PK-PD Modeling and Dosage Determination for Proof-of-Concept Trials - Marc R. Gastonguay, Ph.D. ()
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
IMMPACT-VIII
Early Clinical Study Designs, Emphasizing Proof-of-Concept Trials
June 12-14, 2008
Arlington, VA
PK-PD Modeling and Dosage
Determination for Proof-of-Concept Trials
Marc R. Gastonguay, Ph.D.
(marcg@metrumrg.com)
©2008 metrum research group LLC
PKPD in Proof of Concept Trials: IMMPACT 2008
Overview
- PK/PD (Exposure-Response) and Model-Based Drug
Development
- Role of Exposure-Response Modeling in Proof-of-Concept
Trials
Planning and Design
Analysis and Quantitative Support for PoC Determination
Building Knowledge for Later Stage Development
Other examples of E-R utility
- Summary Points
©2008 metrum research group LLC 2PKPD in Proof of Concept Trials: IMMPACT 2008
Innovation: Planes are modeled long before takeoff
NASA Aerospace Engineering Grid
Wing Models
•Lift Capabilities
Stabilizer Models
•Drag Capabilities
Airframe Models •Responsiveness
•Deflection capabilities
•Responsiveness
Crew
Capabilities
- accuracy
- perception
- stamina
Engine Models
- re -action
times
- SOP’s
•Braking performance
•Steering capabilities
Human Models
•Traction
•Thrust performance
•Dampening capabilities
•Reverse Thrust performance
•Responsiveness
Landing Gear Models •Fuel Consumption
Whole system
It takes simulations
a distributed areorganization
virtual produced by tocoupling
design,
all ofbuild
simulate and the sub -systemsystem
a complex simulations
like an aircraft
©2008 metrum research group LLC http://grids.ucs.indiana.edu/ptliupages/presentations/cendiapril25-05.ppt 3PKPD in Proof of Concept Trials: IMMPACT 2008
PROGRESSION
Pharmacometrics…the science of
DISEASE
interpreting and describing
pharmacology in a quantitative fashion
(e.g. through modeling and simulation)
DOSE CONCENTRATION RESPONSE
PK PD
TRIAL DESIGNS &
DEVELOPMENT STRATEGY KNOWLEDGE
©2008 metrum research group LLC 4PKPD in Proof of Concept Trials: IMMPACT 2008
Modeling and Simulation: A Tool to Facilitate
the Learn-Confirm Continuum
Sheiner LB. Learning versus confirming in clinical drug development.
Clin Pharmacol Ther 1997; 61(3):275-91.
Collect data
Build models to describe data and
confirm prior knowledge
Use M&S to learn from new data and
explore future outcomes
Make informed decisions
Perform new experiment (study)
©2008 metrum research group LLC 5PKPD in Proof of Concept Trials: IMMPACT 2008
M&S Throughout Drug Development
Therapeutic Area Simulation & Optimization
Knowledge: Disease of Phase III Trial Designs
Simulation-Guided
Progression &
(Adaptive) Phase II
Target Response
Designs: Early Pop PK, E-R for
Profile
Probability of Success & Labeling and
Dose-Response Confirmatory
Efficacy Support
Preclinical &
Early Development:
PK-PD, Systems Proof of Concept:
Biology M&S Probability-Based
Decision Rule
Toxicology Human Biomarker, Efficacy, Efficacy, New
PK MTD, PK Tolerability E-R Safety & Dose Formulations
Biomarker Biomarker, Dose-Response Special Bridge to New
E-R Tolerability, E-R Covariates, Pop PK-PD Populations Indications
©2008 metrum research group LLC 6PKPD in Proof of Concept Trials: IMMPACT 2008
What to Learn?
30
30
WR Immediate
WR Immediate
10
10
LPS (min)
LPS (min)
Tolerability PD Efficacy
20
20
8
8
Prob (AE)
6
6
10
10
4
4
5
5
2
2
0
0
0
0
450
450
10
10
WR 0.5 hr
WR 0.5 hr
TST (min)
TST (min)
RESPONSE
LPSres$AUC LPSres$AUC WRres$AUC WRres$AUC
8
8
430
430
6
6
Clinical Outcomes
link
410
410
4
4
2
2
390
390
0
0
30
30
10
10
WR 7 hrs
WR 7 hrs
NAW 2 NAW 2
20
20
Biomarkers
TSTres$AUC TSTres$AUC WRres$AUC WRres$AUC
8
8
NAW
NAW
6
6
10
10
4
4
5
5
2
2
0
0
0
0
NAW 1 NAW 1
20
20
20
20
Dose (mg)
Dose (mg)
Dose (mg)
Dose (mg)
NAW1res$AUC NAW1res$AUC WRres$AUC WRres$AUC
10
10
10
10
Dose
Dose
3
3
3
3
1
1
1
1
0 50 0 100 50 150 100 150
0 50 0 100 50 150 100 150
EXPOSURE (e.g. AUC, Cmax, Css avg)
NG2-73NG2-73
(ng*hr/mL)
NG2-73 AUC (ng*hr/mL) AUC (ng*hr/mL)
AUC (ng*hr/mL) NG2-73 AUC NG2-73 AUC (ng*hr/mL)
NG2-73 AUC (ng*hr/mL)
©2008 metrum research group LLC 7PKPD in Proof of Concept Trials: IMMPACT 2008
Regulatory Support for M&S
- Stanski. Model-Based Drug Development: A Critical Path Opportunity, March 18, 2004
http://www.fda.gov/oc/initiatives/criticalpath/presentations.html
©2008 metrum research group LLC 8PKPD in Proof of Concept Trials: IMMPACT 2008
Regulatory Support for M&S:
Guidance Documents
- Population Pharmacokinetics (FDA and EMEA)
- Exposure-Response Relationships (FDA)
- Dose-Response Information to Support Drug
Registration (ICH-E4)
- General Considerations for the Clinical Evaluation of Drugs (FDA 77-
3040)
- General Considerations for Pediatric Pharmacokinetic Studies (FDA)
- Pharmacokinetics in Patients with Impaired Renal Function (FDA)
- Pharmacokinetics in Patients With Impaired Hepatic Function (FDA)
- Studies in Support of Special Populations:
Geriatrics (ICH-E7)
- Ethnic Factors in the Acceptability of Foreign
Clinical Data (ICH-E5)
- Clinical Investigation of Medicinal Products in the Pediatric Population
(ICH-E11)
©2008 metrum research group LLC 9PKPD in Proof of Concept Trials: IMMPACT 2008
Determination of PoC
- Primary Challenge: Define decision criteria for PoC
determination
Proof of mechanism
Statistically significant efficacy response with approval endpoint
Acceptable probability of achieving multivariate target response
profile
Comparability to active control
- Once defined, probability of meeting PoC decision criteria
for different trial designs can be explored through
modeling and simulation
©2008 metrum research group LLC 10PKPD in Proof of Concept Trials: IMMPACT 2008
Target Response Profile
30
30
WR Immediate
WR Immediate
10
10
LPS (min)
LPS (min)
Tolerability PD Efficacy
20
20
8
8
Prob (AE)
6
6
10
10
4
4
5
5
2
2
0
0
0
0
450
450
10
10
WR 0.5 hr
WR 0.5 hr
TST (min)
TST (min)
RESPONSE
LPSres$AUC LPSres$AUC WRres$AUC WRres$AUC
8
8
430
430
6
6
Clinical Outcomes
410
410
4
4
2
2
390
390
0
0
30
30
10
10
WR 7 hrs
WR 7 hrs
NAW 2 NAW 2
20
20
Biomarkers
TSTres$AUC TSTres$AUC WRres$AUC WRres$AUC
8
8
NAW
NAW
6
6
10
10
4
4
5
5
2
2
0
0
0
0
NAW 1 NAW 1
20
20
20
20
Dose (mg)
Dose (mg)
Dose (mg)
Dose (mg)
NAW1res$AUC NAW1res$AUC WRres$AUC WRres$AUC
10
10
10
10
Dose
Dose
3
3
3
3
1
1
1
1
0 50 0 100 50 150 100 150
0 50 0 100 50 150 100 150
EXPOSURE (e.g. AUC, Cmax, Css avg)
NG2-73NG2-73
(ng*hr/mL)
NG2-73 AUC (ng*hr/mL) AUC (ng*hr/mL)
AUC (ng*hr/mL) NG2-73 AUC NG2-73 AUC (ng*hr/mL)
NG2-73 AUC (ng*hr/mL)
©2008 metrum research group LLC 11PKPD in Proof of Concept Trials: IMMPACT 2008
PK and Exposure-Response M&S
Opportunities in PoC
- PK Modeling
Understand PK in target population and possibly reduce inter-
individual variability in exposure to increase signal/noise: dosing
individualization
Select PoC doses with minimal exposure overlap
Explain unexpected outcomes (e.g. unknown phenotypic
differences in PK)
Adjust for formulation differences
- E-R Modeling
Assessment of E-R relationships for multiple endpoints (e.g. after
dose-ranging based on efficacy endpoint)
Basis for trial simulations: explore performance/options in silico
before initiating clinical trial
©2008 metrum research group LLC 12PKPD in Proof of Concept Trials: IMMPACT 2008
Impact of E-R Varies with PoC Trial Designs
MTD-Type PoC Design
Typically 1 active treatment dose vs. reference
treatment
Dose selected based on Phase I MTD
Standard pair-wise statistical comparison
Dose-Ranging PoC Design
Multiple doses investigated
Dose-range informed by preclinical data, Phase
I, biomarker, competitor data
Model-based data analysis
Often multi-variable PoC assessment
©2008 metrum research group LLC 13PKPD in Proof of Concept Trials: IMMPACT 2008
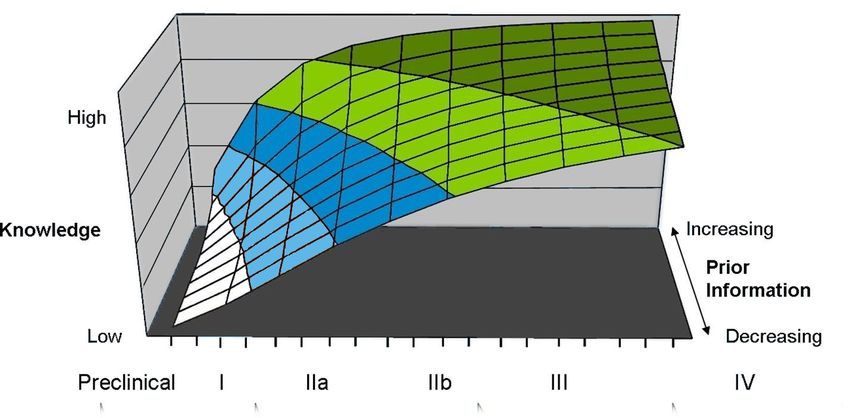
Exposure-Response in MTD-Type PoC:
Proceed with Caution
- Single active treatment arm at
MTD (300 mg) vs. Placebo
- Obtain PK in all individuals
- Explore resulting relationship
between exposure (Cavg) and
Response (1 observation per
individual)
- Can we make an accurate
assessment of the PK-PD
relationship from this design?
Problem described in: Nedelman JR, Rubin DB, Sheiner LB. Diagnostics for confounding in
PK/PD models for oxcarbazepine. Stat Med. 2007 Jan 30;26(2):290-308.
©2008 metrum research group LLC 14PKPD in Proof of Concept Trials: IMMPACT 2008
Exposure-Response in MTD-Type PoC
- Consider possible inter-individual correlation between PK
and PD
©2008 metrum research group LLC 15PKPD in Proof of Concept Trials: IMMPACT 2008
Exposure-Response in MTD-Type PoC
- Resulting exposure-response relationships are misleading
©2008 metrum research group LLC 16PKPD in Proof of Concept Trials: IMMPACT 2008
Exposure-Response in MTD-Type PoC
- One solution: Obtain within-individual E-R (e.g. crossover)
analyzed with mixed-effects modeling
©2008 metrum research group LLC 17PKPD in Proof of Concept Trials: IMMPACT 2008
Exposure-Response in MTD-Type PoC
- Another solution: Population E-R with broad dose-range
©2008 metrum research group LLC 18PKPD in Proof of Concept Trials: IMMPACT 2008
PK-PD in Planning and Design of PoC Trials
- Use prior information, when available
Phase I PK, tolerability, biomarkers
Pre-clinical estimates of effective concentrations,
relative potency
Competitor data
Therapeutic area knowledge
©2008 metrum research group LLC 19PKPD in Proof of Concept Trials: IMMPACT 2008
Toxicity E-R to Inform PoC Dose Selection
Data from SAD, MAD
in healthy volunteers
©2008 metrum research group LLC 20PKPD in Proof of Concept Trials: IMMPACT 2008
Probability of QTc Prolongation
• Explore probability of QTc – related toxicity at
various doses from Phase I data
• Project QTc prolongation at expected Cmax, given
top dose and DDI
• Define dose-limit and early probability of
compound viability
©2008 metrum research group LLC 21PKPD in Proof of Concept Trials: IMMPACT 2008
Modeling Biomarker Data: Phase I MD Study
- PK-PD relationship evident & quantifiable (‘Emax’ model)
- Establish target PoM
- Set doses for investigation in PoC = concentrations within apparent
efficacious range
7
E * Conc O Placebo
6
Marker = E0 + max O Dose 1
EC50 + Conc O Dose 2
O Dose 3
5 --- Model Prediction
Marker
4
3
2
1
0
0 1 2 3 4
Concentration
©2008 metrum research group LLC 22PKPD in Proof of Concept Trials: IMMPACT 2008
E-R Analysis of PoC Trials
- Example
Parallel groups: 4 active doses + placebo + active control
(competing therapy)
Multiple Endpoints: biomarker 1 (efficacy), biomarker 2
(undesired), clinical outcome 1
PoC determination based on model-based posterior probability of
reaching target response profile
©2008 metrum research group LLC 23PKPD in Proof of Concept Trials: IMMPACT 2008
E-R Based PoC: Test & Active Comparator
Response: Biomarker 1 (efficacy)
- Drug X (red) was more potent than Comparator Y (blue)
- Relative potencies (EC50 of X vs. Y) very
Drug consistent across
X (red),Comparator Y (blue) multiple response variables
5
Median observation at each collection time for each treatment (circles)
PK-PD Model Prediction (solid line)
EC50 = dashed lines
Biomarker 1 Response
4
RXij = E0i + EMAXi*Ci/(EC50Xi + Ci) + eij
Median Response
RYij = E0i + EMAXi*Ci/(EC50Yi + Ci) + eij
3
2
Target
1
0
Plasma Drug Concentration
Median Concentration
©2008 metrum research group LLC 24PKPD in Proof of Concept Trials: IMMPACT 2008
PoC: E-R for Biomarker 2 (undesired)
- Identified Drug X concentrations associated with BM II effect
- Consider doses that provide for target concentrations
Concentration range Concentration range
associated with “no effect” associated with “effect”
Marker II
Target
Concentration
©2008 metrum research group LLC 25PKPD in Proof of Concept Trials: IMMPACT 2008
E-R for Clinical Outcome I
Response I
Target
Dose
Cmax (concentration)
Drug X
©2008 metrum research group LLC 26PKPD in Proof of Concept Trials: IMMPACT 2008
Building Knowledge for Phase 2b
- Drug X posterior probability distribution for target response meets
PoC criterion, but which doses should go into Phase 2b, where
primary endpoint will be an approval outcome measure?
- Comparator Y Dose-Response
Literature data
Model = Nonlinear ‘Emax’ model for mean relationship
Uncertainty range: Based on standard errors of parameter estimates
- Scaled for Approximate Dose-Response of Drug X
Based on biomarker relative EC50 of Drug X vs. Comparator Y
Accounted for PK differences
Additional variability for uncertainty in scaling ratios
©2008 metrum research group LLC 27PKPD in Proof of Concept Trials: IMMPACT 2008
Dose-Response Model for Comparator Y: 2b Response
0
1
Response
Literature data (o)
Response
2
Uncertainty
3 range: based
on 95% CI’s of
parameter
Mean Prediction (___) estimates
4
0 1 2 3 4
Dose
Dose Y
©2008 metrum research group LLC 28PKPD in Proof of Concept Trials: IMMPACT 2008
Scaled Dose-Response for Drug X:
Predicted 2b Response
- Select doses to further characterize (reduce uncertainty in) response surface
0
1
Response
2
3
4
0 1 2 3 4
- Target doses ~ 50% (ED50), 80% (ED80) & max effects (Emax)
Dose
©2008 metrum research group LLC 29PKPD in Proof of Concept Trials: IMMPACT 2008
Other Examples of E-R in Analgesic PoC Trials
- Dissociation of rescue drug effects from test treatment
- Model-based inferences with dropout (missing data)
©2008 metrum research group LLC 30PKPD in Proof of Concept Trials: IMMPACT 2008
Dissociating Treatment Effects from
Rescue Dose Effects
- Chronic pain PoC design (PBO plus 4 dose levels)
- Acetaminophen rescue (500 mg) allowed as needed
- Reduction in pain intensity is primary endpoint
- Problem: How to interpret pain response in presence of rescue?
- Proposal: Analyze entire data set with model-based analysis using 2
simultaneous exposure-response relationships:
Study Drug E-R
Rescue E-R
©2008 metrum research group LLC 31PKPD in Proof of Concept Trials: IMMPACT 2008
Consideration
- Potential delay between plasma exposure and exposure at
site of action (e.g.,CNS)
May be more pronounced with
▶ with acute or ‘prn’ dosing
▶ shorter t1/2 and/or rapid Tmax
Figure from: Shinoda S, Aoyama T, Aoyama Y, Tomioka S, Matsumoto
Y, Ohe Y 2007. Pharmacokinetics/pharmacodynamics of acetaminophen
analgesia in Japanese patients with chronic pain. Biol Pharm Bull
30(1):157-161
Also see: Staahl C, Upton R, Foster DJ, Christrup LL, Kristensen K,
Hansen SH, Arendt-Nielsen L, Drewes AM. Pharmacokinetic-
pharmacodynamic modeling of morphine and oxycodone concentrations
and analgesic effect in a multimodal experimental pain model. J Clin
Pharmacol. 2008 May;48(5):619-31.
©2008 metrum research group LLC 32PKPD in Proof of Concept Trials: IMMPACT 2008
Dual E-R Model Schematic
Study Rescue
Drug dose Drug dose
Gut Central Peripheral Gut Central
PD Effect
PD Effect
Effect Effect
Total Observed PD Response
©2008 metrum research group LLC 33PKPD in Proof of Concept Trials: IMMPACT 2008
Individual Contributions to Total Response
- Integrated model of
Study Drug and Rescue
E-R
- Allows interpretation of
individual and joint
effects
- Success of this
approach highly
dependent on adequate
Dose-Ranging design
- Results preliminary:
Evaluation of
performance through
simulation ongoing
©2008 metrum research group LLC 34PKPD in Proof of Concept Trials: IMMPACT 2008
Model-Based Inferences in the Presence of
Dropout
- Acute pain PoC study
- Dropout after first rescue
- Population nonlinear-mixed effects exposure-response model
developed from observed repeated-measures data (missing At
random assumption)
Approach first described in:
Sheiner LB. A new approach to the analysis of analgesic drug trials,
illustrated with bromfenac data. Clin Pharmacol Ther. 1994
Sep;56(3):309-22.
©2008 metrum research group LLC 35PKPD in Proof of Concept Trials: IMMPACT 2008
NPRS Score Frequency (%)
NPRS Score Frequency (%)
Observed Pain Intensity Observed Data
100
120Observed
mg Patients (n=66)
Pain Intensity
Placebo
100
80 Placebo (n=34)
80
of NPRS20Score
Rescued NPRS = 5
60
NPRS = 10
Rescued NPRS
NPRS= =4 5
60
NPRS = 9 NPRS = 3
40
NPRS = 10 NPRS = 4
NPRS = 8= 9
NPRS NPRS
NPRS= =2 3
40
NPRS = 7= 8
NPRS NPRS
NPRS= =1 2
NPRS = 6= 7
NPRS NPRS
NPRS= =0 1
20
NPRS = 6 NPRS = 0
0
0
NPRS Score Frequency (%)
NPRS Score Frequency (%)
0.25 1 2 4 6 8 10 12
0.25 1 2 4 6 8 10 12
Time (hr)Pain Intensity
Observed Observed Pain Intensity
Dose 1 (n=66) Dose
Patients2(n=65)
NPRS Score Frequency (%)
NPRS Score Frequency (%)
Time (hr)
Frequency
100
120 mg Patients
100
60 mg
NPRS Score Frequency (%)
NPRS Score Frequency (%)
Predicted Pain Intensity Extrapolated Pain Intensity
80
80
120Predicted Pain(n=66)
Intensity Extrapolated Pain(n=66)
Intensity
100
40 20 60 40 80 60 100
mg Patients 120 mg Patients
100
100
Placebo (n=34) Placebo (n=34)
Rescued NPRS = 5 Rescued
60
80
NPRS = 10 NPRS = 4 NPRS = 10
80
80 NPRS = 9 NPRS = 3 NPRS = 9
40
NPRS = 8 NPRS = 2 NPRS = 8
60
60
60
NPRS = 7 NPRS = 1 NPRS = 7
20
NPRS = 6 NPRS = 0 NPRS = 6
40
40
40
0
0
20
20
20
20
0.25 1 2 4 6 8 10 12 0.25 1 2 4 6 8 10 12
0
0
0
0
Time (hr) Time (hr)
equency (%)
equency (%)
equency (%)
equency (%)
©2008 metrum research group LLC 0.25
0.25 1 21 42 64 86 10
8 12
10 12 0.250.25 1 1 2 2 4 4 6 6 8 8 1010 1212 36
Predicted Pain Intensity Extrapolated
Predicted PainPain Intensity
Intensity Extrapolated Pai
Time Time
(hr) (hr) Time (hr)
Time (hr)
100
100
100
100
120 mg Patients (n=66) 60120
mgmg Patients
Patients (n=66)
(n=65) 60 mg PatientPKPD in Proof of Concept Trials: IMMPACT 2008
PD Response Time-Course
PI121 ID=2036 PI121 ID=2037 PI121 ID=2038
Pain Intensity
Pain Intensity
Pain Intensity
10
10
10
8
8
8
6
6
6
4
4
4
Pain Intensity (NPRS)
2
2
2
0
0
0
0 2 4 6 8 10 12 0 2 4 6 8 10 12 0 2 4 6 8 10 12
Time (hr) Time (hr) Time (hr)
PI121 ID=2039 PI121 ID=2040 PI121 ID=2041
Pain Intensity
Pain Intensity
Pain Intensity
10
10
10
8
8
8
6
6
6
4
4
4
2
2
2
0
0
0
0 2 4 6 8 10 12 0 2 4 6 8 10 12 0 2 4 6 8 10 12
Time (hr) Time (hr) Time (hr)
PI121 ID=2042 PI121 ID=2043 PI121 ID=2044
Pain Intensity
Pain Intensity
Pain Intensity
10
10
10
8
8
8
6
6
6
4
4
4
2
2
2
0
0
0
0 2 4 6 8 10 12 0 2 4 6 8 10 12 0 2 4 6 8 10 12
Time (hr) Time (hr) Time (hr)
©2008 metrum research group LLC 37NPRS Score Frequency (%)
PKPD in Proof of Concept Trials: IMMPACT 2008
Predicted Pain Intensity Predicted Pain Intensity
Model-Based Extrapolation
60 mg Patients (n=65) 120 mg Patients (n=66)
100
100
60
60
NPRS Score Frequency (%)
NPRS Score Frequency (%)
- Repeated-measures nonlinear mixed effects model used Predicted Pain Intensity
60 mg Patients (n=65)
Predicted Pain Intensity
120 mg Patients (n=66)
20
20
100
100
to extrapolate individual responses over time
0
0
60
60
- View simulated 6 response12 time-course in1 the
2 absence of
20
20
0.25 1 2 4 8 10 0.25 4 6 8 10 12
dropout
0
0
NPRS Score Frequency (%)
Time (hr) Time (hr) 0.25 1 2 4 6 8 10 12 0.25 1 2 4 6 8 10 12
Frequency of NPRS Score
NPRS Score Frequency (%)
NPRS Score Frequency (%)
Frequency of NPRS Score
Time (hr) Time (hr)
Extrapolated Pain Intensity Extrapolated Pain Intensity ExtrapolatedExtrapolated
Pain Intensity
Pain Intensity
60 mgDose 1 (n=65)
Patients 120 mgDose
Patients 2Patients
(n=66)
100
100
60 mg Patients (n=65) 120 mg (n=66)
100
100
60
60
60
60
20
20
0
0
20
20
0.25 1 2 4 6 8 10 12 0.25 1 2 4 6 8 10 12
Time (hr) Time (hr)
0
0
0.25 1 2 4 6 8 10 12 0.25 1 2 4 6 8 10 12
Rescued NPRS = 5
Time (hr) NPRS = 10 NPRS = 4 Time (hr)
NPRS = 9 NPRS = 3
NPRS = 8 NPRS = 2
NPRS = 7 NPRS = 1
NPRS = 6 NPRS = 0
©2008 metrum research group LLC 38
Rescued NPRS = 5PKPD in Proof of Concept Trials: IMMPACT 2008
Summary (1)
The utility of exposure-response in PoC trials depends on
study design and PoC goals.
- MTD-Type PoC
E-R modeling of PoC data has minimal value; may be misleading
PK modeling still useful for understanding target population PK,
reducing variability, or for explaining extreme outcomes
- Dose-Ranging PoC
E-R has high value for design, analysis and PoC determination
Comparative E-R relationships across multiple endpoints/active
controls provides insight into probability of achieving target product
profile
Advances knowledge building for future drug development phases
Basis for trial simulations to explore future designs
©2008 metrum research group LLC 39PKPD in Proof of Concept Trials: IMMPACT 2008
Summary (2)
- PK and E-R modeling and simulation:
are tools for knowledge-building and decision support in drug
development
provide basis for trial simulations to explore and optimize trial
design performance
are best supported by trial designs that explore individual E-R
relationships
of multiple endpoints allows quantitative assessment of drug’s
multivariate response profile, supporting dose-selection decisions
may be useful in assessing test treatment response in presence of
rescue dosing (preliminary)
may be useful for making inferences in the presence of dropout
(for non-regulatory purposes)
©2008 metrum research group LLC 40PKPD in Proof of Concept Trials: IMMPACT 2008
Additional References
- Krall RL, KH Engleman, HC Ko, and CC Peck. “Clinical Trial Modeling and Simulation – Warner KE, Peck
CC, Work in Progress.” /Drug Info J/, 32: 971-976, 1998.
- Peck CC. “Drug development: Improving the process.” /Food and Drug Law J/. 52 (2):163-167, 1997.
- Reigner BG, PEO Williams, IH Patel, J-L Steimer, CC Peck, and P van Brummelen. “An evaluation of the
integration of pharmacokinetic and pharmacodynamic principles in clinical drug development.” /Clin
Pharmacokinet/, 33(2): 142-52, 1997.
- Biomarkers Definitions Working Group. “Biomarkers and surrogate endpoints: Preferred definitions and
conceptual framework.” /Clin Pharm Ther/ 69 (3): 89-95, 2001.
- Galluppi GR, MC Rogge, LK Roskos, LJ Lesko, MD Green, DW Feigal, and CC Peck. “Integration of
pharmacokinetics and pharmacodynamics studies in the discovery, development and review of protein
therapeutic agents: a conference report.” /Clin Pharm Ther/, 2001.
- Holford NHG, JPR Monteleone, HC Kimko, and CC Peck. “Simulation of Clinical Trials” in /Annual Rev
Pharmacol Toxicol./ Vol. 40: 209-234, 2000.
- Lockwood, Ewy, Herman, Holford. Application of Clinical Trial Simulation to Compare Proof of Concept
Designs for Drugs with a Slow Onset of Effect; An Example in Alzheimer’s Disease. Pharm Res. 23:9, 2006.
- Klingenberg B. A Unified Framework for Proof of Concept and Dose Estimation with Categorical Responses.
www.williams.edu/~bklingen .
- Lalonde RL, Kowalski KG, Hutmacher MM, Ewy W, Nichols DJ, Milligan PA, Corrigan BW, Lockwood PA,
Marshall SA, Benincosa LJ, Tensfeldt TG, Parivar K, Amantea M, Glue P, Koide H, Miller R. Model-based
drug development. Clin Pharmacol Ther. 2007 Jul;82(1):21-32.
- Atkinson AJ Jr, Lalonde RL.Introduction of quantitative methods in pharmacology and clinical pharmacology:
a historical overview. Clin Pharmacol Ther. 2007 Jul;82(1):3-6.
FDA Presentations on Model-Based Drug Development
- http://www.fda.gov/oc/initiatives/criticalpath/presentations.html
- http://www.fda.gov/ohrms/dockets/ac/03/slides/3998s1.htm
- http://www.aapspharmaceutica.com/meetings/files/38/Booth.ppt
©2008 metrum research group LLC 41PKPD in Proof of Concept Trials: IMMPACT 2008
Acknowledgements
- Heidi Costa
- Leonid Gibiansky
- Bill Knebel
- Matthew Riggs
- Bill Gillespie
- Industry collaborators
©2008 metrum research group LLC 42You can also read