Placed Based Care: Bedfordshire CCG and Central Bedfordshire Out of Hospital Strategy 2017/18 2022/23 - BLMK CCG
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Placed Based Care:
Bedfordshire CCG and Central Bedfordshire
Out of Hospital Strategy
2017/18 – 2022/23
1
Table of Contents
Vision .................................................................................................................................................... 4
Aims ....................................................................................................................................................... 4
Strategic Fit ......................................................................................................................................... 5
Bedford, Luton and Milton Keynes (BLMK) Sustainability and Transformation
Partnership (STP) ........................................................................................................................... 5
Accountable Care System ........................................................................................................... 6
Challenges ........................................................................................................................................... 6
Financial challenges: .................................................................................................................... 7
Bedfordshire CCG.......................................................................................................................... 7
Central Bedfordshire Council ..................................................................................................... 8
Population Changes ...................................................................................................................... 8
Adult Health Needs:....................................................................................................................... 9
Children’s Health Needs............................................................................................................... 9
Vulnerable groups ....................................................................................................................... 10
Secondary Care ............................................................................................................................ 10
Primary Care .................................................................................................................................. 10
Community Services ................................................................................................................... 10
Estates ............................................................................................................................................ 11
IT systems and information sharing for patient care ......................................................... 11
Patient and service user expectations: .................................................................................. 11
Delivering the Vision ....................................................................................................................... 13
Transforming health and social care ...................................................................................... 13
Locality Based Delivery Model ................................................................................................. 15
Bedfordshire Primary Care Home (PCH) Model ................................................................... 15
What will this mean to local people? ...................................................................................... 19
Community Health and Care Services.................................................................................... 20
Optimising planned care pathways / delivering more care closer to home ................. 21
Streamlining and improving the offer of urgent and out of hours services. ................ 22
Benefits of PCH Model .................................................................................................................... 22
Quantitative benefits ................................................................................................................... 22
Qualitative Benefits ..................................................................................................................... 23
National Delivery Areas .............................................................................................................. 23
What We Have Already Achieved ................................................................................................ 24
Primary Care .................................................................................................................................. 24
Healthy Living Pharmacy ........................................................................................................... 24
2
Care Market.................................................................................................................................... 25
Hear and Treat............................................................................................................................... 25
Mental Health................................................................................................................................. 25
Stroke Services............................................................................................................................. 27
Delivery Areas Requiring Additional Focus.............................................................................. 27
Cancer Services ........................................................................................................................... 27
Children and Young People ...................................................................................................... 28
Mental Health and Learning Disabilities ................................................................................ 28
Funding Mechanisms and Contractual Arrangements .......................................................... 30
Commissioning Intentions ........................................................................................................ 30
Quality, Innovation, Productivity and Prevention (QIPP) .................................................. 30
Integration and Better Care Fund (IBCF) ............................................................................... 31
BCF Plan 2017 -2019 ............................................................................................................... 32
Improved Better Care Fund (IBCF) ...................................................................................... 34
Plans for Year 1: 2017/18 ............................................................................................................... 35
Key Deliverables........................................................................................................................... 35
Enablers.......................................................................................................................................... 35
ICT and Information Sharing ................................................................................................. 35
Estates ........................................................................................................................................ 35
Deliverables in Year 2: 2018/19 ................................................................................................ 36
Deliverables in Year 3: 2019/20 ................................................................................................ 36
Next Steps ...................................................................................................................................... 36
Governance ....................................................................................................................................... 37
APPENDIX 1: Adult and Children’s Outcome Indicators ....................................................... 38
APPENDIX 2: Examples of BCCG Commissioning Intentions ............................................. 40
APPENDIX 3: Out of Hospital projects for delivery in 2017/18 ............................................ 42
3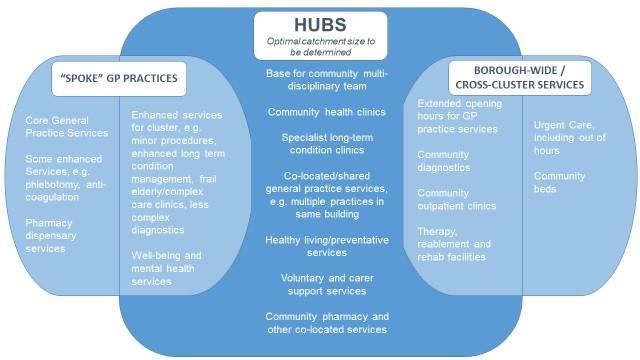
Vision
Our vision is for the people of Central Bedfordshire to have access to good quality, safe,
local health and social care across its towns and rural areas. This will be centred on the
integration of health and social care through a whole systems and seamless approach to
improving physical and mental health, so that people can experience “care without
organisational boundaries” and ‘better care, locally’.
We will ensure our populations are provided with the opportunities to realise their full
potential and have the support they require to lead healthy and independent lives; that they
receive timely access to high quality services such as health and care when they need it.
We will do this by:-
Helping our residents understand their health and care needs - ensuring they
are able to support themselves as much as possible for as long as possible.
Our residents understand how and when to call for support and advice.
Ensuring services are wrapped around the needs of an individual, delivered
seamlessly and residents and patients only have to tell their story once
We will reduce the need for multiple professional assessments and visits by
shared assessments, sharing responsibilities and information between
services.
Aims
The out of hospital strategy has been developed in partnership between Central Bedfordshire
Council (CBC) and Bedfordshire CCG (BCCG). It draws together a number of key areas of
work, some of which have already been or are being delivered, and sets out how financial
mechanisms and contractual arrangements are being used to support the delivery of the
strategy.
The aim of the strategy is to ensure that the health and care system in Central Bedfordshire
helps to support local people including adults, older people, children and young people, carers,
and people with learning disability, mental health, physical disability, or sensory disability
needs, to remain as healthy and independent as possible for as long as possible; and when
they need support they receive joined up and co-ordinated care in a timely manner as close
to home as possible.
The strategy has a strong focus on working with the third sector to develop more resilient and
compassionate communities and on prevention and early intervention to support people to
take control of their own health and wellbeing and help them to maintain their independence
for as long as possible.
The strategy puts the patient or service user at the centre of the health and care system and
in control of their care, supported by integrated primary, community and social care services
4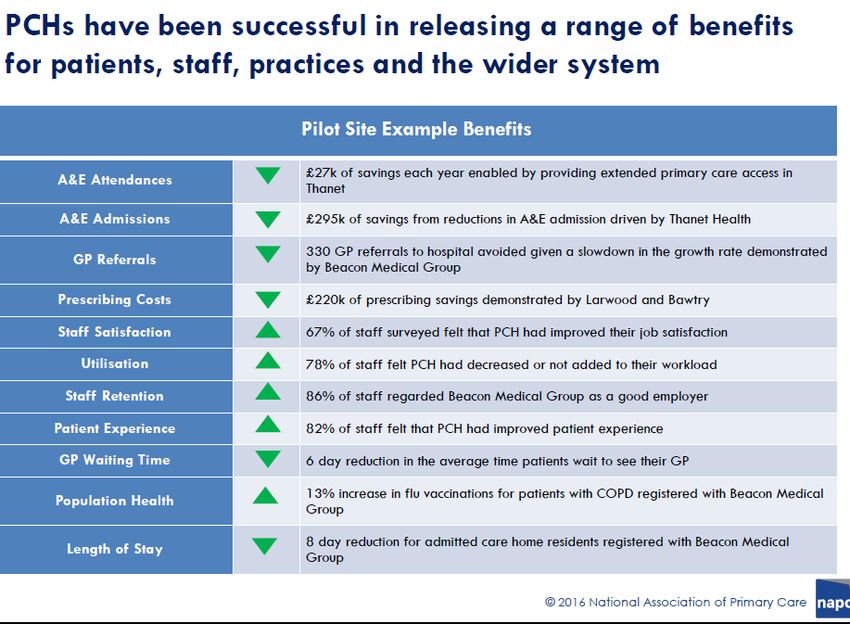
in multi-disciplinary teams (MDTs) who can co-ordinate care to enable the person to achieve
the outcomes that are important to them. Where specialist care is needed this will be delivered
in the community where it is clinically safe to do so.
Our out of hospital plans aim to ensure people only go to hospital when it is clinically necessary
and if admitted they are discharged when they are medically ready with appropriate care and
support in the community if needed.
Strategic Fit
Bedford, Luton and Milton Keynes (BLMK) Sustainability and
Transformation Partnership (STP)
Bedfordshire CCG and Central Bedfordshire Council are part of the BLMK STP. The five
priorities of the STP are:
Priority 1: Illness prevention and health promotion: Preventing ill health and
promoting good health by giving people the knowledge and ability, individually and
through local communities, to manage their own health effectively
Priority 2: Primary, community and social care: Delivering high quality and resilient
primary, community and social care services across Bedfordshire, Luton and Milton
Keynes
Priority 3: Secondary care: Delivering high quality and sustainable secondary
(hospital) care services across Bedfordshire, Luton and Milton Keynes
Priority 4: Digital programme: Working together to design and deliver a digital
programme, maximising the use of information technology to support the delivery of
care and services in the community and in primary and secondary care. BCCG leads
the Information Sharing Phase 1 programme, a key work stream of Priority 4.
Priority 5: Demand management and commissioning: Working together to make
sure the right services are available in the right place, at the right time for everyone
using health and social care in Bedfordshire, Luton and Milton Keynes
The Central Bedfordshire out of hospital strategy is in alignment with the STP. It sets out our
place based plans to support delivery of STP Priority 2 to deliver high quality, and resilient
primary, community and social care services including the development of integrated MDTs
located around clusters of GP practices. The strategy also supports Priority 1 to prevent ill
health including working to strengthen the voluntary sector, and Priority 3 to deliver
sustainable secondary care by providing viable alternatives to A&E for non-emergencies, and
reducing avoidable admissions and delayed transfers of care. The strategy, is also one of the
local building blocks for Priority 5 to develop an Accountable Care System (ACS) across the
BLMK STP footprint.
One of the next stages of the out of hospital work will be to further engage with partners
including providers to understand how and when the strategy will impact on different parts of
the local system so that benefits and risks can be shared by all partners.
5Accountable Care System
In June 2017 NHSE announced that BLMK STP would be one of eight vanguard ACSs in the
first wave of ACS developments across the country. The ACS will be a system in which
commissioners and providers, in partnership with local authorities, take explicit collective
responsibility for resources and population health1. Together, they will manage funding for
their defined population, committing to shared performance goals and a financial system
control total across CCGs and providers.
The ACS will be able to create an effective collective decision-making and governance
structure, aligning the ongoing and continuing individual statutory accountabilities of their
constituent bodies.
In return, the ACS will gain greater freedom and control over the operation of the local health
system and how funding is deployed. The ACS will be given the ability for local commissioners
to have delegated decision rights in respect of commissioning of primary care and specialised
services; a devolved transformation funding package from 2018, potentially bundling together
national funding for the GP Forward View, mental health and cancer; a single ‘one stop shop’
regulatory partnership with NHSE and NHSI in the shape of streamlined oversight
arrangements; and the ability to redeploy staff and related funding from NHSE and NHSI to
support the work of the ACS.
Discussions continue across the BLMK STP around the future ACS system form and the
timeline to becoming a fully functional ACS but the emerging consensus is that a place-based
approach should be taken, aligned to Local Authority footprints an approach that fits with
Central Bedfordshire’s place based approach set out in this strategy.
Challenges
Central Bedfordshire health and care system faces a number of challenges, many of which
are echoed across the BLMK STP footprint and the rest of the country. Central Bedfordshire
is one of the least densely populated unitary councils in England which brings a number of
challenges for commissioning services including increased risk of social isolation and viability
of accessible health and social care services for residents. In addition significant housing
growth is required to meet assessed needs in the borough.
1
An ACS differs from an Accountable Care Organisation (ACO) in that commissioners within an ACO hold a
contract with a single organisation for the majority of services rather than several commissioners holding a
number of contracts.
6Financial challenges:
BLMK system has a predicted financial gap of £311.0m deficit by 2020/11 if we continue to
commission and provide services in the way we are now. BLMK STP is working as a
partnership to reduce this predicted gap.
The local health economy and local government are also operating in an increasingly
challenging financial climate. The growing and aging population and increase in people with
long term conditions has led to an increase in hospital admissions and use of social care
services. The sustainability of the care market is also a challenge, with the impact of rising
costs such as the introduction of the National Living Wage.
Bedfordshire CCG
BCCG has delivered a significant financial turnaround in the years 2014/15 to 2016/17, moving
from a 6% uncontrolled overspend to a surplus position. However, the financial outlook
7continues to be challenging, with any growth monies received being needed to meet
demographic growth and tariff growth. The key financial messages for 2018/19 are:
Business as usual is not sustainable, operationally or financially;
Significant change is required at scale – we need focused commissioning intentions and
transformation of service delivery; this is likely to include different contract types and new
approaches to some service areas;
The anticipated level of allocation growth for the CCG in to 2017/18 is 3.4% with 3.5%
increase in to 2018/19. It is currently anticipated that this will barely offset underlying
demographic growth (1.2% per year) plus the cash impact of tariff growth (estimated to be
2.5% per year);
Currently, 55% of the CCG’s spend funds hospital trust activity, with a significantly smaller
proportion being spent in community services and mental health services. There is a need
to look at how we can redistribute NHS funding differently in the future.
Central Bedfordshire Council
Central Bedfordshire has also seen unprecedented increases in demand for Adult Social
Care with a similar increase in the complexity of cases. The Council is supporting people
to maintain their levels of independence for as long as possible in their own home, thus
avoiding permanent admission to a care or nursing home where this is possible.
However in 2016/17 increases to residential care continued in the 65+ Population and
homecare packages for all ages and client groups also continue to increase with people
living at home longer with complex levels of need.
Adult Social Care gross expenditure on long-term support for older people was 15% higher
than the comparator average in 2015/16, per size of older population.
The council’s expenditure on home care for older people, and on supported living, were
also both comparatively high in 2015/16
The adult social care market in Central Bedfordshire is under pressure and sustainability,
particularly the Home Care market remains a concern.
Population Changes
Central Bedfordshire is a predominantly rural area and is considered to be a highly desirable
place to live and work. It is an area of significant economic opportunity with planned housing
and employment growth. As a consequence the population is growing, rising from 254,400 in
2011 to approximately 278,900 in 2016. Further estimated growth of 19% will see the
population rise to 332,000 by 2031. Although Central Bedfordshire is a relatively affluent area
with life expectancy greater than the national average, there are significant challenges
resulting from an ageing population and pockets of urban and rural deprivation.
Central Bedfordshire has a predominately white British community with only 10.3% of its
residents coming from ethnic minority communities. Migration over the last decade has
largely been from other parts of the UK. The number of people moving into Central
Bedfordshire has been higher than the number of people leaving in each of the years
during the last decade; this is the case both for people moving within the UK and for those
moving internationally.
8 The population in 2016 was 278,900 (ONS 2016 mid-year estimate) and is projected to
rise to 297,700 by 2021, and by 2013 the number of people aged 85 and over is expected
to rise by 90%;
Overall, levels of deprivation in Central Bedfordshire are relatively low. However, five
LSOAs are in the most deprived 10-20% in England; these are: Parkside, Dunstable
Manshead (Downside), Parkside, Houghton Hall / Tithe Farm (Tithe Farm) and Sandy.
Adult Health Needs:
Rates of premature mortality from cancer (lung, colorectal and breast), heart disease, and
stroke and lung disease are higher in Central Bedfordshire than similar Local Authorities.
Alcohol related admissions continue to rise, with admission rates significantly worse than
its statistical neighbours.
GP Survey Data suggests less than two-thirds of people with a long term condition feel
adequately supported by their GP to manage their condition;
The most common cancers resulting in death in those aged 75 years or under were lung,
colorectal, oesophageal and prostate cancers for males and breast, lung, ovary and
colorectal cancers for females.
The number of men aged 18-64 who have a common mental disorder (e.g. anxiety,
depression, obsessive compulsive disorder) is projected to rise from 10,075 in 2014 to
10,075 in 2030 – an increase of nearly 10%. For women the number is projected to rise
from 16,115 in 2014 to 17,454 in 2030 – an increase of 8%.
Between 2013 and 2015 a higher proportion of adults (67.1%) were classified as being
overweight or obese, compared with the England average (64.8%).
The prevalence of diagnosed diabetes in adults aged 17 years and older has continued to
rise and in 2015/16 was 6.0%.Estimates suggest there are 2,850 people with undiagnosed
diabetes.
The prevalence of diabetes is higher in areas with higher deprivation, and people from
Asian and Black ethnic groups are more likely to have diabetes and develop the condition
earlier.
In 2015, approximately 12,205 people aged 65 and over were estimated to have had a fall.
It is important to note that this is the number of people that fall and not the number of falls.
Since 2010-11 injuries due to falls in people aged 65 and over have risen. Consequently,
Central Bedfordshire has fallen from being significantly better than the England average
to being statistically similar.
Children’s Health Needs
In Central Bedfordshire it is estimated that 3,225 children aged 5-16 have a mental
disorder, with a higher number seen in the 11-16 year old age group and in boys.
An estimated 445 new mothers in Central Bedfordshire are affected by mild to moderate
depression, and poor maternal mental health can have long term impacts on the mother,
infant and wider family;
In 2015/16, 13.9% of babies lived in a household with a smoker
Around 1 in 5 five year olds are overweight or obese, rising to 1 in 3 by age ten. Only a
small proportion of children identified as overweight or obese by the National Child
Measurement Programme take up the offer of weight management support;
9 In Central Bedfordshire children are present at almost half of domestic abuse incidents,
the Relay Project alerts schools to children whose parents have been involved in a
domestic violence incident.
Vulnerable groups
At the end of March 2015 there were 275 Looked After Children in Central Bedfordshire
In 2016 1,129 school pupils received Special Educational Needs support;
There were 4,885 adults estimated to have a learning disability, approximately 1.8% of the
local population in 2015. This is expected to rise to 5,796 by 2030 an estimated increase
of 2.2%
592 people with a Learning Disability in receipt of a paid service will have had an up to
date health passport and will have had an annual health check completed by their GP.
Secondary Care
Hospital based services face increasing attendances in A&E up by 12% between 2010
and 2016 with a marked increase in frequent attenders, numbers of emergency
admissions rose by 39% over the same period from 12,336 to 17,141, emergency
admissions in children aged 0 to 4 years doubled over this period but the largest absolute
increase was in working age adults;
The main recorded causes of emergency admissions are respiratory conditions in the 0-4
year olds, and urinary tract infections and respiratory conditions in the over 65s;
The rate of emergency admissions from the most deprived areas is more than double that
from the most affluent areas. Short stays (less than one day and less than five days) have
increased markedly over the last two years;
Delayed transfers of care are also increasing.
Hospitals are also finding it increasingly difficult to meet waiting times targets for A&E,
Cancer waits and planned admissions.
Primary Care
Local GP practices are facing challenges in relation to workforce pressures (difficulties
recruiting GPs and nurses), financial challenges, issues around size and condition of their
premises, and increasing workload as a result of changes within the wider system and the
demographic changes already described. Many local GP practices consider their
businesses to be vulnerable, or their service models to be unsustainable in the long term.
Community Services
Our community based services often operate separately to each other, and some of our
most vulnerable patients with complex needs don’t always receive joined-up care, and
there is a lack of joined up services to prevent unnecessary admissions to hospital.
BCCG has agreed a Service Development Improvement Plan (SDIP) with the current CHS
provider Essex Partnership University NHS Foundation Trust (EPUT) including delivery of
increased capacity in community rehabilitation.
There have been delays in progressing new specifications for the SDIP and in agreeing a
proposal for a Single Point of Access which means delays in achieving service
improvements for patients and service users.
Workforce
10 Across the BLMK footprint the social care vacancy rate is 26.9% and the turnover rate is
11.9%. There are major recruitment issues with qualified/registered staff in general; social
workers, occupational therapists, reablement workers, domiciliary care workers, and
community support workers/ unqualified workers in community social work teams;
Vacancy rates are also high in adult nursing (13.8%), MH nursing (19.4%) and LD nursing
(17%),
BLMK STP footprint has the second highest proportion of GPs due to retire in the next 5-
10 years in East of England at 24%, 4% above the national average. There are more
patients per GP in BLMK STP footprint and the patients are younger than the average
regional and national patient profile.
Estates
Primary care infrastructure in Central Bedfordshire is inadequate for supporting the range
of services intended to be delivered in a community setting in the future. Over half of the
GP practice premises in the area are constrained, which will be further compounded by
significant housing growth planned for the area; there is limited capacity in community
buildings for expanding the range of services delivered; and there are limited opportunities
to co-locate teams into shared bases to support multi-disciplinary working within the
existing configuration of buildings;
Whilst significant progress will be possible through greater use of technology (e.g. mobile
working solutions) and improved information sharing between teams), suitable estates
solutions are required to ensure optimal delivery of the new service model;
Different solutions will be possible within each cluster, based on the suitability and capacity
of existing buildings. “Hubs” will need to operate in partnership with smaller “spoke”
facilities, especially in some of the more rural parts of Central Bedfordshire, to ensure that
services remain easily accessible to all residents within the area.
IT systems and information sharing for patient care
All BCCG GP Practices currently use SystmOne as their clinical system but there is
minimal record sharing across practices and with other providers, such as community and
mental health services and the local acute Trusts;
There is currently no system-wide information sharing agreement, resulting in lost
opportunities to maximise technical sharing capabilities;
Whilst BCCG uses some analytics tools in primary care we do not yet have the functionality
that will be required to deliver the BLMK shared vision regarding risk stratification and
population intelligence.
Patient and service user expectations:
The following graphic synthesises what citizens across the BLMK footprint are saying they
want.
1112
Delivering the Vision
Moving towards becoming an ACS at a BLMK level over the next 2-3 years will provide shared
accountability across the STP footprint for transforming the way care is delivered. The ACS
vanguard priorities are to have integrated services in an integrated system, make tangible
progress in emergency and urgent care reform, strengthen general practice and improve
cancer and mental health services.
The Central Bedfordshire out of hospital strategy sets out how we will transform services
locally, in alignment with STP and ACS priorities, building on the progress that has already
been made and bringing together significant developments that are underway or in the
development stage. The key areas of work are described in the next sections.
Transforming health and social care
Integration offers the opportunity to improve outcomes for people as well as ensuring better
use of resources, financial, estates and workforce. Crucial to this is making better use of public
assets to deliver new models of care and is a key ambition of our STP. In this context, our
approach in Central Bedfordshire is to focus on the ‘Place’.
At its heart, the aim is to secure access to the right care, in the right place and at the right
time. Central to this, is a drive for transformational change across health and social care
based on integrated and seamless care pathways at locality levels. Care should be
coordinated around an individual’s needs with prevention and support for maintaining and
maximising independence at its core. This should be underpinned by the following principles:
Care coordinated around the individual
Decisions made with, and as close to, the individual as possible
Care should be provided in the most appropriate setting; and
Funding flowing to where it is needed.
These principles are importantly centred on our local ambition for the development of an
integrated health and care hub in each locality in Central Bedfordshire as a focal point for
joining up health, social care and other council services and the delivery of care closer to
where people live.
Integrated Health and Care Hubs are crucial to shifting the balance of care from acute
hospitals to a more community-led approach as well as helping to reshape the primary model
which delivers primary care at scale. A locality based integrated health and care hub approach
improves cooperation and joined up working which improves the access and quality of care
provision. It also leads to a reduction of inappropriate hospital admissions and importantly
supports the vision for integrated primary and community services at scale as set out in the
General Practice Forward View.
Central Bedfordshire’s population distribution and its relation to secondary care providers
make it important that the primacy of the Integrated Health and Care Hubs approach is
sustained. Services will be more accessible to people, especially in predominantly rural areas,
and will meet the requirements for delivering health and care services to an expanding and
ageing population. The Integrated Health and Care Hubs will be the main centres for providing
proactive and preventative care, out of hospital services and care packages for people who
are vulnerable or have complex care needs. The Hubs will provide support to children with
complex health needs and the transition from children to adult services.
13By developing greater range and capacity in community-focused care it will be possible to
deliver improved health and care experiences as well as more effective use of resources by:
1. Reshaping the model for prevention and early intervention – through an
integrated approach to primary, secondary, and tertiary prevention to stop or
reduce deterioration in health.
2. Supporting people with long term conditions through multi-disciplinary
working – focussing services around general practice in locality networks and
helping people to manage their own conditions in the community.
3. Expanding the range of services that support older people with frailty and
disabilities – integrating the range of housing, mobility, carers and other services
that wrap around older people with specific conditions and issues and helping to
manage new demand including through the Care Act.
4. Restructuring integrated care pathways for those with urgent care needs –
ensuring that these are seamless, clear, and efficient to help deliver the clinical
shift required to move care away from acute settings, where appropriate, as well
as building future resilience for the responsibilities of the Council under the Care
Act 2014.
The multiplicity of inputs to health and social care, with different agencies and commissioners,
represents a major challenge to the development of integrated and joined up services. Our
vision for integration sees the development of jointly commissioned services as an important
mechanism for overcoming those challenges and securing more cost effective and coherent
services.
There will be a changed relationship between the Council, Health Commissioners and
Provider organisations to enable a greater focus on meeting the needs of the local population.
The STP through the ‘place based’ approach provides a platform for bringing together strategic
decision making between the Council and BCCG and at a ‘cluster’ level between medical
health, social care and the wider community based practitioners. This will translate into:
simpler means of aligning our resources;
collaborative commissioning
integrating hospital services with GP, community health and social care
building capacity and resilience in our communities to be self sustaining
expanded use of assistive technology.
Our vision for out of hospital services recognises the importance of high quality and accessible
secondary and tertiary health care to our population through better and more cost effective
use of hospital services. Local access to appropriate services would prevent people, especially
frail older people, making unnecessary journeys to hospitals and would make important
difference in care outcomes, quality and experience, particularly for those with long term
conditions. Only those people requiring the use of highly specialist diagnostic equipment or
acute hospital facilities would need to be travel out of their local areas.
However, it is important that community based care is underpinned by integrated multi-
disciplinary teams working together within a planned whole systems approach to care delivery.
The co-location of health and care teams in fit for purpose facilities is central to managing
demand and ensuring the future sustainability of our health and care systems.
This approach is consistent with our STP’s Primary Care Home model, through a ‘cluster
based’ approach with health and social care teams working collaboratively with community
14and voluntary groups to empower people to increasingly self-care, improve wellbeing and to
use their own informal and existing networks of support.
Locality Based Delivery Model
The emerging model sees healthcare being delivered through a number of integrated health
and care hubs based on the four localities in Central Bedfordshire. These would provide a
focal point for the provision of out of hospital care services in each locality. Within each locality
there will be an integrated multidisciplinary approach, with ‘one team’ working across
organisational boundaries. The focus of the team’s work will be on a local population covering
a GP grouping or clusters with populations of 30 – 50,000.
As a minimum these hubs are expected to serve as a base for the multi-disciplinary teams
(adults and children’s) being established as part of the community services redesign
programme, including general medical services where possible.
These Hubs will enable the development of new models of care where general practices,
particularly groupings of Practices (Primary Care Networks), will be more effectively and
flexibly integrated with community, mental health and social care.
Bedfordshire Primary Care Home (PCH) Model
Primary Care Home (PCH) Model is based on a hub and spoke model and is an innovative
approach to strengthening and redesigning primary care developed by the National
Association for Primary Care (NAPC). Critically, the model brings together a range of health
and social care professionals to work together to provide enhanced personalised and
preventative care for the local community.
Staff come together as a complete care community drawn from GP surgeries, community,
mental health and acute trusts, social care and the voluntary sector to focus on local
population needs and provide care closer to patients’ homes.
There key characteristics that make up Central Bedfordshire PCH model are:
15 an integrated workforce2, with a strong focus on partnerships spanning primary,
community, secondary and social care;
a combined focus on personalisation of care with improvements in population health
outcomes;
provision of care to a defined, registered population of between 30,000 and 50,000.
the GP remains central to patient care and care planning, supported by the multi-
disciplinary team to coordinate care across the health and social care system;
there is shared decision making and involvement during transitions between sites of care;
designed around a ‘hub and spoke’ model for where services are delivered. The hub and
spoke model will ensure there is a networked range of services available to each defined
population with some services operating across clusters or the borough as shown in the
following diagram.
The PCH model will ensure care is designed around patients, ensuring they receive the right
care in the right place at the right time. GPs remain central to patient care, working as
members of multi-disciplinary teams (MDTs) of health and care professionals so that
community, mental health, social care and appropriate secondary care services can be
integrated with primary care, drawing in voluntary sector support and also aligning with local
council services. Crucially, MDTs will share information enabling shared care planning and
more joined up care as well as making use of new roles in health and care such as Community
Geriatricians and Care Navigators3. Other members of the team such as Pharmacists will be
enabled to work more closely with MDT colleagues.
2
Integrated care as defined by NHS England: For health, care and support to be ‘integrated’, it must be person-
centred, coordinated, and tailored to the needs and preferences of the individual, their carer and family. It
means moving away from episodic care to a more holistic approach to health, care and support needs, that
puts the needs and experience of people at the centre of how services are organised and delivered.
(https://www.england.nhs.uk/ourwork/part-rel/transformation-fund/)
3
A community care navigator is someone that helps people find their way through the many health, care and
voluntary services available - so they get the right service to meet their needs. They also help people develop a
16Where possible, MDTs will work together in shared buildings or hubs, offering a wider range
of joined-up services within the community. Where co-location is not possible or desired MDTs
will work together in ‘virtual hubs’, providing the same function and still working as a single
team and where necessary making use of other hubs in the area that may provide a wider
range of services including those previously delivered in a hospital setting.
The diagram below shows how this new model of care, adapted from the National Association
of Primary Care (NAPC)’s Primary Care Home Model, will work for people in Central
Bedfordshire including those with mental health, learning disability, physical disability or
sensory loss needs. :
plan that works for them and link people with community resources to support them in taking action to
improve their health and wellbeing.
1718
Commissioners have agreed initial key priorities to creating an integrated health and care
system, which will bridge provider boundaries to deliver joined up care without the need for
people to tell their story multiple times, up-skill teams to undertake single assessments on
behalf of multiple providers thereby reducing the number of referrals between services and
the number of individual interventions. This is currently being progressed through a joint
Associate Director post between Essex Partnership University Trust (EPUT) Community
health services and Central Bedfordshire Council’s Social Work practitioners.
The key elements for successful delivery are:
Shared care records
Primary care operating in clusters or networks and ‘at scale’
Development of Multi-disciplinary teams within cluster neighbourhoods
Specialist services designed to support cluster teams
Co location or flexible/shared working locations
Joint Risk Stratification
Pooled budgets (where appropriate)
Joint commissioning (where appropriate)
Integrated operational management
Services will be shaped around local populations and commissioners have agreed to adopt
the National Association of Primary Care model (NAPC), Primary Care Home (PCH). This will
ensure that services are developed around a 30,000 to 50,000 population with the GP being
at the centre of (but not necessarily co-ordinating) the patient’s care.
What will this mean to local people?
Local people will have access to more joined-up health and care services closer to home.
People will experience real improvements in primary care and community based support,
when it is needed.
By 2019, our journey from fragmented working to an integrated and person-centred approach
will be fully embedded. These changes in the way services are organised will mean our
population will:
Experience seamless access to a timely, coordinated offer of health and care support.
Have access to a wider range of support to prevent ill-health, with increased emphasis
on early interventions supported by voluntary, community and long-term condition
groups, enabling them to stay healthier for longer;
Be supported to remain independent with integrated GP and community
multidisciplinary teams delivering care directly within their own home wherever it is
possible to do so;
Have access to a wider range of health and care services in the community that will
help to avoid unnecessary hospital admission and, following any necessary admission,
will enable discharge to home care as soon as it is safe to do so;
Have access to mental health services that are integrated with physical health and
social care services, through acute, primary, community and specialist teams and
aligned to lifestyle Hubs.
Have access to integrated rehabilitation and reablement services that will avoid or
minimise the need to enter into residential or nursing home care;
19 Experience reduced variations in care with improved outcomes;
Have support for carers that is timely and person centred with an integrated response
underpinned with joint planning and assessment, as appropriate;
Experience services that are person-centred, highly responsive and flexible, designed
to deliver the outcomes important to the individual; and
Benefit from stream-lined and integrated working with joint information systems.
Community Health and Care Services
As an integrated health and care economy, our vision is that over time discrete silos of current
health and care provision will be replaced with an integrated model of care aimed primarily at
supporting patients to be self caring, independent and less reliant on acute or specialist
intervention. By developing greater range and capacity in community-focused care it will be
possible to deliver improved health and care experiences as well as more effective use of
resources by:
Reshaping the model for prevention and early intervention – through an integrated
approach to primary, secondary, and tertiary prevention to stop or reduce deterioration
in health.
Supporting people with long term conditions through multi-disciplinary working –
focussing services around general practice in locality networks and helping people to
manage their own conditions in the community.
Expanding the range of services that support older people with frailty and disabilities –
integrating the range of housing, mobility, carers and other services that wrap around
older people with specific conditions and issues and helping to manage new demand
including through the Care Act.
Restructuring integrated care pathways for those with urgent care needs – ensuring
that these are seamless, clear, and efficient to help deliver the clinical shift required to
move care away from acute settings, where appropriate, as well as building future
resilience for the responsibilities of the Council under the Care Act 2014.
A joint procurement programme is underway between BCCG, Bedford Borough Council (BBC)
and CBC to procure Community Health Services (CHS), including adult services and 0-19
children’s services. The new contract is due to commence on 1st April 2018. The procurement
approach being used is Competitive Dialogue and the commissioning model will be based on
delivery of the Adult and Children’s outcomes frameworks. Where no baseline has been set
for an outcome indicator the provider and commissioners will work together to agree a baseline
and trajectory during the first year of the contract. Adult and Children’s Outcome Indicators
are set out in Appendix 1. We will seek to measure these on a population basis rather than
caseload.
The vision for the new Community Services contract is to:
Support the redesign of community health services in the establishment of multi-
disciplinary primary care led working to deliver proactive case management within
geographical clusters of GP practices, with input from GPs, community geriatricians,
practice nurses, community nurses, community advanced nurse practitioners, ANP
Support Workers/, therapists, mental health workers, pharmacists, social care
practitioners, care navigators, , and the voluntary sector.
20 The specification sets out an expectation that the provider will work with Primary Care
and other providers to achieve the outcomes expected of MDT’s which are:
o Reduced avoidable admissions for patients at risk of admission;
o Timely discharge from inpatient acute care as soon as possible when acute
care no longer adds value;
o Reduced spend on medications for frail elderly patients;
o Reduced recurring admissions for the frail elderly;
o Optimise partnership approach between primary, community and secondary
health and social care providers;
o Rapid access to co-ordinated multi-disciplinary assessment and care planning
such as comprehensive geriatric assessment;
o Improved access to specialist knowledge, e.g. cardiac; Increased engagement
of family and support network in assessment and care planning;
o Improved patient and carer experience;
o Engagement with patients and carers to achieve specific outcomes for the
individual.
Procuring a new community services contract based on delivery of outcomes supports our
plans to fundamentally change how community care and support is provided to the population,
integrating with primary and social care services and working in multi-disciplinary teams in a
place based model with a Single Point of Contact.
Optimising planned care pathways / delivering more care closer to home
The NHS RightCare programme aims to improve population-based healthcare by focusing on
value, increasing quality and releasing funds for reallocation to address future demand.
RightCare, together with the New Care Models, support the vision set out in the Five Year
Forward View with its focus on the transformation of healthcare services to drive
improvements in quality and efficiency.
BCCG has been compared to the 10 most demographically similar CCGs in order to identify
realistic opportunities to improve health and healthcare within our population. Based on the
October 2016 ‘Commissioning for value: where to look pack’ the data indicates the potential
to save 28 lives and £13.5m spend per year by addressing variation in planned care. The aim
of the BCCG RightCare Programme is to ensure that commissioning plans are focused on the
opportunities that have the potential to provide the biggest improvements in health outcomes,
resource allocation and reducing inequalities. We have committed to reviewing at least 40%
of the financial opportunity in 2017/18 and a further 40% in 2018/19.
Whilst the approach of the RightCare Programme is Bedfordshire-wide, there are instances
where services need to be commissioned on a locality footprint. We are working collaboratively
with members of Public Health to reflect the needs of our population on the services we are
commissioning.
We are also working with general practice to reduce referral variation by ensuring Advice &
Guidance is available and Peer to Peer Review of all referrals is implemented by October
2017.
21Streamlining and improving the offer of urgent and out of hours services.
Following a procurement programme BCCG in partnership with Luton CCG (LCCG)
commissioned Herts Urgent Care (HUC) to provide an integrated 111 / Out of Hours service
from March 2017. Whilst this service brings together both 111 and GP out of hours services
with the aim of ensuring urgent care services are easier to navigate for patients it is still
bedding down and there are challenges with ensuring the service is viable and meets
standards required. A joint Remedial Action Plan is in place to support full mobilization,
including trajectories to achieve a full staffing model against plan.
BCCG has also commissioned a Hear and Treat service allowing extra time for more detailed
assessment of 999 calls increasing the proportion of calls resolved through telephone advice
(Hear and Treat) by up to 30 per cent, freeing ambulances for patients who need to be treated
at the scene and taken to hospital. It also reduces the proportion of patients treated at the
scene (See and Treat) by around 10 per cent and reduces the proportion of patients taken to
hospital by around 10 per cent. This improves the efficiency of the service overall, and reduces
pressure on A&E Departments4.
Benefits of PCH Model
Quantitative benefits
A review of 15 Rapid PCH Test sites shows the range of quantitative benefits that can
be achieved and that benefits can be expected across the system.
4
https://www.england.nhs.uk/2015/01/medical-accuracy/
22Qualitative Benefits
Staff benefit from workforce development and improved team working and
collaboration across all agencies and breaking down barriers and silo working;
Staff working at the top of their licence;
Commissioners realise more efficient and effective use of resources; use of innovative
and wider range of contractual arrangements based on outcomes; sharing benefits
and risks;
Providers work together to share system benefits and risks and
o Primary care – MDTs working around clusters of practices will release more
time for GPs leading to more sustainable general practices supporting each
other, sharing services and best practice;
o Community services – Playing integral role in prevention and early intervention,
and support for admission avoidance and early discharge;
o Social care – More focussed approach to rehabilitation, reducing or delaying
the need for long term and high cost packages of care;
o Secondary care – improved patient flows and reduced at the front door.
National Delivery Areas
The underlying transformation of how health and care services are organised around the PCH
model (integrated primary, community and social care services and multi-disciplinary teams
co-located around primary care clusters) will support the delivery of improvements in
outcomes for the whole population. The out of hospital strategy has identified a number of
delivery areas which will also support the following NHSE Planning Guidance 2017/2018 and
2018/2019 must do’s :
1. Finance Deliver financial control totals, moderate demand and increase
provider efficiency.
2. Primary Care Ensure the sustainability of General Practice, extend access and
support General Practice at scale.
3. Urgent and emergency care Deliver the four A&E standard including the seven elements of
the A&E improvement plan, eight high impact changes and
priority standards for seven day hospital services; reduce
ambulance conveyances, to meet the 15 minute Ambulance
handover.
4. Referral to treatment times and Deliver the constitutional standard for referral to treatment times,
elective care streamline elective care pathways, including outpatient
redesign, 100 per cent use of e-referrals, and deliver the national
maternity services review.
5. Cancer Deliver cancer standards, implement the national cancer task
force report, improve one year survival rates, roll out follow up
pathways starting with breast cancer
6. Mental Health( IAPT/Dementia Deliver the implementation plan for the Mental Health Forward
standards) View, ensure delivery of the mental health access and quality
standards, increase baseline spend on mental health, maintain
a dementia diagnosis rate of at least two thirds; eliminate out of
area placements for non- specialist acute care.
7. People with learning disabilities Deliver Transforming Care Partnership plans, reduce in-patient
bed capacity for people with learning difficulties, improve access
to healthcare for people with learning disabilities and reduce
premature mortality.
8. Improving quality in organisations Implement plans to improve quality of care.
23What We Have Already Achieved
BCCG and CBC have worked in partnership over many years to improve health and care
services, integrating teams and working across agencies to provide joined up and seamless
services where possible. BCCG has also been working with GPs to develop plans for ensuring
general practice is sustainable for the longer term.
The following sections set out some examples of where we have made tangible progress in
improving services and outcomes across the Central Bedfordshire system.
Primary Care
GP practices in the Central Bedfordshire Localities (Chiltern Vale, Leighton Buzzard, West
Mid Beds and Ivel Valley) have established clusters which will form the basis of the Primary
Care Home model and discussions are underway between BCCG and CBC to agree the
details of the hub and spoke model for Central Bedfordshire.
Many of the clusters are starting to develop shared functions from 17/18, particularly around
how they manage the care of frail elderly patients, as part of delivery of the local GPFV Plan.
There are a number of schemes in place to try to ease pressures on general practice including
Workflow Optimisation. This is a training programme designed to improve capacity in general
practice by training GP practice clerical teams to read, code and action incoming clinical
correspondence. It has now been adopted by NHSE as one of the 10 High Impact Actions to
release time for care. Embedding the methodology in practice has the potential to save up to
40 minutes of GP time per day, provides for a new enhanced role (Clinical Administrators)
within the practice, increases skill mix and builds closer multi-disciplinary working
relationships.
Since January 2017 within the Central Bedfordshire Borough practices we have successfully
trained 18 Clinical Administrators and 16 GP Champions in workflow optimisation to reduce
workload for our GPs. We have also recruited 3 Clinical Pharmacists and increased the
number of Practice Nurse mentors by 15.
BCCG has also implemented GP referral to acute trust for Same Day Assessment pathway.
GP surgeries are provided with a unique telephone number to use when they need to refer a
patient in for same day assessment or to access advice and guidance to avoid an admission.
The calls are answered and managed by nursing staff within the Ambulatory Emergency Care
(AEC) unit and if necessary patients are brought into AEC for initial assessment.
A GP referral to acute trust for Same Day Assessment pathway has been introduced. GP
surgeries are provided with a unique telephone number to use when they need to refer a
patient in for same day assessment or to access advice and guidance to avoid an otherwise
admission. The calls are answered and managed by nursing staff within the Ambulatory
Emergency Care (AEC) unit and if necessary patients are brought into AEC for initial
assessment.
Healthy Living Pharmacy
There are 74 community pharmacies across Bedfordshire, which are community assets able
to promote health and wellbeing in the communities they serve. The Health Living Pharmacy
(HLP) framework aims to utilise community pharmacies to meet local need, improve the health
and wellbeing of the local population and help to reduce health inequalities. This can be
24You can also read