Predicting Risk of Ovulation in New Start Oral Contraceptive Users
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ORIGINAL RESEARCH
Predicting Risk of Ovulation in New Start Oral
Contraceptive Users
Jill L. Schwartz, MD, Mitchell D. Creinin, MD, Helen C. Pymar, MD, and Lynn Reid, PA-C
OBJECTIVE: To assess ovarian follicular development and for the first pack of pills: day 1 of menses, day 5 of menses
ovulation rates in women starting to take oral contracep- or the Sunday after the start of the menstrual cycle.1 How-
tives (OC) on menstrual cycle day 1, 4, or 7. ever, current package inserts offer a choice between a day 1
METHODS: One hundred thirty women starting treatment start and a Sunday start. Women are advised to use no
with OC were randomized to begin use of ethinyl estradiol, back-up contraception with a day 1 start and back-up for 7
30 g, plus norgestrel, 300 g, on menstrual cycle day 1 days with a Sunday start. Conflicting opinions and advice
(group 1), 4 (group 2), or 7 (group 3). Follicular develop- are potentially confusing to both clinicians and OC users.
ment was assessed by vaginal ultrasonography on men-
Of new users of OC, an estimated 6.9% experience failure
strual cycle days 7, 14, 21, and 28, and serum progesterone
levels were measured on menstrual cycle days 21 and 28. At
and 32% discontinue use for method-related reasons in the
a .05 level of significance (two-tailed) and power of 80%, 84 first year of use.2 Inconsistent instructions might contribute
participants were required to complete the study. Eighty- to poor compliance, as patients may perceive that correct
five women who met study criteria, made minimal dosing and effective pill-taking is complicated. In addition, it is
errors, and underwent at least three ultrasonographic ex- unclear whether women who opt for a Sunday start require
aminations were analyzed. use of a back-up method.
RESULTS: A follicle-like structure that reached a maxi- Although multiple studies have analyzed ovarian ac-
mum diameter over 13 mm was observed in three of 29 tivity and ovulation rates during routine contraceptive
(10.3%), five of 29 (17.2%), and 12 of 27 (44.4%) women in use3,4 and with missed pills,5 OC action in the initial
groups 1, 2 and 3, respectively (P ⴝ 0.003). The median cycle of use is not well characterized. Delaying OC
maximum follicle size for each group was 9.0 mm, 9.0 mm, initiation may place patients at higher risk for pregnancy.
and 12.0 mm for start day 1, 4, and 7 respectively (P < Oral contraceptives started on day 1 and day 6 of the
.001). Evidence of ovulation based on serum progesterone menstrual cycle in female monkeys indicates that selec-
was present in two, one, and zero women in groups 1, 2, and
tion of a dominant follicle can occur with delay of
3, respectively (P ⴝ .2).
initiation to day 6.6 A nonrandomized study indicated
CONCLUSION: Although a delay in oral contraceptive initi- that 1 of 11 (9%) women starting OC on day 1 of the
ation results in significantly more ovarian follicular devel-
menstrual cycle had a follicle larger than 10 mm com-
opment, the postponement does not appear to increase
actual ovulation rates. (Obstet Gynecol 2002;99:177– 82.
pared with 7 of 11 (64%) women starting on day 5 of the
© 2002 by the American College of Obstetricians and menstrual cycle.7 Importantly, in view of patient pill-
Gynecologists.) taking errors, it is unknown if a delayed start can con-
tribute to decreased efficacy and justifies use of a back-up
method.
There is no consensus among practitioners on recommen- We assessed ovarian follicle formation and subsequent
dations for using a back-up contraceptive method when ovulation in women starting OC use on menstrual cycle
oral contraceptives (OC) are initiated. Most recommenda- day 1, 4, or 7. We planned to characterize the way in which
tions on the initial efficacy of the OC formulation use start OCs affect ovulation in the first month of use to develop
day as a determinant. A 1993 analysis of OC package consistent use instructions and improve patient compliance.
inserts from nine manufacturers describes three start days
From the Department of Obstetrics, Gynecology and Reproductive Sciences, Uni- Financial Disclosure
versity of Pittsburgh School of Medicine and Magee Womens Research Institute, This research was supported by a grant from Wyeth-Ayerst Labo-
Pittsburgh, Pennsylvania. ratories. The authors received no salary support to perform this
study. Drs. Schwartz and Creinin have received research support
The authors gratefully acknowledge Leslie A. Meyn, MS, for her statistical and and honoraria from Wyeth-Ayerst Laboratories.
editorial support.
VOL. 99, NO. 2, FEBRUARY 2002 0029-7844/02/$22.00 177
© 2002 by The American College of Obstetricians and Gynecologists. Published by Elsevier Science Inc. PII S0029-7844(01)01676-3MATERIALS AND METHODS formed according to random permuted blocks of nine by
We performed a prospective single-center randomized using a random-number table to assure equal groups.
single-masked study in the Clinical Research Center of The study group was written on a card and sealed in
the Magee-Womens Research Institute between Decem- consecutively numbered envelopes. A person unrelated
ber 1997 and April 2000. The study protocol was ap- to the study performed the randomization sequence and
proved by the institutional review board of Magee- prepared the envelopes. The group was assigned by
Womens Hospital, and informed consent was obtained opening the next sequentially numbered sealed opaque
from all volunteers before entry into the study. envelope.
Women 18 to 38 years of age who wished to initiate Women called the investigators at the onset of their
menses and were reminded when to start taking their
OC use were eligible for enrollment if they had regular
OC. They returned for evaluation within 3 days of
menstrual cycles (every 26 to 30 days), were within 35%
menstrual cycle days 7, 14, 21, and 28. Follicular devel-
of ideal body weight, had both ovaries visible on vaginal
opment was measured by using vaginal ultrasonography
ultrasonography, and were willing to be abstinent or use
(GE RT3200 Advantage II or GE Pro Series; General
a barrier method of contraception during the study. If a
Electric, Milwaukee, WI). All ultrasonographic exami-
participant had a previous pregnancy, she must have had
nations were performed by one of the three physician-
one spontaneous menses and be at least 60 days from the
authors (JLS, MDC, or HCP). Although intersonogra-
end of the pregnancy on the day of study drug adminis-
pher or intrasonographer variation was not measured,
tration. Women were excluded if they had: a history of two of the physicians were present for at least the first 10
or current thrombophlebitis or thromboembolic disor- evaluations by each physician. The physicians were
der; a known or suspected clotting disorder; cerebrovas- blinded with respect to start day and were not allowed to
cular or coronary artery disease; myocardial infarction; review the participant’s chart in its entirety until the
breast cancer; known or suspected estrogen-dependent completion of the study. Blinding was further ensured by
neoplasia; undiagnosed abnormal genital bleeding; cho- providing the physicians with a data sheet to complete on
lestatic jaundice of pregnancy or jaundice with previous each participant that was physically separate from her
OC use; hepatic adenoma or carcinoma; known neuro- chart at the time of the visit. In addition, participants
vascular lesion of the eye or serious visual disturbance; were reminded at each visit, before meeting with the
hypertension at baseline examination; migraine head- physician, not to tell the physician any information about
aches; recent Papanicolaou smear with high-grade squa- start day. Maximum follicular diameter was assessed at
mous intraepithelial lesion; a history of polycystic ovary each visit; each follicle 5 mm or larger was measured in
syndrome; current use of rifampin, ampicillin, tetracy- two perpendicular planes. The larger of these two diam-
cline, griseofulvin, carbamazepine, phenytoin, pheno- eters was used as the maximum follicle size for the
barbitol, hypnotics, or any other drug that may affect observation.
oral contraceptive metabolism; use of an injectable con- Serum progesterone levels were measured on men-
traceptive (ie, depomedroxyprogesterone acetate) within strual cycle days 21 and 28. Evidence of ovulation was
12 months of the initial study visit; use of contraceptive defined as a serum progesterone level greater than 3
implants or OC pills within 60 days of study, current ng/mL. Serum progesterone levels were determined in
breast-feeding; previous oophorectomy; known hyper- duplicate by using a radioimmunoassay (Diagnostic
sensitivity to estrogens or progestins; serious adverse Products Corporation, Los Angeles, CA) with a minimal
experience with previous OC use; malabsorption due to detection level of 0.06 nmol/L. Samples were batched
medical condition or surgery; known or suspected drug and analyzed in a single run. The coefficient of variation
or alcohol abuse; use of drugs mandating in the labeling averaged 2.3% across the entire assay range, with values
simultaneous use of effective contraception; or age 35 of 1.9% at a concentration of 75 nmol/L and 3.0% at 5
years or older and smoking. nmol/L.
At the first of five visits, medical and menstrual histo- All participants were asked to keep daily diaries of pill
ries were obtained, and physical examination and a compliance, bleeding, adverse events, and concomitant
high-sensitivity urine pregnancy test were performed. medications and to return the empty pill pack. Pill-taking
Volunteers were randomly assigned to begin the OC on errors were considered minor if the participant missed
menstrual cycle day 1 (group 1), day 4 (group 2), or day one pill and took it the next day, if she missed placebo
7 (group 3). Each oral contraceptive package contained pills, or if she started the regimen one day late. Major
21 days of ethinyl estradiol (30 g)/norgestrel (300 g) errors included missing more than one consecutive pill
and 7 days of inert pills (Lo/Ovral; Wyeth-Ayerst Lab- or incorrectly taking placebo pills instead of active pills.
oratories, St. Davids, PA). Randomization was per- Sample size estimates were based on published data
178 Schwartz et al Predicting Ovulation OBSTETRICS & GYNECOLOGYTable 1. Enrollment and Exclusion Table 2. Demographic Characteristics
Women enrolled 130 Group 1 Group 2 Group 3
Characteristic (n ⫽ 29) (n ⫽ 29) (n ⫽ 27)
Women excluded before first follow-up visit 35
Menstrual cycle lengths meeting exclusion criteria 12 Age (y) 21.2 ⫾ 2.7 22.3 ⫾ 5.1 20.9 ⫾ 2.2
Pregnancy 1 Weight (lb) 143.3 ⫾ 28.1 143.6 ⫾ 28.9 139.6 ⫾ 28.3
Use of emergency contraception 1 Height (in) 65.2 ⫾ 2.6 64.7 ⫾ 3.2 64.9 ⫾ 2.7
Lost to follow-up 21 Race (n)
Women excluded after first follow-up visit 10 White 23 23 23
Unable to visualize both ovaries at first follow-up 1 Black 4 6 2
visit Asian 2 0 2
Missed two visits 2 Parity (n)
Discontinued for side effects 1 Nulliparous 25 23 21
⬎3 missed pills 3 Parous 2 3 1
Lost to follow-up 3 Previous abortions or 2 3 5
Women in final data analysis 85 miscarriages (n)
Data with the plus/minus sign are means (⫾SD).
suggesting that if women are instructed to improperly
take oral contraceptives in the first 5–17 days of the criteria and underwent at least three ultrasonographic
cycle, break-through ovulation rates are 29%.5 In con- examinations were included in the analysis. Inclusion of
trast, ovulation rates in users of monophasic pills have the available data for the three women who were lost to
been calculated to be as low as 0%.4 Thus, we assumed
follow-up and the three women who missed three or
ovulation rates of 0%, 15%, and 30% in groups 1, 2, and
more pills did not change any outcomes. The women in
3 respectively. Sample size calculations were made by
each group were similar in all demographic characteris-
using the study planning software nQuery Advisor Re-
tics and tended to be in their early twenties, white, and
lease 4.0 (Statistical Solutions; Saugus, MA) and were
nulliparous (Table 2). Pill-taking errors in the 85 partic-
based on a 2 test of equal proportions in three groups.
ipants were minor (Table 3).
At a 0.05 level of significance (two-tailed) and power of
The median maximum follicle size was 9.0 mm,
80%, 84 total participants were required to complete the
study (defined as having at least three ultrasonographic 9.0 mm, and 13.0 mm for start day 1, 4, and 7, respec-
evaluations). We initially estimated that approximately tively (P ⬍ .001). A follicle-like structure that reached a
10% of women would not complete the study and calcu- maximum diameter larger than 13 mm was observed in
lated an enrollment of 91 women. However, because of three of 29 (10.3%), five of 29 (17.2%), and 12 of 27
the higher than expected attrition rate, we amended the (44.4%) women in groups 1, 2, and 3, respectively (P ⫽
protocol to increase the total number of women enrolled .003). When we compared the medians of the groups for
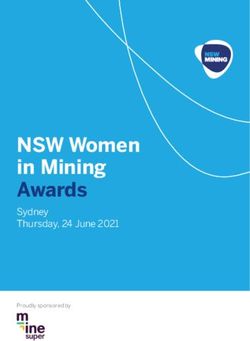
to 130. follicle measurements on day 7, 14, 21, and 28, we
The primary outcome measures were maximum folli- observed a significant difference in increasing follicle size
cle-like structures and ovulation. The groups were com- on day 7 (6.5 mm, 7.0 mm, and 11.0 mm) and day 14
pared according to median maximum follicle diameter (6.0 mm, 6.0 mm, and 9.0 mm) of the cycle in groups 1,
and percentages of maximum follicle diameters larger 2, and 3, respectively. Although the comparison among
than 13 mm; these cut-off values were selected because the three groups on day 28 was statistically significant,
follicle size must generally exceed 13 mm before ovula- this difference is likely to not be clinically significant
tion can occur.8 Ovulation rates and the grouped per- because most of the follicles were smaller than 10 mm
centages of maximum follicle size larger than 13 mm (Figure 1).
were compared by using a 2 test for linear trend.
Median follicle size was compared among groups by
using the Kruskal–Wallis test, since the follicle sizes on Table 3. Pill-Taking and Follow-up Errors in the 85 Ana-
days 7, 14, 21, and 28 were not normally distributed. All lyzed participants
statistical analyses were performed by using SPSS statis- Group 1 Group 2 Group 3
tical software, release 10.0 (Chicago, IL). (n ⫽ 29), (n ⫽ 29), (n ⫽ 27),
n (%) n (%) n (%)
Missed one pill and doubled 3 (10) 2 (7) 5 (18)
RESULTS up the next day
One hundred thirty healthy women participated in the Started regimen 1 day late 0 1 (3) 2 (7)
study (Table 1). Eighty-five women who met study Missed one visit 3 (10) 2 (7) 1 (4)
VOL. 99, NO. 2, FEBRUARY 2002 Schwartz et al Predicting Ovulation 179Figure 1. Distribution of maximum follicle diameters in group 1 (day 1 start), group 2 (day 4 start), and group 3 (day 7 start)
on day 7, 14, 21, and 28 of cycle. Threshold value for follicle diameter was 13 mm. E ⫽ day 1 start; ⫹ ⫽ day 4 start; { ⫽
day 7 start.
Schwartz. Predicting Ovulation. Obstet Gynecol 2002.
Since more subjects from group 3 made minor pill- (one on day 7, one on day 14, and one on day 21)
taking errors (Table 3), we reanalyzed the data without developed follicles larger than 13 mm. In comparison, 10
the 13 participants who started the regimen 1 day late or of the 17 (58.8%) women in groups 2 and 3 who devel-
missed pills. The median maximum follicle size was oped follicles of this size had done so by day 7.
9.0 mm, 9.0 mm, and 12.0 mm for start days 1, 4, and 7, All 85 participants had at least one progesterone level
respectively (P ⫽ .001). In addition, a follicle-like struc- measured. Five values were missing: one day 21 and one
ture that reached a maximum diameter larger than day 28 level for one woman each in groups 1 and 3, and
13 mm was observed in three of 26 (11.5%), four of 26 one day 21 value in group 2. Two, one, and zero women
(15.4%), and 7 of 20 (35.0%) women in groups 1, 2 and in groups 1, 2, and 3, respectively, had evidence of
3, respectively (P ⫽ .055). Although these groups are ovulation on the basis of serum progesterone level (P ⫽
small, the lack of statistical significance at a P value of .2) These three participants had follicle-like structures
.055 suggests that even without the minor pill-taking larger than 13 mm and had diary cards and empty pill
errors (which were more common in group 3) the differ- packs that indicated correct OC use. Of the two women
ence in follicular development is still significant.
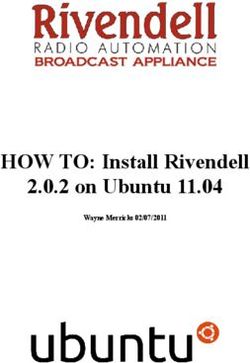
in group 1 who ovulated, one had follicle-like structures
Of the 20 women who developed follicle-like struc-
larger than 13 mm by day 14 and one had such struc-
tures larger than 13 mm, those in group 2 or group 3
tures day 21 (Figure 2). In both women, the follicle-like
were not more likely than those in group 1 to have
structure continued to grow from day 14 to day 21 and
developed a follicle of this size earlier (P ⫽ .7). Similarly,
if women who started OC use on day 1 were compared decreased slightly in size by day 28. Progesterone levels
to a combined population of groups 2 and 3 (all women in both of these women were less than 3 ng/mL on day
who started the pill after day 1), there was still no 21 and greater than 3 ng/mL on day 28. The woman in
difference in how early a follicle-like structure larger than group 2 who ovulated had a follicle-like structure of
13 mm developed. The lack of a statistical difference is 28 mm diameter on day 14 followed by a progesterone
most likely because relatively few women in group 1 level greater than 3 ng/mL on day 21.
180 Schwartz et al Predicting Ovulation OBSTETRICS & GYNECOLOGYFigure 2. Maximum follicular diameters in three women with evidence of ovulation. Threshold value for evidence of ovulation was a progestrone level of 3 ng/mL. E ⫽ subject 1 (group 1); ‚ ⫽ subject 2 (group 1); 䊐 ⫽ subject 3 (group 2). Schwartz. Predicting Ovulation. Obstet Gynecol 2002. DISCUSSION new start may create a dominant follicle capable of Despite high efficacy, OCs do not completely inhibit ovulation. ovarian follicle development.9,10 In theory, delaying ini- In our study, ovarian follicles appeared to be quiescent tiation of the first OC tablet from day 1 to day 7 may by day 21, even with a day 7 start. Therefore, given that place patients at higher risk for pregnancy. We per- pill-taking errors occur, it would be sufficient to use a formed this study because clinicians have made recom- back-up method for 2 weeks. However, two out of the mendations to use back-up methods in the first month of three women with characteristics indicating ovulation OC use based on speculation that women may be more started OCs on day 1 of their menstrual cycle and vulnerable to contraceptive failure in the first cycle of demonstrated maximum follicle size at day 21 (Figure 2). use. Ovarian activity in the first cycle of use may be more Therefore, in this scenario, use of a back-up method for concerning than in future cycles, and OC failure may be 2–3 weeks may offer women a contraceptive advantage. closely linked to delaying start of OC use. Alternatively, despite the difference in ovarian activity, We hypothesized that ovulation and possible preg- there was no significant difference in ovulation; thus, use nancy can occur more readily when there is previous of a back-up method could be argued to confer no added follicular recruitment and residual ovarian activity, as contraceptive benefit to one group over another. with new starters of OCs. Increasing the pill-free interval Although this study indicates that there is significantly from 7 to 11 days in women taking OCs has been shown more ovarian follicle formation in women who delay the to allow more follicular development and estradiol pro- start of OC use until day 7, it did not prove that ovula- duction without leading to method failure.11 In addition, tion is increased in these women. Unexpectedly, two missing pills in specific sequences of four consecutive (6.9%) women with a day 1 start and one (3.6%) with a pills does not lead to ovarian follicle formation and day 4 start had progesterone levels consistent with ovu- ovulation.12 However, delaying the initiation of the first lation. Chowdhury et al5 demonstrated that women who OC package up to 7 days differs from extending the miss up to two consecutive days in any part of the pill pill-free interval and missing pill sequences. In the former cycle may have an escape ovulation compared with case, there is residual ovarian activity because follicular perfectly compliant users, whereas the cervical mucus recruitment begins in the previous cycle, and delaying a remained thick and unfavorable to sperm in all partici- VOL. 99, NO. 2, FEBRUARY 2002 Schwartz et al Predicting Ovulation 181
pants. With this in mind, other mechanisms of OC three low-dose oral contraceptives: A randomized con-
action ensure that ovulation alone does not lead to trolled trial. Obstet Gynecol 1994;83:29 –34.
pregnancy in a compliant pill taker. However, these 5. Chowdhury V, Joshi UM, Gopalkrishna K, Betrabet S,
findings suggest that women who use OC imperfectly Mehta S, Saxena BN. Escape ovulation in women due to
the missing of low dose combination oral contraceptive
and also delay the start of OC may have decreased
pills. Contraception 1980;22:241–7.
efficacy. Although no studies have evaluated compliance
6. Danforth DR, Hodgen GD. “Sunday start” multiphasic
in the first cycle of OC use, studies using electronic pill
oral contraception: ovulation prevention and delayed fol-
dispensers have shown that two to three times more pills licular atresia in primates. Contraception 1989;39:321–30.
were forgotten than women reported.13 Of the 85 7. Killick S, Eyong E, Elstein M. Ovarian follicular develop-
women in our study, 12% of women reported missing ment in oral contraceptive cycles. Fertil Steril 1987;48:
one pill and 3% of women reported starting their pills 409 –13.
one day later than they were told (Table 3). 8. Hoogland HJ, Skouby SO. Ultrasound evaluation of ovar-
We found no difference in the incidence of ovulation ian activity under oral contraceptives. Contraception
when OC start was delayed to day 7. This finding does 1993;47:583–90.
not support recommending use of a back-up method in 9. Callouette JC, Koehler AL. Phasic contraceptive pills and
the first cycle of OC use for women who start on day 1 functional ovarian cysts. Am J Obstet Gynecol 1987;156:
through day 7. However, this study may not have 1538 – 40.
enough power to detect a small difference; we would 10. Egarter C, Putz M, Strohmer H, Speiser P, Wenzl R,
Huber J. Ovarian function during low-dose oral contracep-
recommend a larger study before changing clinical prac-
tive use. Contraception 1995;51:329 –33.
tice. We believe that our findings justify a prospective
11. Killick SR, Bancroft K, Oelbaum S, Morris J, Elstein M.
randomized study to evaluate first cycle pregnancy rates Extending the duration of the pill-free interval during
in women starting OCs on days 1, 4, and 7. combined oral contraception. Adv Contracept 1990;6:
33– 40.
12. Letterie GS, Chow GE. Effect of “missed pills” on oral
REFERENCES contraceptive effectiveness. Obstet Gynecol 1992;79:
1. Williams-Deane L, Potter LS. Current oral contraceptive 979 – 82.
use instructions: An analysis of patient package inserts. 13. Potter L, Oakley D, de Leon-Wong E, Canamar R. Mea-
Fam Plann Perspect 1992;24:111–5. suring compliance among oral contraceptive users. Fam
2. Trussell J, Vaughan B. Contraceptive failure, method- Plann Perspect 1996;28:154 – 8.
related discontinuation and resumption of use: results
from the 1995 National Survey of Family Growth. Fam Address reprint requests to: Mitchell D. Creinin, MD, Univer-
Plann Perspect 1999;31:64 –72, 93. sity of Pittsburgh School of Medicine, Department of Obstet-
3. Crosignani PG, Testa G, Vegetti W, Parazzini F. Ovarian rics, Gynecology and Reproductive Sciences, Magee-Womens
activity during regular oral contraceptive use. Contracep- Hospital, 300 Halket Street, Pittsburgh, PA 15213-3180. E-
tion 1996;54:271–3. mail: mcreinin@mail.magee.edu.
4. Grimes DA, Godwin AJ, Rubin A, Smith JA, Lacarra M. Received June 19, 2001. Received in revised form September 13, 2001.
Ovulation and follicular development associated with Accepted October 2, 2001.
182 Schwartz et al Predicting Ovulation OBSTETRICS & GYNECOLOGYYou can also read