Promethazine overdose: clinical effects, predicting delirium and the effect of charcoal
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Q J Med 2009; 102:123–131
doi:10.1093/qjmed/hcn153 Advance Access publication 28 November 2008
Promethazine overdose: clinical effects, predicting delirium
and the effect of charcoal
C.B. PAGE1, S.B. DUFFULL2, I.M. WHYTE1,3 and G.K. ISBISTER1,3,4
From the 1Department of Clinical Toxicology and Pharmacology, Calvary Mater Newcastle Hospital,
Newcastle, NSW, Australia, 2School of Pharmacy, University of Otago, Dunedin, New Zealand,
3
Discipline of Clinical Pharmacology, Faculty of Health, University of Newcastle, Newcastle, NSW
and 4Tropical Toxinology Unit, Menzies School of Health Research, Charles Darwin University,
Downloaded from https://academic.oup.com/qjmed/article/102/2/123/1535782 by guest on 15 April 2021
Darwin, Australia
Received 8 August 2008 and in revised form 27 October 2008
Summary
Objective: The aim of this study was to describe the admitted to the intensive care unit (ICU) and
clinical effects of promethazine in overdose and four were ventilated. Delirium occurred in 33
explore the relationship between delirium and patients (42%), tachycardia (HR>100) occurred on
possible predictor variables. 44 occasions (56%) and hypotension only twice.
Methods: A case series of promethazine poisonings There were no seizures, dysrhythmias or deaths.
was identified from a prospective database of poi- Multivariate analysis of 215 presentations (in 181
soning admissions to a regional toxicology service. patients) where dose of promethazine ingested
Data were extracted including demographics, details was known demonstrated that dose, administra-
of ingestion, clinical features including delirium, tion of charcoal within 2 h and co-ingestants pre-
complications and medical outcomes. In addition dicted whether patients developed delirium. No
to descriptive statistics, a fully Bayesian approach relationship was shown for sex and age. A plot
using logistic regression was undertaken to investi- of probability that a patient will develop delirium
gate the relationship between predictor variables vs. dose was constructed which showed the prob-
and delirium. ability of delirium for 250 mg was 31%, 500 mg
Results: There were 199 patients with 237 presen- was 42% and for 1 g was 55% for promethazine
tations, including 57 patients with 78 prometha- alone overdoses.
zine alone overdoses. Of these 57 patients who Conclusion: The main feature of promethazine
ingested promethazine alone the median age toxicity is delirium, the probability of which can
was 22 years [interquartile range (IQR): 17–31] be predicted from the dose ingested. The adminis-
and 42 were female (74%). The median dose tration of charcoal and the presence of co-ingestants
ingested was 625 mg (IQR: 350–1250 mg). Median appears to reduce the probability of delirium in a
length of stay was 19 h (IQR: 13–27 h), ten were predictable manner.
Introduction
Promethazine hydrochloride is a phenothiazine antagonist at muscarinic (M1) and dopamine (D2)
derivative antihistamine first introduced in 1946 receptors.1–3 In Australia promethazine is available
which is used in multiple medical conditions as an over-the-counter (OTC) medication either
including allergic conditions, as an antiemetic and alone as a tablet or liquid preparation or in combi-
as a sedative/hypnotic agent. It is primarily a hista- nation with paracetamol and codeine phosphate as
mine (H1) receptor antagonist but is also a direct a syrup.
Address correspondence to Dr C.B. Page, Department of Clinical Toxicology and Pharmacology, Calvary Mater
Newcastle, NSW 2310, Australia. email: cpage@bigpond.net.au
! The Author 2008. Published by Oxford University Press on behalf of the Association of Physicians.
All rights reserved. For Permissions, please email: journals.permissions@oxfordjournals.org124 C.B. Page et al.
Promethazine alone in either formulation is The database in addition to being a quality assur-
rapidly absorbed after oral administration with ance tool is also used for research purposes. Its
peak concentrations after 2–3 h. It undergoes sig- use for retrospective reviews has previously been
nificant first pass metabolism with an oral avail- assessed by the Institutional Ethics Committee as
ability of 25%. Clinical effects are seen within an audit and has been exempted. A preformatted
20 min and its effects last 4–6 h. It is highly plasma admission sheet for all poisoning admissions is used
protein bound (80–90%) with a large volume of by medical staff to collect data17 and this and
distribution (13 l/kg) and undergoes hepatic metab- additional information from the medical record is
olism to three main inactive metabolites which entered into the database by two trained personnel
are renally excreted with only 2% of the drug blinded to any study hypotheses. In addition all
excreted in its parent form.1–4 admissions are reviewed on a weekly basis to
Reports of overdose with promethazine are finalise all data collection and resolve any discre-
predominately case reports5–8 with only one small pancies. Since 1992 additional methods to improve
Downloaded from https://academic.oup.com/qjmed/article/102/2/123/1535782 by guest on 15 April 2021
case series focussing on increased frequency of the accuracy and minimize inconsistencies in
poisoning when promethazine was released as an medical chart reviews as subsequently outlined by
OTC medication in New Zealand.9 Promethazine Gilbert et al.18 with the exception of formal testing
in overdose appears principally to cause central of interrater agreement were also performed.
nervous system (CNS) depression and anticholiner-
gic effects, including delirium, agitation and halluci- Selection of participants
nations. There are also reports of adverse effects All overdoses from the database between January
from therapeutic use of promethazine including 1987 and May 2007 were reviewed and admissions
dystonic reactions, psychosis in the absence of other that included promethazine at any dose either as
anticholinergic symptoms or signs and neuroleptic sole ingestant or with co-ingestants were extracted.
malignant syndrome (NMS).10–15 There is little All patients had a self-reported history of prometha-
information to assist clinicians in risk assessment zine ingestion confirmed on at least two occasions
and treatment of patients with promethazine over- by ED staff and the toxicology team in addition
dose, including what doses are associated with to information available from ambulance officers,
significant toxicity, the time course of CNS seda- family, friends and empty drug containers. Labora-
tion and delirium and the benefit of interventions tory confirmation of ingestion was not routinely
such as activated charcoal. utilised in promethazine ingestions.
We report a case series of consecutive prometha-
zine overdoses over a 20-year period to investigate Data collection and processing
the spectrum of clinical effects of promethazine
taken in overdose and also to explore the relation- The following information was extracted from the
ship between possible predictor variables and the database: patient demographic characteristics (age
occurrence of delirium, which we believe based on and sex), details of the promethazine ingestion
previous clinical experience to be the most impor- [estimated date and time of ingestion and estimated
tant clinical feature. amount ingested (mg)], co-ingested drugs (including
specific classes of drugs where there were enough
for analysis), clinical effects (pulse rate and blood
pressure) on admission and their respective relevant
Materials and methods maximum or minimum recording during admission,
Setting and study design Glasgow Coma Scale (GCS) score on admission,
minimum GCS score during admission, the presence
A case series of consecutive promethazine poison- of delirium (as defined by the attending Clinical
ing cases was included from presentations to a large Toxicologist as a rapid onset of a disturbance in
regional toxicology treatment unit which is the consciousness accompanied by a change in cogni-
primary referral centre for about 300 000 people. tion), outcomes or complications [seizures, dystonic
All patients presenting with poisoning to this unit reactions, neuroleptic malignant syndrome, dys-
are either seen and managed in the Emergency rhythmias, length of stay (LOS), Intensive Care Unit
Department (ED) by the toxicology service or seen, (ICU) admission, mortality], and treatment (decon-
managed and admitted as an in-patient by the tamination with activated charcoal, respiratory and
toxicology service. cardiovascular support). Minor discrepancies in
Detailed data on all presentations (ED atten- reported ingested dose that arose on repeated
dances and in-patient admissions) are entered into history taking were averaged prior to entry into the
a clinical database shortly after hospital discharge.16 database, otherwise more major discrepancies inPromethazine poisoning and delirium 125
dose were not recorded. The administration of char- Gibbs Sampling). This is a Bayesian statistical
coal was a clinical decision made by the attending modelling program that estimates the posterior
physician at the time. A standard dose was 50 g. probability distribution for the parameters of interest
Cathartic use with sorbitol was routine up to 1996. using Markov Chain Monte Carlo (MCMC) numer-
In patients who presented on more than ical simulation methods and can output a variety of
one occasion, the following rules were applied. statistics including the mean, median and credible
For those who only had multiple presentations interval from each posterior distribution. Decisions
of promethazine alone or only promethazine and about the inclusion of covariates can be made
co-ingestants, the first admission was used for sex by examining the probability distribution of the
and age calculation. All presentations were included coefficients, e.g. the posterior probability that the
to calculate other summary statistics. For those who coefficient is positive (or negative) is the area under
had presentations of both ingestions of prometha- the curve above (or below) zero. In addition, the
zine alone as well as with co-ingestants, the first dispersion of the distribution provides information
Downloaded from https://academic.oup.com/qjmed/article/102/2/123/1535782 by guest on 15 April 2021
promethazine alone presentation was used for sex on the strength of the data. Because this approach
and age calculations and subsequent promethazine does not involve hypothesis testing, there are no
alone presentations for other summary statistics. The type I error considerations with respect to each
presentations with promethazine and co-ingestants regression coefficient.
were included for other summary statistics only. The prior probability distributions for the regres-
Criteria for ICU admission for patients present- sion coefficients were defined by a multivariate
ing to the toxicology service are patients with a normal distribution with mean zero and variance of
decreased level of consciousness (GCS score 20% difference with or without the covariate.
Selection of variables was based on visual inspec-
Primary data analysis tion of the data and univariate analysis for the
dichotomous covariates. First order interaction terms
For descriptive statistics, medians and interquartile were considered in the modelling process. Good-
ranges (IQR) are reported for promethazine alone as ness of fit of the model was investigated by visual
a sole ingestant and with co-ingestants. Descriptive inspection of plots of the predicted probabilities
statistics were analysed with STATA version 7 from the logistic regression model vs. the empirical
(Stata Corp., USA). probabilities generated by binning the observed
To explore the relationship between clinically data and calculating the proportion of patients who
important predictor variables and delirium, a logistic had delirium.
regression model was developed with the all the Simulations from the final model in Win-
presentations where dose was known. Based on BUGS were used to create plots of the probability
known biological plausibility the following predictor of delirium vs. dose, including separate plots for
variables were considered: age, sex, prometha- patients not given charcoal and those given char-
zine dose, co-ingestants (including individual drug coal, and for patients taking co-ingestants and those
groups), administration of activated charcoal (at not. Adjusted odds ratios were estimated from the
any time,126 C.B. Page et al.
Table 1 Clinical features, outcomes and treatment of patients with promethazine ingestion
Promethazine alone All cases
Patients Admissions Patients Admissions
N = 57 N = 78 N = 199 N = 237
Age, year (IQR)a 22 (17–31) 29 (19–38)
Sex, female (%) 42 (74) 145 (73)
Dose ingested (IQR) 625 mg 500 mg
(350–1250) (240–1175)
Tachycardia on 43 (55) 119 (50)
admission (HR>100) (%)
Tachycardia during 45 (58) 128 (54)
Downloaded from https://academic.oup.com/qjmed/article/102/2/123/1535782 by guest on 15 April 2021
admission (HR>100) (%)
Hypotension on 0 (0) 3 (1)
admission (BPPromethazine poisoning and delirium 127
support was not required and there were no reported dose for promethazine alone presentations with
ECG changes or dysrhythmias apart from tachycar- delirium was 875 mg (IQR: 575–1250 mg) compared
dia. There were 44 presentations (56%) with an with 500 mg (IQR: 200–1250 mg) in those not
admission GCS score of 0% >10% >20%
Sex Female (%) Male (%)
26 29 3% ( 12 to 22) 64 4
Charcoal Nil (%) Charcoal (%)128 C.B. Page et al.
co-ingestion being included in the model. It was charcoal. Eleven of 36 patients (31%) who did not
found that the logarithmic transform of dose in receive charcoal developed delirium compared to
the covariate model provided the best fit for the four of the 27 patients who did receive charcoal
data. Further analysis with specific co-ingestants (15%). Finally, an analysis was done with random
demonstrated that benzodiazepine and alcohol effects included in the final model and the param-
co-ingestion were significant by themselves in eter estimates were only minimally effected suggest-
univariate analysis (Table 3). Administration of char- ing that there was little over dispersion.
coal within 2 h is more likely to be feasible than
within 1 h, so this was retained in the final model. Limitations
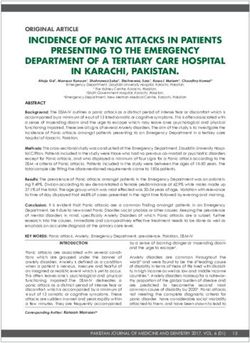
Plots of the probability of delirium vs. the dose
ingested for the final model (i.e. adjusted) showed This study has a number of limitations. Because the
the increasing probability of delirium with dose, study was a non-randomized retrospective analysis
the dose-dependent decreased risk of delirium of data collected at the time of discharge from
Downloaded from https://academic.oup.com/qjmed/article/102/2/123/1535782 by guest on 15 April 2021
with charcoal within 2 h and the dose-dependent patient’s charts, separately from any study hypoth-
eses, detailed information that may be relevant
decreased risk with co-ingestion of particular drugs
to certain drug toxicities may not be recorded. In
(Figure 1). For patients taking promethazine alone
addition, missing data may introduce some error
and not receiving charcoal, the probability that the
or bias in the results. However, entry of data in this
patient will become delirious after 250 mg is 31%,
manner allows the unbiased examination of drugs
500 mg is 42% and for 1 g is 55%. The adjusted odd
and their toxicity. A prospective study may for
ratios for the effect of charcoal, co-ingestants and
example allow more detailed examination of the
dose are provided in Table 4 from the final model.
delirium, including more accurate assessment of
To determine whether the administration of char-
the onset, duration and severity. Another limita-
coal within 2 h was confounded by time of pre-
tion of this study was that promethazine was not
sentation to hospital (within 2 h), we undertook an
measured in plasma to confirm the history of
analysis of a subgroup of patients presenting within
promethazine ingestion. However, all poisoned
2 h which included 63 admissions, 27 who received
patients admitted to having taken promethazine
which was confirmed by history on at least two
occasions, and confirmed by a history from ambu-
lance officers, family and friends as well as evidence
of empty drug containers. There is increasing
evidence that patient reports of ingestion and the
reported doses are reliable for research based on
pharmacokinetic studies.20,21
With regards selection bias, all patients assessed
and managed by the toxicology unit are either
self referred or referred by their primary care
practitioner. These patients are directed to our unit
preferentially over attending other hospitals in our
referral area, which do not have a toxicology
service. Therefore, patients from the total range
of intoxication are assessed and managed only
by our unit. A small number of patients who are
Table 4 Adjusted odds ratios for significant variables in
the final logistic regression model which included dose,
charcoal given within 2 h, coingestants and an interaction
term between dose and charcoal
Predictor Odds Credible limits
variable ratio (2.5% and 97.5%)
Dose [for every 1.11 1.04–1.18
Figure 1. Plots of the mean predicted probability of log(100 mg)]
delirium vs. dose for patients ingesting promethazine Charcoal < 2 h 0.12 0.02–0.39
alone with and without charcoal (top) and for patients Coingestants 0.43 0.21–0.78
co-ingesting other medications (bottom).Promethazine poisoning and delirium 129
significantly intoxicated and therefore requiring Discussion
intensive care may, but not necessarily always be
transferred to our unit from out of our primary This study demonstrates that promethazine in over-
referral area thus introducing a small amount of dose causes CNS depression, tachycardia and delir-
selection bias. ium, the last being the most important in terms of
An important source of bias in this study was the morbidity and resource requirement. There was a
possible misclassification of delirium, the main consistent association between reported dose and
feature of promethazine toxicity. The diagnosis the probability of delirium, not only for prometha-
of delirium although made prospectively was zine alone but also with co-ingestants. Charcoal
made by a number of different medical staff in a administered within 2 h appeared to reduce the
non-standardised manner. However, all patients risk of delirium occurring both in patients taking
recently admitted under the toxicology service are promethazine alone and those co-ingesting other
discussed on a weekly basis and important diagnosis drugs. The co-ingestion effect appears to be due to
Downloaded from https://academic.oup.com/qjmed/article/102/2/123/1535782 by guest on 15 April 2021
like delirium are discussed and finalized prior to sedation because it was significant for benzodiaze-
entry into the database. This review made misclas- pines and alcohol. The median LOS for presenta-
sification of the diagnosis of delirium unlikely. tions with delirium was significantly longer than
Absolute dose was used in the logistic regres- the LOS for presentations without delirium reflecting
sion model rather than dose corrected for weight the increased morbidity of delirium in overdose
(i.e. mg/kg) or dose corrected for lean body weight. presentations.
Although these adjustments may improve the ability There appeared to be a time-dependent effect of
of the model to predict delirium, weight (and height) the administration of charcoal because administer-
is difficult to measure in the clinical environment ing it at increasingly shorter times did decrease the
where overdose patients are managed. As a result probability of delirium. For charcoal administered
this makes the applicability of such a model limited within 2 h the probability of delirium was reduced
in the normal clinical setting where weight and by 20% in all cases or a relative risk of 0.47. It
height are unlikely to be available. would, therefore, appear to be reasonable to offer
The investigation of charcoal could also be charcoal to patients who present within 2 h if they
biased because patients were not randomized. For do not have significant CNS depression. However,
example, charcoal may have been given mainly administration within 4 h only reduced the prob-
to patients with no evidence of sedation, which ability of delirium by 9% and may be an insufficient
would immediately bias charcoal to patients with effect to warrant administration.
less toxicity and less probability of developing Delirium is the most common clinical effect of
delirium. However, the time-dependent effect of importance because of its implications for clinical
charcoal suggests this did not occur, at least not in care. Being able to predict the occurrence of delir-
all cases. Misclassification bias of charcoal use is ium based on dose may potentially improve the
unlikely to be a major source of bias as it is unlikely initial assessment and ongoing management of
to be administered without a written order in the patients. Tachycardia is more common but does
patient chart. The opposite is also unlikely to occur. not require any specific management as hypoten-
Lastly with respect to charcoal it was not possible sion was mild and uncommon. In addition, if it
to ascertain if: (i) the charcoal was completely was to occur it was nearly always present on admis-
taken and (ii) the charcoal was retained, i.e. the sion (Table 1) so its prediction is not required. The
patient did not vomit. However, misclassification other important clinical effects or complications
bias of charcoal use, incomplete administration and such as requirement for ventilation are important
any vomiting soon after charcoal administration will and are likely to be dose-dependent. However,
only bias towards the null and reduce the apparent only four patients who took promethazine alone
effect of charcoal. Doses ingested by those being were ventilated, making such an analysis difficult.
given charcoal within 2 h and those not were As in the case of tachycardia, the majority of
also similar. A re-analysis of patients presenting patient’s level of consciousness on admission did
within 2 h (i.e. able to be administered charcoal not deteriorate any further. Therefore, predicting
within 2 h) found a similar effect of charcoal. the occurrence of coma/respiratory failure adds
Lastly, although there were no dystonic reactions little to simple clinical observation.
reported. It is possible that this figure does not reflect With respect to promethazine alone in overdose,
the true incidence of reactions as these is often the extent of the CNS depression was almost always
delayed and therefore may occur after discharge evident on presentation allowing clinical manage-
requiring the patient to see their primary care ment and disposition decisions to be made at
practitioner or attend another health care facility. this early stage, although delirium may be initially130 C.B. Page et al.
masked by the sedation. Larger overdoses may Conflict of interest: None declared.
require intubation and ventilation for CNS depres-
sion but this was uncommon in our case series.
Other CNS toxicity, e.g. dystonias, NMS and sei- References
zures were not evident in our series reflecting that 1. Sharma A, Hamelin BA. Classic histamine H1 Receptor
these are uncommon. Tachycardia was common antagonists: a critical review of their metabolic and
but was only associated with hypotension on two pharmacokinetic fate from a bird’s eye view. Curr Drug
occasions, both of which were mild. Importantly Metab 2003; 4:105–29.
no dysrhythmias occurred despite some massive 2. Strenkoski-Nix LC, Ermer J, Decleene S, Cevallos W,
ingestions and animal evidence of sodium channel Mayer PR. Pharmacokinetics of promethazine hydrochlor-
ide after administration of rectal suppositories and oral
blockade similar to class one antiarrhythmic drugs.22 syrup to healthy subjects. Am J Health Syst Pharm 2000;
This contrasts with diphenhydramine, another com- 57:1499–505.
monly used antihistamine which has been reported
3. Paton DM, Webster DR. Clinical pharmacokinetics of
Downloaded from https://academic.oup.com/qjmed/article/102/2/123/1535782 by guest on 15 April 2021
to cause arrhythmias in overdose.23 H1 – receptor antagonists (The antihistamines). Clin
Previous reports5–14 have focussed on numerous Pharmacokinet 1985; 10:477–97.
adverse and toxicological effects from prometha- 4. Anonymous. Profile on Promethazine. Aust J Pharm 1984;
zine. These case reports by their nature give us a 65:114–8.
biased impression of the spectrum and/or incidence 5. Shawn DH, McGuigan MA. Poisoning from dermal absorp-
of promethazine toxicity. The one case series pub- tion of promethazine. Can Med Assoc J 1984; 130:1460–1.
lished to date15 only highlighted the high morbidity, 6. Leak D, Carroll D. Promethazine poisoning: Clinical and
i.e. ICU admissions associated with promethazine electroencephalographic observations. BMJ 1967; 2:31–32.
overdose when it became available as an OTC 7. Plant JR, Macleod DB. Response of a promethazine-induced
medication and reported no other clinical effects. coma to flumazenil. Ann Emerg Med 1994; 24:979–82.
Although it has not been validated the presence 8. Cowen PJ. Toxic psychosis with antihistamines reversed
of delirium can be predicted from the plots of the by physostigmine. Postgrad Med J 1979; 55:556–7.
probability of delirium vs. dose (Figure 1) which 9. Bergman J, Wallman P. Promethazine overdose: is it
may assist in helping the treating clinician determine ‘‘Goodnight’’ after all? NZ Med J 1998; 111:246–8.
the resources required, including a safe location, 10. DeGrandi T, Simon JE. Promethazine-induced dystonic
staff utilization and appropriate pharmacological reaction. Pediatr Emerg Care 1987; 3:91–2.
sedation if required. The co-ingestion of a sedating 11. Dollberg S, Hurvitz H, Kerem E, Navon P, Branski D.
medication, mainly benzodiazepines and alcohol Hallucinations and hyperthermia after promethazine
appears to reduce the risk of delirium. ingestion. Acta Paediatr Scand 1989; 78:131–2.
In conclusion, the major clinical effect of 12. Timnak C, Gleason O. Promethazine-induced psychosis in a
promethazine overdose is delirium which was 16-year-old girl. Psychosomatics 2004; 45:89–90.
dose related. The risk of delirium is reduced in 13. Mendhekar DN, Andrade CR. Neuroleptic malignant
patients co-ingesting other drugs, in particular, the syndrome with promethazine. Aust. NZ J Psychiatry 2005;
co-ingestion of benzodiazepines. Our study provides 39:310.
some evidence that the early administration of 14. Duggal HS. Neuroleptic malignant syndrome precipitated by
charcoal within 2 h may be potentially beneficial in promethazine and lorazepam. Aust NZ J Psychiatry 2001;
promethazine overdose but further prospective and 35:250–1.
randomized controlled trials to validate our model 15. Chan-Tack KM. Neuroleptic malignant syndrome due to
are warranted to confirm this. Mild to moderate promethazine. South Med J 1999; 92:1017–8.
CNS depression is common but coma requiring ven- 16. Whyte IM, Buckley NA, Dawson AH. Data collection in
tilatory assistance occurs infrequently, and severe clinical toxicology: are there too many variables? J Toxicol
Clin Toxicol 2002; 40:223–30.
cardiovascular effects did not occur in this study.
17. Buckley NA, Whyte IM, Dawson AH, Reith DA.
Preformatted admission charts for poisoning admissions
facilitate clinical assessment and research. Ann Emerg Med
Acknowledgements 1999; 34(4 Pt 1):476–82.
We acknowledge Debbie Whyte and Toni Nash for 18. Gilbert EH, Lowenstein SR, Koziol-McLain J, Barta DC,
data entry into the Hunter Area Toxicology Service Steiner J. Chart reviews in Emergency Medicine research:
Where are the methods? Ann Emerg Med 1996; 27:305–8.
database.
19. Spiegelhalter DJ, Best NG, Carlin BR, van der Linde A.
Bayesian measures of model complexity and fit. J R Stat Soc.
Funding Ser B-Stat Methodol 2002; 64:583–616.
NHMRC Clinical Career Development Award 20. Isbister GK, Friberg LE, Hackett LP, Duffull SB.
(ID300785 to G.I.). Pharmacokinetics of Quetiapine in overdose and the effectPromethazine poisoning and delirium 131
of activated charcoal. Clin Pharmacol and Ther 2007; 22. Tanaka H, Habuchi Y, Nishimura M, Sato N, Watanabe Y.
81:821–7. Blockade of Na+ current by promethazine in guinea-pig
21. Friberg LE, Isbister GK, Hackett LP, Duffull SB. The ventricular myocytes. Br J Pharmacol 1992; 106:900–5.
population pharmacokinetics of Citalopram after deliberate 23. Sype JW, Khan IA. Prolonged QT interval with markedly
self-poisoning: A Bayesian approach. J Pharmacokinet abnormal ventricular repolarization in diphenhydramine
Pharmacodyn 2005; 32:571–605. overdose. Int J Cardiol 2005; 99:333–5.
Downloaded from https://academic.oup.com/qjmed/article/102/2/123/1535782 by guest on 15 April 2021You can also read