Contraception Update Maryam Nasri MRCGP MFSRH SRH Consultant 30.4.2021 - SP Corporate Services
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Contraception Update
Maryam Nasri MRCGP MFSRH
SRH Consultant 30.4.2021
Maryam Nasri 30.04.21
Agenda • Non LARC Contraception Update • LARC update Maryam Nasri 30.04.21
COVID 19 impact • Change in protocols –see FSRH COVID updates • Change in service delivery • Change in attitudes • SHL , SH24 , online provision , pharmacy provision Maryam Nasri 30.04.21
FSRH website Maryam Nasri 30.04.21
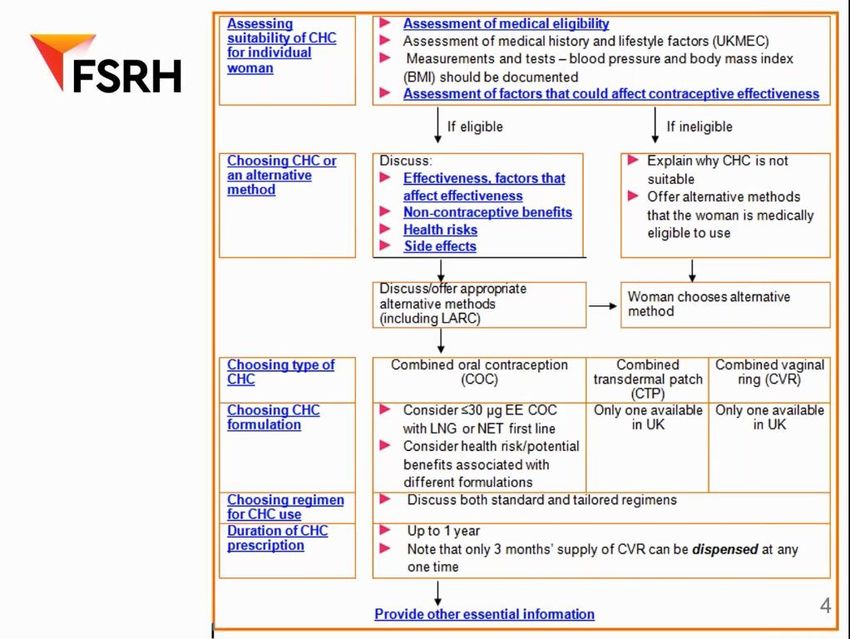
Combined Hormonal
Contraception
Maryam Nasri 30.04.21Maryam Nasri 30.04.21
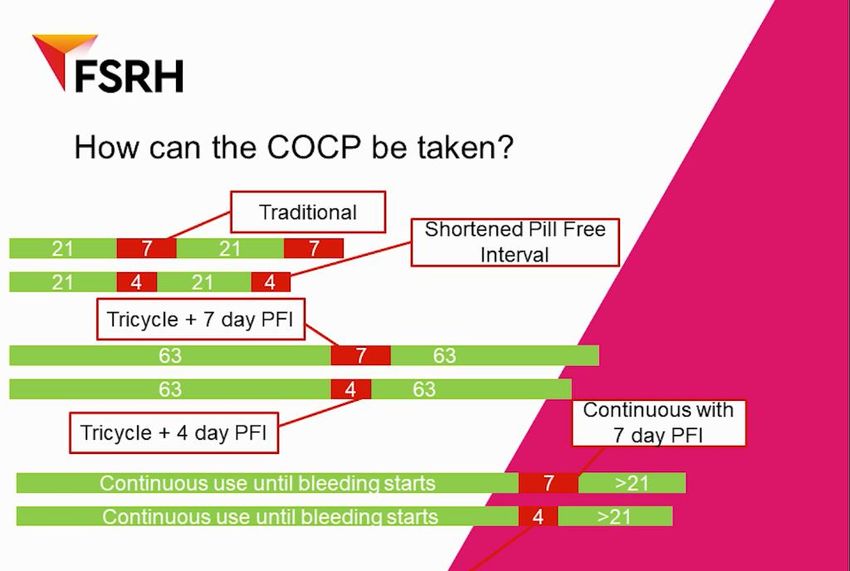
Tailored regiments: key messages
• CHC is as safe and at least as effective for contraception if taken as an extended or continuous course
• A woman using CHC does not need a monthly withdrawal bleed to be healthy
• There is no build up of menstrual blood inside a woman who uses CHC without a break; extended CHC use
keeps the lining of the womb thin
• A monthly bleed on CHC is not a reassurance that the woman is not pregnant
• By using extended or continuous courses the frequency of withdrawal bleeds and symptoms can be reduced
• Ovaries can be activated during the traditional 7 day hormone free interval therefore fewer or shorter breaks
could mean less risk of pregnancy
• Irregular bleeding or spotting can occur in the first few months of a CHC particularly with extended or
continuous courses but it generally improves with time and doesn't mean there is a problem
• Extended or continuous cause does not affect the return of a woman's fertility when she stops CHC
Maryam Nasri 30.04.21Tailored Regimens
type of regimen period of CHC used Hormone free interval
standard use 21 days 7 days
tailored use
shortened hormone free interval 21 days 4
extended use tricycling 9 weeks 4-7 days
flexible extended use continuous use of active pills patches or 4 - 7 days
Rings until breakthrough bleeding
occurs for 3-4 days
continuous use continuous use of active pill patches or none
rings
Maryam Nasri 30.04.21Maryam Nasri 30.04.21
Maryam Nasri 30.04.21
How long can I give a prescription for CHC
• COC:provision of up to a 1 year supply of COC may be appropriate
• COC:it may be appropriate to provide a more limited supply ;3 months for women who
would benefit from returning for a follow-up visit
• CTP :once a woman is established on it ,can be given one year supply /prescription
• CVR :Nuvaring has to be kept refrigerated. After dispensing, it can be stored at room
temperature but has to be used within 4 months maximum. Therefore no more than 1
pack of 3 Nuvaring can be provided at any one time but provide repeat prescription to
prevent users having to return to the provider more than once a year.Syreniring however
can be prescribed for one year .
Follow-up is required annually
Maryam Nasri 30.04.21FSRH CEU Statement : New advice from the MHRA
regarding cyproterone acetate: July 2020
• How does this affect prescribing of Cocyprindiol/Dianette® for
acne/hirsutism?
• New data from a French cohort study indicate that use of high dose cyproterone acetate
(high dose products contain 50-100mg per tablet) is associated with significantly increased
risk of meningioma.
• A cumulative dose of 12-36g was associated with an estimated 6-fold greater risk (annual
incidence 26 per 100,000 users) than a cumulative dose of less than 3g (annual incidence 4.5
per 100,000).
• For reference, the MHRA estimates annual incidence of meningioma in the general
population to be about 6 per 100,000.
Maryam Nasri 30.04.21• Diannette pills contain only 2mg of cyproterone acetate; annual cumulative
exposure to cyproterone acetate is only about 0.8g.
• The Yellow Card scheme has received no reports of meningioma associated
with use of these low-dose products.
• The MHRA advises that although exposure to this low dose of cyproterone
acetate has not been shown to increase risk of meningioma, an association is
plausible and cannot be excluded.
Maryam Nasri 30.04.21FSRH statement
• Cyproterone acetate should not be used by individuals with a history of
meningioma.
• Individuals that have not had meningioma may consider use of cyproterone
acetate 2mg with ethinylestradiol for acne/hirsutism.
• They should be made aware that increased risk of meningioma associated
with cumulative exposure to low dose cyproterone acetate cannot be
excluded, but risk is likely to remain very low.
Maryam Nasri 30.04.21FSRH Clinical Effectiveness Unit Statement: Use of
combined hormonal contraception during the Covid-19
pandemic - Dec 2020
• Why guidance: Concerns regarding use of CHC in patients with COVID 19
who are already at increased risk of VTE
• What we know :However in general, CHC use is associated with increased
risk of thromboembolism and is usually avoided in the presence of
additional risk factors.
• What we do not know :There is no published evidence to directly inform risk
of thromboembolism associated with use of CHC during Covid-19
infection.
Maryam Nasri 30.04.21Why not stop CHC in everyone with COVID
19?
• 1.It is the most widely used contraception
• 2.Risk of unplanned pregnancy
• 3.Suggested that that estrogens - both endogenous and exogenous - could
potentially be protective against the immune inflammatory response
associated with the most serious complications of Covid-19.
Maryam Nasri 30.04.21Healthy individuals • Do not stop routinely during pandemic • Offer all other methods • Counsel regarding risk of VTE Maryam Nasri 30.04.21
Current CHC users with asymptomatic Covid-
19 infection
• Can continue to use CHC.
• Some may wish to make an immediate switch to a progestogen-only pill to
try to reduce thrombotic risk,
Maryam Nasri 30.04.21Individuals with symptomatic Covid-19
infection not requiring hospitalisation
• should be managed according to severity of illness and degree of immobility.
• Discontinuation of CHC and initiation of a progestogen-only pill (POP) should be
considered.
• Where appropriate, emergency contraception should be discussed.
• After recovery, the individual may wish to continue POP or to consider an alternative
contraceptive method that is not associated with increased risk of thromboembolism.
• Restarting CHC may be considered when the individual is no longer systemically unwell and
has regained full mobility
• it is not known how long elevated thromboembolic risk associated with Covid-19 infection
persists.
Maryam Nasri 30.04.21Current CHC users requiring hospital admission because of severe Covid-19 infection • should discontinue CHC. • Where appropriate, emergency contraception should be discussed. • An alternative effective contraceptive method such as a POP should, where appropriate, be initiated prior to discharge from hospital. • After recovery, the individual may wish to continue POP or to consider an alternative contraceptive method that is not associated with increased risk of thromboembolism. • Restarting CHC may be considered when the individual is no longer systemically unwell and has regained full mobility • it is not known how long elevated thromboembolic risk associated with Covid-19 infection persists. Maryam Nasri 30.04.21
Antibiotics and CHC
• Aronson and Ferner, 2020 “Analysis of reports of unintended pregnancies
associated with the combined use of non-enzyme inducing antibiotics and
hormonal contraceptives”
• Medscape drug interaction calculator
• Liverpool drug interaction
• FSRH drug interaction guidance
Maryam Nasri 30.04.21CEU response 2.2.21
• No change in current guidance
• Substantial limitations, the findings are not scientifically robust enough to warrant
any change to FSRH CEU guidance.
• FSRH CEU guidance remains that additional contraceptive precautions are not
required when antibiotics are prescribed to users of hormonal contraception.
• In women using known enzyme-inducing medications long-term, including enzyme
inducing antibiotics, the FSRH CEU recommends intrauterine contraception (IUC)
or injectable contraception (DMPA)
Maryam Nasri 30.04.21Maryam Nasri 30.04.21
Progesterone only
contraception
Maryam Nasri 30.04.21Types of POPs in UK
POPs currently available in the UK contain
• NET 350 µg (Micronor®, Noriday®),
• LNG 30 µg (Norgeston®)
• DSG 75 µg (Cerazette® ,Cerrelle, Zeletta and other branded generic
products).
Maryam Nasri 30.04.21DSG containing pills DSG pills may have potential benefits over traditional POPs • Ovulation is inhibited in up to 97% of cycles • 12-hour window for missed pills. • Management of dysmenorrhoea • Bleeding patterns (50% Vs 10%) Maryam Nasri 30.04.21
POP and weight
• No increased risk of pregnancy in POP users with a heavier body weight or a
higher body mass index.
• Insufficient evidence to support a dose of more than one pill per day for
women who are heavy or overweight.
• No causal association between POP use and weight change.
• Use one pill per day, even in women with a BMI >30 kg/m2.
Maryam Nasri 30.04.21“Use of effective contraception following provision of the progestogen-only pill for
women presenting to community pharmacies for emergency contraception (Bridge-It):
a pragmatic cluster-randomised crossover trial.” Cameron, et al
November 2020
• Participating pharmacy clusters in Scotland and London;In the UK, most oral EC is
provided in pharmacies
• In the control phase, individuals receiving LNG-EC were advised to attend their
usual contraceptive provider for ongoing contraception.
• In the intervention phase individuals received LNG-EC plus a three-month
desogestrel 75mcg POP and a card allowing them priority access to their local SRH
service.
• Followed up by phone or online ;and they self-reported their use of effective
contraception.
Maryam Nasri 12.3.21• At four months, subjects in the intervention group were 20% more likely to be using effective contraception than those in the control group, and significantly less likely to have required further emergency contraception (EC). • Provision of the rapid-access card did not increase the likelihood of subjects attending their local SRH service—most chose to access ongoing contraception via their GP. • The contraceptive method most commonly used at four months was POP in the intervention group and combined oral contraception in the control group. The uptake of LARC was similar and low in both groups. • Maryam Nasri 12.3.21
What does this mean for practice?
• The Bridge-It study indicates that provision of a 3-month bridging supply of
a desogestrel POP by a pharmacist when an individual presents to the
pharmacy requesting oral EC could increase their future use of effective
contraception.
Maryam Nasri 12.3.21FSRH consultation response: FSRH fully supports
reclassification of the progestogen-only pill as a Pharmacy
medicine
• MHRA is consulting on reclassifying two brands of the desogestrel pill into
pharmacy provided medicine
• Sexual and reproductive healthcare is an essential part of healthcare ; barriers to
access must be reduced to reduce unplanned pregnancy rates.
• POPs are safe, reliable, easy to use and a very popular contraceptive
• Relieve unnecessary pressures on GPs, reduce repeat prescriptions.
• The 75mcg desogestrel POP can be taken from menarche to menopause and has
very low risk of serious adverse events and there are few medical contraindications.
Maryam Nasri 30.04.21DMPA
• Depot medroxyprogesterone acetate (DMPA) use may reduce pain associated with endometriosis.
• DMPA is a contraceptive option for women with sickle cell disease and may reduce the severity of sickle
crisis pain.
• The efficacy of DMPA contraception is not reduced with concurrent use of enzyme inducing drugs.
• The progestogen-only injectable is listed within National Institute for Health and Care Excellence (NICE)
guidelines as a possible treatment for the management of heavy menstrual bleeding
• DMPA is often prescribed in women with learning disabilities
Maryam Nasri 30.04.21DMPA and weight gain
• Higher initial BMI is predictive of weight gain with DMPA use in adolescents (aged under 18
years )
• The association between weight gain and higher BMI at initiation of DMPA has not been
observed in adult women.
• The available evidence suggests that women who experience an increase of more than 5% of
their starting weight within the first 6 months of use are likely to continue to experience weight
gain.
Maryam Nasri 30.04.21DMPA continued
• After 45 DMPA moves from category 1 of UK MEC to category 2
• Review every 2 years
• If any additional risk factors :smoking ,inactivity ,family history ,vitamin D deficiency advise
to consider alternative methods
• Do not offer routine bone density scan or monitoring of serum lipids or use of oestrogen
• Women over 50 should be counselled on alternative methods if they do not wish to stop
then consideration should be given to continuation providing the benefits and risks are
understood
Maryam Nasri 30.04.21Sayana Press
An additional choice for women
• Side effects
• Efficacy
• Safety
• Price
• Licensed for self administration
• www.medisa.com
• www.sayanaanswers.co.uk
• Advice re competent adult at home when first self
injecting
Maryam Nasri 30.04.21Missed pill rules Maryam Nasri 30.04.21
• EC is required/not required.
• She can take the missed pill as soon as possible and continue taking the
remaining pills at the usual time.
• She needs/does not need additional contraceptive precaution.
• She needs a pregnancy test
Maryam Nasri 30.04.21Maryam Nasri 30.04.21
Maryam Nasri 30.04.21
Maryam Nasri 30.04.21
Missed pill case
• Kathy has called for her repeat pill prescription. You realize that Kathy had actually ran out of her
medication. She had had to self isolate and could not pick up any scripts. Her new pill was due 3 days ago.
• She has had sex 3 days ago and says she thought she was protected.
• How would you manage Kathy?
• Would you do pregnancy test?
• Would you ask her to stop her pills?
• Would you offer her EC/PCIUCD
• Would you tell her to do a pregnancy test ?
• Does she need to use condoms ?
Maryam Nasri 30.04.21What is the current guidance?
EC should be considered:
• if the pill-free interval is extended,
• or if 2-7 pills are missed in the first week following a pill-free interval,
• or if more than 7 pills are missed in any week of scheduled pill-taking (this
situation is considered a new start rather than restart of COC)
•
Maryam Nasri 30.04.21EC is generally not advised
• if 1 pill is missed at any time during scheduled pill taking
• or if 2-7 pills are missed in week 2 or week 3 after the pill-free interval (or
subsequent consecutive weeks of continuous pill-taking).
if any progestogen (including progestogen in CHC) has been taken in the 7
days prior to EC, LNG-EC should be considered, with immediate quick start
of suitable effective contraception. If UPA-EC is used in this situation, use of
hormonal contraception should be delayed for 5 days after UPA-EC.
Maryam Nasri 30.04.21• Hannah is 23 year old. She has used COC for many years. She had resumed
her pills after her PFI and had taken 4 of them. She had not had any sex
during her PFI. But then forgot to take her pill for two days and had sex on
the second day.
• She attends on the third day, less than 72 hours from her UPSI.
• Would you give her EC?
• Which EC would you give her?
Maryam Nasri 30.04.21• She went to the pharmacy and was given Ella One on the 3rd day of missed
pills and advised to continue with her COC.
Maryam Nasri 30.04.21• UPA-EC works by delaying ovulation until sperm from previous unprotected
sex are no longer viable (5 days after sex).
• we know that individuals who take UPA-EC when they are close to ovulation
in a natural menstrual cycle are significantly more likely to ovulate in the
following 5 days if they start a COC or progestogen-only pill immediately
after UPA-EC.
• Delayed start of hormonal contraception is therefore recommended in this
situation.
Maryam Nasri 30.04.21Banh Study
“The effects on ovarian activity of delaying versus immediately restarting
combined oral contraception after missing three pills and taking ulipristal
acetate 30mg”Nov 2020
• This new study by Banh, et al. considers a different scenario, in which UPA-
EC users are already established on COC. The findings can only be applied
to that scenario.
Maryam Nasri 30.04.21Change in guidance only relates to one specific
situation
• Specific situation
• 1. Established CHC user
• 2.Restarts CHC after a hormone-free interval
• 3. Then misses 2-7 pills in the first week of pill taking (or makes an equivalent error with
combined patch or ring use):
• LNG-EC may be offered, with immediate restart of CHC and use of condoms for 7 days (no
change to guidance) if UPA-EC is preferred, it may be offered, now with immediate restart of
CHC and use of condoms for 7 days (new recommendation for this specific scenario only)
• Unless an individual taking UPA-EC is an established CHC user in the specific situation
described above, hormonal contraception should not be started for 5 days after UPA-EC
Maryam Nasri 30.04.21When is contraception no longer needed ?
• At 50 :DMPA and CHC –switch to other methods
• At 55 all methods are stopped
• IUD s should be removed and can not stay indefinitely
• IUCDs inserted after 40 can remain till 55
• IUS inserted after 45 can remain in situ till 55 unless for HRT or woman’s
pattern of bleeding changes
Maryam Nasri 30.04.21References
• https://www.oconmed.com/fileadmin/user_upload/Ocon-IUB-Doctors-Overview-DO_EN_090215_2.pdf
• https://www.fsrh.org/standards-and-guidance/current-clinical-guidance/quick-starting-contraception/
• https://www.fsrh.org/standards-and-guidance/documents/fsrh-guidance-contraception-for-women-aged-
over-40-years-2017/https://www.fsrh.org/news/the-fsrh-ceu-statement-regarding-delaying-versus-
immediately/
• https://www.fsrh.org/documents/fsrh-ceu-recommendation-on-extended-use-of-the-etonogestrel/
• https://www.fsrh.org/news/fsrh-new-guidance-service-provision-covid-second-wave/
• https://www.fsrh.org/documents/fsrh-rcog-rcm-statement-postpartum-contraception-
covid19/https://www.fsrh.org/documents/fsrh-clinical-effectiveness-unit-statement-use-of-combined/
Maryam Nasri 30.04.21LARC Maryam Nasri 30.04.21
Maryam Nasri 30.04.21
Extended use of LARC during the pandemic
• IUCDs (10 years ) extended to 12 years
• Contraceptive effectiveness cannot be guaranteed with extended use of 52
mg IUS :Individuals may wish to use condoms in addition, or to add in a
progestogen-only contraceptive pill (POP).
• After 4 completed years of use of the ENG-IMP and 6 completed years of
use of the 52mg LNG-IUS, all women should be advised to use condoms in
addition or to add a POP
Maryam Nasri 30.04.21• Jaydess, Kyleena and 5 year IUCDs not extended
• Levosert :extended license to 6 years for contraception –for HMB still 5
years and remains unlicensed for Endometrial protection
Maryam Nasri 30.04.21New IUS Kyleena Levosert Maryam Nasri 30.04.21
Comparison of the different IUS
Type of LNG-IUS
Total LNG content-mg
Kyleena
19.5
Mirena
52
Levosert
52
Jaydess
13.5
Frame size W x Hmm 28 x 3 32x32 32 x 32 28 x 30
Inserter one-handed EvoInserter one-handed EvoInserter Two handed inserter One handed EvoInserter
Insertion tube diameter -mm 3.8 4.4 4.8 3.8
Licence duration of use for 5 5 6 3
contraception in years
Licence for endometrial no yes no no
protection
Licence for heavy menstrual no yes-5 years yes-5 years no
bleeding
Minimum uterine cavity not indicated in SPC not indicated in SPC 5.5 cm not indicated in SPC
length in cm
unit cost per £ 76 88 66 69.22
cost per year over period of 15.2 17.6 16.5 23.07
licenced use
Maryam Nasri 30.04.21IUS vs IUCD for EC
• Turok DK, Gero A, Simmons RG, Kaiser JE, Stoddard GJ, Sexsmith CD,
Gawron LM, Sanders JN. Levonorgestrel vs. Copper Intrauterine Devices for
Emergency Contraception. New England Journal of Medicine
2021;384(4):335-44.
Maryam Nasri 30.04.21What we know
• In USA (but not the UK) IUS can be quick started with LNG EC.
• A previous study by Turok et al indicated user preference for the LNG-IUS
over the Cu-IUD in this situation and reported no pregnancies amongst 121
individuals requiring EC who took LNG-EC and also quick started a 52mg
LNG-IUS.
• levonorgestrel can directly interfere with sperm transport, sperm
capacitation, the acrosome reaction, and oviduct transport
Maryam Nasri 30.04.21Postulation
• The authors of the current study postulate that the LNG-IUS would be
effective for emergency contraception
• Randomised USA trial on 711 women who requested EC in two arms
• either a T380A Cu-IUD or a Liletta® 52mg LNG-IUS
• IUS group : One pregnancy was recorded, in an individual who had reported
one episode of UPSI 48 hours prior to insertion of the LNG-IUS.
• IUCD group :no pregnancies were recorded
Maryam Nasri 30.04.21How does this affect practice?
• The FSRH CEU recommends no change to current practice at this time.
• The study had limitations including selection bias and different baseline risk
of pregnancy
• ??the 52mg LNG-IUS could be an effective method of emergency
contraception
• ??quick start of the LNG-IUS with LNG-EC or in situations in which a
pregnancy test is negative but there has been UPSI in the last 21 days
Maryam Nasri 30.04.21No ideal contraception yet!! Maryam Nasri 30.04.21
Maryam Nasri 30.04.21
Maryam Nasri 30.04.21
Progesterone implant • 0.0 5% failure rate • no age restriction to its use :menarche –menopause • Licenced for 3 years Maryam Nasri 30.04.21
Effectiveness • In 4th year –no routine • BMI • EID • UPA (daily) ,Ella one as EC Maryam Nasri 30.04.21
UKMEC 3 and 4 • Breast cancer • Arterial thromboembolic events • Undiagnosed vaginal bleeding • Decompensated Cirrhosis • Hepatocellular carcinoma Maryam Nasri 30.04.21
Counselling • Local migration • Distant intravascular migration • Feel the SDI in situ • Local reaction/nerve damage/IM insertion • Hormonal side effects Maryam Nasri 30.04.21
Hormonal side effects –Bleeding • Cause is not clear • The number of days is less than a normal period or on COC • Evidence for management :CHC and Mefenamic acid • So counsel! • 50% better Maryam Nasri 30.04.21
Maryam Nasri 30.04.21
Other side effects • Acne :new onset/existing • Weight gain • Depression Maryam Nasri 30.04.21
Noncontraceptive benefits • Reduction in dysmenorrhoea • Reduction in endometriosis related pain • HMB? • In women with PCO no induction of WDB needed Maryam Nasri 30.04.21
Extended use • Extended use started in the pandemic • There is some evidence • Not advised routinely • EC probably not needed • Methods can be quick started in the 4 th year Maryam Nasri 30.04.21
Maryam Nasri 30.04.21
When can it be given ?
• Day 1-5 of natural menstrual cycle
• Immediately after delivery up to 21 days without any additional
contraception
• Up to day 5 after TOP without additional contraception even at the time of
mifepristone administration
• After EC :
Maryam Nasri 30.04.21Insertion
• Contraceptive implant was introduced in UK in 1999-Implanon ,
• In 2010 :Nexplanon was introduced :new inserter did not prevent deep
insertions
• Since introduction in 1998 up to 2019 :107 implants have migrated
worldwide into the chest
• Can migrate , can cause neurovascular damage , can be difficult to remove
Maryam Nasri 30.04.21Position over New position
January 2020
biceps
Maryam Nasri 30.04.21• FSRH guidance to insert on Biceps
• NORA study published in March 2018 :Nexplanon Observational Risk
Assessment Study in USA 2011-2017 on 7364 women
• Deep implants incidence 8.8/1000 insertions
• Observational study in 100 women :if performed correctly , it usually
migrates less than 2 cm .
Maryam Nasri 30.04.21Neurovascular anatomy of the adult female medial arm in relationship to
potential sites for insertion of the etonogestrel contraceptive implant
Contraception Journal
• Objective :Anatomic assessment of the medial upper arm to identify potential sites
for insertion of the etonogestrel (ENG) implant.
• Forty female cadaveric arms were dissected.
• Two rows of 1×2-cm dissection windows were created in the inner arm overlying
the triceps approximately 2-3 and 4-5 cm posterior to the bicipital sulcus (sulcus).
• The primary window was 8-10 cm proximal to the medial epicondyle and
approximately 2-3 cm posterior to the sulcus.
• Neurovascular structures within each window were identified.
• The entire medial upper arm was dissected to visualize underlying structures.
Maryam Nasri 30.04.21Maryam Nasri 30.04.21
Maryam Nasri 30.04.21
• Conclusion:
• As no major neurovascular structures were identified overlying the triceps 8-
10 cm proximal to the medial epicondyle and 3-5 cm posterior to the sulcus,
ENG implant insertion at this location may minimize risk of injury
associated with improper deep insertion.
• Elbow flexion deflects the ulnar nerve away from this area and may further
decrease risk of injury secondary to inadvertent deep insertion.
Maryam Nasri 30.04.21Maryam Nasri 30.04.21
Maryam Nasri 30.04.21
Recommendations /new site CEU reviewed manufacturer’s recommendations and MHRA’s approval • Only by trained professional • Exchanges: New position • New patients :New position • Unexpired :No need to remove and replace until expired • In nondominant arm-no need to change arm after few insertions • A URL hosting videos demonstrating the insertion and removal of Nexplanon is available at www.nexplanonvideos.eu. Maryam Nasri 30.04.21
New Site
Nondominant arm
elbow flexed and
hand behind head
Start at medical epicondyle
Measure 8-10 cm proximally along sulcus-avoid
sulcus
Then measure 3-5 cm posteriorly
Insert with 30 degree angle
Maryam Nasri 30.04.21Insertion and removal • Inject at point of insertion vs along the track • Lidocaine(max 2-3 mls of 1%) +/- adrenaline • Ethyl chloride spray use • Palpate and document • No need to abstain prior to removal Maryam Nasri 30.04.21
Anticoagulated individuals and those with
bleeding disorders
• I and R are minor procedures
• LMWH, DOAC, Warfarin,atiplatelets drugs should generally not be stopped
if standardized INR and stable
• LMWH and DOAC , timing is important
• Do not use NSAIDS periprocedure
• Discuss with haematologist if inherited bleeding disorders or platelet lower
than50x10 billion /L
Maryam Nasri 30.04.21Complications of I and R • Rare • Local migration • Distant migration • Damage to nerves • Deep implants Maryam Nasri 30.04.21
Maryam Nasri 30.04.21
Maryam Nasri 30.04.21
References
• https://www.oconmed.com/fileadmin/user_upload/Ocon-IUB-Doctors-Overview-DO_EN_090215_2.pdf
• https://www.fsrh.org/standards-and-guidance/current-clinical-guidance/quick-starting-contraception/
• https://www.fsrh.org/standards-and-guidance/documents/fsrh-guidance-contraception-for-women-aged-
over-40-years-2017/https://www.fsrh.org/news/the-fsrh-ceu-statement-regarding-delaying-versus-
immediately/
• https://www.fsrh.org/documents/fsrh-ceu-recommendation-on-extended-use-of-the-etonogestrel/
• https://www.fsrh.org/news/fsrh-new-guidance-service-provision-covid-second-wave/
• https://www.fsrh.org/documents/fsrh-rcog-rcm-statement-postpartum-contraception-
covid19/https://www.fsrh.org/documents/fsrh-clinical-effectiveness-unit-statement-use-of-combined/
Maryam Nasri 30.04.21You can also read