Paediatric rheumatology Identification of 4 subgroups of juvenile dermatomyositis by principal component analysis-based cluster analysis
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Paediatric rheumatology
Identification of 4 subgroups of juvenile dermatomyositis
by principal component analysis-based cluster analysis
J. Zhang1, Y. Xue1, X. Liu2, W. Kuang1, X. Tan1, C. Li1, C. Li1
1
Department of Rheumatology, Beijing Children’s Hospital, National Centre for Children’s Health,
Beijing; 2Nutrition Research Unit, Beijing Paediatric Research Institute, Beijing Children’s Hospital,
Capital Medical University, Beijing, China.
Abstract
Objective
Juvenile dermatomyositis (JDM) is an autoimmune disease characterised by a great heterogeneity in its clinical
manifestations. In this study, we aimed to investigate the association between different clinical subtypes, laboratory
data, and myositis antibodies of JDM.
Methods
A total of 132 JDM patients were enrolled and their medical records were retrospectively reviewed and autoantibodies
tested. Twenty-one variables, including clinical manifestations and laboratory findings, were selected for analysis.
We selected principal component analysis (PCA) as a pre-processing method for cluster analysis to convert the 21
original variables into independent principal components. We then conducted a PCA-based cluster analysis in order
to analyse the association between patient clusters and the clinical data, laboratory data, and myositis autoantibodies.
Results
We identified 4 distinct JDM subgroups by PCA-based cluster analysis, namely: cluster A, JDM patients with arthralgia
and intense inflammation; cluster B, JDM patients with clinical manifestations of vasculitis; cluster C, hypermyopathic
JDM patients; and cluster D, JDM patients with skin involvement. There were significant differences between the 4
groups in serum alkaline phosphatase levels, usage of aggressive immunosuppressive therapy, and autoantibody
expression of anti-mi2, anti-MDA5, anti-Jo1, and anti-PM-Scl100.
Conclusion
We conducted cluster analysis of a cohort of JDM patients and identified 4 subgroups that represented diverse
characteristics in the distribution of laboratory data and myositis autoantibodies, indicating that multidimensional
assessment of clinical manifestations is highly valuable and urgently needed in JDM patients. These subgroups may
contribute to individualised treatments and improved JDM patient prognosis.
Key words
principal component analysis, cluster analysis, juvenile dermatomyositis, autoantibody
Clinical2022
Clinical and Experimental Rheumatology and Experimental Rheumatology 2022; 40: 443-449.Identification of 4 subgroups of JDM / J. Zhang et al.
Junmei Zhang, MD Introduction JDM (4, 5). Patients with juvenile
Yuan Xue, PhD As one of the most prevalent inflam- polymyositis (JPM) were excluded to
Xuanyi Liu, MD
matory myopathies in children, juve- reduce the interference, as JPM has
Weiying Kuang, BD
Xiaohua Tan, MD nile dermatomyositis (JDM) affects already been identified as a distinct
Chao Li, MD 1.9 patients per million children in the subtype with a different pathological
Caifeng Li, PhD United Kingdom (1) and 2.4–4.1 pa- mechanism compared with JDM. Other
Please address correspondence to: tients per million children in the USA myopathies were also excluded. Ethics
Caifeng Li, (2). The mortality rate of JDM in de- approval and informed patient consent
Department of Rheumatology, veloped countries is currently estimated were obtained from patients and their
Beijing Children’s Hospital,
at 2–3% (3). JDM has been proven to guardians.
Nan Li Shi Road 56,
Beijing 100045, China. be of great heterogeneity: the clini-
E-mail: licaifengbch@sina.com cal symptoms are widely diverse and Data extraction
Received on December 1, 2020; accepted include muscle and skin involvement, Data at the time of first hospitalisation
in revised form on February 17, 2021. interstitial lung disease (ILD), arthritis, were collected from the patients’ medi-
© Copyright Clinical and and cardiac damage. cal charts. These included the following
Experimental Rheumatology 2022. Of note, JDM shares criteria with DM. parameters: demographics, IIM-related
The identification of clinical DM phe- clinical manifestations, laboratory find-
notypes tends to be of great significance ings, and immunosuppressive therapy.
for the prognosis and has been the focus We also documented the administration
of extensive research. Bohan and Peter of aggressive immunosuppressive ther-
(4, 5) reported 4 subtypes of DM, and apy, which was defined as a repeated
juvenile DM is one of them; the other corticosteroid impulse therapy for ≥2
three subtypes are DM associated with times. We chose methylprednisolone
malignancy, DM associated with other (MP) for impulse therapy with a dose
connective tissue diseases (CTD), and of 10–20 mg/kg/d, 3–5 days per pulse.
idiopathic DM. The European League
Against Rheumatism (EULAR)/Ameri- Data analysis
can College of Rheumatology (ACR) In recent years, grouping techniques
(6) have validated classification crite- have become prominent analysis meth-
ria for adult and juvenile idiopathic in- ods. As one of the most popular meth-
flammatory myopathies (IIM) and their ods of unsupervised learning, cluster
major subgroups. However, studies analysis has shown great advantage in
dedicated to identifying the subtypes identifying subgroups by similar char-
of DM, and especially of JDM, are still acteristics (7). In this study, cluster
scarce. analysis was performed to achieve sub-
We designed this study to investigate typing in JDM patients. Four critical
the association between different clini- steps were performed in the statistical
cal subtypes, laboratory data, and my- analysis, including selection of clini-
ositis antibodies in JDM. In this study, cal variables, cluster analysis of these
we adopted a principal component anal- variables to explore the relationships
ysis (PCA)-based cluster analysis as an between them, PCA to reduce interac-
exploratory method, which proved to tions between the variables, and cluster
be suitable for identifying JDM sub- analysis of patients based on the PCA-
types. Four distinct JDM subtypes were transformed data.
identified and then validated by detect- Variables with abnormal distribution
ing significant differences in immune- were expressed as median and then
suppressive therapies, laboratory data, compared using non-parametric tests.
and expression of myositis antibodies. Categorical data are presented as num-
bers (percentages), and the chi-square
Method test was utilised.
Population
A total of 132 patients diagnosed with Variable selection
JDM from inpatient wards of the Bei- We selected 21 variables frequently
Funding: this work was supported by the jing Children’s Hospital between June found in the JDM and detected myositis
Capital’s Funds for Health Improvement 2015 and September 2018 were en- antibodies and then included these orig-
and Research (CFH2018-2-2093). rolled in our study. The Bohan and inal variables in the analysis (Table I).
Competing interests: none declared. Peter criteria were applied to diagnose The 21 variables were included in the
444 Clinical and Experimental Rheumatology 2022Identification of 4 subgroups of JDM / J. Zhang et al.
Table I. Clinical characteristics and an- which can be verified by clustering. (25.0%). The median CK level was
tibody positive rate of 132 patients with Western blotting and 16 items of the 163.0 U/L (11.0–18397.0 U/L), and
juvenile dermatomyositis.
anti-myositis spectrum kit (European) alkaline phosphatase (ALP) level was
Patients, n (%) were used to detect serum antibodies 144.1±84.0 U/L. A total of 75 (50.3%)
(n=132) in 132 patients, including anti-Mi-2α, patients received repeated corticoster-
anti-Mi-2 β, anti-TIF1-γ, anti-MDA5, oid impulse therapy.
Demographics
Female 67 (50.8)
anti-NXP2, anti-SAE1, anti-Ku, anti-
Age at onsetb, years 8.1 (3.7) PM-Scl100, anti-PM-Scl75, anti-Jo-1, CATPCA
Course of diseasea, months 10.0 (20.7) anti-SRP, anti-PL-7, anti-PL-12, anti- Twenty-one independent principal
Clinical featuresa EJ, anti-OJ, anti-Ro-52. Continuous components were obtained by CAT-
Heliotrope rash 98 (74.2) variables, such as age at onset and CK PCA of the original variables. These
Gottron sign 102 (77.3)
Muscle weakness 109 (82.6)
level, were standardised by evaluating principal components explained all the
Myalgia/muscle tenderness 21 (15.9) the distribution, mean value, median variance and were included in the clus-
Eyelid swelling 21 (15.9) value, and extremum of the continu- ter analysis.
Calcinosis cutis 20 (15.2) ous variables. Then, the variables were
Digital ulcer 7 (5.3)
Fever 46 (34.8) standardised by removing the mean and Cluster analysis
Raynaud’s phenomenon 3 (2.3) scaling unit variance. Hierarchical cluster analysis was con-
Cough 33 (25.0) ducted on the 132 patients on the basis
Periungual telangiectasia 26 (19.7) Identification of distinct clusters of CATPCA. Figure 1 displays the re-
Arthritis/arthralgia 33 (25.0)
Dysphagia 12 (9.1) We performed categorical PCA (CATP- sults of the hierarchical cluster analysis
Choking cough 15 (11.4) CA) to detect critical features and reduce of the 21 clinical variables. Figure 2
Hoarseness 6 (4.5) dimensionality of the original variables, shows the process of clustering of the
Alopecia 4 (3.0)
for which our data was mixed with both patients. On the basis of the equiparti-
WBCc 8.4 (3.6)
Fatigue 109 (82.6) continuous and binary variables. By tion principle, the clustering resulted in
Movement limitation 5 (3.8) reducing variances or eigenvalues, the 4 clusters.
Chiblian rash 2 (1.5) original variables were transformed into
Laboratory data 21 independent components for cluster Relationship between ALP,
Creatine kinase levelbU/L 163.0 (119.0)
ALP levelc,U/L 144.1 (84.0)
analysis. Agglomerative clustering algo- immunosuppressive therapy,
Repeated corticosteroid impulse 73 (55.3) rithms were applied to cluster variables. antibodies and clusters
therapy Hierarchical clustering hierarchically To validate the classification, we ex-
Antibody combined clusters with the smallest amined the relationship between the
Mi2 18 () distances (7). Through this process, the clusters and laboratory data, immuno-
TIFγ 26 (19.7)
MDA5 16 (12.1)
Ward method was selected to decrease suppressive therapy, and expression of
NPX2 30 (22.7) the total within-cluster variance; then, antibodies. These parameters were not
SAE1 1 (0.8) squared Euclidean distance was applied used for clusters. The results of this
Ku 8 (6.1) for similarity measurement. For con- analysis are presented in Table II. There
PMScl100 7 (5.3)
PMScl75 9 (16.8)
tinuous normally distributed variables, were significant differences between
Jo1 3 (2.3) differences between the clusters were the 4 groups in serum ALP levels, us-
SRP 8 (6.1) compared using non-parametric tests in- age of aggressive immunosuppressive
PL7 3 (2.3) cluding the Kruskal-Wallis test, and the therapy, and autoantibody expression
PL12 3 (2.3)
EJ 0 (0.0) chi-square test or Fisher’s exact test was of anti-mi2, anti-MDA5, anti-Jo1, and
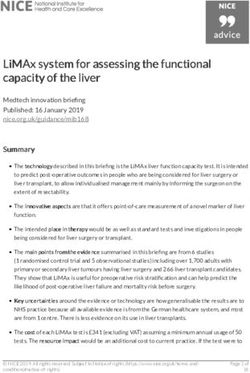
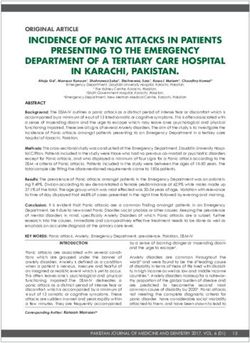
OJ 5 (3.8) used for categorical variables. pIdentification of 4 subgroups of JDM / J. Zhang et al. Fig. 1. Dendrogram showing the process and results of hierarchical cluster analysis of 21 variables. The horizontal axis represents the rescaled distance cluster combination in which the largest distance between clusters was marked as 25. Horizontal lines on the left represent the clustering observations, which in this case are clinical variables. Fig. 2. Agglomerative hierarchical clustering of the132 dermatomyositis patients based on categorical principal components analysis. Here, we present the process of combination from 21 clusters to 1 cluster. The number in the parenthesis indicates the number of patients included in each cluster. tribution of laboratory data and myosi- To detect critical features and reduce the integrity of data, PCA outstands tis autoantibodies, which indicated that the dimensionality of the original vari- other pre-processing methods, includ- multidimensional assessment of clinical ables, PCA was selected as a pre-pro- ing factor analysis (7), PCA (8) and as- manifestations is valuable and urgently cessing method for cluster analysis. sociation analysis (9), and ensures that needed in JDM patients. First, as an autoimmune disease, JDM these less prevalent symptoms are not In our study, a PCA-based cluster is prominently characterised by multi- missed due to methodological flaws. analysis of variables was applied, re- ple-system damage and heterogeneity Second, PCA was conducive to effec- sulting in a dendrogram in which vari- of symptoms. Some symptoms are less tuate independence of variables and ables with similar distribution patterns prevalent but significant in the clinical eliminate noisy variables. Independ- were categorised into the same groups. practice. With the ability to maintain ence of the variables, as a prerequisite 446 Clinical and Experimental Rheumatology 2022
Identification of 4 subgroups of JDM / J. Zhang et al.
for cluster analysis, was a critical fac- Table II. Clinical characteristics of 132 patients with juvenile dermatomyositis according
tor for the reliability of clustering (10). to the clusters identified using principal component analysis-based cluster analysis.
Clinically, the original variables were Group A Group B Group C Gourp D p-value
limited in independence, which led to (n=52) (n=24) (n=26) (n=30)
unsatisfactory results by direct cluster
analysis (11). The results of our study Demographics
Female (%) 26 (50.0) 14 (58.3) 14 (53.8) 13 (43.3) 0.726
also indicated that PCA-based cluster Age at onseta, years 9.1 (3.2) 7.8 (2.5) 7.5 (3.4) 6.8 (3.6) 0.045*
analysis would be appropriate for sub- Course of diseaseb, months 10.1 (7.2) 11.4 (3.5) 14.0 (3.7) 9.7 (8.1) 0.634
grouping JDM, a heterogeneous auto- Clinical features
immune disease. Heliotrope rash (%) 42 (80.8) 14 (58.3) 17 (68.0) 24 (80.0) 0.031*
In our study, the 4 groups identified Gottron sign (%) 40 (76.9) 16 (66.7) 20 (80.0) 23 (76.7) 0.688
were consistent with some specific sub- Muscle weakness (%) 23 (44.2) 3 (12.5) 1 (4.0) 9 (30.0) 0.001*
Myalgia/muscle tenderness (%) 9 (17.3) 5 (20.8) 2 (8.0) 5 (16.7) 0.610
types referred to in previous studies and Blephoraedema (%)% 5 (9.5) 4 (16.7) 4 (15.4) 8 (26.7) 0.249
criteria. The characteristics of cluster Calcinosis cutis (%) 7 (13.5) 1 (4.2) 0 (0.0) 2 (6.7) 0.165
B (JDM with vasculitis) and cluster C Digital ulcer (%) 1 (1.9) 1 (4.2) 0 (0.0) 1 (3.3) 0.762
(hypermyopathic JDM) were in accord- Fever (%) 21 (40.4) 10 (41.7) 4 (19.2) 10 (33.3) 0.036*
Raynaud’s phenomenon (%) 1 (1.9) 0 (0.0) 2 (7.7) 0 (0.0) 0.169
ance with the 1975 classification crite- Cough (%) 16 (30.8) 9 (37.5) 6 (23.1) 2 (6.7) 0.024*
ria for DM proposed by Bohan and Pe- Periungual telangiectasia (%) 11 (30.8) 3 (12.5) 8 (30.8) 4 (13.3) 0.307
ter (4, 5), as well as with Sontheimer’s Arthritis/arthralgia (%) 16 (30.8) 8 (33.3) 5 (19.2) 4 (13.3) 0.220
Dysphagia (%) 5 (9.6) 1 (4.2) 2 (7.7) 4 (13.3) 0.700
standalone classification criteria for de-
Choking (%) 7 (13.5) 2 (8.3) 2 (7.7) 4 (13.3) 0.825
fining amyopathic DM (12). Hoarseness (%) 3 (5.8) 0 (0.0) 1 (3.8) 2 (6.7) 0.648
The presence of various autoantibodies Lipsotrichia (%) 3 (5.8) 0 (0.0) 1 (3.8) 2 (6.7) 0.648
can often be observed in JDM, contrib- Laboratory data
uting to the classification, diagnosis, Creatine kinase level, U/L 137.0 (1423.6) 135.5 (1127.6) 204.5 (1112.8) 180.5 (1345.7) 0.886
and emergence of particular comor- ALP level, U/L 97.5 (118.7) 148.0 (163.7) 130.0 (158.7) 124.5 (159.0) 0.025*
bidities. According to previous studies, Usage of aggressive 21 (40.4) 20 (83.3) 11 (42.3) 21 (70.0) 0.001*
immunosuppressive therapy
anti-Mi2 is associated with classic skin
features such as heliotrope rash, Got- Antibody
Mi2 8 (6.1) 1 (4.2) 1 (3.8) 8 (26.7) 0.011*
tron papules, shawl sign, V-sign, pho- TIFγ 10 (19.2) 3 (12.5) 6 (23.1) 7 (23.3) 0.748
tosensitivity, and cuticular overgrowth MDA5 11 (21.1) 1 (4.2) 2 (7.7) 2 (6.7) 0.038*
(13); anti-MDA5 is associated with NPX2 10 (19.2) 6 (25.0) 7 (26.9) 7 (23.3) 0.875
ulcerations over areas such as lateral SAE1 1 (1.9) 0 (0.0) 0 (0.0) 0 (0.0) 0.673
Ku 5 (9.6) 1 (4.2) 2 (7.7) 0 (0.0) 0.343
nailfolds and elbows, and Gottron pap- PMScl100 2 (3.8) 4 (16.7) 1 (3.8) 0 (0.0) 0.044*
ules, oral mucosal pain, tender palmar PMScl75 3 (5.8) 1 (4.2) 2 (7.7) 3 (10.0) 0.835
papules, and ILD (subacute or rapidly Jo1 0 (0.0) 0 (0.0) 0 (0.0) 3 (10.0) 0.016*
SNP 5 (9.6) 1 (4.2) 1 (3.8) 1 (3.3) 0.592
progressive) (14); anti-TIF1γis most
PL7 2 (3.8) 1 (4.2) 1 (3.8) 0 (0.0) 0.707
frequently observed in patients with PL12 0 (0.0) 1 (4.2) 0 (0.0) 0 (0.0) 0.522
palmar hyperkeratotic papules, malig- EJ 1 (1.9) 0 (0.0) 0 (0.0) 0 (0.0) 1.000
nancy, and psoriasis-like lesions (15); OJ 1 (1.9) 3 (12.5) 0 (0.0) 1 (3.3) 0.090
RO52 12 (23.1) 11 (45.8) 7 (26.9) 14 (46.7) 0.073
anti-NXP2 is associated with periph-
eral oedema, dysphagia, myalgia, cal-
cinosis, and malignancy (16); and anti- a
Values are expressed as medians (interquartile ranges).
Jo1 is associated with antisynthetase
b
Values are expressed as the mean (standard deviation).
syndrome and mechanic’s hands (17,
18), while anti-PM-Scl100 is most B (JDM patients with clinical manifes- pathic JDM patients). Therefore, the
frequently observed in patients with tations of vasculitis including RP) and results of our study confirm the find-
Raynaud’s phenomenon (RP) and ar- cluster A (JDM patients with arthralgia ings of previous studies.
thritis (19, 20). In our study, we found and intense inflammation), and anti- Besides autoantibodies, our results
that anti-MDA5, anti-PMScl100, anti- MDA5 had the highest positive rate in also indicate that the distribution of
Jo1, and Anti-Mi2 showed significant cluster A (JDM patients with arthralgia clinical manifestations is in accordance
differences across the 4 identified and intense inflammation including with previously reported data. Through
clusters (pIdentification of 4 subgroups of JDM / J. Zhang et al.
telangiectasia were also integrated to- JDM patients) and include choking, it possible to distinguish diverse phe-
gether, shedding light on homologous hoarseness, dysphagia, muscle weak- notypes and demonstrate potential dis-
pathological mechanisms among heter- ness, and myalgia. Cluster C also ease pathogenesis. The cluster analysis
ogenous symptoms. showed a relatively high rate of ag- identified 4 subgroups, all of which fit
Cluster A (JDM patients with arthralgia gressive immunosuppressive therapy well with the context of previous stud-
and intense inflammation) is character- (42.3%), and the CK level ranked the ies and literature. Novel subgroups of
ised by prominent symptoms of active first among the 4 clusters despite an clinical features were also presented for
inflammation, including higher WBC in insignificant difference (median of CK further exploration. These subgroups
peripheral blood, fever, and arthralgia. level was 204.5 U/L, p=0.886). The may contribute to individualised treat-
Cough is also categorised into cluster positive rate of anti-NXP2 was the ments and improved patient prognosis
A, indicating potential lung involve- highest in this cluster, although it failed in the future.
ment. However, cluster A showed less to show a significant difference, which
muscle involvement and demonstrated was consistent with the clinical mani- References
more features of amyopathic dermato- festations. 1. SYMMONS DP, SILLS JA, DAVIS SM: The in-
cidence of juvenile dermatomyositis: results
myositis (ADM) (21). Anti-MDA5 was Cluster D (JDM patients with skin in- from a nation-wide study. Br J Rheumatol
with the highest positive rate in this volvement) was characterised by skin 1995; 34: 732-6.
cluster, which partially explains such involvement and blephoraedema. The 2. MENDEZ EP, LIPTON R, RAMSEY-GOLDMAN
a distribution. The clinical features positive rate of Anti-Mi2 took the lead R et al.: NIAMS Juvenile DM Registry Phy-
sician Referral Group. US incidence of ju-
of ADM patients with positive anti- of the 4 clusters, which explains the dis- venile dermatomyositis, 1995–1998: results
MDA5 antibody have been reported tribution pattern, as anti-Mi2 is closely from the National Institute of Arthritis and
previously and matched with our find- associated with skin involvement (13).. Musculoskeletal and Skin Diseases Registry.
Arthritis Rheum 2003; 49: 300-5.
ings (22, 23). With aggressive progres- We also found that serum ALP levels
3. HUBER A, FELDMAN BM: Long-term out-
sion of ILD, the prognosis is reported to were significantly different among the comes in juvenile dermatomyositis: how did
be unfavourable, with a 40% mortality 4 clusters, and cluster B had the high- we get here and where are we going? Curr
rate (24). est median level of serum ALP of 148.0 Rheumatol Rep 2005; 7: 441-6.
4. BOHAN A, PETER JB: Polymyositis and der-
Cluster B patients (JDM patients with U/L. As an enzyme detected in osteo- matomyositis (first of two parts). N Engl J
clinical manifestations of vasculitis) blasts in the 1980s, ALP demonstrates Med 1975; 292: 344-7.
tend to be conspicuous due to symp- higher plasma activity with active bone 5. BOHAN A, PETER JB: Polymyositis and der-
toms of vasculitis, including Raynaud’s turnover (27). Moreover, ALP repre- matomyositis (second of two parts). N Engl J
Med 1975; 292: 403-7.
phenomenon, digital ulcer, and peri- sents a direct indicator of vascular cal- 6. LUNDBERG IE, TJARNLUND A, BOTTAI M et
ungual telangiectasia. Calcinosis cutis, cification (28-30). As calcinosis cutis al.: 2017 European League Against Rheu-
which is more commonly found in chil- was also included in cluster B, the high- matism/American College of Rheumatology
dren and adolescents, is also included est level of ALP seems to be a reflection classification criteria for adult and juvenile
idiopathic inflammatory myopathies and their
in this cluster. Raynaud’s phenomenon of calcium and phosphorus metabolism major subgroups. Arthritis Rheumatol 2017;
is one of the most prevalent symptoms in JDM patients and is worthy of fur- 69: 2271-82.
in the mixed connective tissue disease. ther exploration. 7. IZENMAN AJ: Modern Multivariate Statisti-
cal Techniques: Regression, Classification,
Digital ulcer and periungual telangiec- There are also some limitations to our and Manifold Learning. New York, NY:
tasia are often found in systemic scle- study. As a retrospective study, the Springer; 2006: 996.
rosis (SSc). The highest positive rate identified 4 clusters should be vali- 8. RENNARD SI, LOCANTORE N, DELAFONT B
of anti-PM-Scl100 in cluster B was in dated through a long-term prospective et al.: Identification of five chronic obstruc-
tive pulmonary disease subgroups with dif-
accordance with the feature of variable follow-up. We are planning to conduct ferent prognoses in the ECLIPSE cohort
distribution. Anti-PM-Scl100 was gen- a prospective study on the basis of the using cluster analysis. Ann Am Thorac Soc
erally found in patients with PM, DM, current work and explore specific sub- 2015; 12: 303-12.
SSc, and other connective diseases and types including ILD in cluster A, ac- 9. BURGEL P-R, PAILLASSEUR J-L, CAILLAUD D
et al.: Clinical COPD phenotypes: a novel ap-
most frequently found in overlap syn- companied CTD in cluster B, or ma- proach using principal component and cluster
dromes of SSc with PM or DM (24-26). lignancy in clusters C and D. Besides, analyses. Eur Respir J 2010; 36: 531-9.
The distribution pattern of variables in independent cohorts with larger sample 10. KIM JJ, MANDELLI L, LIM S et al.: Associa-
tion analysis of heat shock protein 70 gene
cluster B indicated other accompanying scales are also necessary to validate the polymorphisms in schizophrenia. Eur Arch
CTD. Though with minimal muscle in- reliability of the classification described Psychiatry Clin Neurosci 2008; 258: 239-44.
volvement, cluster B showed the maxi- in our study. 11. ZHU H, WU C, JIANG N et al.: Identification of
mal rate of aggressive immunosuppres- Hereby, we applied cluster analysis to 6 dermatomyositis subgroups using principal
component analysis-based cluster analysis.
sive therapy (83.3%), which may be a cohort of JDM patients for the first Int J Rheum Dis 2019; 22: 1383-92.
due to additional immunosuppressive time and explored the intrinsic asso- 12. CONCHA JSS, TARAZI M, KUSHNER CJ,
treatment required for the other CTD ciation between specific antibodies GAFFNEY RG, WERTH VP: The diagnosis
and classification of amyopathic dermatomy-
gathered in cluster B. and clusters of clinical symptoms. The
ositis: a historical review and assessment of
Symptoms related to myopathy pre- study included 132 JDM patients with existing criteria. Br J Dermatol 2019; 180:
dominate in cluster C (hypermyopathic myositis antibodies measured, making 1001-8.
448 Clinical and Experimental Rheumatology 2022Identification of 4 subgroups of JDM / J. Zhang et al.
13. MURO Y, SUGIURA K, AKIYAMA M: Cutane- ositis. J Am Acad Dermatol 2018; 78: 769-75. PRUIJN GJ: Cell and molecular biology of the
ous manifestations in dermatomyositis: key 19. MARGUERIE C, BUNN CC, COPIER J et al.: exosome: how to make or break an RNA. Int
clinical and serological features – a compre- The clinical and immunogenetic features of Rev Cytol 2006; 251: 159-208.
hensive review. Clin Rev Allergy Immunol patients with autoantibodies to the nucleolar 25. MAHLER M, BLÜTHNER M, POLLARD KM:
2016; 51: 293-302. antigen PM-Scl. Medicine 1992; 71: 327-36. Advances in B-cell epitope analysis of au-
14. FIORENTINO D, CHUNG L, ZWERNER J et al.: 20. HAUSMANOWA-PETRUSEWICZ I, KOWAL- toantigens in connective tissue diseases. Clin
The mucocutaneous and systemic phenotype SKA-OLEDZKA E, MILLER FW et al.: Clini- Immunol 2003; 107: 65-79.
of dermatomyositis patients with antibod- cal, serologic, and immunogenetic features in 26. BROUWER R, VREE EGBERTS WT, HENGST-
ies to MDA5 (CADM-140): a retrospective Polish patients with idiopathic inflammatory MAN GJ et al.: Autoantibodies directed to
study. J Am Acad Dermatol 2011; 65: 25-34. myopathies. Arthritis Rheum 1997; 40: 1257- novel components of the PM/Scl complex,
15. FIORENTINO DF, KUO K, CHUNG L et al.: 66. the human exosome. Arthritis Res 2002; 4:
Distinctive cutaneous and systemic features 21. EUWER RL, SONTHEIMER RD: Amyopathic 134-8.
associated with antitranscriptional interme- dermatomyositis (dermatomyositis sine my- 27. GARRETT G, SARDIWAL S, LAMB EJ, GOLD-
diary factor-1c antibodies in adults with der- ositis): presentation of six new cases and re- SMITH DJ: PTH – a particularly tricky hor-
matomyositis. J Am Acad Dermatol 2015; 72: view of the literature. J Am Acad Dermatol mone: why measure it at all in kidney patients?
449-55. 1991; 24: 959-66. Clin J Am Soc Nephrol 2013; 8: 299-312.
16. ROGERS A, CHUNG L, LI S et al.: Cutaneous 22. FIORENTINO D, CHUNG L, ZWERNER J, RO- 28. TONELLI M, CURHAN G, PFEFFER M et al.:
and systemic findings associated with nuclear SEN A, CASCIOLA-ROSEN L: The mucocuta- Relation between alkaline phosphatase, se-
matrix protein 2 antibodies in adult dermato- neous and systemic phenotype of dermato- rum phosphate, and all-cause or cardiovascu-
myositis patients. Arthritis Care Res 2017; myositis patients with antibodies to MDA5 lar mortality. Circulation 2009; 120: 1784-92.
69: 1909-14. (CADM-140): a retrospective study. J Am 29. ABRAMOWITZ M, MUNTNER P, COCO M et
17. MURO Y, SUGIURA K, AKIYAMA M: Cutane- Acad Dermatol 2011; 65: 25-34. al.: Serum alkaline phosphatase and phos-
ous manifestations in dermatomyositis: key 23. HAMAGUCHI Y, KUWANA M, HOSHINO K et phate and risk of mortality and hospitaliza-
clinical and serological features – a compre- al.: Clinical correlations with dermatomyosi- tion. Clin J Am Soc Nephrol 2010; 5: 1064-71.
hensive review. Clin Rev Allergy Immunol tis-specific autoantibodies in adult Japanese 30. KRISHNAMURTHY VR, BAIRD BC, WEI G,
2016; 51: 293-302. patients with dermatomyositis: a multicenter GREENE T, RAPHAEL K, BEDDHU S: Asso-
18. CONCHA JSS, MEROLA JF, FIORENTINO D, cross-sectional study. Arch Dermatol 2011; ciations of serum alkaline phosphatase with
WERTH VP: Re-examining mechanic’s hands 147: 391-8. metabolic syndrome and mortality. Am J Med
as a characteristic skin finding in dermatomy- 24. SCHILDERS G, van DIJK E, RAIJMAKERS R, 2011; 124: 566 e1-7.
Clinical and Experimental Rheumatology 2022 449You can also read