Pelvic inflammatory disease: The importance of aggressive treatment in adolescents - Cleveland Clinic Journal of ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

REVIEW
ELLEN S. ROME, M D , M P H
Head, Section of Adolescent Medicine, Cleveland
Clinic; Assistant Professor, Ohio State University
School of Medicine; Clinical Instructor, Case Western
Reserve University School of Medicine.
Pelvic inflammatory disease:
The importance of aggressive
treatment in adolescents
ABSTRACT ELVIC INFLAMMATORY DISEASE (PID)
causes more morbidity in young women
Pelvic inflammatory disease (PID), an infection of the of reproductive age than all other serious infec-
female genital tract, presents a number of difficult tions combined. Nonetheless, PID and its
challenges in diagnosis and management. Adolescents in major sequelae of tubal scarring, chronic pelvic
particular require aggressive care of PID to prevent the pain, and infertility are preventable if physi-
long-term sequelae of chronic pelvic pain and infertility. cians diagnose it early and treat it aggressively.
This article reviews the etiology, microbiology, diagnosis, Unfortunately, many young women, and
and management of PID, with an emphasis on treating especially adolescents, delay seeking care and
adolescents with PID. fail to comply with treatment. And, as the
Centers for Disease Control and Prevention
KEY POINTS noted in its 1998 Guidelines for the Treatment
of Sexually Transmitted Diseases,1 many cases
A recent study found that many clinicians were not of PID go undiagnosed because both patients
following specific CDC recommendations for PID, such as and physicians fail to recognize the implica-
those concerning hospitalization of adolescents. tions of mild, nonspecific symptoms.
This article describes the diagnosis and
treatment of PID, with a special emphasis on
Clinicians should consider the diagnosis of PID in any
adolescents, the age group most at risk.
adolescent or young woman with abdominal pain, but also
when mild or nonspecific symptoms or signs (eg, abnormal • W H O GETS PID?
bleeding, dyspareunia, or vaginal discharge) are present.
PID occurs in 1% of women ages 15 to 25 in
In caring for patients suspected of having PID, especially the United States, 2 ' 3 and of the 1 million
adolescents, physicians should establish trust by explaining women who develop PID annually, approxi-
patient confidentiality before taking a sexual history. mately 200,000 require hospitalization. Major
surgical procedures are required as a conse-
Most cases of PID are diagnosed based on clinical criteria, quence of infection in over 100,000 women.4
although laparoscopy remains the gold standard for The annual cost in this country was over $4-2
billion in 1990 and is expected to exceed $10
diagnosis.
billion by the year 2000. 4
For many reasons, adolescents remain the
group at highest risk for sexually transmitted
diseases and PID. Westrom 5 found that 15-
year-old girls had a risk of 1:8 for PID, where-
as 16-year-old girls had a risk of 1:10, and 24-
year-old women had a risk of 1:80.
C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E VOLUME 65 • NUMBER 7 JULY / A U G U S T 1998 343
Downloaded from www.ccjm.org on January 23, 2022. For personal use only. All other uses require permission.
PELVIC INFLAMMATORY
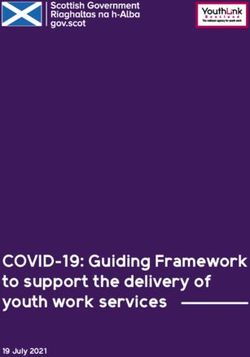
Adolescents display a combination of Use of prophylactic antibiotics. This
physiologic (FIGURE 1) and sociologic factors increased risk may be reduced with prophylac-
that account for this increased risk. tic use of antibiotics at insertion; preliminary
data suggest that use of doxycycline 200 mg
Physiologic f a c t o r s orally 1 hour prior to IUD insertion and then
Physiologically, the adolescent may have low daily for 2 days after insertion may decrease
levels of protective antibodies in the local the risk of PID.15
immune system due to lack of previous expo-
sure to the various pathogens. 6 Also, estro- Sociologic f a c t o r s
genic dominance and cervical ectopy (colum- Sociologically, adolescent risk behaviors tend
nar epithelium on the ectocervix) in postpu- to be multifactorial and to occur in clusters.
bertal girls enhance risk. The cervical mucus That is, risk breeds risk—and infection. A
may be more penetrable in this age group.7 teen who drinks alcohol or uses drugs is more
Adolescents ages 15 to 19 have a higher likely to have unprotected sex, increasing the
prevalence of Neisseria gonorrhoeae and risk of acquiring a sexually transmitted disease,
Chlamydia trachomatis than is seen in older age and teens who engage in one risky behavior
groups. are more likely to participate in other risky
Menses increases the risk of P I D , possi- behaviors. Teens who initiate sexual activity
bly due to the spread of infection by retrograde at younger ages are less likely to use condoms
flow from the uterus out to the fallopian tubes, and are more likely to have multiple partners,
shown to occur in 2 5 % of healthy women. even by serial monogamy, thereby increasing
Vaginal douching has also been shown to their risk of sexually transmitted diseases and
increase the risk of PID. 8 - 1 0 In a study of 131 PID.16,17
women ages 18 to 40 after a first episode of
PID, as compared with 294 control subjects • PATHOGENESIS OF PID
with no history of PID from the same patient
population, women who douched had a rela- PID is polymicrobial in origin. In the United
tive risk of acquiring PID of 2.1 ( 9 5 % confi- States, C trachomatis has been isolated in 2 5 %
Vaginal dence interval 1.2-3.9). Those who douched to 4 0 % of cases, N gonorrhoeae in 3 0 % to 50%,
once weekly increased their relative risk to 3.9 and various other anaerobes and facultative
douching ( 9 5 % CI, 1 . 4 - 1 0 . 9 ) . 8 T h e relative risk aerobes in fallopian tube samples in 2 5 % to
increases P I D increased further to 7.9 ( 9 5 % CI, 2.6-24.3) 50% of women with acute PID. 18 Anaerobes
for those women who cited infection as the include Bacteroides, Pepto streptococcus, and
risk reason for douching; in this group, douching Peptococcus; facultative bacteria include
may be a marker of infection, rather than a Gardnerella vaginalis, Streptococcus, Escherichia
causative factor. Possible mechanisms of coli, and Haemophilus influenzae. Cervical recov-
action for the increased risk of PID include ery of N gonorrhoeae has been found in as many
upward spread of a lower genital tract infec- as 8 1 % of women with PID. 19 However, the use
tion by mechanical pressure and creation of a of culdocentesis and laparoscopy to obtain cul-
more hospitable environment for infection tures from the fallopian tubes or the peritoneal
through altered vaginal pH. cavity, or both, has shown that the presence of
Insertion of intrauterine devices. Despite pathogenic bacteria in the endocervix does not
earlier studies implicating specific intrauterine indicate that such bacteria are associated with
devices (IUDs) as a possible risk factor for salpingitis. When gonococcal salpingitis
nongonococcal, nonchlamydial PID, 11 - 12 a occurs, symptoms develop within 7 days of
more recent review argued against the IUD as menses in up to 6 5 % to 75% of patients.
a significant risk factor. 13 However, insertion
of an IUD may introduce infection.1^1 Since Bacterial vaginosis
adolescents are more likely to have multiple In the past 10 years, bacterial vaginosis has
partners, even with serial monogamy, the IUD been shown to be associated with PID. 2 - 20 " 22
is not an ideal form of contraception due to In 9 ( 2 9 % ) of 31 women with laparoscopical-
the risk of infection with insertion. ly confirmed acute PID, bacterial vaginosis
370 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E VOLUME 65 • NUMBER 7 JULY / A U G U S T 1998
Downloaded from www.ccjm.org on January 23, 2022. For personal use only. All other uses require permission.
Physiological factors in pelvic i n f l a m m a t o r y
disease (PID) in adolescents
•Retrograde menstrual f l o w
May spread infection,
increasing the risk of PID
• I n s e r t i o n of
intrauterine device
Possible risk factor for
nongonococcal and
nonchlarnydial PID •Estrogen dominance
Unopposed estrogen
- can occur in anovulatory
cycles, common in young
•Cervical mucus teenage girls; this can
May be more lead to cervical ectopy
penetrable in
adolescents
•Bacterial vaginosis •Cervical ectopy
Associated bacteria found The presence of
in the endometrium are columnar epithelium
etiologic agents for upper in the ectocervix
genital tract infection — enhances risk in
postpubertal girls
•Vaginal douching
May increase the risk of • L o w levels o f a n t i b o d i e s
PID by causing upward Adolescents lack previous
spread of lower genital exposure to the various
tract infection via pathogens
mechanical pressure, and
by altering the vaginal pH,
creating a hospitable
environment for infection
FIGURE 1
with histologic endometritis was detected by histologic endometritis. The researchers con-
endometrial biopsy.20 Hillier et al 21 confirmed cluded that the bacteria associated with bac-
that organisms such as Prevotella bivia, terial vaginosis, when found in the endometri-
Peptostreptococcus species, and Mycoplasma um, are etiologic agents for upper genital tract
hominis associated with bacterial vaginosis infection independent of gonococcal or
were among the pathogens associated with chlamydial infection.
C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E VOLUME 65 • NUMBER 7 JULY / A U G U S T 1998 343
Downloaded from www.ccjm.org on January 23, 2022. For personal use only. All other uses require permission.
PELVIC INFLAMMATORY
: DISEASE
•
ROME
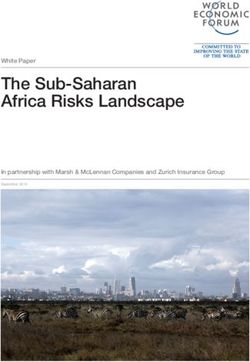
TABLE 1 • DIAGNOSIS OF ACUTE PID
Major and minor criteria Clinicians should consider the diagnosis of
f o r t h e diagnosis of acute pelvic PID in any adolescent girl with abdominal
i n f l a m m a t o r y disease pain. Those clinicians who do not provide
All three of the following must be present: gynecologic care to their patients should know
when to refer patients for further evaluation.
Lower abdominal pain
Pregnancy, either normal or ectopic, must also
Cervical motion tenderness
be considered in the differential diagnosis.
Adnexal tenderness (may be unilateral)
Because many cases of PID go unrecog-
Plus at least one of the following: nized, clinicians should have a low threshold
Temperature > 38°C for suspecting PID, especially in adolescent
White blood cell count > 10,500/mm3 and young adult women who present with
Purulent material obtained by culdocentesis mild or nonspecific symptoms or signs (eg,
Pelvic mass on bimanual exam or sonogram abnormal bleeding, dyspareunia, vaginal dis-
Sedimentation rate > 15 mm/hour
charge).
Gram-negative intracellular diplococci on Gram's stain
Monoclonal antibody or other test for C trachomatis
Presence of > 5 white blood cells per oil-immersion field The role of laparoscopy
on Gram's stain of endocervical discharge Laparoscopy continues to be the gold standard
SOURCE: MODIFIED FROM SWEET RL, REFERENCE 2 4
for diagnosing PID. However, most patients
with PID are diagnosed based on their clinical
symptoms, as laparoscopy requires technical
skill, surgical risk, and added cost, making it
TABLE 2 impractical for use as a screening proce-
dure.^
Laboratory evaluation for suspected Unfortunately, clinical diagnosis is less
pelvic inflammatory disease precise than laparoscopy: jacobson and
Westrom 25 found that laparoscopy confirmed
Complete blood count with differential the clinical diagnosis in only 6 5 % of cases,
Beta human chorionic gonadotropin (HCG) with 12% having other surgically identified
Test for C trachomatis and N gonorrhoeae conditions and 23% showing no pelvic
pathology at laparoscopy. When laparoscopy is
Rapid plasma reagin test for syphilis
used as the gold standard, the positive predic-
Sedimentation rate
tive value of a clinical diagnosis of PID is 6 5 %
Sonogram (if tubo-ovarian abscess or mass is suspected) to 90%.
Clinical diagnosis
Sweet 24 devised a set of major criteria (lower
• ESTABLISHING TRUST abdominal pain, cervical motion tenderness,
W I T H THE PID PATIENT and adnexal tenderness) and eight minor cri-
teria (TABLE 1 ) for the diagnosis of acute PID.
Adolescents with PID tend to seek medical Diagnosis is based on the presence of all three
attention later than adults do, 23 increasing major criteria and at least one minor criterion.
their risk for complications from PID. Other clinical clues include the onset of
When meeting with an adolescent patient pain 1 week after menses in those with gono-
for the first time, the physician should clearly coccal PID, new or increased vaginal dis-
outline the confidentiality of care before try- charge, a partner with recent urethritis,
ing to identify high-risk behaviors via the sex- dysuria in those with concomitant urethral
ual history. Teens are more likely to seek care, infection, and increased menstrual flow or
appear at follow-up appointments, and comply cramps. Diagnoses to be excluded include
with treatment regimens if they feel they can ectopic pregnancy, which is a surgical emer-
trust the care provider. gency requiring prompt recognition, ruptured
372 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E V O L U M E 65 • NUMBER 7 JULY/AUGUST 1998
Downloaded from www.ccjm.org on January 23, 2022. For personal use only. All other uses require permission.
ovarian cyst, endometriosis, appendicitis, and TABLE 3
a normal pelvis. Useful laboratory tests can be
found in T A B L E 2 . Clinical characteristics useful in i d e n t i f y i n g
At initial presentation, pregnancy should t u b o - o v a r i a n abscess in adolescents w i t h
be excluded with a urine beta human chori- pelvic i n f l a m m a t o r y disease
onic gonadotropin (HCG) test, and a blood
Last menstrual period > 18 days prior to admission
workup should include a complete blood
Previous episode of pelvic inflammatory disease
count, sedimentation rate, and a rapid plasma
Palpable adnexal mass
reagin test for syphilis. If PID is suspected,
White blood cell count > 10,500/mm3
endocervical tests for chlamydia and gonor-
Sedimentation rate > 15 mm/hour
rhea should be performed before initiating
Heart rate > 90
antibiotic treatment. Pelvic ultrasound should
be performed if a pelvic mass is suspected, or if
there is no clinical improvement at 48 hours
after initiating antibiotic treatment.
Subacute or "silent" P I D can occur with
C trachomatis, and substantial tubal destruc- Treatment guidelines
tion can still occur despite the absence of for pelvic i n f l a m m a t o r y disease
symptoms. Hillis et al 27 found that women
REGIMEN A
with chlamydial infection are more likely to Cefoxitin 2 g IV every 6 hours, or
delay care than women with gonorrhea, and Cefotetan 2 g IV every 12 hours
that a delay in care in women with PID was
PLUS
associated with a threefold increase in risk of
infertility and ectopic pregnancy. The burden Doxycycline 100 mg orally or IV every 12 hours
is on the clinician to diagnose and treat
chlamydial infections promptly, so as to pre-
REGIMEN B
vent subacute PID in the first place. Clindamycin 900 mg IV every 8 hours
Adolescent patients, in particular, need to be PLUS
educated on risk reduction and disease preven- Gentamycin 2 mg/kg body weight as a loading dose IV or intra-
tion. Each teen should be aware that she muscularly, then maintenance doses of 1.5 mg/kg every 8 hours
should have a pelvic examination within 3 to
6 months of any new partner to detect hidden ADDITIONAL PARENTERAL REGIMENS
infection. Ofloxacin 400 mg IV every 12 hours
Gynecologic consult should be obtained
PLUS
when tubo-ovarian abscess is suspected, in all
cases of ectopic pregnancy, and when pelvic Metronidazole 500 mg IV every 8 hours
pain persists despite appropriate use of antibi-
otics. Ampicillin/sulbactam 3g IV every 6 hours
Fitz-Hugh-Curtis syndrome. A syndrome
of right upper quadrant pain due to perihepati- PLUS
tis is seen in about 5% to 20% of all women
with PID and has been called Fitz-Hugh-Curtis Doxycycline 100 mg IV or orally every 12 hours
syndrome. The syndrome includes:
• Perihepatitis associated with PID Ciprofloxacin 200 mg IV every 12 hours
• Pain and tenderness; abnormal liver
function tests PLUS
• A direct association with N gonor- Doxycycline 100 mg IV or orally every 12 hours
rhoeae and C trachomatis.
PLUS
Right upper quadrant pain may radiate to
the shoulder or the back. The pain may occur Metronidazole 500 mg IV every 8 hours
SOURCE: CENTERS FOR DISEASE CONTROL A N D PREVENTION, 1 9 9 8 SEXUALLY TRANSMITTED
either simultaneously with symptoms of salp- DISEASE TREATMENT GUIDELINES FOR PELVIC I N F L A M M A T O R Y DISEASE, REFERENCE 1
ingitis or up to 2 weeks later.
C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E VOLUME 65 • NUMBER 7 JULY / A U G U S T 1998 3 4 3
Downloaded from www.ccjm.org on January 23, 2022. For personal use only. All other uses require permission.
PELVIC INFLAMMATORY DISEASE ROME
• DIAGNOSIS OF T U B O - O V A R I A N ABSCESS: be recommended for any adolescent patient
A C O M P L I C A T I O N OF PID who may be at risk for poor follow-up or non-
compliance. No evidence on long-term out-
Another complication of PID is tubo-ovarian come and sequelae after use of oral regimens in
abscess, a consequence of purulent material adolescents with PID currently exists, so cau-
from an infected fallopian tube coming into tion is encouraged.
contact with the adjacent ovary. Tubo-ovarian Use of broad-spectrum antibiotics is rec-
abscess occurs in 7 % to 16% of all cases of ommended to cover possible C trachomatis,
acute PID. A ruptured tubo-ovarian abscess is penicillinase-producing N gonorrhoeae, gram-
a surgical emergency; and as many as 3 % to negative enterics, penicillinase-producing
15% of all tubo-ovarian abscesses rupture. anaerobes, and those bacteria associated with
Women with tubo-ovarian abscesses may be bacterial vaginosis.1-21 The 1998 C D C recom-
acutely ill at presentation. mendations are listed in TABLE 4, with efficacy
In a retrospective study, Slap et al 28 found confirmed by a recent meta-analysis of antibi-
that the clinical characteristics listed in T A B L E 3 otic regimens.1
correctly identified 78% of women who had After the initial 48 hours of inpatient
tubo-ovarian abscesses and 8 8 % of those who care, the bimanual examination should be
did not. The investigators validated these repeated. If the teen has increasing or per-
characteristics in a subsequent series of sisting pain, further evaluation may be need-
women, in whom the model correctly identi- ed to exclude the diagnosis of tubo-ovarian
fied 8 3 % of those who had tubo-ovarian abscess or other pelvic disease. If the pain is
abscesses and 77% of those who did not. improving but is still significant, the teen
Ultrasound can be a useful adjunct in the may need another 24 hours of intravenous
diagnosis of PID with tubo-ovarian abscess; antibiotics. If she has no pain, she may be
Golden et al 29 found sonographic evidence of sent home to finish a 10- to 14-day course of
tubo-ovarian abscess in 11 (19.3%) of 57 ado- doxycycline.
lescents with PID. Transvaginal ultrasound Follow-up. A follow-up appointment
increases the sensitivity to 8 5 % and the speci- should be arranged prior to discharge to aid in
Ultrasound ficity to 100% according to one small study compliance and to minimize the risk of rein-
which used endometrial biopsy to confirm the fection. Although the 1998 C D C treatment
can aid the diagnosis.30 However, sonographic examina- guidelines do not mandate a test of cure, if a
diagnosis of tion may be negative in patients with laparo- culture for C trachomatis or N gonorrhoeae is
scopically confirmed PID. 28 positive, repeat culture should be performed to
PID with evaluate for reinfection. Since polymerase
tubo-ovarian • TREATMENT OF PID chain reaction and ligase chain reaction tests
for chlamydia and gonorrhea can remain posi-
abscess According to the 1993 Sexually Transmitted tive for up to 3 weeks after treatment, test for
Diseases Treatment Guidelines from the reinfection should be performed 1 month after
Centers for Disease Control and Prevention treatment.
(CDC),31 all adolescents with PID should be Patient education. The clinician should
hospitalized because of the high risk of non- also use the hospitalization as a time for
compliance and the severity of side effects if patient education and for partner notification
untreated. and treatment, if possible. Clinical pathway
The 1998 Sexually Transmitted Diseases guidelines for use on an inpatient ward have
Treatment Guidelines no longer require hospi- been developed and can help ensure that
talization as long as ongoing antibiotic thera- these tasks are achieved. 32
py is ensured. These guidelines emphasize that Further studies are necessary to evaluate
no current data compare the efficacy of par- whether outpatient treatment with a strong
enteral vs oral therapy or inpatient vs outpa- emphasis on patient education and close fol-
tient therapy. The issues of compliance and low-up can improve compliance and decrease
future risk to fertility remain greater in the the incidence of negative sequelae in this
adolescent age group; hospitalization should group.
374 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E V O L U M E 65 • NUMBER 7 JULY / A U G U S T 1998
Downloaded from www.ccjm.org on January 23, 2022. For personal use only. All other uses require permission.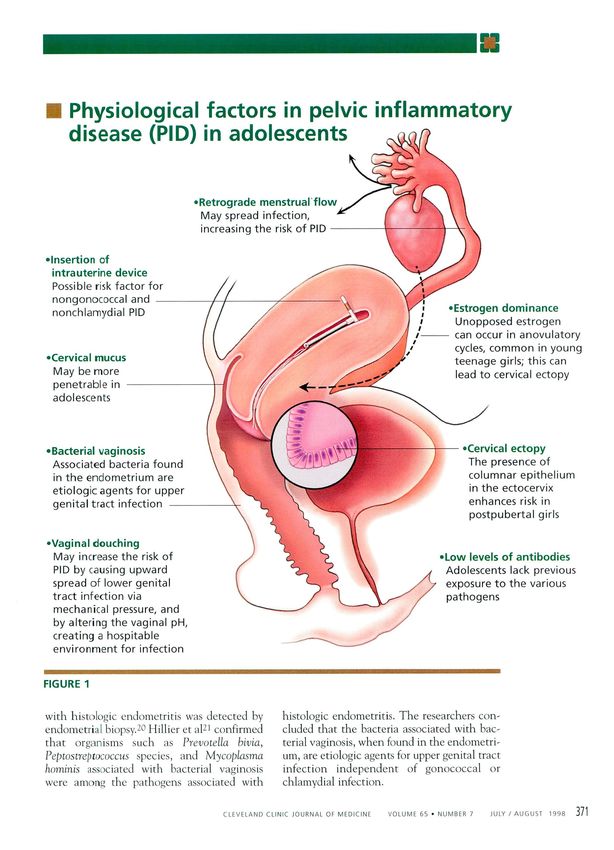
a P R E V E N T I O N OF PID IN PATIENTS • THE I M P O R T A N C E OF A G G R E S S I V E
W I T H SEXUALLY T R A N S M I T T E D DISEASES M A N A G E M E N T OF PID BY P H Y S I C I A N S
In 1994, the prevention of chlamydial infec- A study of 1,165 physicians in California
tion became a national priority because of its revealed that more than half (553 physicians)
significant impact on the reproductive had treated a case of PID in the past year.
health of women. 33 A recent cost analysis However, 5 2 % of these clinicians were not fol-
compared the use of azithromycin vs doxy- lowing the C D C recommendations for PID 3 7
cycline to treat chlamydial infection to pre- because they were unaware of specific recom-
vent PID. 3 4 This analysis found that use of a mendations, especially concerning hospitaliza-
single dose of azithromycin, compared with tion of adolescents. Pediatricians and physi-
the standard, less-expensive 7-day course of cians with more years since residency training
doxycycline, would prevent an additional were more likely to follow the C D C 1993 treat-
5 4 , 0 0 0 cases of PID among an estimated 2 ment guidelines, while family practitioners
million women who become infected with were more likely to deviate from the guidelines.
Chlamydia annually. 4 - 34 Single-dose therapy T h e C D C guidelines were designed to
with azithromycin was also estimated to save reduce adverse health sequelae and to he cost-
approximately $ 1 9 0 million in PID-associat- effective. Other regimens that include effective
ed medical costs. 3 4 Although azithromycin antimicrobial coverage against gonococcus and
has been shown to be effective in the treat- anaerobes can be used but may be more expen-
ment o f asymptomatic and uncomplicated sive. Use of a clinical pathway guideline in one
chlamydial cervicitis, its efficacy in the small study for inpatient care of adolescents
direct treatment of PID in the adolescent with PID preliminarily resulted in decreased
remains to be determined. 3 5 ' 3 6 length of stay and cost per case. 32 C3
REFERENCES
Centers for Disease Control and Prevention. 1998
Guidelines for treatment of sexually transmitted diseases.
12. Grimes DA. Intrauterine devices a n d pelvic Inflammato-
ry disease: recent developments. Contraception 1987;
A single
M M W R 1998; 47(RR-1):1-116.
S w e e t RL. Role of bacterial vaginosis in pelvic inflamma- 13.
36:97-109.
Bromham DR. Intrauterine contraceptive devices: a reap-
dose of
tory disease. Clin Infect Dis 1995; 20(Suppl 2):S271-S275.
B u m a k i s TG, Hildebrandt NB. Pelvic inflammatory disease: 14.
praisal. Br M e d Bull 1993; 49:100-123.
Burkman RT. Association between intrauterine device and
azithromycin
a review with emphasis on antimicrobial therapy. Rev
Infect Dis 1986; 8:86-116.
pelvic inflammatory disease. Obstet Gynecol 1981;
57:269-276.
prevents PID
Washington AE, Katz P. Cost of and payment source for
pelvic inflammatory disease. J A M A 1991; 266:2565-2569.
15. Zorlu CG, Aral K, Cobanoglu O, Gurler S, G o k m e n O.
Pelvic inflammatory disease and intrauterine devices: pro-
in women
W e s t r o m L, Incidence, prevalence, and trends of acute
pelvic inflammatory disease and its consequences in
phylactic antibiotics t o reduce febrile complications. Adv
Contraception 1993; 9:299-302.
with
industrialized countries. A m J Obstet Gynecol 1980;
138:880-892.
16. Hingson RW, Strunin L, Berlin B M , Heeren T. Beliefs about
AIDS, use of alcohol a n d drugs, and unprotected sex
Chlamydia
R o m e ES. Felvic inflammatory disease in the adolescent. a m o n g Massachusetts adolescents. A m J Public Health
Curr Opin Pediatr 1994; 6:383-387. 1990; 80:295-299.
Washington AE, Aral SO, Wolner-Hanssen P, Grimes DA, 17. DiClemente RJ, Durbin M, Siegel D, Krasnovsky F, Lazarus
Holmes KK. Assessing risk for pelvic inflammatory disease N. Determinants of condom use among junior high school
and its sequelae. J A M A 1991; 266:2581-2586. students In a minority, Inner-city school district. Pediatrics
Scholes D, Daling JR, Stergachis A, et al. Vaginal douch- 1992; 89:197-202.
ing as a risk factor for acute pelvic inflammatory disease. 18. Shafer M A . Sexually transmitted disease syndromes. In:
Obstet Gyrecol 1993; 81:601-606. McAnarney ER, Kreipe RE, Orr DP, and Comerci GD, edi-
Wolner-Hanssen P, Eschenbach DA, P a a v o n e n J, e t al. tors. Textbook of Adolescent Medicine. Philadelphia: W . B .
Association b e t w e e n vaginal douching a n d acute pelvic Saunders Company, 1992:703-705.
inflammatory disease. J A M A 1990; 263:1936-1941. 19. S w e e t RL. Diagnosis and treatment of acute salpingitis. J
10. Forrest KA, W a s h i n g t o n AE, Daling JR, S w e e t RL. Vaginal Reprod M e d 1977; 19:21-30.
douching as a possible risk factor for PID. J Natl M e d 20. P a a v o n e n J, Teisala K, Heinonen PK, et al.
Assoc 1989; 81:159-165. Microbiological a n d hlstopathologlcal findings in acute
ii. W e s t r o m L Bengtsson LP, M a r d h PA. The risk of pelvic pelvic inflammatory disease. Br J Obstet Gynaecol 1987;
inflammatory disease in w o m e n using intrauterine con- 94:454-460.
traceptive devices as compared to non-users. Lancet 1976; 21. Hillier SL, Kiviat NB, Critchlow C, et al. Bacterial vaginosis-
2:221-224. associated bacteria as etiologic agents of pelvic Inflamma-
C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E VOLUME 65 • NUMBER 7 JULY / A U G U S T 1998 375
Downloaded from www.ccjm.org on January 23, 2022. For personal use only. All other uses require permission.
CME CALENDAR 19 9 8 ROME
C O U R S E S are held at Bunts Auditorium, Cleveland
Clinic unless noted. Information and brochure:
(800) 762-8173 or (216) 444-5696
tory disease (abstract). Proceedings of t h e annual meet-
ing of the Infectious Diseases Society of Obstetrics and
Gynecology (San Diego), 1992.
A U G U S T
22. Eschenbach DA, Hillier S, Critchlow C, e t al. Diagnosis
15TH INTERNATIONAL FIBRINOGEN WORKSHOP a n d clinical manifestations of bacterial vaginosis. A m J
August 13-15 Obstet Gynecol 1988; 158:819-828.
Renaissance Cleveland Hotel 23. Spence MR, Adler J, McLellan R. Pelvic inflammatory dis-
ease in the adolescent. J Adolesc Health Care 1990;
HORIZONS IN PULMONARY AND CRITICAL CARE MEDICINE
4:304-309.
August 27-28
24. S w e e t RL. Pelvic inflammatory disease a n d Infertility
in w o m e n . Infect Dis Clin N o r t h A m 1987; 1:199-215.
PEDIATRIC BOARD REVIEW
August 31-September 4 25. Jacobson L, W e s t r o m L. Objectivized diagnosis of acute
pelvic inflammatory disease. Arm J Obstet Gynecol 1969;
105:1088-1098.
26. Centers for Disease Control a n d Prevention. Pelvic
S E P T E M B E R inflammatory disease. W M W R 1993; 42:75-81.
27. Hillis SD, Joesoef R, March banks PA, et al. Delayed care
ENDOCRINOLOGY BOARD REVIEW of pelvic inflammatory cisease as a risk factor for
September 10-12 impaired fertility. A m J Obstet Gynecol 1993;
168:1503-1509.
COMPUTERS IN CARDIOLOGY 1998
28. Slap G B , Forke C M , Cnaan A , et al. R e c o g n i t i o n of
September 13-16
Renaissance Cleveland Hotel t u b o - o v a r i a n abscess ir adolescents w i t h pelvic
i n f l a m m a t o r y disease. J Adolesc H e a l t h 1996;
OPHTHALMOLOGY 18:397-403.
September 18-19 29. G o l d e n NH, Cohen H, Gennari G, e t al. The use of
pelvic ultrasonography in t h e e v a l u a t i o n of adolescents
ADOLESCENT MEDICINE w i t h pelvic inflammatory disease. A J D C 1987;
September 25
141:1235-1238.
30. Cacciatore B, Leminen A, Ingman-Friberg S, Ylostalo P,
P a a v o n e n J. Transvaginal sonographic findings in ambu-
latory patients with suspected pelvic inflammatory dis-
O C T O B E R
ease. Obstet Gynecol 1992; 80:912-916.
31. Centers for Disease Control a n d Prevention. 1993
INTERNATIONAL TRANSPLANT CONFERENCE
October 2-^1 Guidelines for treatmen: of sexually transmitted disease.
Cleveland Marriott Hotel at Key Center M M W R 1993; 42(RR-14):75-81.
32. Rome ES, Moszczenski SA, Craighill MC, et al. A n inpa-
HEART FAILURE tient clinical pathway for pelvic inflammatory disease.
October 9-10 Clinical Performance and Quality Health Care 1995;
Renaissance Cleveland Hotel
3:185-196.
33. US Department of Health a n d H u m a n Services, Public
NEW HORIZONS AND INNOVATIONS
IN BIOMEDICAL ENGINEERING Health Service. For a healthy nation: returns on invest-
October 10-13 ment in public health. The Joint Council of Governmental
Renaissance Cleveland Hotel Public Health Agencies, 1994.
34. Haddix AC, Hillis SD, Kassler W J . T h e cost-effectiveness
INVASIVE ECHOCARDIOGRAPHY
of azithromycin f o r Chlamydia trachomatis infections in
October 14-16
w o m e n . Sexually TransniLted Diseases 1995;
PELVIC DISORDERS 22:274-280.
October 23-24 35. Martin DH, Mroczkowski TF, Dalu ZA, et al. A controlled
Renaissance Cleveland Hotel trial of a single dose of azithromycin for t h e treatment
of chlamydial urethritis and cervicitis. N Engl J M e d 1992;
BIOSTATISTICS IN MEDICINE 327:921-925.
October 28-29
36. Hammerschklag MR, Golden NH, O h M K , et al. Single
dose of azithromycin for the t r e a t m e n t of genital
chlamydial infections in adolescents. J Pediatr 1993;
122:961-965.
N O V E M B E R
37. Hessol NA, Prlddy FH, Bolan G, et al. M a n a g e m e n t of
pelvic inflammatory disease by primary care physicians. A
SURVEY OF ANESTHESIOLOGY
November 6-8 comparison with Centers for Disease Control and
Renaissance Cleveland Hotel Prevention guidelines. Sexually Transmitted Diseases
1996; 23:157-163.
INTERVENT 99
November 8
AHA Satellite Conference ADDRESS: Ellen S. Rome, MD, Department of Adolescent
Medicine, A120, The Cleveland Clinic Foundation, 9500 Euclid
GASTROENTEROLOGY COURSE 1998 Avenue, Cleveland, OH 44195.
November 18-19
SCHEDULE UPDATES: http://www.ccf.org/ed/netcme.htm
C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E VOLUME 65 • NUMBER 7 JULY / A U G U S T 1998
Downloaded from www.ccjm.org on January 23, 2022. For personal use only. All other uses require permission.You can also read