Precision Medicine in Colorectal Cancer 2021 - Michael Morse, MD Professor of Medicine
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Precision Medicine in
Colorectal Cancer
2021
Michael Morse, MD
Professor of Medicine
Duke University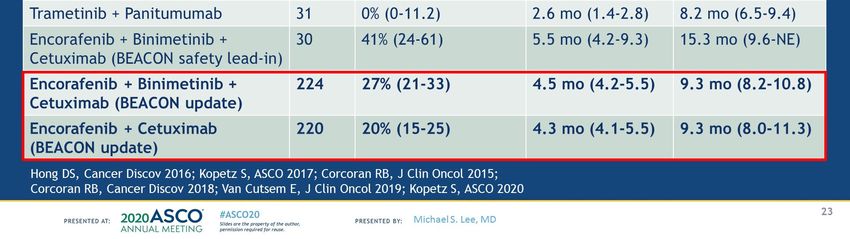
Disclosures
Biomarker Subgroups in CRC This lecture will not address MSI‐H and TMB‐H
RAS mutation ± 45%
PIK3CA/PTEN mutation 8% PIK3CA/PTEN mutation
1% p6 235-237,
2%
2%1% 26%
2% 2%2%
Kinase inhibitor 8%
MET inhibitor
Anti‐HER2 Tx Wild type
Anti‐PD‐1/PD‐L1 Anti‐EGFR therapies
BRAF V600E
BRAF inhibitor + anti‐EGFR ± MEK inhibitor
Dienstmann. ASCO Ed Book. 2018. Slide credit: clinicaloptions.com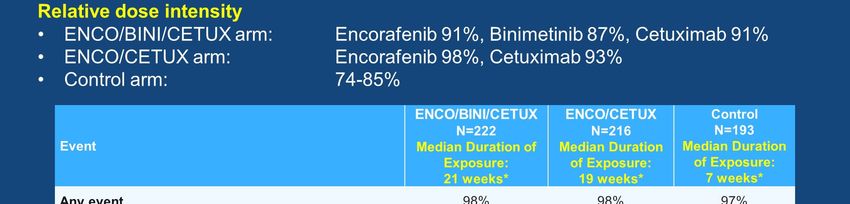
Next‐generation sequencing results of TRIBE2 study
BRAF V600E
KRAS G12C
HER2 Ampl
HER2 Mut
MSI‐H
POLE mut
TMB high
Right sided
20% had “actionable” alterations
Antoniotti C, Eur J Cancer. 2021 Aug 5;155:73‐84.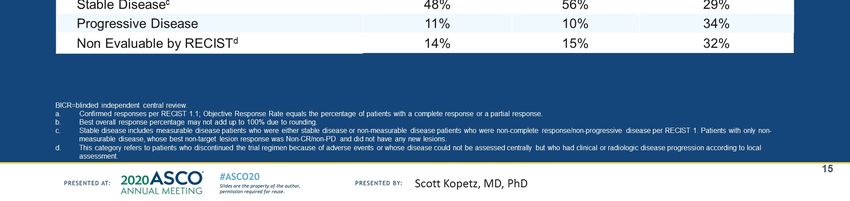
BRAF V600E Targeting
This section is courtesy John Strickler, MD
BRAF V600E mutant mCRC has poor prognosis with chemotherapy Presented By Michael Lee at ASCO 2020
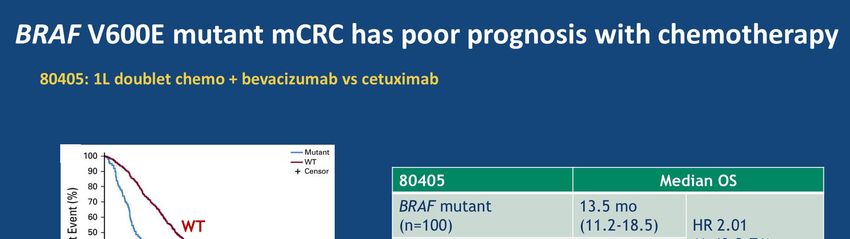
BRAFV600E mutations in metastatic CRC
• ~5‐8% of CRC
• Right sided
• High grade
• More likely to be MSI‐H
• Poor prognosis
• Limited benefit from anti‐EGFR
therapy
Strickler et al., Cancer Treat Rev. 2017 Nov;60:109‐119.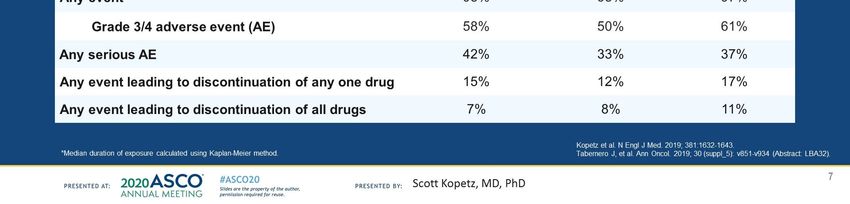
Rationale for inhibition of BRAF + EGFR +/‐ MEK
Presented By Eric Von Cutsem at 2018 ESMO GI Meeting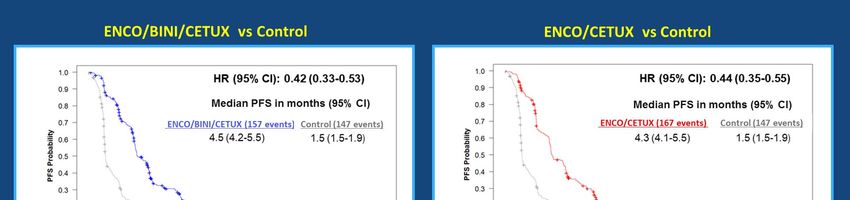
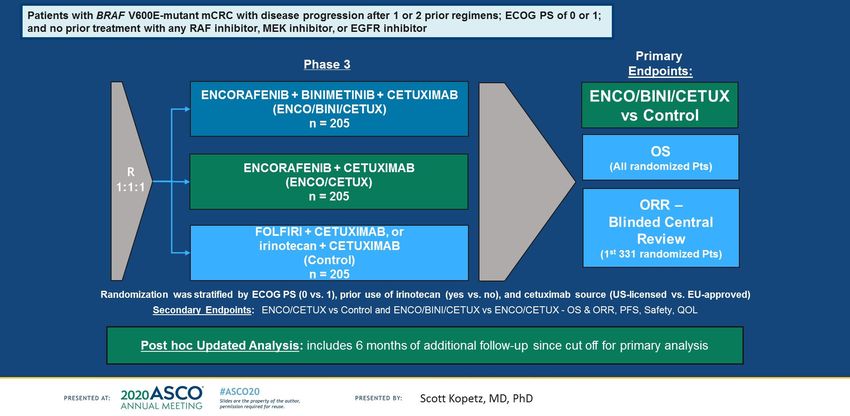
BEACON CRC Phase 3 Study Design
Kopetz et al., J Clin Oncol 38: 2020 (suppl; abstr 4039)
Van Cutsem. JCO. 2019;[Epub]. Taberno. ESMO 2019. LBA32. Kopetz. NEJM. 2019;[Epub]. NCT02928224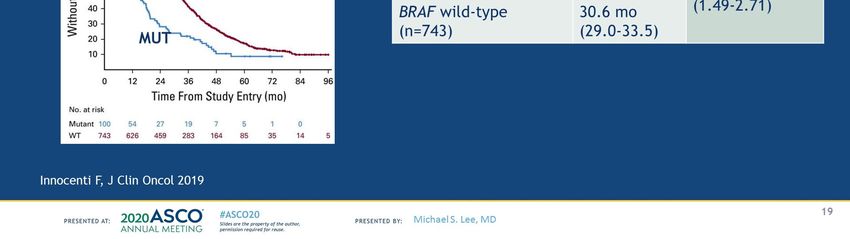
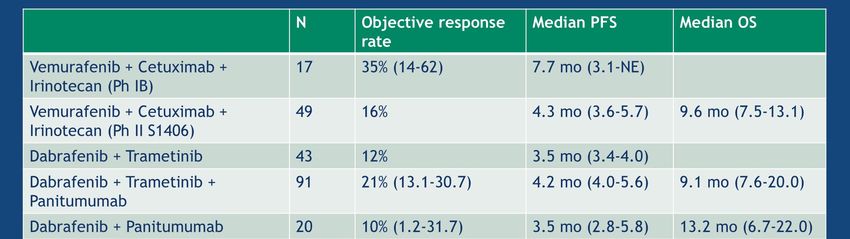
BEACON: Updated Overall Survival
Kopetz et al., J Clin Oncol 38: 2020 (suppl; abstr 4039)BEACON: Updated Objective Response Rates
Kopetz et al., J Clin Oncol 38: 2020 (suppl; abstr 4039)BEACON: Updated Progression Free Survival
Kopetz et al., J Clin Oncol 38: 2020 (suppl; abstr 4039)Overall Summary of Safety
Kopetz et al., J Clin Oncol 38: 2020 (suppl; abstr 4039)ANCHOR CRC: A SINGLE‐ARM, PHASE 2 STUDY OF ENCORAFENIB, BINIMETINIB PLUS CETUXIMAB
IN PREVIOUSLY UNTREATED BRAFV600E–MUTANT METASTATIC COLORECTAL CANCER
Grothey, ESMO2020, LBA5Recent prior studies in BRAF mutant CRC Presented By Michael Lee at ASCO 2020
Encorafenib + anti‐EGFR is the new standard of care
for BRAFV600E mutated metastatic CRC
• Can we give encorafenib + anti‐
EGFR 1st line?
• Are there patient sub‐populations
who need the triplet (anti‐MEK)?
• What to do after progression?HER2 (ERBB2) targeting in mCRC
HER2 in mCRC ~3% of patients with mCRC Usually left sided Primary resistance to EGFR monoclonal antibodies (cetuximab, panitumumab) Not mutually exclusive with RAS mutations Probably not prognostic Different ways to measure HER2 expression (IHC, ISH, NGS on tissue; NGS on ctDNA)
Different studies used different criteria
Ann Oncol. 2018;29(5):1108–1119.
(More stringent)
NGS (cutoff 6): Applying HERACLES diagnostic criteria, IHC and NGS show 92% concordance
at the positive HER2 cutpoint and 99% concordance if equivocal cases are also considered positive
Am J Clin Pathol. 2019 Jun 5;152(1):97-108HER2 amplification by tissue vs ctDNA vs IHC
Tissue NGS vs IHC: Applying HERACLES diagnostic criteria, IHC and NGS show 92% concordance
at the positive HER2 cutpoint and 99% concordance if equivocal cases are also considered positive
Am J Clin Pathol. 2019 Jun 5;152(1):97-108
International Cohort of mCRC tested for HER2+ by
tissue (IHC, ISH, NGS) or blood (NGS)
Raghav, ASCO2021;abstract 3589Determining HER2 positivity-NCCN
HER2 targeting (NCCN guidelines) for HER2
amplified and RAS/BRAF WT
Trastuzumab+ [pertuzumab or lapatinib] or fam-
trastuzumab deruxtecan nxki
Initial Therapy: Pt not appropriate for intensive therapy
Subsequent therapy
Notes activity for fam-trastuzumab deruxtecan nxki in
some with prior HER2-targeted treatmentHER2 targeted therapy in mCRC
Therapy Study Criteria Outcome
Trastuzumab + Laptinib 1HERACLES-A HER2+ mCRC with PD post std tx ORR: 28%, SD 41%
PII, N = 32 KRAS exon 2 wt mPFS 4.7m, mOS 10m
Trastuzumab + Pertuzumab 2MyPathway HER2+ mCRC refractory to std tx ORR 31% (KRAS wt)
PII, N = 84 (allowed mKRAS; 68 were wt) 3mPFS 5.3m (KRAS wt)
3mOS 14m (KRAS wt)
4TRIUMPH
Trastuzumab + Pertuzumab HER2+ mCRC, refract to std tx ORR 35%
PII, N = 17 (tissue) RAS wt mPFS 4.0m
Trastuzumab + Pertuzumab TAPUR
5 HER2+ mCRC, no std tx options ORR 25%, DCR 50%
PII, N=28 No data on RAS mPFS 4 m; mOS 25m
Trastuzumab + Tucatinib 6MOUNTAINEERP HER2+ mCRC, prior F, Ox, Iri, VEGF ORR 55%, SD 9%
II, N = 26 RAS wt mPFS 6.2m, mOS 17m
7HERACLES-B HER2+ mCRC, refract to std tx
T-DM1 + pertuzumab ORR 10%, SD 68%
PII, N=30 RAS/BRAF wt mPFS 4.1
8DESTINY-CRC01 HER2+ mCRC , ≥2 prior regimens.
Fam-Trastuzumab ORR 45%; DOR 7m
deruxtecan (T-Dxd) PII, N=54 RAS wt mPFS 6.9m; mOS 15.5 m
1Tosi F, 2020 Dec;19(4):256-262.e2. 2Meric-Bernstam, ASCO 2021; 3004. 3Meric-Bernstam, Lancet Oncol. 2019;20:518-530. 4Nakamura Y, ESMO 2019.
5Gupta R, GI ASCO 2020. 6Strickler, ESMO2019; 527PD. 7Sartore-Bianchi, ESMO Open. 2020;5(5):e000911. 7Yoshino ASCO2021;3505Balancing efficacy and toxicity
Adapted from M. Lee, ASCO2020Other considerations: Need adequate HER2 expression
Destiny-CRC01 cohorts with IHC2+/ISH- and IHC1+ had minimal benefit from T-Dxd
HER2 IHC 3+ or 2+/ISH+
HER2 IHC 3+ or 2+/ISH+
Adapted from Yoshino ASCO2021;3505Even among the HER2+, better response if IHC3+
Adapted from Yoshino ASCO2021;3505mKRAS generally does not respond
In MyPathway study
Not known if T-Dxd has activity in mRAS Meric-Bernstam, ASCO 2021; 3004.Activity for T-Dxd in prior HER2 treated pts
Adapted from Yoshino ASCO2021;3505Resistance to HER2 targeted therapy
Pts progressing
After T + lapatinib
ERBB2,
RAS,
PIK3CA
mutations
are associated
with resistance
to HER2 blockade
in mCRC
Siravegna, Cancer Cell 2018;34:148–162.e7.HER2 mutations generally do not respond, but….
HER2 mutations in ~ 2% of mCRC patients
– Concurrent HER2 amplification and mutation found in ~ 0.5%.
HER2 mutations clustered in TK, JM, TM, and EC domains.
Mutations in the tyrosine kinase domain (L755S, V842I, D769Y, and
K753E) increase kinase activity and are resistance to both anti-HER2
antibodies and small-molecule HER2 kinase inhibitors
Mutations in the ECD, such as S310F and S310Y, lead to the increased
dimerization of HER2 and subsequent signaling
– Remain sensitive to both trastuzumab and HER2 TKIs
Case report of patient with RAS WT metastatic CRC and a concurrent HER2 amplification
and HER2 S310F mutation who responded to trastuzumab/lapatinib and briedly to T-Dxd
Wang, J Natl Compr Canc Netw. 2021 Jun 30;19(6):670-674.Current anti-HER2 trials for metastatic CRC
Trial Ph Treatment Line Comments
Cetuximab +
National
irinotecan vs
SWOG-1613 II ≥ 2nd cooperative
Trastuzumab +
group study
pertuzumab
NSABP Neratinib
Primary
foundation: II +Trastuzumab or ≥ 3rd
endpoint PFS
NCT03457896 Neratinib + Cetuximab
Pyrotinib + ≥ 3rd Conducted in
NCT03843749 II
trastuzumab China
Courtesy of John Strickler, MDKRAS G12C targeting in mCRC
KRAS mutations in mCRC
Most mutations are in glycine12 (G12), glycine13 (G13),
and glutamine61 (Q61).
These mutations prevent GAPs from accessing GTP
so that hydrolysis is blocked, resulting in a persistently
activated GTP‐bound state
Merz, Front. Oncol., 11 March 2021KRAS G12C in mCRC and inhibitors
Drugs targeting KRAS directly are challenging to develop because of its small size,
smooth surface, and strong binding affinity for GTP (and high amount of GTP present in cells)
Sotorasib forms an irreversible, covalent bond
with the cysteine residue of KRAS G12C,
holding the protein in its inactive GDP bound
Adagrasib is also a covalent inhibitor of KRASG12C
that irreversibly and selectively binds KRASG12C
in its inactive, GDP‐bound state
KRAS has a protein resynthesis half life of 24 hrsSotorasib (AMG510) CodeBreak100: Study Design
Phase 1, Multicenter, Open-Label Study – Dose Escalation Dose Expansion
– 2–4 patients enrolled in
each cohort
– Intra–patient dose Cohort 4
Key Eligibility escalation allowed 960 mg
Screening / Enrollment
Screening / Enrollment
Long Term Follow-upa
Long Term Follow-upa
– Additional patients
Safety Follow-up &
Safety Follow-up &
– Locally advanced or
may be added to any
metastatic malignancy
dose deemed safe Cohort 3
– Received prior 720 mg Patients with
standard therapies KRASG12C mutant
– KRAS G12C mutation advanced tumors
as assessed by Cohort 2 – Repeated oral daily Expansion dose
molecular testing of 360 mg dosing with 21-day cycles determined
tumor biopsies – Treatment until disease
– No active brain Cohort 1 progression, intolerance,
metastases 180 mg or consent withdrawal
– Radiographic scan every 6
weeks
Primary endpoints: dose limiting toxicities (DLTs), safety
Key secondary endpoints: PK, objective response rate, duration of response, disease control rate, PFS, duration of stable disease
a30 (+7) days after end of treatment for safety follow-up; every 12 weeks for long term follow-up. PK: pharmacokinetics; PFS: progression-free survival.
Target dose for expansion: 960mg Q.D.
Presented By John Strickler at 2020 ESMO World GIEfficacy in CRC
Best percent change in tumor burden from baseline
100
Best Percent Change from Baseline in
Efficacy measures N=42
80
Sum of Longest Diameters
60 PD PD Objective response rate 7.1% (3/42)
40 Disease control rate 76.2% (32/42)
PD PD SD SD
PD SD SD
20 PD SD SD
SD SD SD* SD SD SD* SD SD* PD
0
PD SD SD SD SD
-20 SD SD SD SD SD* SD
SD SD SD* SD
-40 PR* PR* PR*
-60
-80
-100 *Treatment ongoing Planned Dose: 180 mg 360 mg 720 mg 960 mg
All 3 responses were confirmed and ongoing as of cutoff
Progression-Free Survival
All dose levels (N = 42)
1.00 960 mg (N = 25)
PFS, month Median (min, max)
All doses 4.0 (0.7, 11.0) 0.75
Probability
960 mg 4.2 (1.2, 5.7+) 6‐mo PFS KM estimate:
0.50
• All doses: 20.6%
+: censored value.
3‐mo PFS KM estimate:
• All doses: 58.5%
0.25
• 960 mg: 59.7%
0.00
0 2 4 6 8 10
Number at risk Months
All doses 42 32 18 2 1 1
Presented
960 mgBy John
25 Strickler at 2020
20 ESMO
12 World GI 0 0 0Patient Incidence of Adverse Events
Treatment-related adverse Treatment-related adverse
events events of any grade N = 59, n (%)
N = 59, n (%) occurring in > 1 patients
Any grade 27 (45.8) Diarrhea 10 (16.9)
Grade ≥ 2 12 (20.3)
Fatigue 6 (10.2)
Grade ≥ 3 3 (5.1)
Grade ≥ 4 0 (0.0) Nausea 2 (3.4)
Dose-limiting toxicities 0 (0.0) Blood alkaline phosphatase
2 (3.4)
increase
Serious AEs 0 (0.0) Blood creatine
2 (3.4)
phosphokinase increase
Fatal AEs 0 (0.0)
Anemia 3 (5.1)
AEs leading to
treatment 0 (0.0) Vomiting 2 (3.4)
discontinuation
• Grade 3 treatment-related adverse events: Diarrhea (2/59, 3.4%) and Anemia (1/59, 1.7%)
Presented By John Strickler at 2020 ESMO World GIAdagrasib in mCRC
Hypothesis: Despite activity of KRASG12C inhibition,
reactivation of RAS/MAPK pathway signaling may occur
through adaptive feedback mediated by EGFR
Combining adagrasib with cetuximab, an EGFR inhibitor, may
enhance inhibition of KRASdependent signaling or overcome
adaptive feedback and improve clinical outcomes
Taberno, ESMOGI 2021Summary • HER2 targeted therapies for HER2+ mCRC, while not FDA approved yet, are NCCN guideline listed • mBRAF/EGFR targeting improves PFS and OS compared with chemotherapy plus cetuximab and is FDA approved and NCCN guideline listed. • RAS targeting is finally a reality (at least for KRAS G12C) and other RAS inhibitors are in development as are combinations
You can also read