Overview of Changes to the Minimum Data Set 3.0 - NYSHFA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

10/19/2018
Overview of Changes to the
Minimum Data Set 3.0
Maureen McCarthy, RN, BS, RAC-MT, QCP-MT, DNS-MT
President/CEO
Celtic Consulting
www.celticconsulting.org
MDS 3.0
• MDS 3.0 Version 1.16.1 will become effective as of October 1, 2018
• The MDS 3.0 and associated documents are available at the following links:
– Link to Webpage: https://www.cms.gov/Medicare/Quality-Initiatives-Patient- Assessment-
Instruments/NursingHomeQualityInits/ NHQIMDS30TechnicalInformation.html
– Direct Link to MDS 3.0 Version 1.16.1: https://www.cms.gov/Medicare/Quality- Initiatives-Patient-Assessment-
Instruments/NursingHomeQualityInits/Downloads/MDS- 30-Item-Sets-v1-16-0R-DRAFT-Revised-for-October-1-2018-
Release.zip
– Item Set Version Changes: There is an Item Changes document within the zip file of item sets that explains which
items were changed from draft version 1.16.0 to final version 1.16.1. The Item changes document is the first file within
the zip
2
1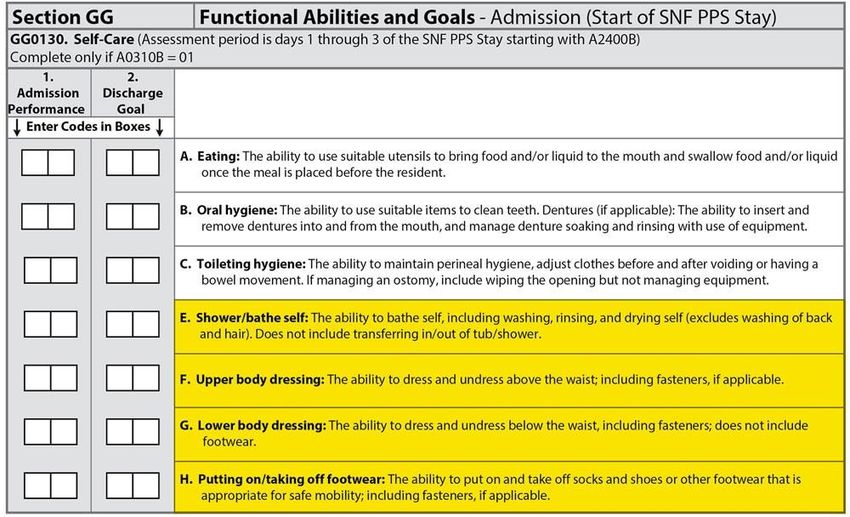
10/19/2018
References and materials utilized from:
• Skilled Nursing Facility Quality Reporting Program Provider Training
• CMS, Abt Associates, RTI
• July/August 2018
• Baltimore, MD
• Four Seasons Hotel
3
Objective: Review Changes by Section
• Sections Changed:
• Section GG- largest number of changes, will review this section last*
• Section I
• Section J
• Section K
• Section M
• Section N
• Section O
• Miscellaneous guidance/clarifications
4
2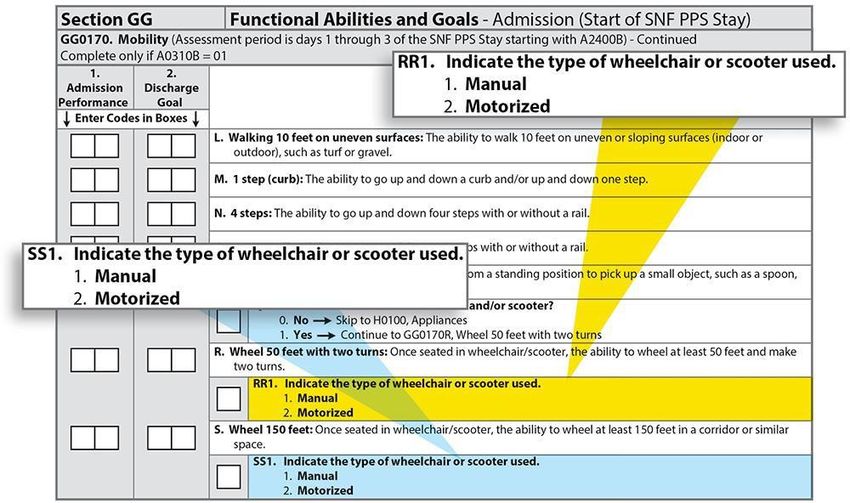
10/19/2018
Item I0020. Indicate the
Resident's Primary Medical
Condition Category
I0020. Indicate the Resident’s Primary Medical
Condition Category
6
3
10/19/2018
I0020 Steps for Assessment
Review the documentation in the medical record
to identify the resident’s primary medical
condition associated with admission to the facility
7
I0020
Steps for Assessment (cont.)
• Medical record sources for physician diagnoses include:
– The most recent history and physical
– Transfer documents
– Discharge summaries
– Progress notes
– Other resources, as available
8
4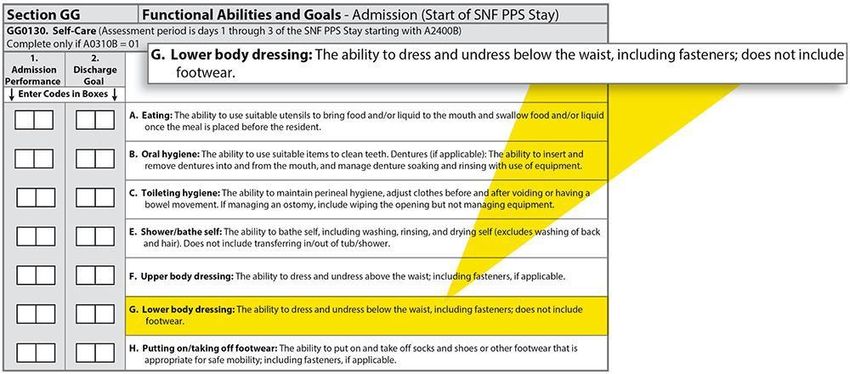
10/19/2018
Fourteen Primary Condition Categories
Associated With the SNF Admission
• Stroke
• Non-traumatic Brain Dysfunction
• Traumatic Brain Dysfunction
• Non-traumatic Spinal Cord Dysfunction
• Traumatic Spinal Cord Dysfunction
• Progressive Neurological Conditions
• Other Neurological Conditions
9
Fourteen Primary Condition Categories
Associated With the SNF Admission (cont.)
• Amputation
• Hip and Knee Replacement
• Fractures and Other Multiple Trauma
• Other Orthopedic Conditions
• Debility, Cardiorespiratory Conditions
• Medically Complex Conditions
• Other Medical Condition
• – Used when no other condition category applies
10
5
10/19/2018
I0020
Coding Instructions
• Complete only if A0310B = 01 (Start of Part AProspective Payment System (PPS) stay)
• Enter the code that represents the primary medical condition that resulted in the resident’s
admission
• If codes 1 through 13 do not apply, enter code 14, “Other Medical Condition,” for I0020
and proceed to I0020A
• Include the primary medical condition coded in Item I0020 in Section I0100 through I8000:
Active Diagnoses in the
• Last 7 Days
11
Section I – Quadriplegia Coding
• Quadriplegia primarily refers to the paralysis of all four limbs, arms and legs,
caused by spinal cord injury.
• Coding I5100 Quadriplegia - limited to spinal cord injuries & must be a
primary diagnosis, not the result of another condition.
• Functional quadriplegia refers to complete immobility due to severe physical
disability or frailty. Conditions such as cerebral palsy, stroke, contractures,
brain disease, advanced dementia, etc. can also cause functional paralysis
that may extend to all limbs hence, the diagnosis functional quadriplegia.
Code the actual diagnosis on the MDS & not the resulting paralysis or paresis.
12
6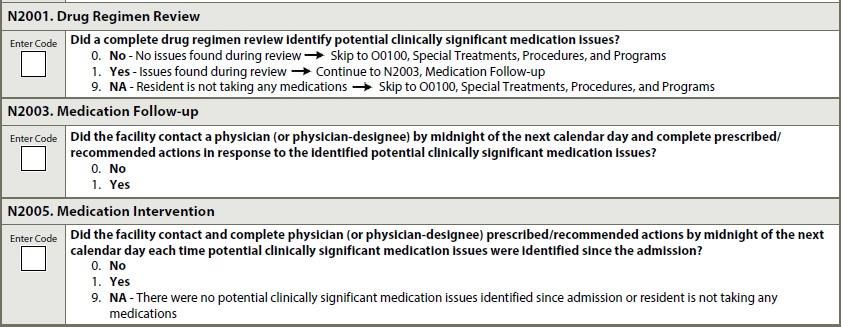
10/19/2018
Section J. Health Conditions
Item J2000. Prior Surgery
7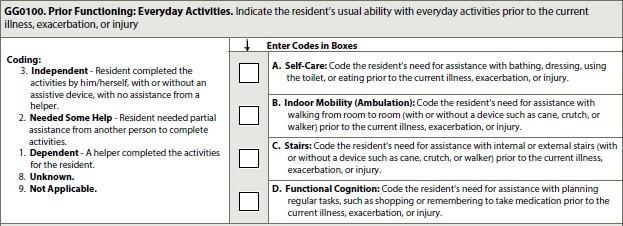
10/19/2018
J2000. Prior Surgery
15
J2000 Steps for Assessment
1. Ask the resident and family or significant other about any
surgical procedures in 100 days prior to admission
2. Review the resident’s medical record to determine whether
the resident had major surgery during the 100 days before
admission
16
8
10/19/2018
J2000 Steps for Assessment (cont.)
• Medical record sources include:
– Medical records received from facilities where the resident
received health care during the previous 100 days
– The most recent history and physical
– Transfer documents
– Discharge summaries
– Progress notes
– Other resources, as available
17
J2000 Coding Instructions
• Code 0, No, if the resident did not have major surgery
during the 100 days prior to admission
• Code 1, Yes, if the resident had major surgery during the 100
days prior to admission
• Code 8, Unknown, if it is unknown or cannot be determined
whether the resident had major surgery during the 100 days
prior to admission
18
9
10/19/2018
J2000 Coding Tips
• Generally, a major surgery for Item J2000 refers to
a procedure that meets all the following criteria:
1. The resident was an inpatient in an acute care hospital for
at least 1 day in the 100 days prior to admission to the
SNF
2. The resident had general anesthesia during the procedure
3. The surgery carried some degree of risk to the resident’s
life or the potential for severe disability
19
K0510: Nutritional Approaches
• CMS does not require completion of Column 1 for items K0510C and
K0510D; however, some States continue to require its completion. It is
important to know your State’s requirements for completing these items.
• If the State does not require the completion of Column 1 for items K0510C and
K0510D, use the standard “no information” code (a dash, “-”).
20
1010/19/2018
K0710: Percent Intake by Artificial Route
• CMS does not require completion of Column 1. While Not a Resident for
items K0710A and
• K0710B; however, some States continue to require its completion. It is
important to know your State’s requirements for completing these items.
• If the State does not require the completion of Column 1 for this item,
use the standard “no information” code (a dash, “-”).
21
Section M: Skin Conditions
• The terms “injury” or “injuries”
has been added in the Section
M heading of the following
items:
• M0100
• M0150
• M0210
• M0300, M0300A
• M0300E, M0300E1,
and M0300E2
• M0300G,
• M0300G1, M0300G2
22
1110/19/2018
Section M: Skin Conditions (cont. 1)
• Removed the term “suspected deep tissue injury in evolution” and
replaced with “deep tissue injury” in items:
• –M0300G and M0300G1
23
Section M: Skin Conditions (cont. 2)
• Items Retiring October 1, 2018:
– M0300B3. Date of oldest Stage 2 pressure ulcer
– M0610A-M0610C. Dimensions of Unhealed Stage 3 or 4
Pressure Ulcers or Eschar
– M0700. Most Severe Tissue Type for Any Pressure Ulcer
– M0800A–M0800F. Worsening in Pressure Ulcer Status Since Prior
Assessment (Omnibus Budget Reconciliation Act (OBRA) or
Scheduled PPS)
– M0900A–M0900D. Healed Pressure Ulcers
• Skip patterns have been updated
24
1210/19/2018
Present On Admission & Pressure Ulcers
Stage 3 If ulcer Present on
5 Day POA Admission or Re-Entry, &
becomes Unstageable
Unstageable *
14 Day NOT POA
during the SNF stay, it
then should NOT be
Unstageable * coded Present on
30 Day NOT POA Admission
* Due to Slough or Eschar
25
Present On Admission & Pressure Ulcers
Residents with an ulcer
Stage 3 who are hospitalized & the
DC/RA ulcer increases Stage or
becomes Unstageable
Unstageable* or Stage 4 during hospitalization, then
5 Day POA on Re-entry the it’s POA on return
* Due to Slough or Eschar
26
1310/19/2018
Present On Admission & Pressure Ulcers
Stage 2 If a staged ulcer becomes
5 Day POA Unstageable then becomes
Unstageable *
stageable again, then compare
14 Day NOT POA stage before & after it was
unstageable. If the stage is
Stage 3 higher, then it should NOT be
30 Day NOT POA coded Present on Admission
* Due to Slough or Eschar
27
Other Section M Coding Guidance
• Kennedy Ulcers – Not to be coded as Pressure per CMS
• Non-surgical dressings – Do Not include adhesive bandages (steri’s,
BandAids)
• Open Lesions – Develop as part of disease or condition – added
more examples (boils, cysts, vesicles)
28
1410/19/2018
Section N: Medications
Definitions
Section N: Medications (cont.)
30
1510/19/2018
Drug Regimen Review (DRR)
• A DRR includes:
– Medication reconciliation
– A review of all medications a resident is currently using
– A review of the drug regimen to identify, and, if possible, prevent
potential clinically significant medication adverse consequences
31
What Does the DRR Include?
• The DRR includes all medications:
– Prescribed and over the counter, including nutritional
supplements, vitamins, and homeopathic and herbal products
– Administered by any route
• The DRR also includes total parenteral nutrition (TPN) and
oxygen
32
1610/19/2018
Potential or Actual Clinically Significant
Medication Issue
• A clinically significant medication issue is a potential or actual
issue that, in the clinician’s professional judgment, warrants:
– Physician (or physician-designee) communication and
– Completion of prescribed/recommended actions by midnight of the
next calendar day (at the latest)
33
Potential or Actual Clinically Significant
Medication Issue (cont. 1)
• Clinically significant means effects, results, or consequences that
materially affect or are likely to affect an individual’s mental, physical,
or psychosocial well-being either:
– Positively by preventing a condition or reducing a risk or
– Negatively by exacerbating, causing, or contributing to a symptom, illness,
or decline in status
34
1710/19/2018
Potential or Actual Clinically Significant
Medication Issue (cont. 2)
• Any circumstance that does not require this immediate attention is
not considered a potential or actual clinically significant medication
issue for the purpose of the DRR items
35
Clinically Significant Medication Issues
• Clinically significant medication issues include, but are not limited to:
– Medication prescribed despite documented medication allergy or prior
adverse reaction
– Excessive or inadequate dose
– Adverse reactions to medication
– Ineffective drug therapy
– Drug interactions
– Duplicate therapy
– Wrong resident, drug, dose, route, and time errors
36
1810/19/2018
Clinically Significant Medication Issues (cont.)
• Clinically significant medication issues include, but are not limited to (cont.):
– Medication dose, frequency, route, or duration not consistent with
resident’s condition, manufacturer’s instructions, or applicable standards
of practice
– Use of a medication without evidence of adequate indication for use
– Presence of a medical condition that may warrant medication therapy
– Omissions
– Nonadherence
37
Contact with Physician
• Communication to the physician to convey an identified potential or
actual clinically significant medication issue AND
• A response from the physician to convey
prescribed/recommended actions in response to the medication
issue
38
1910/19/2018
Contact With Physician (cont. 1)
• Examples of communication methods:
– In person
– Telephone
– Voice mail
– Electronic means
– Fax
– Any other means that appropriately conveys the resident’s status
39
Contact With Physician (cont. 2)
• Communication is directly with the physician/physician-
designee
40
2010/19/2018
How is Physician-Designee Defined?
• According to Appendix PP of the State Operations Manual,
“Physician/practitioner” (physician assistant, nurse practitioner,
clinical nurse specialist) means the individual who has responsibility
for the medical care of a resident
• The role of physician-designee (non-physician practitioner) is
defined by Federal and State licensure regulations
• Please refer to these regulations to determine which clinicians are
licensed to act as physician-designees
41
Medication Follow-Up
• Medication follow-up includes the process of:
– Contacting a physician to communicate the identified
medication issue and
– Completing all physician- prescribed/recommended actions by
midnight of the next calendar day (at the latest)
42
2110/19/2018
New Section N Items:
Coding Guidance
Data Sources/Resources for Coding the DRR
Items
• Medical record sources include:
– Medical records received from facilities where the resident received healthcare
– The resident’s most recent history and physical
– Transfer documents
– Discharge summaries
– Medication lists/records
– Clinical progress notes
– Other resources as available
44
2210/19/2018
Data Sources/Resources for Coding the DRR
Items (cont.)
• Discussions may supplement and/or clarify the information
gleaned from the resident’s medical records, including
discussions with:
– The acute care hospital
– Other staff and clinicians responsible for completing the DRR
– The resident
– The resident’s family/significant other
45
Key Point!
Data in the MDS should be consistent with
information reported in the resident’s medical
record.
46
2310/19/2018
Who Can Code DRR Items?
• The Centers for Medicare & Medicaid Services (CMS) does not
provide guidance on who can or cannot code the DRR items
• Please refer to facility, Federal, and State policies and procedures
to determine which SNF staff members may complete a DRR
• Each facility determines their policies and procedures for
completing the assessments
• Each facility provides resident care according to their unique
characteristics and standards (e.g., resident population)
47
Coding Tips (cont. 1)
• Example of a physician-recommended action that would
take longer than midnight of the next calendar day to
complete:
• –The physician writes an order instructing the clinician to
monitor the medication issue over the next 3 days and call if the
problem persists
48
2410/19/2018
Coding Tips (cont. 2)
• Examples of by midnight of the next calendar day:
– A clinically significant medication issue is identified at 10:00 a.m. on
9/12/2017. The physician-prescribed/-recommended action is completed on
or before 11:59 p.m. on 9/13/2017.
– A clinically significant medication issue is identified at 11:00 p.m. on
9/12/2017. The physician-prescribed / recommended action is completed on
or before 11:59 p.m. on 9/13/2017.
49
N2001 Steps for Assessment
1. Complete a DRR upon admission (start of SNF PPS stay) or as close
to the actual time of admission as possible to identify any
potential or actual clinically significant medication issues
2. Review the medical record documentation to determine whether a
DRR was conducted upon admission (start of SNF PPS stay), or as
close to the actual time of admission as possible, to identify any
potential or actual clinically significant medication issues
50
2510/19/2018
N2003 Steps for Assessment
1. Review the medical record to determine whether the following
criteria were met for any potential and actual clinically significant
medication issues that were identified upon admission:
– Two-way communication between the clinician(s) and the
physician was completed by midnight of the next calendar day,
AND
– All physician-prescribed/recommended actions were completed
by midnight of the next calendar day
51
N2003 Coding Instructions
• Code 0, No: if the facility did not contact the physician and complete
prescribed/recommended actions in response to each identified
potential or actual clinically significant medication issue by midnight
of the next calendar day
• Code 1, Yes: if the facility contacted the physician AND completed
the prescribed/recommended actions by midnight of the next
calendar day after each potential or actual clinically significant
medication issue was identified
52
2610/19/2018
N2001 and N2003 Coding When DRR Is Not
Completed
• If the DRR was not completed upon admission, then N2001
and N2003 are coded with a dash (–)
• CMS expects dash use to be a rare occurrence
53
N2005 Steps for Assessment
• Review the medical record to determine whether the following
criteria were met for any potential and actual clinically significant
medication issues that were identified upon admission or at any
time during the resident’s stay:
– Two-way communication between the clinician(s) and the physician was
completed by midnight of the next calendar day, AND
– All physician-prescribed/recommended actions were completed by
midnight of the next calendar day
54
2710/19/2018
Section GG:
Functional Abilities and Goals
Changes to Section GG: MDS 3.0
• Added Item GG0100. Prior Functioning: Everyday
Activities
• Added Item GG0110. Prior Device Use
• New Code 10, Not attempted due to environmental
limitations (e.g., lack of equipment, weather constraints)
• Goals: Coding goals with “activity not attempted codes” (07,
09, 10, 88) is permissible
• Overall scoring guidance addresses safety, so the word
“safely” was removed from individual items
56
2810/19/2018
Changes to Section GG: MDS (cont. 1)
• Coding and item definitions clarified and aligned:
– “Contact guard” added to definition of code 04, Supervision or
touching assistance
– Eating (Item GG0130A) definition clarified to include the ability to bring food
and liquid to the mouth and swallow food once the meal is placed before
the resident
– Oral hygiene (Item GG0130B) revised to: …The ability to insert and remove
dentures into and from the mouth and manage denture soaking and rinsing
with use of equipment
57
Changes to Section GG: MDS (cont. 2)
• MDS item definitions clarified and aligned:
– Toileting hygiene (GG0130C) revised to: … adjust clothes before
and after voiding or having a bowel movement
– Sit to stand (GG0170D): revised to include wheelchair … from
sitting in a chair, wheelchair, or on the side of the bed
– Wheelchair/scooter: wheelchair and/or scooter
58
2910/19/2018
GG0100
Prior Functioning: Everyday Activities
GG0100. Prior Functioning: Everyday Activities
60
3010/19/2018
GG0100: Coding Instructions
• Code 3, Independent, if the resident completed the activities by himself or herself, with or without
an assistive device, with no assistance from a helper
• Code 2, Needed Some Help, if the resident needed partial assistance from another person to
complete the activities
• Code 1, Dependent, if the helper completed the activities for the resident or the assistance of two
or more helpers was required for the resident to complete the activity
• Code 8, Unknown, if the resident’s usual ability prior to the current illness, exacerbation, or
injury is unknown
• Code 9, Not Applicable, if the activity was not applicable to the resident prior to the current
illness, exacerbation, or injury
61
GG0110.
Prior Device Use
3110/19/2018
GG0110. Prior Device Use
• Complete only at the start of SNF PPS Stay
63
GG0110: Coding Instructions
• Check all devices that apply:
A. Manual wheelchair
B. Motorized wheelchair and/or scooter
C. Mechanical lift
D. Walker
E. Orthotics/Prosthetics
• Check Z, None of the above, if the resident did not use any of the
listed devices or aids immediately prior to the current illness,
exacerbation, or injury
64
3210/19/2018
Overview: GG0130: Self-Care, GG0170: Mobility
GG0130: New Self-Care Items
66
3310/19/2018
GG0170: New Mobility Items
67
GG0130 & GG0170: Steps for Assessment
1. Assess the resident’s self-care and mobility performance based on
direct observation; the resident’s self-report; and reports from clinicians,
care staff, or family reports, documented in the resident’s medical record
during the
• 3-day assessment period
2. Residents should be allowed to perform activities as independently
as possible, as long as they are safe
3. If helper assistance is required because a resident’s performance is
unsafe or of poor quality, score according to amount of assistance
provided
4. For Section GG, a “helper” is defined as facility staff who are direct
employees and facility-contracted employees (e.g., rehabilitation staff,
nursing agency staff)
68
3410/19/2018
GG0130 & GG0170: Steps for Assessment
(cont.)
5. Activities may be completed with or without assistive device(s). Use of
assistive device(s) to complete an activity should not affect coding of the
activity.
6. If the resident’s self-care and mobility performance varies during the
assessment period, record the resident’s usual ability to perform each
activity.
– Do not record the resident’s most independent performance
– Do not record the resident’s most dependent performance
7. Refer to facility, Federal, and State policies and procedures to determine
which SNF staff members may complete an assessment. Resident
assessments are to be done in compliance with facility, Federal, and
State requirements.
69
Usual Status
• Admission (Start of SNF PPS Stay):
• The resident’s functional status should be based on a clinical
assessment of the resident’s performance that occurs soon
after the resident’s admission
• The admission function scores are to reflect the resident’s
admission baseline status prior to any benefit from therapeutic
interventions
• Discharge (End of SNF PPS Stay):
• Code the resident’s discharge functional status based on
a clinical assessment that occurs as close to the resident’s
discharge as possible
70
3510/19/2018
Usual Status (cont.)
• A resident’s functional status can be impacted by the
environment or situations encountered at the facility
• Observing the resident’s interactions with others in different
locations and circumstances is important for a
comprehensive understanding of the resident’s functional
status
• If the resident’s status varies, record the resident’s usual ability
to perform each activity
• Do not record the resident’s best performance and worst
performance; instead, record the resident’s usual performance
71
GG0130 & GG0170: Coding Instructions
• Code the resident’s usual performance for each activity using the
six-point scale:
– Code “06” for Independent
– Code “05” for Setup or clean-up assistance
– Code “04” for Supervision or touching assistance
– Code “03” for Partial/moderate assistance
– Code “02” for Substantial/maximal assistance
– Code “01” for Dependent
72
3610/19/2018
GG0130 & GG0170: Coding Instructions
(cont.)
• If the activity was not attempted during the entire 3-day assessment period,
indicate the reason the activity was not attempted:
– Code “07” for Resident refused
– Code “09” for Not applicable: Resident did not attempt to perform the activity and did
not perform this activity prior to the current illness, exacerbation, or injury
– Code “10” for Not attempted due to environmental limitations (e.g., lack of
equipment, weather constraints)
– Code “88” for Not attempted due to medical condition or safety concerns
73
Definition: GG0130A
• The definition of GG0130A. Eating has been
clarified:
• The ability to use suitable utensils to bring food and/or
liquid to the mouth and swallow food and/or liquid once
the meal is placed before the resident
74
3710/19/2018
GG0130A: Coding Tips
• GG0130A. Eating:
Assesses eating and drinking by mouth only
o If the resident eats and drinks by mouth and relies partially on obtaining nutrition
and liquids via tube feedings or total parenteral nutrition (TPN), code the Eating
item based on the amount of assistance the resident requires to eat and drink by
mouth
o Assistance with tube feedings or TPN is not considered when coding
the Eating item
o If the resident eats finger foods with his or her hands, code based upon the
amount of assistance provided
75
Definition: GG0130C
• The definition of GG0130C. Toileting hygiene has
been clarified:
• – It is “The ability to maintain perineal hygiene, adjust
clothes before and after voiding or having a bowel
movement. If managing an ostomy, include wiping the
opening but not managing equipment.”
76
3810/19/2018
GG0130C: Coding Tips
• Toileting hygiene:
– Includes the tasks of managing undergarments, clothing, and incontinence
products, and performing perineal cleansing before and after voiding or having a
bowel movement
– Can take place before and after use of the toilet, commode, bedpan, or urinal
• If the resident does not usually use undergarments, then
assess the resident’s need for assistance to manage lower-
body clothing and perineal hygiene
• If the resident has an indwelling urinary catheter and has
bowel movements, code the toileting hygiene item based on
the amount of assistance needed by the resident when moving
his or her bowels
77
GG0130E: Coding Tips
• Shower/bathe self:
– Includes the ability to wash, rinse, and dry the face, upper and lower body, perineal area,
and feet
– Does not include washing, rinsing, and drying the resident’s back or hair
– Does not include transferring in/out of a tub/shower
• Assessment of shower/bathe self can take place in a shower or bath, at a sink, or at
the bedside (i.e., sponge bath)
• If the resident bathes himself or herself and a helper sets up materials for
bathing/showering, then code as 05, Setup or clean- up assistance
• If the resident cannot bathe his or her entire body because of a medical condition,
then code shower/bathe self based on the amount of assistance needed to
complete the activity
78
3910/19/2018
Definition: GG0130F. Upper Body Dressing
• The ability to dress and undress above the waist; including
fasteners, if applicable
79
GG0130G. Lower Body Dressing
80
4010/19/2018
Definition: GG0130H
• Definition of GG0130H. Putting on/taking off
footwear:
• The ability to put on and take off socks and shoes or other
footwear that is appropriate for safe mobility; including
fasteners, if applicable
81
GG0130. Discharge Goal: Coding Tips
• Use the six-point scale or ‘activity was not attempted” codes to code the resident’s
Discharge Goal(s). Use of codes 07, 09, 10, or 88 is permissible to code discharge
goal(s).
• For the SNF QRP, a minimum of one self-care or mobility goal must be coded. However,
facilities may choose to complete more than one self-care or mobility discharge goal.
• Use of a dash (–) is permissible for any remaining self-care or mobility goals that were
not coded.
• Using the dash in this allowed instance after the coding of at least one goal does not
affect Annual Payment Update (APU) determination.
82
4110/19/2018
GG0130. Discharge Goal: Coding Tips (cont.)
• Licensed clinicians can establish a resident’s Discharge Goal(s) at the time of
admission based on:
– Resident’s prior medical condition(s)
o Prior and current self-care and mobility status
o Discussions with resident and family concerning discharge goals
– Professional’s standard of practice
– Expected treatments
– Resident motivation to improve
– Anticipated length of stay
– Resident’s planned discharge setting/home
• Goals should established as part of the resident’s care plan
83
GG0130. Discharge Goals: Coding Examples
• Discharge Goal Code Is Higher Than 5-Day PPS Admission
Assessment Performance Code:
– If the clinician and resident determine that the resident is expected to make
gains in function by discharge
• Discharge Goal Code Is the Same as 5-Day PPS Admission
Assessment Performance Code:
– If the clinician and resident determine that the resident is expected to
maintain function and is not anticipated to progress to a higher level
of functioning for an activity
84
4210/19/2018
GG0130. Discharge Goals: Coding Examples
(cont.)
• Discharge Goal Code Is Lower Than 5-Day PPS
Assessment Admission Performance Code
• – The clinician determines that a resident with a progressive
condition is expected to rapidly decline and that receiving
skilled therapy services may slow the decline of function
85
GG0170
Mobility
4310/19/2018
Definition: GG0170A
• Definition of GG0170A. Roll left and right has been
clarified:
• The ability to roll from lying on back to left and right side,
and return to lying on back on the bed
87
GG0170E: Coding Tips
• Chair/bed-to-chair transfer begins with the resident sitting in
a chair or wheelchair or sitting upright at the edge of the
bed and returning to sitting in a chair or wheelchair or sitting
upright at the edge of the bed
• If a mechanical lift is used to assist in transferring a resident
for a chair/bed-to-chair transfer and two helpers are needed to
assist with the mechanical lift transfer, then code as 01,
Dependent, even if the resident assists with any part of the
chair/bed-to-chair transfer
88
4410/19/2018
Changes to GG0170I
• GG0170I. Walk 10 feet includes a skip pattern if the activity did
not occur. If Walk 10 feet is coded as 07, 09, 10, or 88, skip to
item GG0170M (Admission) or GG0170M (Discharge) “1 step
curb.”
• The gateway questions “Does the Resident Walk?”
GG0170H1 (Admission) and GG0170H3 (Discharge) have
been removed.
89
Coding Tips for Walking Items
• Walking activities do not need to occur during one session.
• When coding GG0170 walking items, do not consider the
resident’s mobility performance when using parallel bars.
• The turns included in the items GG0170J (walking with two
turns) are 90-degree turns. The turns may be in the same
direction or may be in different directions.
90
4510/19/2018
GG0170L: Definition
• Definition of GG0170L. Walking 10 feet on uneven
surfaces:
• The ability to walk 10 feet on uneven or sloping surfaces
(indoor or outdoor), such as turf or gravel
91
Definition: GG0170M
• Definition of GG0170M. 1 step (curb): The ability to go up
and down a curb and/or up and down one step
• – Note the skip pattern:
• If the resident’s admission performance is coded 07, 09, 10, or 88
• Skip to GG0170P. Picking up object
92
4610/19/2018
GG0170Q: Coding Tips
• If the resident uses a wheelchair for self- mobility and is not
exclusively transported by others using a wheelchair, then the
gateway wheelchair item
• GG0170Q1. Does the resident use a wheelchair and or
scooter is coded 1, Yes
93
GG0170C: Coding Tips
• Clinical judgment should be used to determine what is considered
a “lying” position for a particular resident
• If the resident’s feet do not reach the floor upon lying to sitting, the
clinician will determine if a bed height adjustment or a footstool is
required
• Back support refers to an object or person providing support for the
resident’s back
• If bed mobility cannot be assessed because of the degree to which the
head of the bed must be elevated because of a medical condition, then
code the activities GG0170A. Roll left and right; GG0170B. Sit to lying;
and GG0170C. Lying to sitting on side of bed as 88, Not attempted due
to medical condition or safety concern
94
4710/19/2018
GG0170RR1 & GG0170SS1. Indicate the Type
of Wheelchair and/or Scooter Used
95
Section GG:
Functional Abilities and Goals
Summary of Changes
4810/19/2018
Section GG: Functional Abilities and Goals
• New item
• GG0100. Prior Functioning: Everyday Activities
97
Section GG: Functional Abilities and Goals
(cont. 1)
• New item
• GG0110. Prior Device Use
98
4910/19/2018
Section GG: Functional Abilities and Goals
(cont. 2)
• GG0130 A-C Item definitions clarified and aligned across all item sets
• 6-point scale:
– Added “contact guard” to definition of code 04, Supervision or touching assistance
– Helper provides verbal cues and/or touching/steadying and/or contact guard
assistance as resident completes activity. Assistance may be provided throughout the
activity or intermittently.
– Added definition to code 09, Not applicable Not attempted and the resident did not
perform this activity prior to current illness, exacerbation of injury to the item set
– Added new code 10, Not attempted due to environmental limitations
• (e.g., lack of equipment, weather constraints)
99
Section GG: Functional Abilities and Goals
(cont. 3)
• Discharge Goals: Updated guidance for coding GG0130 and
GG0170 discharge goals:
• Use of codes 07, 09, 10, or 88 is permissible to code discharge
goal(s)
100
5010/19/2018
Section GG: Functional Abilities and Goals
(cont. 4)
• New item
• GG0130E, GG0130F, GG0130G, & GG0130H
101
Section GG: Functional Abilities and Goals
(cont. 5)
• Skip pattern: Added a skip pattern to GG0170I
walking item if the activity did not occur
• Removed the walking gateway questions:
– Admission: GG0170H1. Does the resident walk?
– Discharge: GG0170H3. Does the resident walk?
102
5110/19/2018
Section GG: Functional Abilities and Goals
(cont. 6)
• New items
• GG0170A,
GG170G, &
GG0170I
103
Section GG: Functional Abilities and Goals
(cont. 7)
• New items
• GG0170L, GG170M, GG0170N, GG0170O, & GG0170P
104
5210/19/2018
Other RAI Updates
• Item B0700 – Makes Self Understood: Never/Rarely and Interviews
• Section C – BIMS Interview – added methods of writing, pointing, sign
language, & cue cards
• Interviews - If not conducted, must still say Yes to Gateway Question-
“Should” interview be conducted, then dash items.
• Do Not complete Staff assessment if interview should have been conducted!
• Tamoxifen – Not to be coded as Chemo, it is a hormonal agent
• Section O – Invasive vs Non-Invasive Vents
105
RAI Manual Updates
RAI Manual updates for October 1, 2018 have been released which
include coding instructions and examples for the new items & other
miscellaneous guidance for existing items. Sections for NEW items are :
• Self-Care and Mobility in Section GG
• Primary Medical Condition in Section I
• Prior Surgery in Section J
• Skin Conditions in Section M
• Drug Regimen Review in Section N
106
5310/19/2018
Questions??
Maureen McCarthy, RN, BS, RAC-MT, QCP-MT, DNS-MT
President, CEO
Phone (Office): 860-321-7413
Email: mmccarthy@celticconsulting.org
www.celticconsulting.org
107
54You can also read