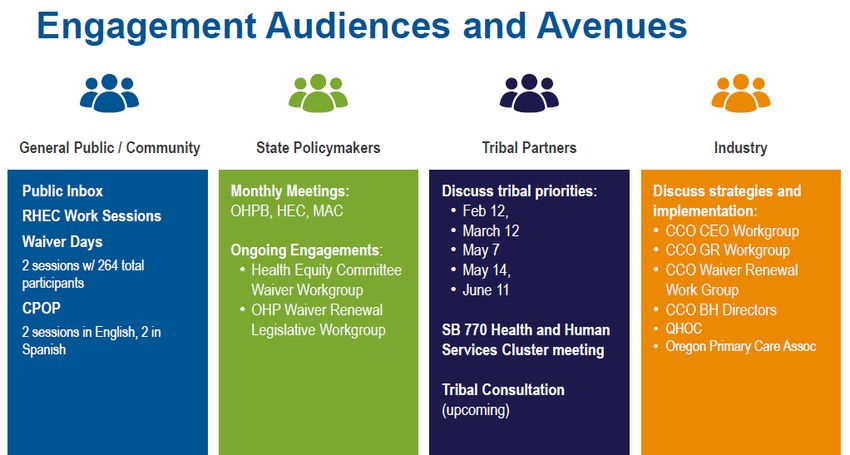
that’s not the price tag for full rollout to literally all people so being able to expand beyond the
initial populations that we'll cover is really contingent on what revenue looks like in buying and
going forward.
(Members were invited to ask questions)
Patrick addressed the rates of increase of vaccine, we continue to see an increase in
communities of color. Collectively with work from local partners we’ve closed the vaccine gap in
communities of color by 50% vaccinated now. We’re continuing to make progress.
Brenda Johnson questioned if there is any additional information in terms of forecasting recovery
for the workforce, or anything in particular the state is looking at doing other than the kid of surge
support mentioned. Also curious about the kinds of things that we can influence from the way we
set goals and targets within the system. I'm specifically wondering about our CCO measures,
how 2021 will pan out for the end of the year, and expectations we have from OHA, or any other
relief in that neck of the woods.
Patrick’s response – The Metrics & Scoring Committees is going to be considering this month as
a package of how to characterize it. Not eliminating or making metrics report only but dialing
them back below past path levels of performance. There shouldn’t be a lot of effort that needs to
go into meeting those metrics. They’re not going to disrupt the structure of the overall system;
going forward and trying to deal with those is the way that they’re envisioning trying to move
through that.
Oscar Arana asked if there were any data regarding how CCOs are doing, related to vaccinating
their members. If some of the CCOs are potentially doing better than others, and what kind of
strategies some CCOs might benefit from learning from one another?
Patrick’s response – Medicaid members generally are lagging the overall population in
vaccination, with other data that tracks to education levels, race, ethnicity, income levels, those
are all indicators of challenges and getting populations vaccinated; there’s a strong geographic
component as well. We can work on getting you some specifics for that.
3. Public Comment
Felisa Higgins gave public comment, “Hi, I'm Felisa Higgins. I'm a political director at SEIU Local
49. And a former member of the Oregon Health Policy Board, it's good to see you all. And it's
great to have been following your continued and amazing work. I'm actually testifying today on
House Bill 2362, which you'll actually hear a summary of later in your meeting today. So, I think
my comments are maybe a little premature. So, I'm just going to go through really briefly what it
does, because I think you'll get a more detailed summary from the staff later on in your meeting.
But House Bill 2362, which was passed in the last legislative session, and is implemented later
in 2022, is a bill that allows the Oregon Health Authority to review mergers and positions
between hospitals, insurance companies and small affiliated clinics. So, what this really does, it's
very critical for our state in the reaching the goals that we all hope to accomplish. I think, you
know, as long as I have a policy board has been in existence, and we've moved to the health
authority, and for much longer than that organ has really been trying to strive towards containing
the cost of care. And we've taken major steps in moving in that direction, including the
sustainable cost growth committee, the incredible work that happened during the legislative
September 7, 2021 | meeting minutes Pg. 2session of setting that cost growth target. This is a core piece of that work. Massachusetts have
modeled this when they had set their sustainable cost growth target by really laying a foundation
to review what the impact of mergers and acquisitions are, not on health systems alone, but
what really, they are on costs. And all the academic research that has been done on mergers
and acquisitions, say there's little to no improvement in quality. But there are major impacts to
costs when health systems or larger systems come together and merge. And so, this would
allow the Oregon Health Authority to really look into those until we think it's a really core
component of the health care costs work that we've been doing. The other important thing I think
critical component of this where Oregon did something that I think Oregonians reaffirmed time
and time, again, is that we implemented an equity provision in this really where we look at not
just costs, but what are the impacts on some of the core services and essential services? I’ll let
staff explain more on that.”
An Do gave public comment: “Morning everyone. My name is An Do. I'm the executive director
of Planned Parenthood advocates of Oregon. Thank you all so much for having me here today.
Thank you to Felisa for providing some context before I provide my public comment on Planned
Parenthood advocates of Oregon were among many, many supporters of this recently passed
mergers and acquisitions legislation. All part groups really are centering health equity and trying
to work with in lockstep with the state to ensure that everyone has access to the care they need,
regardless of where they live, how they are covered or how much money they make. We're
excited that implementation is getting underway. And now while not all healthcare murders are
inherently detrimental, we have observed a troubling pattern of reproductive and gender
affirming care services being restricted once the ink has dried on past deals, unfortunately, once
transactions are finalized, it's impossible to reverse the impact of denied or delayed care for
patients. Thankfully in the legislature passed legislation will enable our state to proactively act in
the best interest of Oregonians by establishing a clear pre transaction review process, including
transparency around changes and access to essential services. Specifically, we are really
encouraged that the merger review process will involve soliciting the explicit input of local
communities those most impacted if a transaction may result in the loss or change in access to
essential services, or statute, which will have the authority to appoint a review board have
stakeholders from affected communities, consumer advocates and healthcare experts to
conduct a comprehensive review, the review board will be empowered to hold the public
meetings and otherwise engage additional community members. This process directly supports
O'Shea's broader goals to increase the involvement of individuals and family members in all
aspects of health care delivery and planning and to increase accountability of the healthcare
system. The inclusion of community voices as important is an important step in acknowledging
that well, community is always one of the most important stakeholders in any transaction, and
certainly the most impacted, they rarely have a meaningful seat at the table. TBL will be
continuing to stay engaged as the program is further developed, and we wholeheartedly support
this effort. Thank you.”
Dr. Jack Haciak gave public comment: “Good morning. This is Dr. Jack Haciak. I'm a retired
psychologist and program administrator. I have my own consultation organization called
Dynamic Changes LLC here in Salem, Oregon. Because it is just very briefly, as I make input to
other meetings from governmental offices, I would appreciate if the public comments section
could be moved more toward the end, following the major agenda item discussions. I prepare,
when I do the agenda items, for certain meeting two that are of value to me. I do some
homework, I talk with a couple of legislators and prepare so that I can listen attentively to the
September 7, 2021 | meeting minutes Pg. 3new input made during the meeting, and then form a comment or a question that I would like,
have an attention by the next meeting. So that would be advantageous to me. I'm not sure if that
can be accommodated, but I thought I'd make my input. Thank you very much.”
4. OHA 1115 Medicaid Waiver Update – Lori Coyner & Jeremy Vandehey
Lori gave us a basic understanding of what’s been done across the previous 5-6 months of
obtaining feedback from community and stakeholders and other partners.
✓Acknowledge realities of COVID-19 in Oregon
✓Be accountable and responsive to community
✓Educate, inform, listen
✓Incorporate waiver feedback
✓Re-route non-waiver feedback appropriately
Lori discussed who they’ve engaged with; had opportunities for lots of different folks to weigh in;
now working to incorporate waiver feedback and rerouting non-waiver feedback. The waiver is
geared towards asking we waive federal rule in ways to improve both the quality of care and
equity for Oregonians on the Oregon Health Plan.
One of the areas of feedback that we’ve received from our community partners has been really
positive, for members to self-attest income, their income gets verified most of the time through
data processing. We want to continue that as it does not require a waiver. We can engage in
that work directly without having to include it in the waiver.
The required public comment period is coming up:
• A 30-day public notice and comment period.
September 7, 2021 | meeting minutes Pg. 4• A comprehensive description of the proposed waiver “that contains a sufficient level of
detail to ensure meaningful input from the public.”
• A current website to share these materials and allow for any interested parties to sign up
for an email list to be kept apprised of the application.
• Hold at least two public hearings on separate dates in separate location that offer the
public an opportunity to learn about the application and comment on it. (one will be
through our Medicaid Advisory Council)
Lori made note to list ways to stay informed:
Stay informed about progress and review concept paper drafts at our website:
oregon.gov/1115waiverrenewal
Submit comments and questions related to the waiver
1115Waiver.Renewal@dhsoha.state.or.us
Incentivizing Equitable Care
Advanced Health Equity
To achieve this, our policy framework breaks down the drivers of health inequities into four
actionable sub-goals:
1) Maximizing OHP Coverage
2) Stabilizing transitions to minimize disruptions in care
3) Encouraging smart, flexible spending for health equity
4) Focused health equity investments
We also are going to propose to redistribute how some of the decision-making power is
structured so that there's a stronger community voice in what's measured; to rethink how this will
advance equity overall.
Proposal
Restructure the Quality Incentive Program into two complementary components
• Downstream Metrics
• Upstream Metrics focused on equity
Redistributing decision-making power
Rethink the incentive structure to better advance equity
Waiver Concepts: Refocusing CCO Metrics
Upstream
o Root causes of health inequities. These metrics focus on things like socio-
economic factors and institutional racism. For example: Meaningful Language
Access to Culturally Responsive Care
September 7, 2021 | meeting minutes Pg. 5Downstream
o Medical model. These metrics focus on things like injury and disease. For
example: Controlling High Blood Pressure or Emergency Department Utilization.
What the team is proposing is to work with the Oregon Legislature to change the health plan
quality metrics committee to a health equity quality metrics committee. This committee would
have oversight and approval of the downstream metrics. Meaning those CMS core metrics,
selected by the metrics and scoring, would advise on how measures operate, operationalizing
measures. Developing specifications form metrics that address member and community
concerns; it will provide a mechanism having community engagement and some member voice
in what these metrics are. By changing this to equity centered committee will align and set
inventive payments to better advance balance and equity. We’re working with Oregon legislature
to change the Health Plan Quality Metrics Committee to the Health Equity Quality Metrics
Committee.
• Oversight and approval of downstream metrics selected by Metrics & Scoring Committee
• Advise on operationalizing measures to address member and community concerns and
priorities
• Incorporation of community engagement and member voice
Rethink the incentive structure to better advance equity
• OHA will work with new Health Equity Quality Metrics Committee and Metrics and Scoring
Committee to decide how upstream metrics are incentivized to best improve health equity
• Incentive payments for upstream and downstream metrics will use a withhold structure
Lori and Jeremy fielded questions and comments with regards to transitioning from a bonus kind
of incentive measures sort of structure to that of a withhold. A withhold means that we hold some
September 7, 2021 | meeting minutes Pg. 6money back from the CCOs and then pay out based on their performance. A true bonus means
they get money on top; withholds are easier for us to track how the dollars are spent. That
money is then reinvested in community for example, it's more motivating for CCOs to do well. I
see three ways that we're going to mitigate that.
• We have upstream metrics that will have lots of weight, they are directly involved equity.
• The downstream metrics: we will look at by reset ethnicity and language to see if there
are improvements across those different language groups, racial groups, etc.
• Have health equity metrics committee that will provide oversight and input in terms of
what’s happening so there’s a connection with community voice that has a much stronger
voice in the metrics as opposed to the way that the Health Plan Quality Metrics
Committee; policy folks and industry folks, not a big proportion of community.
In terms of part of what we're going to have to think about in terms of intended and unintended
consequences. There's a financial impact of this, because of the accounting treatment of
withhold versus a bonus. At the end of the day, we need to make sure that we're clear that what
we're getting is worth the lift that goes into it.
5. New Behavioral Health Metrics and Incentives Committee: Overview & Update – Steve
Allen & Kyleen Zimber
Steve gave a short background on the initiative. The legislature wanted confidence that this
large body of investments would lead to real change. We ultimately landed on the Behavioral
Health Metrics and Incentives Committee; we’ve expanded and leveraged the Committee scope
because it works more broadly. The concept behind this is that a variety of metrics would be
shared or common across a variety of parnters, the individuals that are receiving the least
impactful and effective are often those that are multi-systems involved. This gives us an
opportunity to set a var for changes in the system to bring partners together in new ways to
reward for success.
Goals:
Change how we work to realize meaningful outcomes and eliminate health inequities
• Align support for priorities at the legislative level, the governor’s level across key agencies
and key decision-making bodies to engage partners meaningfully.
• Engage partners meaningfully; not just providers and funders in the system but to bring
new voices in as well. Specifically, from communities of color, and people who want and
need these services.
• Bring down barriers that limit partner participation
• Redistribute power and resources
• Be accountable for outcomes
Transformation Work
2023 Bills/Budget sorted into transformational priorities
• Infrastructure: we haven’t been able to deliver services, access to resources because we
haven’t had the infrastructure built in to provide those services. There’s a very significant
infrastructure investment that includes both brick and mortar facilities.
• Incentives and Accountability
September 7, 2021 | meeting minutes Pg. 7• Children’s System: this is a continuation of significant legislation that was delivered in
2019
• Intensive Services: those folks who are most often multi system involved, court involved,
including people under civil commitment, and aid and assist.
• Crisis System: We have an opportunity with 988, the 911 for behavioral health coming
online in July 2022 to rebuild our crisis system, also mobile crisis, mobile response for
children and families as well as areas to provide crisis services other than emergency
departments and jails.
• Workforce
Kyleen continued going through the slides to explain HB 2086, Behavioral Health Committee.
The conversations they’ve had with legislators who sponsored and how they’ve envisioned this
committee working. Measure 110 was passed by voters in Nov 2020; we established an
oversight and accountability counsel under measure 110. That committee would be representing
people with lived experience and people who were disproportionately impacted by the war on
drugs.
The Behavioral Health Committee
Voting Members
• Health Plan Quality Metrics Committee Chair
• OHPB Health Equity Committee Chair
• CCO Behavioral Health Director
• Community Mental Health Program Representative
• Data Analysis expert
• Consumer Advisory Council member representing adults with mental illness
• System of Care Advisory Council Representative (ORS 418.978)
• Ballot Measure 110 (2020) Oversight and Accountability Council member representing
adults with addictions or co-occurring conditions
• System of Care (ORS 418.976) Representative
• Consumer Representative
• Tribal Government Representative
• One representative of an organization that advocates on behalf of individuals with
intellectual and developmental disabilities
• Behavioral Health Service providers Representative
• Any other member that the OHA Director deems appropriate
Objective: To have the committee filled with at least 51% people who have lived experience.
Behavioral Health Key Upcoming Dates
November 1st –
Report to Legislature on contract changes needed to comply with quality
metrics and incentives developed by the Behavioral Health Committee
December 1st – Report to Legislature – barriers including:
• Legislative changes or changes to the demonstration project under section 1115 of
the Social Security Act needed to apply the quality metrics and incentives developed by
the committee to contracts with coordinated care organizations and counties
September 7, 2021 | meeting minutes Pg. 8• OHA’s specific needs for data infrastructure to implement the quality metrics and
incentives
• Recommendations for facilitating risk-sharing agreements within the health care
delivery system to achieve the goals of the quality metrics
• Recommendations for counties to share in the costs of a hospitalization at OSH 30
days after county is notified that the patient no longer needs hospital level care
February 1st, 2022
• Behavioral Health Committee recommendations regarding metrics and incentives
December 1, 2022
• The $49m Special Purpose Appropriation to support metrics/incentives must be allocated
by the Legislature (if the legislature is unable to allocate the $49 million by December of
2022, then it just goes back into the general emergency fund)
Per the statute (HB 2086), the committee, OHA as staff will need to implement a process for
collecting the health outcome and quality measure data; then report that data to the Oregon
Health Policy Board. Establishing an ongoing communication between that committee and the
Oregon Health Policy Board.
Additional Key Upcoming Dates – Infrastructure Investments
• September 3, 2021 – Applications due from communities to support planning for
behavioral health residential and housing needs
We’re inviting community to provide resources to support the work that people need to do to
effectively plan for this infrastructure. We’ll be awarding up to $5m and grants up to $50k apiece;
we’ll be reviewing those applications with grants going out in the coming weeks to allow wide
range community participation at the local and regional level on identifying the way forward.
• December 1, 2021 – OHA to issue Requests for Proposals for Behavioral Health
Infrastructure Grants
• March 1, 2022 – OHA to demonstrate to Legislature the use of $130M investment so
funds can be released
6. Draft Framework for Reviewing Proposed Material Change Transactions for the Health
Care Market Oversight Program – John McConnell, PhD, Jeremy Vandehey & Zachary
Goldman
John started the presentation by explaining the different types of consolidation in health care.
Horizontal vs Vertical and Provider vs Payer.
Horizontal Consolidation – Like groups or creating systems with like scripts. This could be
hospitals come together to form a big hospital system or the physician groups come together to
form a big physician group.
Vertical Consolidation – Hospitals and physicians coming together to form one big system.
This can affect referral networks and create other types of market power.
September 7, 2021 | meeting minutes Pg. 9There are active, intense negotiations that happen between insurer groups and provider groups.
Insurers know that providers often have a status with a well-known clinic or well know hospital.
Insurers know they need to get those in network in order to be competitive and sell those to
employers or people on the exchange market.
Providers must have a group that increases their ability to negotiate higher prices through
consolidation, bringing everything together, increased market concentration so they have status
and can negotiate for higher rates.
Consolidation is not the same as Integration
By bringing these groups together, the concern among health economists is that you're
aggregating ownership, that that's leading to increased market power on the provider side, and
that's leading to higher prices, and maybe no change in quality or maybe lower quality.
There's another story that's plausible, that you bring groups together, and that by consolidating
these in terms of vertical and horizontal groups, you get a lot of coordination of production, you
get increased efficiency, so maybe less redundancy, lower prices, and higher quality.
Horizontal Hospital Consolidation
• Higher Prices for insurers
• Lower or unchanged quality (e.g., mortality rate)
• Some scale economies
• Costs lower only when facilities combined (e.g., hospital closure, consolidating service
lines)
- Average 6% price increase for mergers of geographically close hospitals, 2007-2011
- Monopoly hospitals have 12% higher prices
- Monopoly hospitals’ contracts place more risk on insurers (e.g., prices as share of
charges)
Vertical Integration
- Vertical integration associated with higher prices (e.g., 6% higher in independent
practices vs hospital owned)
- Almost all savings from Medicare MSSP ACO program come out of physician-owned
ACOs; no savings from hospital-integrated ACOs
- No change in quality from integration
Insurer Consolidation – Prices
We'd like premiums to be low for consumers and individuals; insurance markets are becoming
more concentrated. If there's lots and lots of insurance competition among insurers, but if the
provider market is really concentrated, then what you're left with is probably pretty high
premiums, because providers have market power, they're going to have lots of insurers, insurers
don't have market power. So the balance of powers on the provider side and the prices and
premiums tend to be higher.
• Allows insurers to negotiate lower provider prices
September 7, 2021 | meeting minutes Pg. 10o In one study, insurers with market shares of 15% or more negotiated prices for
physician office visits that were 21% lower than those with less than 5% market
share.
Insurer Consolidation - Premiums
There may be insurers that are able to negotiate lower prices, when they're talking to the
providers, they may hold on to that lower price, and then turn to the employers and individuals
and charge a high premium; we don’t usually see these savings passed on to the consumer as
lower premiums. Insurer consolidation tends to lead to premium increases, they've got more
market power; when they go out to employers and individuals, they don't share that back, but
that may differ for between for profit and not for profit insurer groups.
The insurance market in Oregon, is really characterized as one that's not concentrated. Oregon
is the only states where there are no Metropolitan Statistical Areas that exceed the threshold for
highly concentrated commercial markets.
Consider Tradeoffs
• Consolidation may help keep some providers afloat
• Evidence: higher prices, quality does not improve
• Higher prices are passed on in the form of higher premiums and lower wages for most
Oregonians
I don't want to come down on the side and say, competition is always helpful, I think what I do
want to come down on firmly is that there is increasing consolidation. The impact on commercial
premiums of commercial market is generally deleterious; we're creating systems and
consolidating, and that's going to lead to economies of scale, better quality. I would agree with
that, once you have a cap on prices, if you introduce competition, it's not exactly clear what
you're asking to compete for; there can be competition around for selection on patients rather
than competition for quality.
Jeremy gave a brief overview on what House Bill 2362 (2021). What House Bill 2362 (2021)
does is define types of transactions that represent mergers or acquisitions or affiliations; defines
those as material change transactions and creates authority for and responsibility for OHA to
preview those requires notice be filed with the state. This provides an expedited process, a more
elongated process, a timeline in which we would do the review; including certain points where
we would get community input and increased transparency so that the community knows that
this transaction is, potentially going to occur. The three major “buckets” of the types of
transactions that are for a change of the ownership or control of the organization:
Merger – Two organizations combine and become a new organization
Acquire – One organization takes over the different organizations; sometimes completely
goes away, sometimes remains a subsidiary
Affiliate – Organizations will come to a new type of business arrangement; creates a new
governance structure and the way they do business together
The goal here isn't to say, not allowing you these transactions to go forward its really to create a
process for view and to make sure that we're bringing in an equity lens that we're understanding
September 7, 2021 | meeting minutes Pg. 11what the purpose of the transaction is; what the potential impact of good or bad could be for the
community and developing so the community has a voice and that there's transparency before it
moves forward. A lot of the time folks have no idea that a major local provider might be in the
process of being purchased by out of state company or by another organization until a press
release announces that the transaction is final. The idea here is to slow things down, to give the
community a voice, and make sure that they've got a voice and understand the potential impacts
on their local healthcare system before a transaction moves forward. The legislation will have
OHA approve with conditions or reject the transaction based off of whether what the impact will
be on equity, access, and cost, that’s a very significant change. There’s a lot of talk of other
states looking at similar types of programs. There will be a lot of attention on us as we’re getting
this off the ground.
Zachary discussed some specifics, particularly financial thresholds, because that's a key part of
the bill. In terms of what transactions will be reviewed, those transactions that one entity has $25
million or more in average revenue, and another has $10 million more average revenue. There
could be cases in which there's an out of state entity affiliating, acquiring or merging with an
instate entity. Those transactions could be reviewed, if an instate entity is involved in that
transaction, the aforementioned revenue thresholds are met. And as the statute states, the
transaction may result in increases in price, limit access, etc. This isn’t solely focusing on
domestic carriers only in Oregon Hospitals, providers or whoever, they could involve
transactions that include out of state entities as well. We're in the process of developing rules
that will clearly outline what transactions would be subject and what transactions would not be
subject to review.
Transactions Subject to Review:
• Would change the governance or control of an entity
• A merger of one health care entity with another entity
• An acquisition of one or more health care entities by another entity
• A new contract, new clinical affiliation, or new contracting affiliation that will eliminate or
significantly reduce essential services
• A corporate affiliation involving at least one health care entity and is not excluded from
review
• Forms a new partnership, joint venture, accountable care organization, parent
organization or management services organization
Transactions NOT Subject to Review:
• Large purchases of equipment, supplies or services
• Medial services contracts (as defined in the bill)
• Contracts where one health care entity provides patient services on behalf of a second
health care entity that is responsible for and bills and receives reimbursement for patient
care
• Affiliation between health care entities to adopt advanced VBP methodologies to meet the
state’s health care cost growth target
• Affiliations for collaborating on clinical trials or graduate medical education programs
• Transactions involving FQHCs
September 7, 2021 | meeting minutes Pg. 12Department of Consumer and Business Services
They currently have authority to review mergers and acquisitions that involve carriers,
specifically, this program or talking about the healthcare market oversight program. It could
include those healthcare entities, insurance carriers, but not just insurance carriers.
If this material change transaction does involve a domestic health insurer, then DCBS makes the
final determination on the transaction, but OHA would be providing our review that would have
that equity focus, the cost access quality focus, which is a bit broader than DCBSs current focus.
It’s a little different, but we collaborate very closely with DCBS for those transactions that involve
the carrier.
Department of Justice
The primary purpose of DOJs authority to review transactions involving charitable assets is to
ensure:
• That any sale, merger, or transfer of a nonprofit is on fair terms,
• That the proceeds continue to be used for the hospital’s charitable purposes, and
• That insiders do not receive a financial benefit from the transaction
OHPB’s Role
HP2362 directs OHA to adopt by rule criteria approved by the Oregon Health Policy Board for
the consideration of requests by health care entities to engage in a material change transaction.
Criteria = guiding principles framework
OHPB previously reviewed and approved criteria for SB 1041
Proposed Guiding Principles
When reviewing proposed material transactions, OHA shall:
• Focus on the health of people living in Oregon
• Ground all analyses in the impact to health equity, access to care, health care quality, and
costs
• Meaningfully engage the public & stakeholders in a robust & transparent process, which
may include the creation of stakeholder review boards
• Use resources wisely and collaborate with DCBS & DOJ when applicable
Proposed Framework – OHA’s review of a proposed transaction shall consider the following:
• Costs to consumers, access to services, and quality of health care for all people living in
Oregon
• Health equity, including the entities demonstrated commitment to addressing health
disparities and inequities
• The ability of the entities to achieve Oregon’s Sustainable Health Care Cost Growth
Target
• The market share of the entities involved in the transaction
• The financial stability of the entities involved in the transaction, for situations in which
there is an immediate threat to health care services and the transaction is urgently
needed to protect the interest of consumers
September 7, 2021 | meeting minutes Pg. 13Proposed Framework – For material change transactions involving CCOs, OHA’s review will
also include the following:
• The CCO’s relationship with its local community, including Community Advisory
Council(s) and others
• The ability of the CCO to innovate, coordinate care, provide value, and delivery high-
quality services
• The CCO’s governance and its ability to satisfy State requirements, including OHA’s
policy priorities as outline din contract or as adopted by OHPB
• The ability of the CCO to support social determinants of health
• The financial stability of the CCO, including the CCO’s financial strategies that may
influence the merged organization
Next Steps for the Health Care Market Oversight Program
• Launch website
• Publish informational materials about the program
• Publish timeline for Rules Advisory Committee
Develop Rules
7. OHPB Committees Liaisons: Proposed New Assignments – Tara Chetock
Tara went over the liaison role as and provided an overview on current OHPB liaisons and
presented a proposal for new liaison assignments discussion. Tara explained the OHPB Chair
and Vice Chair are excused from the liaison role because they are contributing so much time in
weekly planning meetings and other Board responsibilities (but they are welcome to serve).
The committees are at the heart of a lot of the work behind the board. And they are the driving
force where a lot of the work gets completed. We need to support and lift up those committees
with expertise of board members. Tara highlight below some of the great bodies of work from
our committees.
September 7, 2021 | meeting minutes Pg. 14Committees & Liaisons
Currently we have four members, Brenda Johnson, Kirsten Isaacson, John Santa and David
Bangsberg serving as liaison across seven OHPB committees. There is currently 10 committees
(soon to be 11) and only eight OHPB members so it’s a challenge to have a liaison for each
committee, so liaison roles are prioritized according to member interest/expertise and the
committee’s work as it relates to OHPB priorities.
Special Projects
There are four OHPB members serving on the Committee Membership Project as sponsors.
Additionally, we have members participating on a new workgroup to help plan the first Cost
Growth Target public hearing.
September 7, 2021 | meeting minutes Pg. 15Framework
When OHPB leadership and OHA staff started to think about
how we wanted to match liaisons and committees, we decided
to focus on a multi-pronged framework that considers the
OHPB priorities (focusing work on health equity, implementing
the cost growth target program, the OHA 1115 waiver
renewal, as well as committees of the board work).
Additionally, we wanted to prioritize committees involved in
OHPB priority related work to ensure liaison coverage and
support. Another consideration beyond OHPB priority related
work is to consider if committees have large strategic planning
efforts, goals, or they're going to need OHPB and liaison
support. Another consideration is the member and their
capacity, interest and expertise. These elements were
considered by OHPB leadership and OHA staff in developing
a proposal for new liaison assignments.
Additionally, at our retreat earlier this year, we discussed the
idea to find natural links and connections between committees
and liaisons to support the work and to create some
collaborative opportunities.
Additional Considerations
- Members are welcome to all committee meetings
- Committees may have multiple liaisons
- Adapt to changing environment
- New tier (current + lined + future liaisons)
- Others?
September 7, 2021 | meeting minutes Pg. 16We'd certainly like to hear if there's any thoughts, concerns, or additional considerations that
you'd all like to share before we conclude today's meeting and start moving into supporting these
transitions with our liaisons.
(no member concerns or edits – the proposed liaison roles will be adopted and transition among
the current and new liaisons will take place over the next couple months).
8. Wrap-up & Final thoughts – Chair David Bangsberg
David reminded members about the upcoming educational webinar on September 14 th at 8am
regarding the interim waiver evaluation and a second educational webinar on September 21st
about the OHA Ombuds Program.
Thank you for all the presenters and the board members for a great discussion. I think we've
made a lot of progress today, and I look forward to seeing you all the upcoming webinar and or
meeting. Take good care everyone.
The next OHPB meeting is Tuesday, October 5th.
(meeting adjourn)
September 7, 2021 | meeting minutes Pg. 17You can also read